Antimicrobial Susceptibility of Neisseria gonorrhoeae Isolates in Baltimore, Maryland, 2016: The Importance of Sentinel Surveillance in the Era of Multi-Drug-Resistant Gonorrhea

Abstract
:1. Introduction
2. Methods
2.1. Clinical Isolates
2.2. Antimicrobial Susceptibility Testing
2.3. Molecular Characterization of Resistance Markers
3. Results
3.1. Isolate Characteristics and Subject Demographics
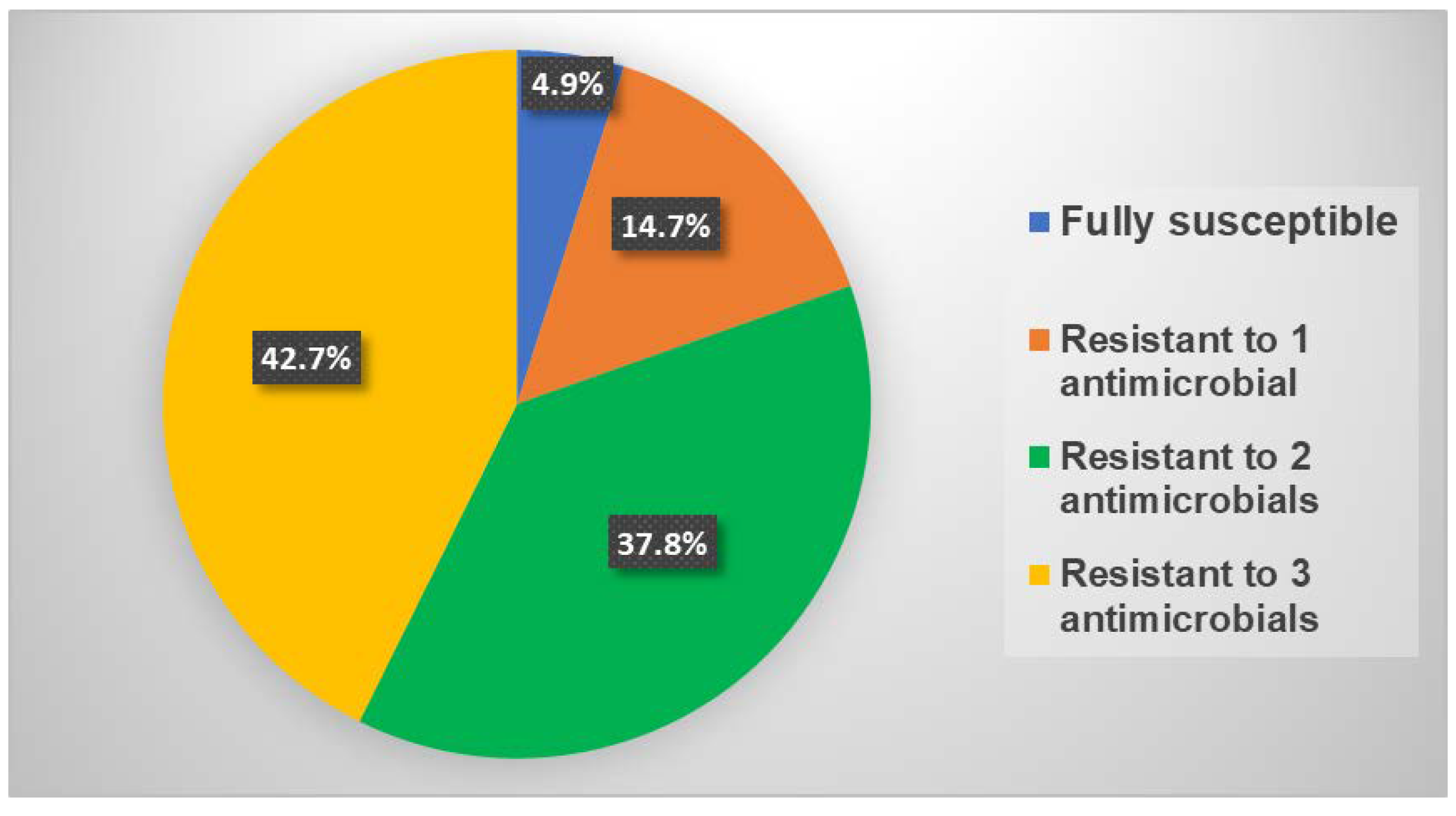
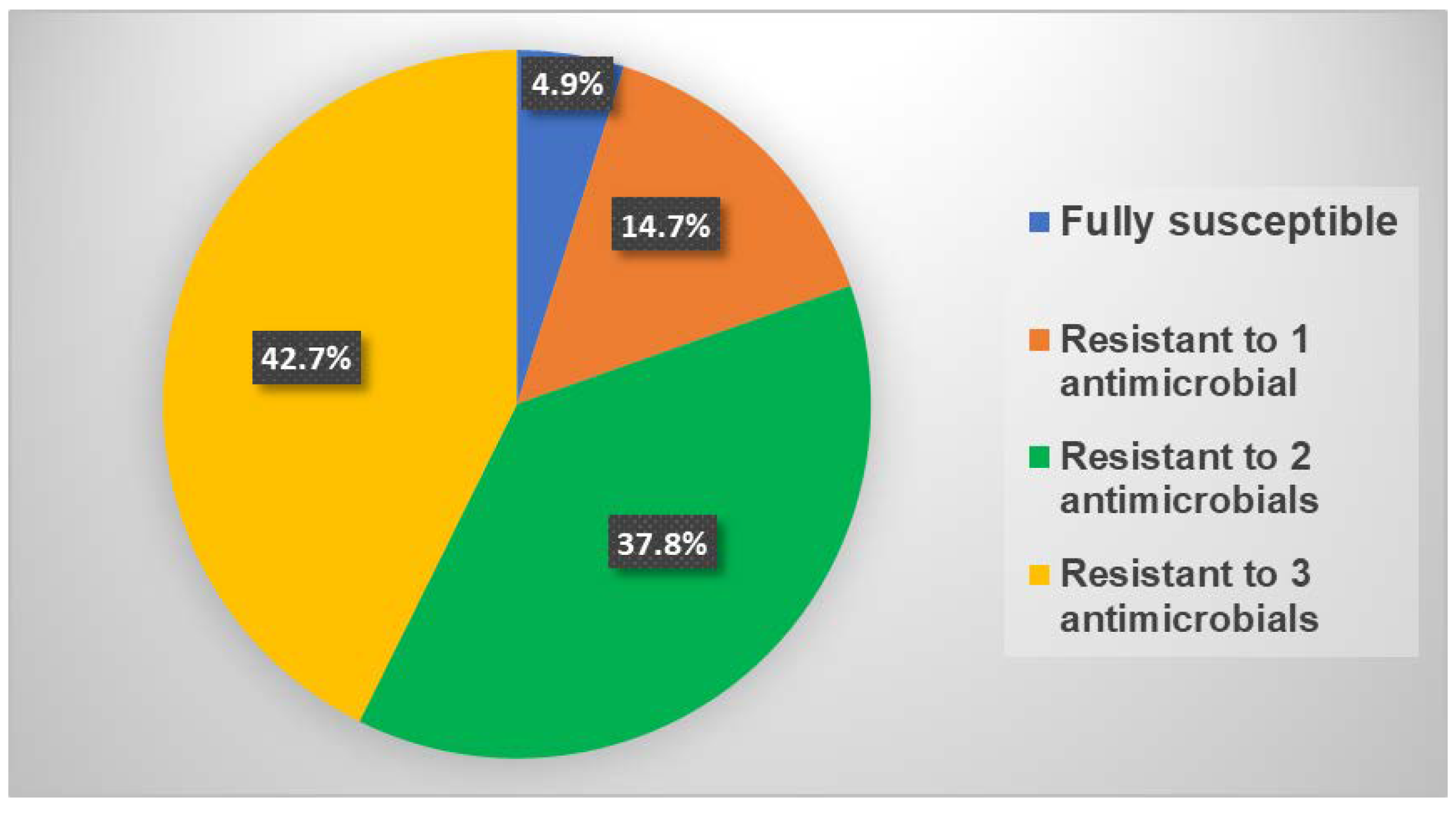
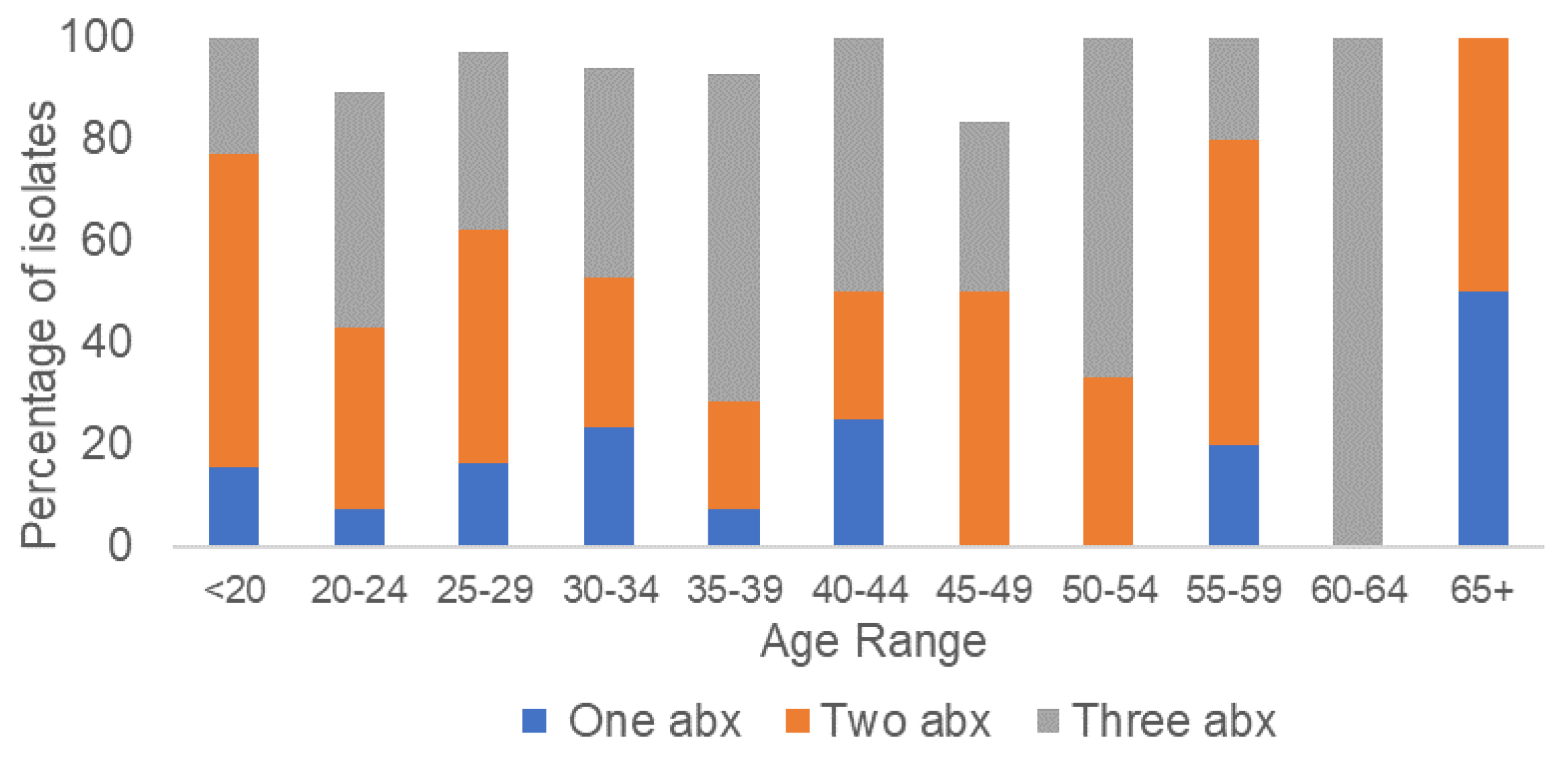
3.2. Antimicrobial Susceptibility
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Newman, L.; Rowley, J.; Vander Hoorn, S.; Wijesooriya, N.; Unemo, M.; Low, N.; Stevens, G.; Gottlieb, S.; Kiarie, J.; Temmerman, M. Global