E-Health Tools to Improve Antibiotic Use and Resistances: A Systematic Review


 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Search Strategy and Inclusion Criteria
(clinical-decision-support-system OR decision-support-system OR computer-assisted decision-making OR expert-system OR decision-support) AND (antimicrobial resistance OR antimicrobial OR antibiotic* OR antimicrobial management) AND (electronic health OR e-health) NOT Tele-health.
2.3. Quality Assessment of the Included Studies
- (1)
- Allocation of study groups (random: 2, quasi-random: 1, selected controls: 0);
- (2)
- Unit of allocation (cluster (such as a practice): 2, physician: 1, patient: 0);
- (3)
- Baseline differences (presence of baseline differences with statistical adjustments: 2, baseline with no adjustments: 1, no baseline differences: 0);
- (4)
- Objectivity of the outcome (blinded assessment: 2, no blinding but defined assessment criteria: 1, no blinding and poorly defined: 0);
- (5)
- Completeness of follow-up (>90%: 2, 80–90%: 1, <80% or not described: 0).
2.4. Data Extraction and Analysis
3. Results
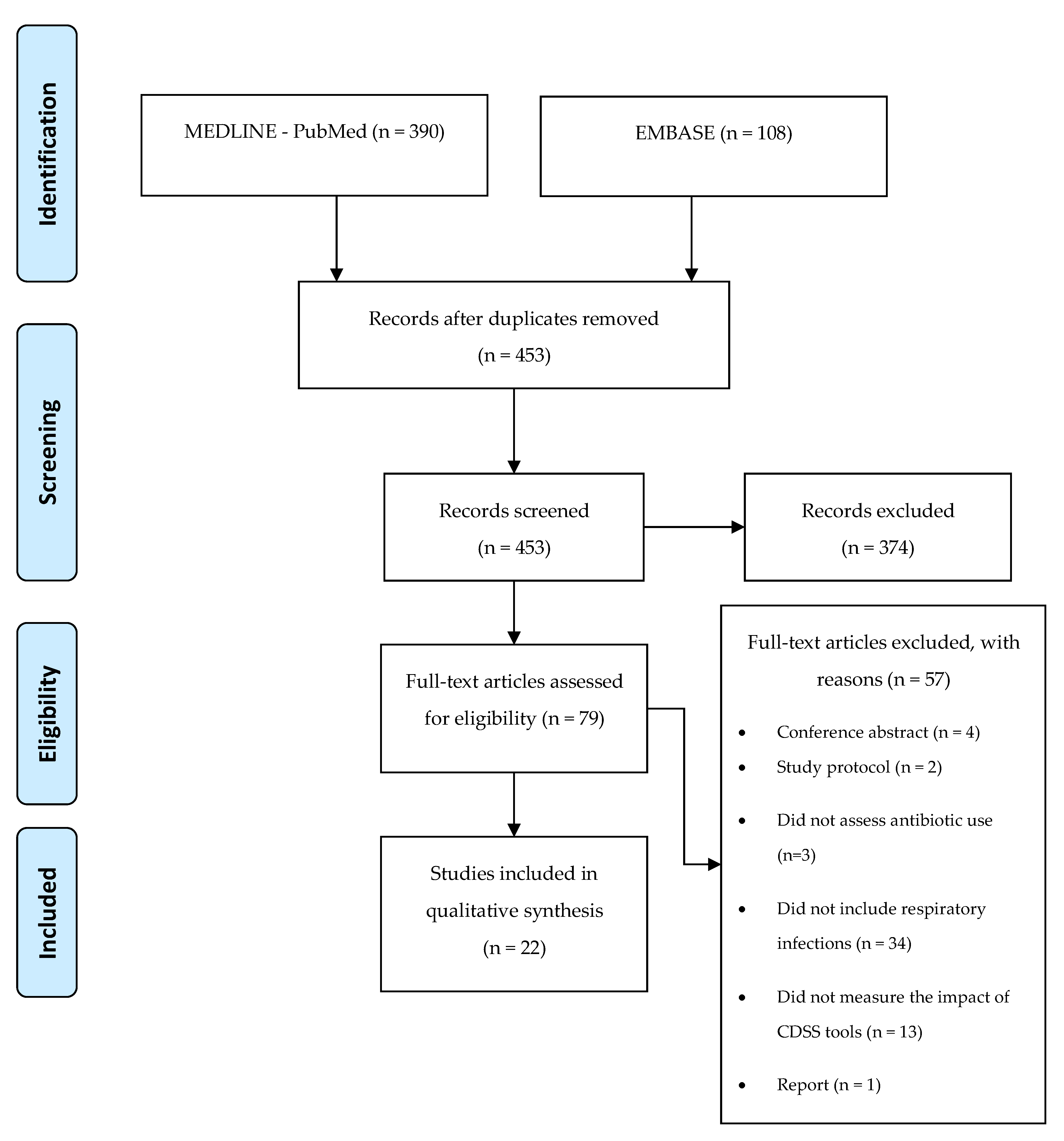
3.1. Study Selection
3.2. Quality Assessment
3.3. Study Characteristics
3.3.1. Study Design
3.3.2. Location
3.3.3. Setting
3.3.4. Study Population
3.3.5. Diseases
3.3.6. Intervention
3.3.7. Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mohr, K.I. History of Antibiotics Research. Curr. Top. Microbiol. Immunol. 2016, 398, 237–272. [Google Scholar] [CrossRef] [PubMed]
- Goossens, H.; Ferech, M.; Vander Stichele, R.; Elseviers, M. Outpatient antibiotic use in Europe and association with resistance: A cross-national database study. Lancet 2005, 365, 579–587. [Google Scholar] [CrossRef]
- Aslam, B.; Wang, W.; Arshad, M.I.; Khurshid, M.; Muzammil, S.; Rasool, M.H.; Nisar, M.A.; Alvi, R.F.; Aslam, M.A.; Qamar, M.U.; et al. Antibiotic resistance: A rundown of a global crisis. Infect. Drug Resist. 2018, 11, 1645–1658. [Google Scholar] [CrossRef] [Green Version]
