The Business Model and Innovation Analyses: The Sustainable Transition Obstacles and Drivers for the Hospital Supply Chains

 , ,
, ,
Abstract
:1. Introduction
2. Literature Review
2.1. The Business Model and Innovation Concepts in the Hospital Context
2.2. The Sustainable TransitionsSupportive of the New Business Models and Innovation
2.3. The Sustainable Supply Chain for the Improvement of the Business Model and Innovation Perspectives
- The strategy—the holistic and purposeful identification of the individual SSC initiatives that align and support the organization’s overall sustainable strategy;
- The risk management—it includes the contingency planning for both upstream and downstream supply chains;
- The organizational culture—it is deeply rooted and encompasses the organizational citizenship, which includes the high ethical standards and the expectations (a foundation for the SSC), along with the respect for the society (both inside and outside the organization) and the natural environment; and
- The transparency—it is in terms of the engagement and the proactive communication with the key stakeholders and the traceability and the visibility in the upstream processes and the downstream supply chain operations.
3. Methodology
4. Results
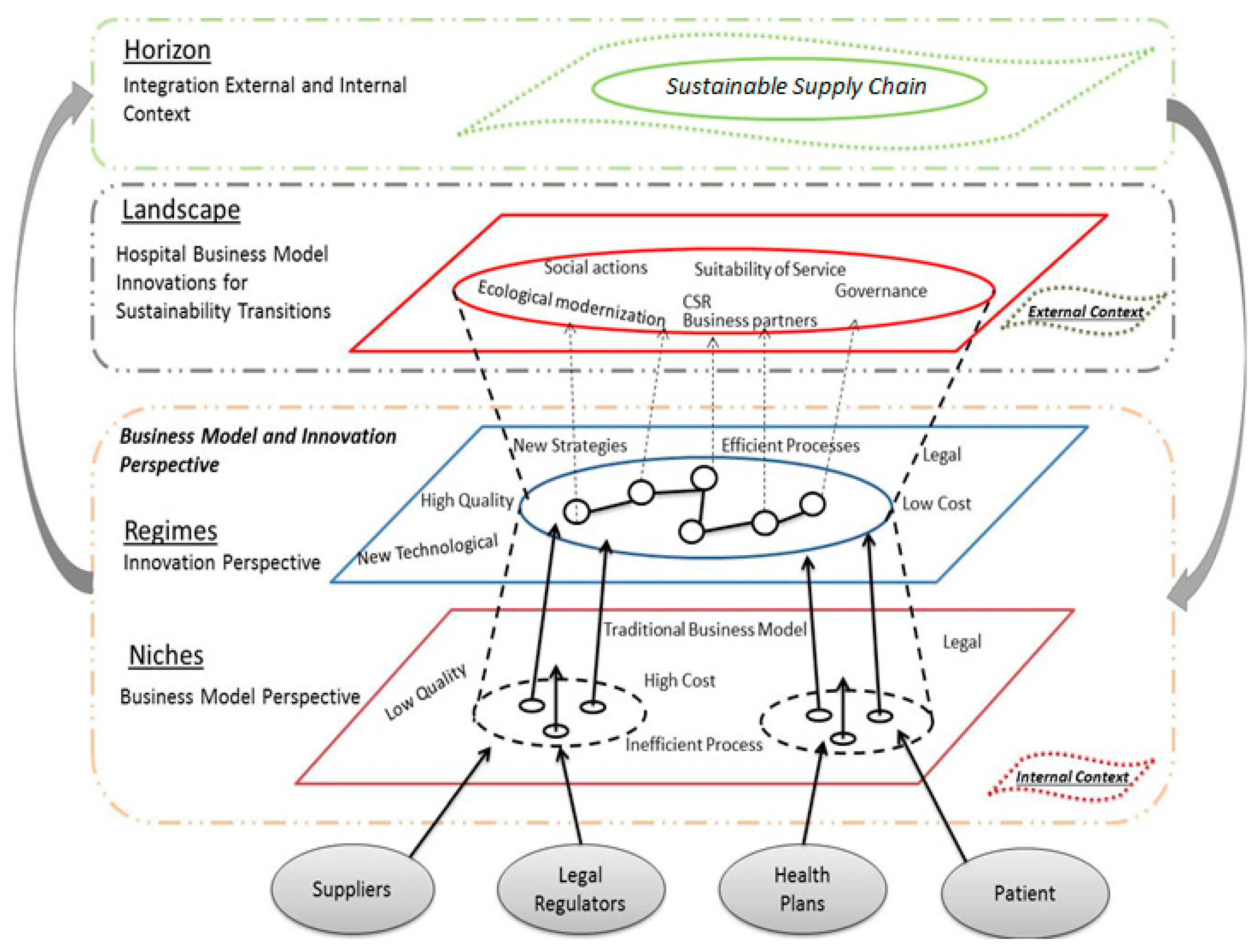
4.1. The Proposal of a Model to Assess the Business Models and the Innovation from the Perspective of the Sustainable Transitions and the Enablers for the Sustainable Supply Chain in the Hospitals
4.2. The Experts’ Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Christensen, C.M.; Overdorf, M. Meeting the challenge of disruptive change. Harvard Bus. Rev. 2000, 78, 66–77. [Google Scholar]
- Boons, F.; Lüdeke-Freund, F. Business models for sustainable innovation: State-of-the-art and steps towards a research agenda. J. Clean. Prod. 2013, 45, 9–19. [Google Scholar] [CrossRef]
- Osterwalder, A.; Pigneur, Y. Business Model Generation; John Wiley & sons: Hoboken, NJ, USA, 2010. [Google Scholar]
- Bohrer, C.T.; Vargas, E.R. Innovation in hospital services from a perspective of technical operations: Case studies in university hospitals. In Proceedings of the 7th International Conference on Innovation & Management, Wuhan, China, 4–5 December 2010. [Google Scholar]
- Amit, R.; Zott, C. Creating value through business model innovation. MIT Sloan Manag. Rev. 2012, 53, 41–42. [Google Scholar]
- Markard, J.; Raven, R.; Truffer, B. Sustainability transitions: An emerging field of research and its prospects. Res. Policy 2012, 41, 955–967. [Google Scholar] [CrossRef]
- Daunorienė, A.; Drakšaitė, A.; Snieška, V.; Valodkienė, G. Evaluating sustainability of sharing economy business models. Procedia Soc. Behav. Sci. 2015, 213, 836–841. [Google Scholar] [CrossRef]
- Dubois, E.; Schor, J.; Carfagna, L. Connected consumption: A sharing economy takes hold. Rotman Manag. 2014, 50–55. [Google Scholar]
- Manga, V.E.; Forton, O.T.; Mofor, L.A.; Woodard, R. Health care waste management in Cameroon: A case study from the Southwestern Region. Resour. Conserv.Recycl. 2011, 57, 108–116. [Google Scholar] [CrossRef]
- Kemp, R.; Schot, J.; Hoogma, R. Regime shifts to sustainability through processes of niche formation: The approach of strategic niche management. Technol. Anal. Strat. Manag. 1998, 10, 175–198. [Google Scholar] [CrossRef]
- Christensen, C M.; Horn, M.B.; Johnson, C.W. How Disruptive Innovation Will Change the Way We Learn; Education Week: Bethesda, MD, USA, 2008; Volume 27, pp. 25–36. [Google Scholar]
