
Microbiology of Prosthetic Joint Infections: A Retrospective Study of an Italian Orthopaedic Hospital
 ,
,
Abstract
:1. Introduction
2. Results
- MSSA (Methicillin-susceptible Staphylococcus aureus) + Enterococcus faecalis
- MSSA + Enterococcus faecalis
- MRSE (Methicillin-resistant Staphylococcus epidermidis) + Finegoldia magna
- MRSE + Finegoldia magna
- MRSE + MSSE (Methicillin-susceptible Staphylococcus epidermidis)
- MRSE + S. warneri
- MRSE + S. lugdunensis
- Streptococcus mitis + Cutibacterium acnes
- Corynebacterium amycolatum + Corynebacterium jeikeium + Morganella morganii
- MRSE + Cutibacterium acnes
- MRSA (Methicillin-resistant Staphylococcus aureus) + Staphylococcus saprophyticus
- MSSA + MRSE
- MRSE + Staphylococcus lugdunensis
- MSSA + Staphylococcus capitis
3. Discussion
- false negative cultures
- diagnostic delays
- treatment delays
- patients undergoing surgery close to the time limits of the study (PJIs occurring on prostheses implanted before 2017 and possible PJIs manifested in 2022)
- incorrect/different ICD-9 encoding in surgery records
- PJIs treated in other hospitals
- possible deaths due to PJI
4. Materials and Methods
4.1. Setting
4.2. Selection Criteria
- Patients who underwent both
- hip, knee, or shoulder arthroplasty
- a second surgical procedure for diagnosed or suspected PJI or other prosthetic joint-related complications where intraoperative cultures were collected
- 2.
- Both procedures were performed at the Galeazzi Orthopaedic Institute
- 3.
- Both procedures were performed between 01/01/17 and 31/12/21
- (1)
- hip, knee, or shoulder arthroplasty (ICD-9 81.51, 81.54, 81.80)
- (2)
- Any surgery related to the diagnosis of infection or other complications related to joint replacements (ICD-9 966.66, 966.67, 966.77)
- Revision surgeries not related to PJI (e.g., aseptic loosening confirmed by negative intraoperative cultures)
- PJI occurring more than 1 year after the index surgery
- Patients undergoing the two surgical procedures at different joints
- For the purposes of our study, we have classified PJI by onset, as follows:
- Early: less than 4 weeks from surgery
- Delayed: between 4 weeks and 1 year
- Late: more than 1 year (excluded from the study)
4.3. Microbiological Testing
4.4. Pathogens and Resistance Profiles
- -
- resistance to oxacilline in Staphilococcus spp.
- -
- resistance to penicillin in Streptoccus spp.
- -
- resistance to cefotaxime in E. coli and P. mirabilis
5. Conclusions
- -
- a predominance of staphylococcal infections and, in general, a predominance of gram+ over gram−
- -
- a percentage of MRSA lower than the Italian average and similar to the European one
- -
- a high percentage of MRSEs, which exhibit high rates of resistance to other classes of antibiotics, as already highlighted in the literature
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aboltins, C.A.; Berdal, J.E.; Casas, F.; Corona, P.S.; Cuellar, D.; Ferrari, M.C.; Hendershot, E.; Huang, W.; Kuo, F.C.; Malkani, A.; et al. Hip and Knee Section, Prevention, Antimicrobials (Systemic): Proceedings of International Consensus on Orthopedic Infections. J. Arthroplasty 2019, 34, S279–S288. [Google Scholar] [CrossRef]
- Engesæter, L.B.; Lie, S.A.; Espehaug, B.; Furnes, O.; Vollset, S.E.; Havelin, L.I. Antibiotic Prophylaxis in Total Hip Arthroplasty: Effects of Antibiotic Prophylaxis Systemically and in Bone Cement on the Revision Rate of 22,170 Primary Hip Replacements Followed 0-14 Years in the Norwegian Arthroplasty Register. Acta Orthop. Scand. 2003, 74, 644–651. [Google Scholar] [CrossRef]