- Shively, N.R.; Buehrle, D.J.; Clancy, C.J.; Decker, B.K. Prevalence of Inappropriate Antibiotic Prescribing in Primary Care Clinics within a Veterans Affairs Health Care System. Antimicrob. Agents Chemother. 2018, 62, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hulscher, M.E.; Grol, R.P.; van der Meer, J.W. Antibiotic prescribing in hospitals: A social and behavioural scientific approach. Lancet Infect. Dis. 2010, 10, 167–175. [Google Scholar] [CrossRef]
- Forum of International Respiratory Societies. Respiratory Diseases in the World Realities of Today-Opportunities for Tomorrow, 1st ed.; European Respiratory Society: Sheffield, UK, 2013; ISBN 9781849840569. Available online: https://www.theunion.org/what-we-do/publications/technical/english/FIRS_report_for_web.pdf (accessed on 24 June 2020).
- Pattemore, P.K.; Jennings, L.C. Epidemiology of Respiratory Infections. In Pediatric Respiratory Medicine; Elsevier: Amsterdam, The Netherlands, 2008; pp. 435–452. ISBN 9780323040488. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7151775/ (accessed on 24 June 2020).
- Brenda Tesini Overview of Viral Respiratory Infections-Infectious Diseases-MSD Manual Professional Edition. Available online: https://www.msdmanuals.com/professional/infectious-diseases/respiratory-viruses/overview-of-viral-respiratory-infections (accessed on 23 May 2020).
- Sahadulla, M. Infections of the Respiratory System. In Concise Handbook of Infectious Diseases; Jaypee Brothers Medical Publishers (P) Ltd.: New Delhi, India, 2018; ISBN 0963117211. Available online: https://www.jaypeedigital.com/book/9789386261939/chapter/ch11 (accessed on 23 May 2020).
- World Health Organization. 2019 Antibacterial Agents in Clinical Development-an Analysis of the Antibacterial Clinical Development Pipeline; World Health Organization: Geneva, Switzerland, 2019; ISBN 9789240000193. Available online: https://apps.who.int/iris/bitstream/handle/10665/330420/9789240000193-eng.pdf (accessed on 27 May 2020).