- Mathivathanan, D.; Kannan, D.; Haq, A.N. Sustainable supply chain management practices in Indian automotive industry: A multi-stakeholder view. Resour. Conserv. Recycl. 2018, 128, 284–305. [Google Scholar] [CrossRef]
- Balck, B.; Cracau, D. Empirical Analysis of Customer Motives in the Shareconomy: A Cross-Sectoral Comparison; University Magdeburg: Magdeburg, Germany, 2015. [Google Scholar]
- Gong, M.; Simpson, A.; Koh, L.; Tan, K.H. Inside out: The interrelationships of sustainable performance metrics and its effect on business decision making: Theory and practice. Resour. Conserv. Recycl. 2018, 128, 155–166. [Google Scholar] [CrossRef] [Green Version]
- Geels, F.W. Technological transitions as evolutionary reconfiguration processes: A multi-level perspective and a case-study. Research Policy 2002, 31, 1257–1274. [Google Scholar] [CrossRef]
- Schot, J.; Geels, F.W. Strategic niche management and sustainable innovation journeys: Theory, findings, research agenda, and policy. Technol. Analy. Strateg. Manag. 2008, 20, 537–554. [Google Scholar] [CrossRef]
- Geels, F.W. Ontologies, socio-technical transitions (to sustainability), and the multi-level perspective. Res. Policy 2010, 39, 495–510. [Google Scholar] [CrossRef]
- Lozano, R. Envisioning sustainability three-dimensionally. J. Clean. Prod. 2008, 16, 1838–1846. [Google Scholar] [CrossRef]
- Gansky, L. The Mesh: Why the Future of Business Is Sharing; Penguin: New York, NY, USA, 2010. [Google Scholar]
- Lin, K.P.; Tseng, M.L.; Pai, P.F. Sustainable supply chain management using approximate fuzzy DEMATEL method. Resour. Conserv. Recycl. 2018, 128, 134–142. [Google Scholar] [CrossRef]
- Schaltegger, S.; Hansen, E.; Lüdeke-Freund, F. Business models for sustainability: Origins, present research, and future avenues. Organ. Environ. 2016. [Google Scholar] [CrossRef]
- Dou, Y.; Togawa, T.; Dong, L.; Fujii, M.; Ohnishi, S.; Tanikawa, H.; Fujita, T. Innovative planning and evaluation system for district heating using waste heat considering spatial configuration: A case in Fukushima, Japan. Resour. Conserv. Recycl. 2018, 128, 406–416. [Google Scholar] [CrossRef]
- Zott, C.; Amit, R.; Massa, L. The business model: Recent developments and future research. J. Manag. 2011, 37, 1019–1042. [Google Scholar]
- Shafer, S.M.; Smith, H.J.; Linder, J.C. The power of business models. Bus. Horiz. 2005, 48, 199–207. [Google Scholar] [CrossRef]
- Osterwalder, A.; Pigneur, Y. Modeling value propositions in e-Business. In Proceedings of the 5th international conference on Electronic commerce—ICEC ’03, Pittsburgh, PA, USA, 30 September–3 October 2003; ACM Press: New York, NY, USA, 2003; pp. 429–436. [Google Scholar]
- Osterwalder, A.; Pigneur, Y.; Tucci, C.L. Clarifying Business Models: Origins, Present and Future of the Concept. Commun. Assoc. Inf. Syst. 2005, 16, 1–29. [Google Scholar] [CrossRef]
- Zott, C.; Amit, R.; Massa, L. The Business Model: Theoretical Roots, Recent Developments, and Future Research; IESE Business School: Barcelona, Spain, 2010. [Google Scholar]
- Gallouj, F.; Weinstein, O. Innovation in services. Res. Policy 1997, 2, 537–556. [Google Scholar] [CrossRef]
- Hwang, J.; Christensen, C.M. Disruptive innovation in health care delivery: A framework for business-model innovation. Health Aff. 2008, 27, 1329–1335. [Google Scholar] [CrossRef] [PubMed]
- Pfannstiel, M.A.; Rasche, C. Service Business Model Innovation in Healthcare and Hospital Management; Springer Science and Business Media: Berlin, Germany, 2017. [Google Scholar]