estimates of the prevalence and incidence of four curable sexually transmitted infections in 2012 based on systematic review and global reporting. PLoS ONE 2015, 10, e0143304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unemo, M.; Del Rio, C.; Shafer, W.M. Antimicrobial resistance expressed by Neisseria gonorrhoeae: A major global public health problem in the 21st century. Microbiol. Spectr. 2016, 4, 1–10. [Google Scholar]
- Workowski, K.A.; Bolan, G.A. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm. Rep. 2015, 64, 1–37. [Google Scholar] [PubMed]
- WHO Guidelines for the Treatment of Neisseria gonorrhea. Available online: http:www.who.int/reproductivehealth/publications/rtis/gonorrhoea-treatment-guidelines/en/ (accessed on 1 July 2018).
- Unemo, M.; Jensen, J.S. Antimicrobial-resistant sexually transmitted infections: Gonorrhoea and Mycoplasma genitalium. Nat. Rev. Urol. 2017, 14, 139–152. [Google Scholar] [CrossRef] [PubMed]
- Global Action Plan to Control the Spread and Impact of Antimicrobial Resistance in Neisseria gonorrhoeae. Available online: http:www.who.int/reproductivehealth/publications/rtis/9789241503501/en/ (accessed on 1 July 2018).
- Schwarcz, S.; Zenilman, J.; Schnell, D.; Knapp, J.S.; Hook, E.W., 3rd; Thompson, S.; Judson, F.N.; Holmes, K.K. National surveillance of antimicrobial resistance in Neisseria gonorrhoeae. JAMA 1990, 264, 1413–1417. [Google Scholar] [CrossRef] [PubMed]
- Kirkcaldy, R.D.; Harvey, A.; Papp, J.R.; Del Rio, C.; Soge, O.O.; Holmes, K.K.; Hook, E.W., 3rd; Kubin, G.; Riedel, S.; Zenilman, J.; et al. Neisseria gonorrhoeae Antimicrobial Susceptibility Surveillance—The Gonococcal Isolate Surveillance Project, 27 Sites, United States, 2014. MMWR Surveill. Summ. 2016, 65, 1–19. [Google Scholar] [CrossRef] [PubMed]
- STI Data & Statistics. Available online: https://phpa.health.maryland.gov/OIDPCS/CSTIP/Pages/STI-Data-Statistics.aspx (accessed on 25 June 2018).
- 2013 Sexually Transmitted Diseases Surveillance. Available online: https://www.cdc.gov/std/gisp2013/default.htm (accessed on 28 June 2018).