- Kraus, E.M.; Pelzl, S.; Szecsenyi, J.; Laux, G. Antibiotic prescribing for acute lower respiratory tract infections (LRTI) – guideline adherence in the German primary care setting: An analysis of routine data. PLoS ONE 2017, 12, e0174584. [Google Scholar] [CrossRef]
- Velickovski, F.; Ceccaroni, L.; Roca, J.; Burgos, F.; Galdiz, J.B.; Marina, N.; Lluch-Ariet, M. Clinical Decision Support Systems (CDSS) for preventive management of COPD patients. J. Transl. Med. 2014, 12, S9. [Google Scholar] [CrossRef] [Green Version]
- dos Santos, M.A.F.R.N.; Tygesen, H.; Eriksson, H.; Herlitz, J. Clinical decision support system (CDSS)–effects on care quality. Int. J. Health Care Qual. Assur. 2014, 27, 707–718. [Google Scholar] [CrossRef] [Green Version]
- Sutton, R.T.; Pincock, D.; Baumgart, D.C.; Sadowski, D.C.; Fedorak, R.N.; Kroeker, K.I. An overview of clinical decision support systems: Benefits, risks, and strategies for success. NPJ Digit. Med. 2020, 3, 17. [Google Scholar] [CrossRef] [Green Version]
- Kawamoto, K.; Houlihan, C.A.; Balas, E.A.; Lobach, D.F. Improving clinical practice using clinical decision support systems: A systematic review of trials to identify features critical to success. BMJ 2005, 330, 765. [Google Scholar] [CrossRef] [Green Version]
- Kannry, J.; McCullagh, L.; Kushniruk, A.; Mann, D.; Edonyabo, D.; McGinn, T. A Framework for Usable and Effective Clinical Decision Support: Experience from the iCPR Randomized Clinical Trial. eGEMs 2015, 3, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sim, I.; Gorman, P.; Greenes, R.A.; Haynes, R.B.; Kaplan, B.; Lehmann, H.; Tang, P.C. Clinical Decision Support Systems for the Practice of Evidence-based Medicine. J. Am. Med. Informatics Assoc. 2001, 8, 527–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehmann, C.U.; Séroussi, B.; Jaulent, M.-C. Troubled Waters: Navigating Unintended Consequences of Health Information Technology. Yearb. Med. Inform. 2016, 25, 5–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SPMS-Serviços Partilhados do Ministério da Saúde. eHealth em Portugal-Visão 2020; SPMS: Lisboa, Portugal, 2015; Available online: http://spms.min-saude.pt/wp-content/uploads/2015/11/Relatório-Think-Tank-eHealth-2020-v05112015.pdf (accessed on 4 June 2020).
- Bremmer, D.N.; Trienski, T.L.; Walsh, T.L.; Moffa, M.A. Role of Technology in Antimicrobial Stewardship. Med. Clin. North Am. 2018, 102, 955–963. [Google Scholar] [CrossRef]
- PRISMA PRISMA Statement-Checklist. Available online: http://www.prisma-statement.org/PRISMAStatement/Checklist (accessed on 27 May 2020).
- Carvalho, É.F.S.; Estrela, M.; Figueiras, A.; Roque, F.; Herdeiro, M.T. eHealth tools to improve antibiotic use and resistances: A systematic review. PROSPERO 2020 CRD42020167316. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=167316 (accessed on 4 June 2020).
- Carracedo-Martinez, E.; Gonzalez-Gonzalez, C.; Teixeira-Rodrigues, A.; Prego-Dominguez, J.; Takkouche, B.; Herdeiro, M.T.; Figueiras, A. Computerized Clinical Decision Support Systems and Antibiotic Prescribing: A Systematic Review and Meta-analysis. Clin. Ther. 2019, 41, 552–581. [Google Scholar] [CrossRef]
- Garg, A.X.; Adhikari, N.K.J.; McDonald, H.; Rosas-Arellano, M.P.; Devereaux, P.J.; Beyene, J.; Sam, J.; Haynes, R.B. Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: A systematic review. J. Am. Med. Assoc. 2005, 293, 1223–1238. [Google Scholar] [CrossRef]
- Bourgeois, F.C.; Linder, J.; Johnson, S.A.; Co, J.P.T.; Fiskio, J.; Ferris, T.G. Impact of a computerized template on antibiotic prescribing for acute respiratory infections in children and adolescents. Clin. Pediatr. (Phila). 2010, 49, 976–983. [Google Scholar] [CrossRef]
- Gifford, J.; Vaeth, E.; Richards, K.; Siddiqui, T.; Gill, C.; Wilson, L.; DeLisle, S. Decision support during electronic prescription to stem antibiotic overuse for acute respiratory infections: A long-term, quasi-experimental study. BMC Infect. Dis. 2017, 17, 528. [Google Scholar] [CrossRef] [Green Version]
- Linder, J.A.; Schnipper, J.L.; Tsurikova, R.; Yu, T.; Volk, L.A.; Melnikas, A.J.; Palchuk, M.B.; Olsha-Yehiav, M.; Middleton, B. Documentation-based clinical decision support to improve antibiotic prescribing for acute respiratory infections in primary care: A cluster randomised controlled trial. Inform. Prim. Care 2009, 17, 231–240. [Google Scholar] [CrossRef] [Green Version]