- Steinberg, J.P.; Braun, B.I.; Hellinger, W.C.; Kusek, L.; Bozikis, M.R.; Bush, A.J.; Dellinger, E.P.; Burke, J.P.; Simmons, B.; Kritchevsky, S.B.; et al. Timing of Antimicrobial Prophylaxis and the Risk of Surgical Site Infections: Results from the Trial to Reduce Antimicrobial Prophylaxis Errors. Ann. Surg. 2009, 250, 10–16. [Google Scholar] [CrossRef]
- Natsuhara, K.M.; Shelton, T.J.; Meehan, J.P.; Lum, Z.C. Mortality during Total Hip Periprosthetic Joint Infection. J. Arthroplasty 2019, 34, S337–S342. [Google Scholar] [CrossRef]
- Tande, A.J.; Patel, R. Prosthetic Joint Infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplasty 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef]
- Sia, I.G.; Berbari, E.F.; Karchmer, A.W. Prosthetic Joint Infections. Infect. Dis. Clin. N. Am. 2005, 19, 885–914. [Google Scholar] [CrossRef]
- Pellegrini, A.; Suardi, V.; Legnani, C. Classification and Management Options for Prosthetic Joint Infection. Ann. Jt. 2022, 7. [Google Scholar] [CrossRef]
- Zimmerli, W.; Lew, P.D.; Waldvogel, F.A. Pathogenesis of Foreign Body Infection. Evidence for a Local Granulocyte Defect. J. Clin. Investig. 1984, 73, 1191–1200. [Google Scholar] [CrossRef]
- Zimmerli, W.; Waldvoge, F.A.; Vaudaux, P.; Nydegger, D.E. Pathogenesis of Foreign Body Infection: Description and Characteristics of an Animal Model. J. Infect. Dis. 1982, 146, 487–497. [Google Scholar] [CrossRef]
- Gupta, P.; Sarkar, S.; Das, B.; Bhattacharjee, S.; Tribedi, P. Biofilm, Pathogenesis and Prevention—A Journey to Break the Wall: A Review. Arch. Microbiol. 2016, 198, 1–15. [Google Scholar] [CrossRef]
- Lu, T.K.; Collins, J.J. Dispersing Biofilms with Engineered Enzymatic Bacteriophage. Proc. Natl. Acad. Sci. USA 2007, 104, 11197–11202. [Google Scholar] [CrossRef]
- Flemming, H.C.; Wingender, J. The Biofilm Matrix. Nat. Rev. Microbiol. 2010, 8, 623–633. [Google Scholar] [CrossRef]
- Otto, M. Staphylococcal Infections: Mechanisms of Biofilm Maturation and Detachment as Critical Determinants of Pathogenicity. Annu. Rev. Med. 2013, 64, 175–188. [Google Scholar] [CrossRef]
- Rabin, N.; Zheng, Y.; Opoku-Temeng, C.; Du, Y.; Bonsu, E.; Sintim, H.O. Biofilm Formation Mechanisms and Targets for Developing Antibiofilm Agents. Future Med. Chem. 2015, 7, 493–512. [Google Scholar] [CrossRef]
- Costerton, J.W.; Stewart, P.S.; Greenberg, E.P. Bacterial Biofilms: A Common Cause of Persistent Infections. Science 1999, 284, 1318–1322. [Google Scholar] [CrossRef]
- McDougald, D.; Rice, S.A.; Barraud, N.; Steinberg, P.D.; Kjelleberg, S. Should We Stay or Should We Go: Mechanisms and Ecological Consequences for Biofilm Dispersal. Nat. Rev. Microbiol. 2011, 10, 39–50. [Google Scholar] [CrossRef]
- Sambri, A.; Fiore, M.; Tedeschi, S.; De Paolis, M. The Need for Multidisciplinarity in Modern Medicine: An Insight into Orthopaedic Infections. Microorganisms 2022, 10, 756. [Google Scholar] [CrossRef]
- Southwood, R.T.; Rice, J.L.; McDonald, P.J.; Hakendorf, P.H.; Rozenbilds, M.A. Infection in Experimental Hip Arthroplasties. J. Bone Joint Surg. Br. 1985, 67, 229–231. [Google Scholar] [CrossRef]
- Linea Guida SIOT: Prevenzione Delle Infezioni in Chirurgia Ortopedica. 2021. Available online: https://siot.it/wp-content/uploads/2021/06/LG-366-SIOT-Prevenzione-delle-infezioni-in-chirurgia-ortopedica.pdf (accessed on 4 March 2024).