- Tabrizi, S.N.; Chen, S.; Tapsall, J.; Garland, S.M. Evaluation of opa-based real-time PCR for detection of Neisseria gonorrhoeae. Sex. Transm. Dis. 2005, 32, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Melendez, J.H.; Hardick, J.; Barnes, M.; Barnes, P.; Geddes, C.D.; Gaydos, C.A. Molecular characterization of markers associated with antimicrobial resistance in Neisseria gonorrhoeae identified from residual clinical samples. Sex. Transm. Dis. 2018, 45, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Wayne, P.A. Clinical and laboratory standard institute. performance standards for antimicrobial susceptibility testing. Inform. Suppl. 2011, 31, 100–121. [Google Scholar]
- Kirkcaldy, R.D.; Soge, O.O.; Papp, J.R.; Hook, E.W., 3rd; Del Rio, C.; Kubin, G.; Weinstock, H.S. Analysis of Neisseria gonorrhoeae azithromycin susceptibility in the United States by the Gonococcal Isolate Surveillance Project, 2005 to 2013. Antimicrob. Agents Chemother. 2015, 59, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.B.; Krysiak, R.; Kamanga, G.; Mapanje, C.; Kanyamula, H.; Banda, B.; Mhango, C.; Hoffman, M.; Kamwendo, D.; Hobbs, M.; et al. Neisseria gonorrhoeae antimicrobial susceptibility in Lilongwe, Malawi, 2007. Sex. Transm. Dis. 2010, 37, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Chisholm, S.A.; Quaye, N.; Cole, M.J.; Fredlund, H.; Hoffmann, S.; Jensen, J.S.; Van de Laar, M.J.; Unemo, M.; Ison, C.A. An evaluation of gentamicin susceptibility of Neisseria gonorrhoeae isolates in Europe. J. Antimicrob. Chemother. 2011, 66, 592–595. [Google Scholar] [CrossRef] [PubMed]
- Mann, L.M.; Kirkcaldy, R.D.; Papp, J.R.; Torrone, E.A. Susceptibility of Neisseria gonorrhoeae to gentamicin-gonococcal isolate surveillance project, 2015–2016. Sex. Transm. Dis. 2018, 45, 96–98. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, K.; Raymundo, L., Jr.; Drew, W.L. Chromogenic cephalosporin spot test to detect beta-lactamase in clinically significant bacteria. J. Clin. Microbiol. 1979, 9, 205–207. [Google Scholar] [PubMed]
- Giles, J.; Hardick, J.; Yuenger, J.; Dan, M.; Reich, K.; Zenilman, J. Use of applied biosystems 7900HT sequence detection system and TaqMan assay for detection of quinolone-resistant Neisseria gonorrhoeae. J. Clin. Microbiol. 2004, 42, 3281–3283. [Google Scholar] [CrossRef] [PubMed]
- Goire, N.; Freeman, K.; Tapsall, J.W.; Lambert, S.B.; Nissen, M.D.; Sloots, T.P.; Whiley, D.M. Enhancing gonococcal antimicrobial resistance surveillance: A real-time PCR assay for detection of penicillinase-producing Neisseria gonorrhoeae by use of non-cultured clinical samples. J. Clin. Microbiol. 2011, 49, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Cole, M.J.; Spiteri, G.; Jacobsson, S.; Woodford, N.; Tripodo, F.; Amato-Gauci, A.J.; Unemo, M.; Euro-GASP Network. Overall low extended-spectrum cephalosporin resistance but high azithromycin resistance in Neisseria gonorrhoeae in 24 European countries, 2015. BMC Infect. Dis. 2017, 17. [Google Scholar] [CrossRef] [PubMed]
- Unemo, M.; Workowski, K. Dual antimicrobial therapy for gonorrhea: what is the role of azithromycin? Lancet Infect. Dis. 2018, 18, 486–488. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Update to CDC’s sexually transmitted diseases treatment guidelines, 2006: Fluoroquinolones no longer recommended for treatment of gonococcal infections. MMWR Morb. Mortal. Wkly. Rep. 2007, 56, 332–336. [Google Scholar]