- Linder, J.A.; Bates, D.W.; Williams, D.H.; Connolly, M.A.; Middleton, B. Acute infections in primary care: Accuracy of electronic diagnoses and electronic antibiotic prescribing. J. Am. Med. Inform. Assoc. 2006, 13, 61–66. [Google Scholar] [CrossRef]
- Linder, J.; Schnipper, J.L.; Volk, L.A.; Tsurikova, R.; Palchuk, M.; Olsha-Yehiav, M.; Melnikas, A.J.; Middleton, B. Clinical decision support to improve antibiotic prescribing for acute respiratory infections: Results of a pilot study. AMIA Annu. Symp. Proc. 2007, 468–472. [Google Scholar]
- Litvin, C.B.; Ornstein, S.M.; Wessell, A.M.; Nemeth, L.S.; Nietert, P.J. Use of an electronic health record clinical decision support tool to improve antibiotic prescribing for acute respiratory infections: The ABX-TRIP study. J. Gen. Intern. Med. 2013, 28, 810–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mainous, A.G., 3rd; Lambourne, C.A.; Nietert, P.J. Impact of a clinical decision support system on antibiotic prescribing for acute respiratory infections in primary care: Quasi-experimental trial. J. Am. Med. Inform. Assoc. 2013, 20, 317–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann, D.; Knaus, M.; McCullagh, L.; Sofianou, A.; Rosen, L.; McGinn, T.; Kannry, J. Measures of user experience in a streptococcal pharyngitis and pneumonia clinical decision support tools. Appl. Clin. Inform. 2014, 5, 824–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCullagh, L.J.J.; Sofianou, A.; Kannry, J.; Mann, D.M.M.; McGinn, T.G.G. User centered clinical decision support tools: Adoption across clinician training level. Appl. Clin. Inform. 2014, 5, 1015–1025. [Google Scholar] [CrossRef] [Green Version]
- McCullough, J.M.; Zimmerman, F.J.; Rodriguez, H.P. Impact of clinical decision support on receipt of antibiotic prescriptions for acute bronchitis and upper respiratory tract infection. J. Am. Med. Inform. Assoc. 2014, 21, 1091–1097. [Google Scholar] [CrossRef] [Green Version]
- McDermott, L.; Yardley, L.; Little, P.; van Staa, T.; Dregan, A.; McCann, G.; Ashworth, M.; Gulliford, M. Process evaluation of a point-of-care cluster randomised trial using a computer-delivered intervention to reduce antibiotic prescribing in primary care. BMC Health Serv. Res. 2014, 14, 594. [Google Scholar] [CrossRef]
- McGinn, T.G.; McCullagh, L.; Kannry, J.; Knaus, M.; Sofianou, A.; Wisnivesky, J.P.; Mann, D.M. Efficacy of an evidence-based clinical decision support in primary care practices: A randomized clinical trial. JAMA Intern. Med. 2013, 173, 1584–1591. [Google Scholar] [CrossRef]
- Ginzburg, R.; Conway, J.J.; Waltermaurer, E.; Song, W.; Jellinek-Cohen, S.P. Using Clinical Decision Support Within the Electronic Health Record to Reduce Incorrect Prescribing for Acute Sinusitis. J. Patient-Cent. Res. Rev. 2018, 5, 196–203. [Google Scholar] [CrossRef]
- Rattinger, G.B.; Mullins, C.D.; Zuckerman, I.H.; Onukwugha, E.; Walker, L.D.; Gundlapalli, A.; Samore, M.; Delisle, S. A sustainable strategy to prevent misuse of antibiotics for acute respiratory infections. PLoS ONE 2012, 7, e51147. [Google Scholar] [CrossRef] [Green Version]
- Rubin, M.A.; Bateman, K.; Donnelly, S.; Stoddard, G.J.; Stevenson, K.; Gardner, R.M.; Samore, M.H. Use of a personal digital assistant for managing antibiotic prescribing for outpatient respiratory tract infections in rural communities. J. Am. Med. Inform. Assoc. 2006, 13, 627–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webb, B.J.; Sorensen, J.; Mecham, I.; Buckel, W.; Ooi, L.; Jephson, A.; Dean, N.C. Antibiotic Use and Outcomes after Implementation of the Drug Resistance in Pneumonia Score in ED Patients With Community-Onset Pneumonia. Chest 2019, 156, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, R.; Anderer, T.; McCulloch, C.E.; Maselli, J.H.; Bloom, F.J.J.; Graf, T.R.; Stahl, M.; Yefko, M.; Molecavage, J.; Metlay, J.P. A cluster randomized trial of decision support strategies for reducing antibiotic use in acute bronchitis. JAMA Intern. Med. 2013, 173, 267–273. [Google Scholar] [CrossRef]
- Graham, T.A.D.; Bullard, M.J.; Kushniruk, A.W.; Holroyd, B.R.; Rowe, B.H. Assessing the sensibility of two clinical decision support systems. J. Med. Syst. 2008, 32, 361–368. [Google Scholar] [CrossRef]