- Diagnosis and Prevention of Periprosthetic Joint Infections Evidence-Based Clinical Practice Guideline. Available online: https://www.aaos.org/globalassets/quality-and-practice-resources/pji/pji-clinical-practice-guideline-final-2-17-21.pdf (accessed on 11 April 2024).
- ECDC. Antimicrobial Resistance Surveillance in Europe 2016. 2017. Available online: https://www.ecdc.europa.eu/en/publications-data/antimicrobial-resistance-surveillance-europe-2016 (accessed on 11 April 2024).
- Mussa, M.; Manciulli, T.; Corbella, M.; Mariani, B.; Cambieri, P.; Gipsz, N.; Scudeller, L.; Abbott, D.M.; Brunetti, E.; Mosconi, M.; et al. Epidemiology and Microbiology of Prosthetic Joint Infections: A Nine-Year, Single-Center Experience in Pavia, Northern Italy. Musculoskelet. Surg. 2021, 105, 195–200. [Google Scholar] [CrossRef]
- Thabit, A.K.; Fatani, D.F.; Bamakhrama, M.S.; Barnawi, O.A.; Basudan, L.O.; Alhejaili, S.F. Antibiotic Penetration into Bone and Joints: An Updated Review. Int. J. Infect. Dis. 2019, 81, 128–136. [Google Scholar] [CrossRef]
- Drago, L.; de Vecchi, E.; Bortolin, M.; Zagra, L.; Romanò, C.L.; Cappelletti, L. Epidemiology and Antibiotic Resistance of Late Prosthetic Knee and Hip Infections. J. Arthroplasty 2017, 32, 2496–2500. [Google Scholar] [CrossRef]
- Montanaro, L.; Speziale, P.; Campoccia, D.; Ravaioli, S.; Cangini, I.; Pietrocola, G.; Giannini, S.; Arciola, C.R. Scenery of Staphylococcus Implant Infections in Orthopedics. Future Microbiol. 2011, 6, 1329–1349. [Google Scholar] [CrossRef]
- Carrega, G.; Bartolacci, V.; Burastero, G.; Casalino-Finocchio, G.; Grappiolo, G.; Salomone, C.; Sandrone, C.; Santoriello, L.; Riccio, G. Etiology of Prosthetic Joint Infections in a Tertiary Care Centre in Italy. Infez. Med. 2008, 16, 204–208. [Google Scholar]
- ECDC. Antimicrobial Resistance Surveillance in Europe 2017. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2017 (accessed on 11 April 2024).
- Nelson, G.N.; Davis, D.E.; Namdari, S. Outcomes in the Treatment of Periprosthetic Joint Infection after Shoulder Arthroplasty: A Systematic Review. J. Shoulder Elbow Surg. 2016, 25, 1337–1345. [Google Scholar] [CrossRef]
- Drago, L.; de Vecchi, E.; Cappelletti, L.; Mattina, R.; Vassena, C.; Romanò, C.L. Role and Antimicrobial Resistance of Staphylococci Involved in Prosthetic Joint Infections. Int. J. Artif. Organs 2014, 37, 414–421. [Google Scholar] [CrossRef]
- Hellmark, B.; Unemo, M.; Nilsdotter-augustinsson, Å.; Söderquist, B. Antibiotic Susceptibility among Staphylococcus Epidermidis Isolated from Prosthetic Joint Infections with Special Focus on Rifampicin and Variability of the RpoB Gene. Clin. Microbiol. Infect. 2009, 15, 238–244. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Adam, H.J.; Baxter, M.R.; Fuller, J.; Nichol, K.A.; Denisuik, A.J.; Lagacé-Wiens, P.R.S.; Walkty, A.; Karlowsky, J.A.; Schweizer, F.; et al. Antimicrobial Susceptibility of 22746 Pathogens from Canadian Hospitals: Results of the CANWARD 2007-11 Study. J. Antimicrob. Chemother. 2013, 68 (Suppl. S1), i7–i22. [Google Scholar] [CrossRef]
- Becker, K.; Heilmann, C.; Peters, G. Coagulase-Negative Staphylococci. Clin. Microbiol. Rev. 2014, 27, 870–926. [Google Scholar] [CrossRef]
- Landersdorfer, C.B.; Bulitta, J.B.; Kinzig, M.; Holzgrabe, U.; Sörgel, F. Penetration of Antibacterials into Bone: Pharmacokinetic, Pharmacodynamic and Bioanalytical Considerations. Clin. Pharmacokinet. 2009, 48, 89–124. [Google Scholar] [CrossRef]
- Niska, J.A.; Shahbazian, J.H.; Ramos, R.I.; Francis, K.P.; Bernthal, N.M.; Miller, L.S. Vancomycin-Rifampin Combination Therapy Has Enhanced Efficacy against an Experimental Staphylococcus Aureus Prosthetic Joint Infection. Antimicrob. Agents Chemother. 2013, 57, 5080–5086. [Google Scholar] [CrossRef] [PubMed]
- Mini, E.; Nobili, S.; Periti, P. Methicillin-Resistant Staphylococci in Clean Surgery. Is There a Role for Prophylaxis? Drugs 1997, 54 (Suppl. S6), 39–52. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing Breakpoint Tables for Interpretation of MICs and Zone Diameters Version 12.0, Valid from 2022-01-01.