- Allan-Blitz, L.T.; Humphries, R.M.; Hemarajata, P.; Bhatti, A.; Pandori, M.W.; Siedner, M.J.; Klausner, J.D. Implementation of a rapid genotypic assay to promote targeted ciprofloxacin therapy of Neisseria gonorrhoeae in a large health system. Clin. Infect. Dis. 2017, 64, 1268–1270. [Google Scholar] [CrossRef] [PubMed]
- Allan-Blitz, L.T.; Hemarajata, P.; Humphries, R.M.; Kimble, M.; Elias, S.; Klausner, J.D. Ciprofloxacin may be efficacious in treating wild-type Gyrase A genotype Neisseria gonorrhoeae infections. Sex. Transm. Dis. 2018, 45. [Google Scholar] [CrossRef] [PubMed]
- Bazzo, M.L.; Golfetto, L.; Gaspar, P.C.; Pires, A.F.; Ramos, M.C.; Franchimi, M.; Ferreira, W.A.; Unemo, M.; Benzaken, A.S.; Brazilian-GAPS Network. First nationwide antimicrobial susceptibility surveillance for Neisseria gonorrhoeae in Brazil, 2015–16. J. Antimicrob. Chemother. 2018, 73, 1854–1861. [Google Scholar] [CrossRef] [PubMed]
- Dowell, D.; Kirkcaldy, R.D.E. Effectiveness of gentamicin for gonorrhea treatment systematic review and meta-analysis. Sex. Transm. Infect. 2012, 88, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Kirkcaldy, R.D.; Weinstock, H.S.; Moore, P.C.; Philip, S.S.; Wiesenfeld, H.C.; Papp, J.R.; Kerndt, P.R.; Johnson, S.; Ghanem, K.G.; Hook, E.W., 3rd. The efficacy and safety of gentamicin plus azithromycin and gemifloxacin plus azithromycin as treatment of uncomplicated gonorrhea. Clin. Infect. Dis. 2014, 59, 1083–1091. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Antibiotics | MIC Breakpoint (µg/mL) a | Number of Isolates (%) | ||||
|---|---|---|---|---|---|---|
| S | I | R | S | I | R | |
| Ciprofloxacin | ≤0.06 | 0.125–0.5 | ≥1 | 79 (55.2) | 1 (0.7) | 63 (44.1) |
| Penicillin | ≤0.06 | 0.12–1 | ≥2 | 19 (13.3) | 92 (64.3) | 32 (22.4) |
| Tetracycline | ≤0.25 | 0.5–1 | ≥2 | 24 (16.8) | 104 (72.7) | 15 (10.5) |
| Azithromycin | ≤1 | ≥2 | 140 (97.9) | 3 (2.1) | ||
| Ceftriaxone | ≤0.25 | 143 (100) | ||||
| Gentamicin | ≤4 | 8–16 | ≥32 | 143 (100) | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melendez, J.H.; Hardick, J.; Barnes, M.; Page, K.R.; Gaydos, C.A. Antimicrobial Susceptibility of Neisseria gonorrhoeae Isolates in Baltimore, Maryland, 2016: The Importance of Sentinel Surveillance in the Era of Multi-Drug-Resistant Gonorrhea. Antibiotics 2018, 7, 77. https://doi.org/10.3390/antibiotics7030077
Melendez JH, Hardick J, Barnes M, Page KR, Gaydos CA. Antimicrobial Susceptibility of Neisseria gonorrhoeae Isolates in Baltimore, Maryland, 2016: The Importance of Sentinel Surveillance in the Era of Multi-Drug-Resistant Gonorrhea. Antibiotics. 2018; 7(3):77. https://doi.org/10.3390/antibiotics7030077
Chicago/Turabian StyleMelendez, Johan H., Justin Hardick, Mathilda Barnes, Kathleen R. Page, and Charlotte A. Gaydos. 2018. "Antimicrobial Susceptibility of Neisseria gonorrhoeae Isolates in Baltimore, Maryland, 2016: The Importance of Sentinel Surveillance in the Era of Multi-Drug-Resistant Gonorrhea" Antibiotics 7, no. 3: 77. https://doi.org/10.3390/antibiotics7030077
APA StyleMelendez, J. H., Hardick, J., Barnes, M., Page, K. R., & Gaydos, C. A. (2018). Antimicrobial Susceptibility of Neisseria gonorrhoeae Isolates in Baltimore, Maryland, 2016: The Importance of Sentinel Surveillance in the Era of Multi-Drug-Resistant Gonorrhea. Antibiotics, 7(3), 77. https://doi.org/10.3390/antibiotics7030077