- Grayson, M.L.; Melvani, S.; Kirsa, S.W.; Cheung, S.; Korman, A.M.; Garrett, M.K.; Thomson, W.A. Impact of an electronic antibiotic advice and approval system on antibiotic prescribing in an Australian teaching hospital. Med. J. Aust. 2004, 180, 455–458. [Google Scholar] [CrossRef]
- Gulliford, M.C.; van Staa, T.; Dregan, A.; McDermott, L.; McCann, G.; Ashworth, M.; Charlton, J.; Little, P.; Moore, M.V.; Yardley, L. Electronic health records for intervention research: A cluster randomized trial to reduce anti biotic prescribing in primary care (eCRT study). Ann. Fam. Med. 2014, 12, 344–351. [Google Scholar] [CrossRef] [Green Version]
- Gulliford, M.C.; Prevost, A.T.; Charlton, J.; Juszczyk, D.; Soames, J.; McDermott, L.; Sultana, K.; Wright, M.; Fox, R.; Hay, A.D.; et al. Effectiveness and safety of electronically delivered prescribing feedback and decision support on antibiotic use for respiratory illness in primary care: REDUCE cluster randomised trial. BMJ 2019, 364, l236. [Google Scholar] [CrossRef] [Green Version]
- Hingorani, R.; Mahmood, M.; Alweis, R. Improving antibiotic adherence in treatment of acute upper respiratory infections: A quality improvement process. J. Community Hosp. Intern. Med. Perspect. 2015, 5, 27472. [Google Scholar] [CrossRef]
- Jones, B.E.; Haroldsen, C.; Madaras-Kelly, K.; Goetz, M.B.; Ying, J.; Sauer, B.; Jones, M.M.; Leecaster, M.; Greene, T.; Fridkin, S.K.; et al. In Data We Trust? Comparison of Electronic Versus Manual Abstraction of Antimicrobial Prescribing Quality Metrics for Hospitalized Veterans with Pneumonia. Med. Care 2018, 56, 626–633. [Google Scholar] [CrossRef]
- Holstiege, J.; Mathes, T.; Pieper, D. Effects of computer-aided clinical decision support systems in improving antibiotic prescribing by primary care providers: A systematic review. J. Am. Med. Informatics Assoc. 2015, 22, 236–242. [Google Scholar] [CrossRef]
- Baysari, M.T.; Lehnbom, E.C.; Li, L.; Hargreaves, A.; Day, R.O.; Westbrook, J.I. The effectiveness of information technology to improve antimicrobial prescribing in hospitals: A systematic review and meta-analysis. Int. J. Med. Inform. 2016, 92, 15–34. [Google Scholar] [CrossRef] [PubMed]
- Shebl, N.A.; Franklin, B.D.; Barber, N. Clinical decision support systems and antibiotic use. Pharm. World Sci. 2007, 29, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.P.; Hernandez, B.; Charani, E.; Castro-Sanchez, E.; Herrero, P.; Hayhoe, B.; Hope, W.; Georgiou, P.; Holmes, A.H. A systematic review of clinical decision support systems for antimicrobial management: Are we failing to investigate these interventions appropriately? Clin. Microbiol. Infect. 2017, 23, 524–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granja, C.; Janssen, W.; Johansen, M.A. Factors Determining the Success and Failure of eHealth Interventions: Systematic Review of the Literature. J. Med. Internet Res. 2018, 20, e10235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, A.G.; Simões, P.; Santos, R.; Queirós, A.; Rocha, N.P.; Rodrigues, M. A scale to assess the methodological quality of studies assessing usability of electronic health products and services: Delphi study followed by validity and reliability testing. J. Med. Internet Res. 2019, 21, e14829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horsky, J.; Schiff, G.D.; Johnston, D.; Mercincavage, L.; Bell, D.; Middleton, B. Interface design principles for usable decision support: A targeted review of best practices for clinical prescribing interventions. J. Biomed. Inform. 2012, 45, 1202–1216. [Google Scholar] [CrossRef] [Green Version]
- Sirajuddin, A.M.; Osheroff, J.A.; Sittig, D.F.; Chuo, J.; Velasco, F.; Collins, D.A. Implementation pearls from a new guidebook on improving medication use and outcomes with clinical decision support. Effective CDS is essential for addressing healthcare performance improvement imperatives. J. Healthc. Inf. Manag. 2009, 23, 38–45. [Google Scholar]
- Peters, D.H.; Tran, N.T.; Adam, T. Implementation Research in Health-A Practical Guide; World Health Organization: Geneva, Switzerland, 2013; ISBN 9789241506212. Available online: https://apps.who.int/iris/bitstream/handle/10665/91758/9789241506212_eng.pdf;jsessionid=8EA86C567F2C099387E235828FC55D35?sequence=1 (accessed on 3 July 2020).