- Villa, J.M.; Pannu, T.S.; Riesgo, A.M.; Patel, P.D.; Mont, M.A.; Higuera-Rueda, C.A. Dual Antibiotic Prophylaxis in Total Knee Arthroplasty: Where Do We Stand? J. Knee Surg. 2020, 33, 100–105. [Google Scholar] [CrossRef]
- Peel, T.N.; Astbury, S.; Cheng, A.C.; Paterson, D.L.; Buising, K.L.; Spelman, T.; Tran-Duy, A.; Adie, S.; Boyce, G.; McDougall, C.; et al. Trial of Vancomycin and Cefazolin as Surgical Prophylaxis in Arthroplasty. N. Engl. J. Med. 2023, 389, 1488–1498. [Google Scholar] [CrossRef] [PubMed]
- Branch-Elliman, W.; Ripollone, J.E.; O’Brien, W.J.; Itani, K.M.F.; Schweizer, M.L.; Perencevich, E.; Strymish, J.; Gupta, K. Risk of Surgical Site Infection, Acute Kidney Injury, and Clostridium Difficile Infection Following Antibiotic Prophylaxis with Vancomycin plus a Beta-Lactam versus Either Drug Alone: A National Propensity-Score-Adjusted Retrospective Cohort Study. PLoS Med. 2017, 14, e1002340. [Google Scholar] [CrossRef] [PubMed]
- Tsukayama, D.T.; Goldberg, V.M.; Kyle, R. Diagnosis and Management of Infection after Total Knee Arthroplasty. J. Bone Joint Surg. Am. 2003, 85 (Suppl. S1), 75–80. [Google Scholar] [CrossRef] [PubMed]
- De Vecchi, E.; Bottagisio, M.; Bortolin, M.; Toscano, M.; Lovati, A.B.; Drago, L. Improving the Bacterial Recovery by Using Dithiothreitol with Aerobic and Anaerobic Broth in Biofilm-Related Prosthetic and Joint Infections. Adv. Exp. Med. Biol. 2017, 973, 31–39. [Google Scholar] [CrossRef]