- Teece, D.J. Business models, business strategy and innovation. Long Range Plan. 2010, 43, 172–194. [Google Scholar] [CrossRef]
- Ahmadi, H.B.; Kusi-Sarpong, S.; Rezaei, J. Assessing the social sustainability of supply chains using best worst method. Resour. Conserv. Recycl. 2017, 126, 99–106. [Google Scholar] [CrossRef]
- Salge, T.O.; Kohli, R.; Barrett, M. Investing in information systems: On the behavioral and institutional search mechanisms underpinning hospitals is investment decisions. Mis. Q. 2015, 39, 61–90. [Google Scholar] [CrossRef]
- Woolridge, A.; Morrissey, A.; Phillips, P.S. The development of strategic and tactical tools, using systems analysis, for waste management in large complex organisations: A case study in UK healthcare waste. Resour. Conserv. Recycl. 2005, 44, 115–137. [Google Scholar] [CrossRef]
- Lehoux, P.; Daudelin, G.; Williams-Jones, B.; Denis, J.L.; Longo, C. How do business model and health technology design influence each other? Insights from a longitudinal case study of three academic spin-offs. Res. Policy 2014, 43, 1025–1038. [Google Scholar] [CrossRef]
- Janssen, M.; Moors, E.H. Caring for healthcare entrepreneurs-towards successful entrepreneurial strategies for sustainable innovations in Dutch healthcare. Technol. Forecast. Soc. Change 2013, 80, 1360–1374. [Google Scholar] [CrossRef]
- King, R.; Green, P. Governance of primary healthcare practices: Australian insights. Bus. Horiz. 2012, 55, 593–608. [Google Scholar] [CrossRef]
- Faezipour, M.; Ferreira, S. A system dynamics perspective of patient satisfaction in healthcare. Procedia Comput. Sci. 2013, 16, 148–156. [Google Scholar] [CrossRef]
- Nelson, M.L.; Sen, R. Business rules management in healthcare: A lifecycle approach. Decis. Support Syst. 2014, 57, 387–394. [Google Scholar] [CrossRef]
- Sousa-Zomer, T.T.; Miguel, P.A.C. Sustainable business models as an innovation strategy in the water sector: An empirical investigation of a sustainable product-service system. J. Clean. Prod. 2016. [Google Scholar] [CrossRef]
- Grin, J.; Rotmans, J.; Schot, J. Transitions to Sustainable Development: New Directions in the Study of Long Term Transformative Change; Routledge: London, UK, 2010. [Google Scholar]
- Smith, A.; Voß, J.P.; Grin, J. Innovation studies and sustainability transitions: The allure of the multi-level perspective and its challenges. Res. Policy 2010, 39, 435–448. [Google Scholar] [CrossRef]
- Loorbach, D.; Frantzeskaki, N.; Thissen, W. A transition research perspective on governance for sustainability. In European Research on Sustainable Development; Springer Berlin Heidelberg: Heidelberg, Germany, 2011; pp. 73–89. [Google Scholar]
- Hekkert, M.P.; Negro, S.O. Functions of innovation systems as a framework to understand sustainable technological change: Empirical evidence for earlier claims. Technol. Forecast. Soc. Change 2008, 76, 584–594. [Google Scholar] [CrossRef]
- Russo, F. What is the CSR’s focus in healthcare? J. Bus. Ethics 2016, 134, 323–334. [Google Scholar] [CrossRef]
- Van der Geest, S.; Speckmann, J.D.; Streefland, P.H. Primary health care in a multi-level perspective: Towards a research agenda. Soc. Sci. Med. 1990, 30, 1025–1034. [Google Scholar] [CrossRef]
- Geels, F.W. From sectoral systems of innovation to socio-technical systems: Insights about dynamics and change from sociology and institutional theory. Res. Policy 2004, 33, 897–920. [Google Scholar] [CrossRef]
- Shove, E.; Walker, G. CAUTION! Transitions ahead: politics, practice, and sustainable transition management. Environ. Plan. A 2007, 39, 763–770. [Google Scholar] [CrossRef]