- Ferri, M.; Ranucci, E.; Romagnoli, P.; Giaccone, V. Antimicrobial resistance: A global emerging threat to public health systems. Crit. Rev. Food Sci. Nutr. 2017, 57, 2857–2876. [Google Scholar] [CrossRef]

{kind=link}
| Author (Year) | Title | Study Design | Location | Setting | Disease | Study Population | Intervention |
|---|---|---|---|---|---|---|---|
| Bourgeois FC (2010) [25] | Impact of a computerized template on antibiotic prescribing for acute respiratory infections in children and adolescents. | RCT | USA | Pediatric practice | RTI | Children and Adolescents | Template for diagnosis with clinical support |
| Gifford J (2017) [26] | Decision support during electronic prescription to stem antibiotic overuse for acute respiratory infections: a long-term, quasi-experimental study. | Retrospective study | USA | Hospital care | RTI | ALL | CDSS deployed at the moment of AB prescription |
| Ginzburg R (2018) [37] | Using Clinical Decision Support Within the Electronic Health Record to Reduce Incorrect Prescribing for Acute Sinusitis. | Observational cohort | USA | Primary care clinics | Sinusitis | ALL | Best practice alert |
| Gonzales R (2013) [41] | A cluster randomized trial of decision support strategies for reducing antibiotic use in acute bronchitis. | CRCT | USA | Primary care clinics | Uncomplicated acute bronchitis | ALL | Best practice alert |
| Grayson ML (2004) [43] | Impact of an electronic antibiotic advice and approval system on antibiotic prescribing in an Australian teaching hospital. | Prospective, Non-randomized: Pre/post-study | Australia | Hospital care | CAP | ALL | Computer-generated AB approval |
| Gulliford MC (2014) [44] | Electronic health records for intervention research: a cluster randomized trial to reduce antibiotic prescribing in primary care (eCRT study). | RCT | UK | Primary care clinics | RTI | Adult | CDSS with education and decision support |
| Gulliford MC (2019) [45] | Effectiveness and safety of electronically delivered prescribing feedback and decision support on antibiotic use for respiratory illness in primary care: REDUCE cluster randomized trial. | CRCT | UK | Primary care clinics | RTI | Adult | Webinar + AB reports + Decision support tools |
| Hingorani R (2015) [46] | Improving antibiotic adherence in treatment of acute upper respiratory infections: a quality improvement process. | Prospective, Non-randomized: Pre/post-study | USA | Primary care clinics | Sinusitis, pharyngitis | ALL | Didactic teaching, AB guidelines, CDSS integrated on EHR |
| Jones BE (2018) [47] | In Data We Trust? Comparison of Electronic Versus Manual Abstraction of Antimicrobial Prescribing Quality Metrics for Hospitalized Veterans With Pneumonia. | Retrospective study | USA | Hospital care | Uncomplicated pneumonia | ALL | Electronic vs manual Medication Use Evaluation (MUE) |
| Linder J (2007) [29] | Clinical decision support to improve antibiotic prescribing for acute respiratory infections: results of a pilot study. | Prospective, Non-randomized: Pre/post-study | USA | Primary care clinics | RTI | ALL | ARI Smart Form: assistance in AB prescription for RTI visits |
| Linder JA (2006) [28] | Acute infections in primary care: accuracy of electronic diagnoses and electronic antibiotic prescribing. | Retrospective study, (double) cross-sectional | USA | Primary care clinics | RTI | ALL | Use of electronic prescribing |
| Linder JA (2009) [27] | Documentation-based clinical decision support to improve antibiotic prescribing for acute respiratory infections in primary care: a cluster randomized controlled trial. | CRCT | USA | Primary care clinics | RTI | n.m. | ARI Smart Form: assistance in AB prescription for RTI visits |