- Geels, F.W.; Hekkert, M.P.; Jacobsson, S. The dynamics of sustainable innovation journeys. Technol. Anal. Strateg. Manag. 2008, 20, 521–536. [Google Scholar] [CrossRef]
- Broerse, J.; Grin, J. Toward Sustainable Transitions in Healthcare Systems; Taylor& Francis: Abingdon, UK, 2017. [Google Scholar]
- Jacobsson, S.; Bergek, A. Innovation system analyses and sustainability transitions: Contributions and suggestions for research. Environ. Innov. Soc. Transit. 2011, 1, 41–57. [Google Scholar] [CrossRef]
- Seuring, S.; Müller, M. From a literature review to a conceptual framework for sustainable supply chain management. J. Clean. Prod. 2008, 16, 1699–1710. [Google Scholar] [CrossRef]
- Carter, C.R.; Easton, L.P. Sustainable supply chain management: Evolution and future directions. Int. J. Phys. Distrib Logist. Manag. 2011, 41, 46–62. [Google Scholar] [CrossRef]
- Viani, C.; Vaccari, M.; Tudor, T. Recovering value from used medical instruments: A case study of laryngoscopes in England and Italy. Resour. Conserv. Recycl. 2016, 111, 1–9. [Google Scholar] [CrossRef]
- Kleindorfer, P.R.; Singhal, K.; Wassenhove, L.N. Sustainable operations management. Prod. Oper. Manag. 2005, 14, 482–492. [Google Scholar] [CrossRef]
- Zhang, M.; Tse, Y.K.; Doherty, B.; Li, S.; Akhtar, P. Sustainable supply chain management: Confirmation of a higher-order model. Resour. Conserv. Recycl. 2018, 128, 206–221. [Google Scholar] [CrossRef] [Green Version]
- Pagell, M.; Wu, Z. Building a more complete theory of sustainable supply chain management using case studies of 10 exemplars. J. Supply Chain Manag. 2009, 45, 37–56. [Google Scholar] [CrossRef]
- Beske, P. Dynamic capabilities and sustainable supply chain management. Int. J. Phys. Distrib. Logist. Manag. 2012, 42, 372–387. [Google Scholar] [CrossRef]
- Epstein, M.J.; Roy, M.J. Sustainability in action: Identifying and measuring the key performance drivers. Long Range Plan. 2001, 34, 585–604. [Google Scholar] [CrossRef]
- Campion, N.; Thiel, C.L.; Woods, N.C.; Swanzy, L.; Landis, A.E.; Bilec, M.M. Sustainable healthcare and environmental life-cycle impacts of disposable supplies: A focus on disposable custom packs. J. Clean. Prod. 2015, 94, 46–55. [Google Scholar] [CrossRef]
- Russo, M.V.; Fouts, P.A. A resource-based perspective on corporate environmental performance and profitability. Acad. Manag. J. 1997, 40, 534–559. [Google Scholar]
- Mani, V.; Gunasekaran, A.; Papadopoulos, T.; Hazen, B.; Dubey, R. Supply chain social sustainability for developing nations: Evidence from India. Resour. Conserv. Recycl. 2016, 111, 42–52. [Google Scholar] [CrossRef] [Green Version]
- Chen, I.J.; Paulraj, A. Towards a theory of supply chain management: the constructs and measurements. J. Oper. Manag. 2004, 22, 119–150. [Google Scholar] [CrossRef] [Green Version]
- Inghels, D.; Dullaert, W.; Bloemhof, J. A model for improving sustainable green waste recovery. Resour. Conserv. Recycl. 2016, 110, 61–73. [Google Scholar] [CrossRef]
- Carter, C.R.; Rogers, D.S. A framework of sustainable supply chain management: Moving toward new theory. Int.J. Phys. Distrib. Logist. Manag. 2008, 38, 360–387. [Google Scholar] [CrossRef]
- Rotmans, J.; Loorbach, D. Complexity and transition management. J. Ind. Ecol. 2009, 13, 84–196. [Google Scholar] [CrossRef]
- Machado, C.M.; Scavarda, A.; Vaccaro, G.; Korzenowski, A.L.; Batista, E. Analysis of hospital’s sustainability: Economical, environmental, and social lenses. In Proceedings of the 2015 Industrial and Systems Engineering Research Conference, Nashville, TN, USA, 30 May–2 June 2015. [Google Scholar]
- Liamputtong, P. Qualitative Research Methods; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- World Health Organization. Technical Brief: HIV Patient Monitoring and Case Surveillance: Adapting and Implementing New Recommendations on HIV Patient Monitoring; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Unger, S.; Landis, A. Assessing the environmental, human health, and economic impacts of reprocessed medical devices in a Phoenix hospital’s supply chain. J. Clean. Prod. 2016, 112, 1995–2003. [Google Scholar] [CrossRef]
- Manogaran, G.; Thota, C.; Lopez, D.; Sundarasekar, R. Big data security intelligence for healthcare industry 4.0. In Cybersecurity for Industry 4.0; Springer International Publishing: Berlin, Germany, 2017; pp. 103–126. [Google Scholar]
- Thuemmler, C.; Bai, C. Health 4.0: Application of Industry 4.0 Design Principles in Future Asthma Management. In Health 4.0: How Virtualization and Big Data Are Revolutionizing Healthcare; Springer International Publishing: Berlin, Germany, 2017; pp. 23–37. [Google Scholar]
- Wang, Y.; Kung, L.; Wang, W.Y.C.; Cegielski, C.G. An integrated big data analytics-enabled transformation model: Application to health care. Inf. Manag. 2017. [Google Scholar] [CrossRef]
- Rosca, E.; Arnold, M.; Bendul, J.C. Business models for sustainable innovation—An empirical analysis of frugal products and services. J. Clean. Prod. 2016. [Google Scholar] [CrossRef]
- Robert, G.B.; Anderson, J.E.; Burnett, S.J.; Aase, K.; Andersson-Gare, B.; Fulop, N.J. A longitudinal, multi-level comparative study of quality and safety in European hospitals: The QUASER study protocol. BMC Health Serv. Res. 2011, 11, 285. [Google Scholar] [CrossRef]
- Lapointe, L.; Mignerat, M.; Vedel, I. The IT productivity paradox in health: A stakeholder’s perspective. Int. J. Med. Inf. 2011, 80, 102–115. [Google Scholar] [CrossRef]
- Gaustad, G.; Krystofik, M.; Bustamante, M.; Badami, K. Circular economy strategies for mitigating critical material supply issues. Resour. Conserv. Recycl. 2017. [Google Scholar] [CrossRef]
- Schor, J.B. Born to Buy: The Commercialized Child and the New Consumer Cult; Simon and Schuster: New York, NY, USA, 2014. [Google Scholar]
- Oftelie, A. Leadership in the new era of convergence. Kennedy Sch. Rev. 2015, 15, 113–120. [Google Scholar]
- Angeli, F.; Jaiswal, A.K. Business model innovation for inclusive health care delivery at the bottom of the pyramid. Organ. Environ. 2016, 29, 486–507. [Google Scholar] [CrossRef]
- Bonciu, F.; Balgar, A.C. Sharing economy as a contributor to sustainable growth, an EU perspective. Rom. J. Eur. Aff. 2016, 16, 36. [Google Scholar]
- Boons, F.; Montalvo, C.; Quist, J.; Wagner, M. Sustainable innovation, business frameworks and economic performance: an overview. J. Clean. Prod. 2013, 45, 1–8. [Google Scholar] [CrossRef]
- Miller, B.J.; Moore, D.W.; Schmidt, C.W., Jr. Telemedicine and the sharing economy: The “Uber” for healthcare. Am. J. Manag. Care 2016, 22, 420–422. [Google Scholar]
- Geels, F.W. The impact of the financial-economic crisis on sustainability transitions: Financial investment, governance and public discourse. Environ. Innov. Soc. Transit. 2013, 6, 67–95. [Google Scholar] [CrossRef]
- Christensen, C.M.; Grossman, J.H.; Hwang, J. The Innovator’s Prescription. Soundview Executive Book Summaries. Available online: https://www.lumc.nl/sub/9300/att/1402060248071959.pdf (accessed on 2 November 2017).