| Litvin CB (2013) [30] | Use of an electronic health record clinical decision support tool to improve antibiotic prescribing for acute respiratory infections: the ABX-TRIP study. | Prospective, Non-randomized: Pre/post study | USA | Primary care clinics | RTI | ALL | ABX-TRIP: guidelines, diagnostic criteria, AB use recommendation |
| Mainous AG (2013) [31] | Impact of a clinical decision support system on antibiotic prescribing for acute respiratory infections in primary care: quasi-experimental trial. | Prospective, Non-randomized: Pre/post-study | USA | Primary care clinics | RTI | Adult | CDSS on EHR, helps with appropriate diagnosis and AB suggestions |
| Mann D (2014) [32] | Measures of user experience in a streptococcal pharyngitis and pneumonia clinical decision support tools. | RCT | USA | Academic center | streptococcal pharyngitis and pneumonia | ALL | CDSS tool (iCPR) with Smartset (medication bundled-order set) |
| McCullagh LJ (2014) [33] | User centered clinical decision support tools: adoption across clinician training level. | RCT | USA | Academic medical institution | streptococcal pharyngitis and pneumonia | ALL | CDSS tool (iCPR) with Smartset (medication bundled-order set) |
| McCullough JM (2014) [34] | Impact of clinical decision support on receipt of antibiotic prescriptions for acute bronchitis and upper respiratory tract infection. | Retrospective study | USA | Primary care clinics | RTI | ALL | CDSS use assessment |
| McDermott L (2014) [35] | Process evaluation of a point-of-care cluster randomised trial using a computer-delivered intervention to reduce antibiotic prescribing in primary care. | Mixed methods | UK | Primary care clinics | RTI | ALL | Computer point-of-care |
| McGinn TG (2013) [36] | Efficacy of an evidence-based clinical decision support in primary care practices: a randomized clinical trial. | RCT | USA | Primary care clinics | Streptococcal pharyngitis and pneumonia. | ALL | Clinical prediction tool |
| Rattinger GB (2012) [38] | A sustainable strategy to prevent misuse of antibiotics for acute respiratory infections. | Retrospective study | USA | Hospital care | RTI | ALL | CDSS with treatment paths for fluoroquinolones and azithromycin |
| Rubin MA (2006) [39] | Use of a personal digital assistant for managing antibiotic prescribing for outpatient respiratory tract infections in rural communities. | Observational randomized study | USA | Primary care clinics | RTI | ALL | CDSS with diagnostic and therapeutic recommendation |
| Webb BJ (2019) [40] | Antibiotic Use and Outcomes After Implementation of the Drug Resistance in Pneumonia Score in ED Patients With Community-Onset Pneumonia. | Prospective, Non-randomized: Pre/post-study | USA | Hospital care | Pneumonia | Adult | DRIP score calculator |
| Author (Year) | Population (n) | Results | p-Value/CI | Observations |
|---|---|---|---|---|
| Bourgeois FC (2010) [25] | C = 12, P = 146, V = 419 | (1) Intervention group vs control group: 39.7% vs 46% prescription rate; * (2) Intervention group: with ARI-IT users vs non-ARI-IT users: 31.7% vs 39.9% prescription rate. | (1) p = 0.844; * (2) p = 0.02 | Usability: ARI-IT likely to improve efficiency |
| Ginzburg R (2018) [37] | P= 54, V = 438 | (1) Prescription reduction: 86.3% to 61.7%; (2) Incorrect prescription: 88.5% to 78.7%. | (1) p < 0.01; (2) p = 0.02 | |
| Gonzales R (2013) [41] | C = 12, P = 155, V = 12826 | Prescription reduction: 74.3% to 60.7% | p = 0.014 | |
| Gulliford MC (2014) [44] | C = 100, V = 603 409 | Prescription reduction by 9.69%. | p = 0.034 | |