{kind=link}
| Expert’s | Professional Position | Years of Experience | Education | Hospital |
|---|---|---|---|---|
| Expert 1 | Controller Manager | 15 years | Master | Private |
| Expert 2 | Quality Coordinator | 20 years | Ungraduate | Private |
| Expert 3 | Financial Manager | 10 years | Specialist | Private |
| Expert 4 | Operations Manager | 19 years | Master | Private |
| Expert 5 | Manager of Supply Chain | 11 years | Specialist | Private |
| Expert 6 | Marketing Supervisor | 8 years | Specialist | Private |
| Expert 7 | Services Manager | 12 years | Master | Private |
| I) What is the hospital’s business model? How has it developed over time? What are the latest changes? How and why did they happen? |
| II) What is the impact of governance on business models? |
| III) What is the impact of technology on business models? |
| IV) What impact does quality generate on business models? |
| V) What is the impact of external context strategies on business models? |
| VI) How do you relate business models to innovation? |
| VII) What does the hospital expect when considering innovation in the business model (if there is an integrated approach)? What are the expected results of the different innovations? Are there success stories and failure cases that can illustrate this relationship? How did they behave? Why were they satisfactory or not? |
| VIII) Are there moves in business models that aim at a transition to sustainability in the hospital context? |
| IX) What does the hospital expect when it considers sustainability in the business model (if there is an integrated approach)? What are the expected results of the different sustainable actions in the business? Are there success stories and failure cases that can illustrate this relationship? How did they behave? Why were they satisfactory or not? |
| X) Assessing the context in which hospitals are embedded, is it possible to determine which key actors interfere with business models? |
| XI) In the context of the actors, it is possible to determine that an actor can influence their relationship network/partnerships? What are the possible influences that can be generated? |
| XII) Does the relationship determined by the set of actors generate benefits or not within its centrality? |
| XIII) Within the idea of governance, does governance exist within this set of actors? Are there examples? |
| XIV) Is it possible that sustainable supply chain may exist within this network of actors? Are there successes and failures to illustrate these partnerships? What are the key benefits expected? |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopes, C.M.; Scavarda, A.J.; Carvalho, M.N.M.d.; Korzenowski, A.L. The Business Model and Innovation Analyses: The Sustainable Transition Obstacles and Drivers for the Hospital Supply Chains. Resources 2019, 8, 3. https://doi.org/10.3390/resources8010003
Lopes CM, Scavarda AJ, Carvalho MNMd, Korzenowski AL. The Business Model and Innovation Analyses: The Sustainable Transition Obstacles and Drivers for the Hospital Supply Chains. Resources. 2019; 8(1):3. https://doi.org/10.3390/resources8010003
Chicago/Turabian StyleLopes, Catia Milena, Annibal José Scavarda, Mauricio Nunes Macedo de Carvalho, and André Luis Korzenowski. 2019. "The Business Model and Innovation Analyses: The Sustainable Transition Obstacles and Drivers for the Hospital Supply Chains" Resources 8, no. 1: 3. https://doi.org/10.3390/resources8010003