| Gulliford MC (2019) [45] | C = 79 | Prescription intervention group vs control group (RR = 0.88). | CI (0.78–0.99); p = 0.040 | No effect in children < 15 years and adults > 84 years |
| Jones BE (2018) [47] | C = 30, P = 111, V = 2004 | Evaluations as excessive AB duration: mMUE = 82.3%, eMUE = 84.0% | p < 0.001 | |
| Linder J (2007) [29] | P = 10, V = 26 | Prescription reduction: Intervention group = 35% vs control group = 38%, | - | |
| Linder JA (2006) [28] | C = 9, P = 96 | AB prescription on 45% of ARI visits | - | Electronic prescription increased from 2000 (15%) to 2003 (25%) (p = 0.03), becoming non-significant after clustering by clinic (p = 0.18) or clinician (p = 0.23) |
| Linder JA (2009) [27] | C = 27, P = 443, V = 21961 | Prescription rate: Intervention group = 39% vs control group = 43% (OR = 0.8) * | CI (0.5–1.3) * | |
| Litvin CB (2013) [30] | C = 9, Ph=27, N = 6, A = 6 | (1) Inappropriate AB use: +1.57% *, (2) Broad spectrum AB use: −16.30% | (1) CI (−5.35%, 8.49%) *; (2) CI (−24.81%, −7.79%) | |
| Mainous AG (2013) [31] | C = 70 | (1) Inappropriate AB use: Intervention group vs control group: −0.6%/+4.2%/; (2) Broad-spectrum AB use: Intervention group vs control group: −16.6%/+1.2% | (1) p = 0.03; (2) p < 0.0001 | |
| Mann D (2014) [32] | P = 168, V = 586 | Reduced prescription using Smartset (OR = 0.5) | CI (0.3–0.9); p = 0.01 | Acceptance of iCRP components (diagnosis and antibiotic combination: 14%) |
| McCullagh LJ (2014) [33] | P = 168, V = 556 | Antibiotics ordered using Smartset: PGY1 = 26.4%, PGY2 = 24.3%, PGY3 = 33.1%, Attendings = 37.1% | p = 0.52 | |
| McCullough JM (2014) [34] | V = 3317 | Use of CDSS associated with a 19% lower likelihood of prescription | - | |
| McDermott L (2014) [35] | C = 100, P = 103 | System could decrease AB prescription rates | - | Useful features of CDSS |
| McGinn TG (2013) [36] | V = 984 | AB prescription: intervention group vs control group (RR = 0.74) | CI (0.60–0.92) | |
| Webb BJ (2019) [40] | V = 2169 | Broad-spectrum antibiotic use (OR = 0.62) | CI (0.39–0.98), p = 0.039 |
| Author (Year) | Population (n) | Results | p-Value/CI | Observations |
|---|---|---|---|---|
| Gifford J (2017) [26] | V = 1131 | Adjusted odds of guideline concordance vs “all other antibiotics”:
| CI Az (5.7–13.6); CI GT (9.0–66.3); CI Fl (CI 3.5–8.8) | |
| Grayson ML (2004) [43] | V = 2000 | Exact concordance/concordance in 76% of the cases | - | |
| Hingorani R (2015) [46] | Ph = 27, N = 1, V = 240 | Intervention group = 91.25% vs control group = 78.6% | p < 0.001 | Usage rate: 40.5% |
| Rattinger GB (2012) [38] | V = 3831 | Congruent prescription (RR = 2.57) | CI (1.865–3.540) | |
| Rubin MA (2006) [39] | V = 14393 | 82% adherence to CDSS, 2.7% change | p = 0.016 | Usability score of 4.6 (on a 1–5 scale) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carvalho, É.; Estrela, M.; Zapata-Cachafeiro, M.; Figueiras, A.; Roque, F.; Herdeiro, M.T. E-Health Tools to Improve Antibiotic Use and Resistances: A Systematic Review. Antibiotics 2020, 9, 505. https://doi.org/10.3390/antibiotics9080505
Carvalho É, Estrela M, Zapata-Cachafeiro M, Figueiras A, Roque F, Herdeiro MT. E-Health Tools to Improve Antibiotic Use and Resistances: A Systematic Review. Antibiotics. 2020; 9(8):505. https://doi.org/10.3390/antibiotics9080505
Chicago/Turabian StyleCarvalho, Érico, Marta Estrela, Maruxa Zapata-Cachafeiro, Adolfo Figueiras, Fátima Roque, and Maria Teresa Herdeiro. 2020. "E-Health Tools to Improve Antibiotic Use and Resistances: A Systematic Review" Antibiotics 9, no. 8: 505. https://doi.org/10.3390/antibiotics9080505