- De Vecchi, E.; Bortolin, M.; Signori, V.; Romanò, C.L.; Drago, L. Treatment With Dithiothreitol Improves Bacterial Recovery From Tissue Samples in Osteoarticular and Joint Infections. J. Arthroplasty 2016, 31, 2867–2870. [Google Scholar] [CrossRef]
- Gilbert, D.N.; Chambers, H.F.; Saag, M.S.; Pavia, A.; Boucher, H.W.; Black, D.; Schwartz, B.S.; Freedman, D.O.; Kim, K. The Sanford Guide to Antimicrobial Therapy; Antimicrobial Therapy, Inc.: Sperryville, VA, USA, 2021; p. 308. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Total | Early | Delayed | Hip and Knee | Shoulder | ||
|---|---|---|---|---|---|---|
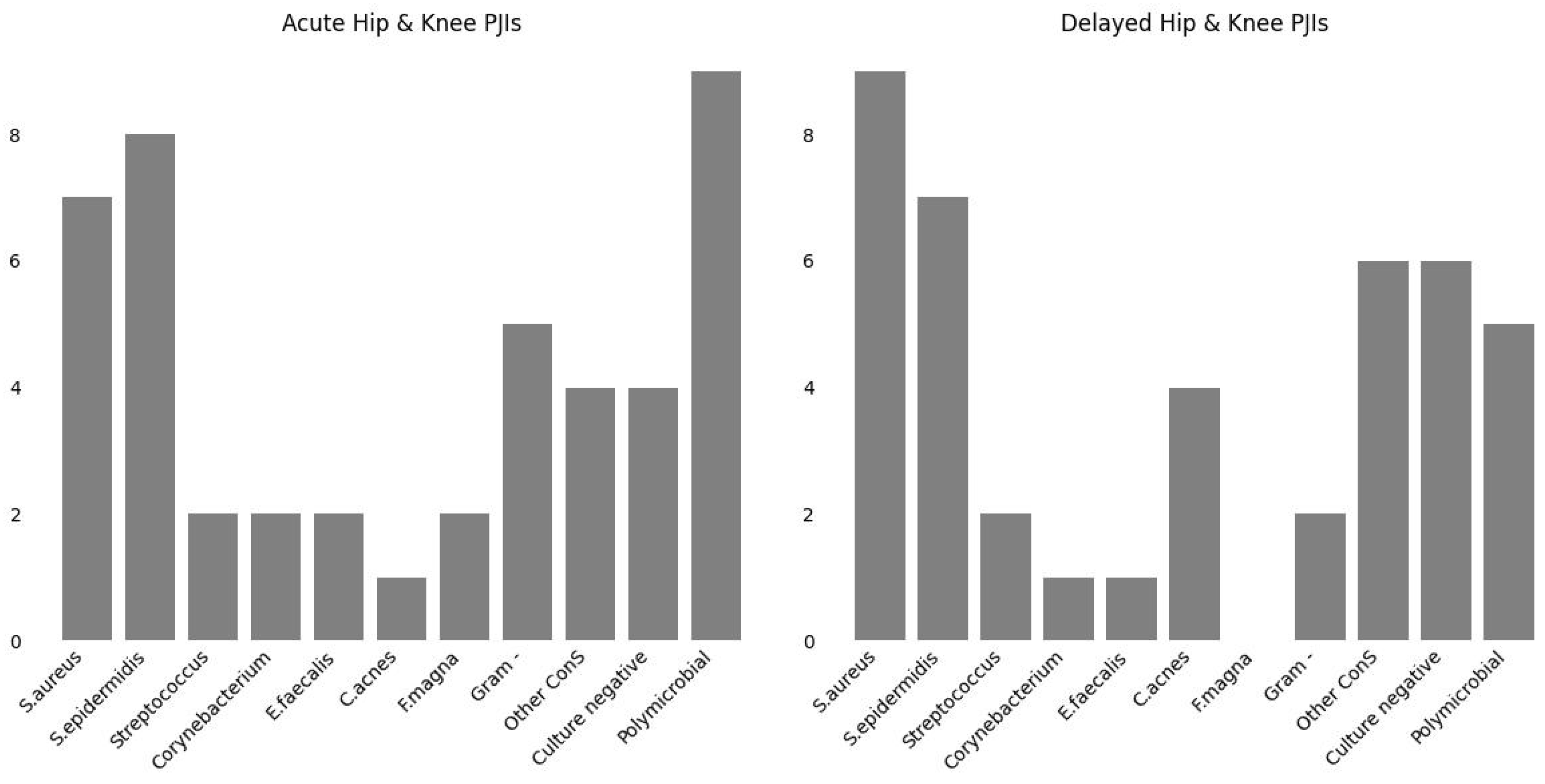
| Gram+ | S. aureus | 16 | 7 | 9 | 15 | 1 |
| S. epidermidis | 15 | 8 | 7 | 13 | 2 | |
| S. lugdunensis | 6 | 3 | 3 | 6 | ||
| S. saprophyticus | 1 | 1 | 1 | |||
| S. capitis | 1 | 1 | 1 | |||
| S. caprae | 1 | 1 | 1 | |||
| S. warneri | 1 | 1 | 1 | |||
| S. pneumoniae | 1 | 1 | 1 | |||
| S. mitis | 1 | 1 | 1 | |||
| S. agalactiae | 1 | 1 | 1 | |||
| S. equisimilis | 1 | 1 | 1 | |||
| C. amycolatum | 1 | 1 | 1 | |||
| C. jeikeium | 1 | 1 | 1 | |||
| C. striatum | 1 | 1 | 1 | |||
| E. faecalis | 3 | 2 | 1 | 3 | ||
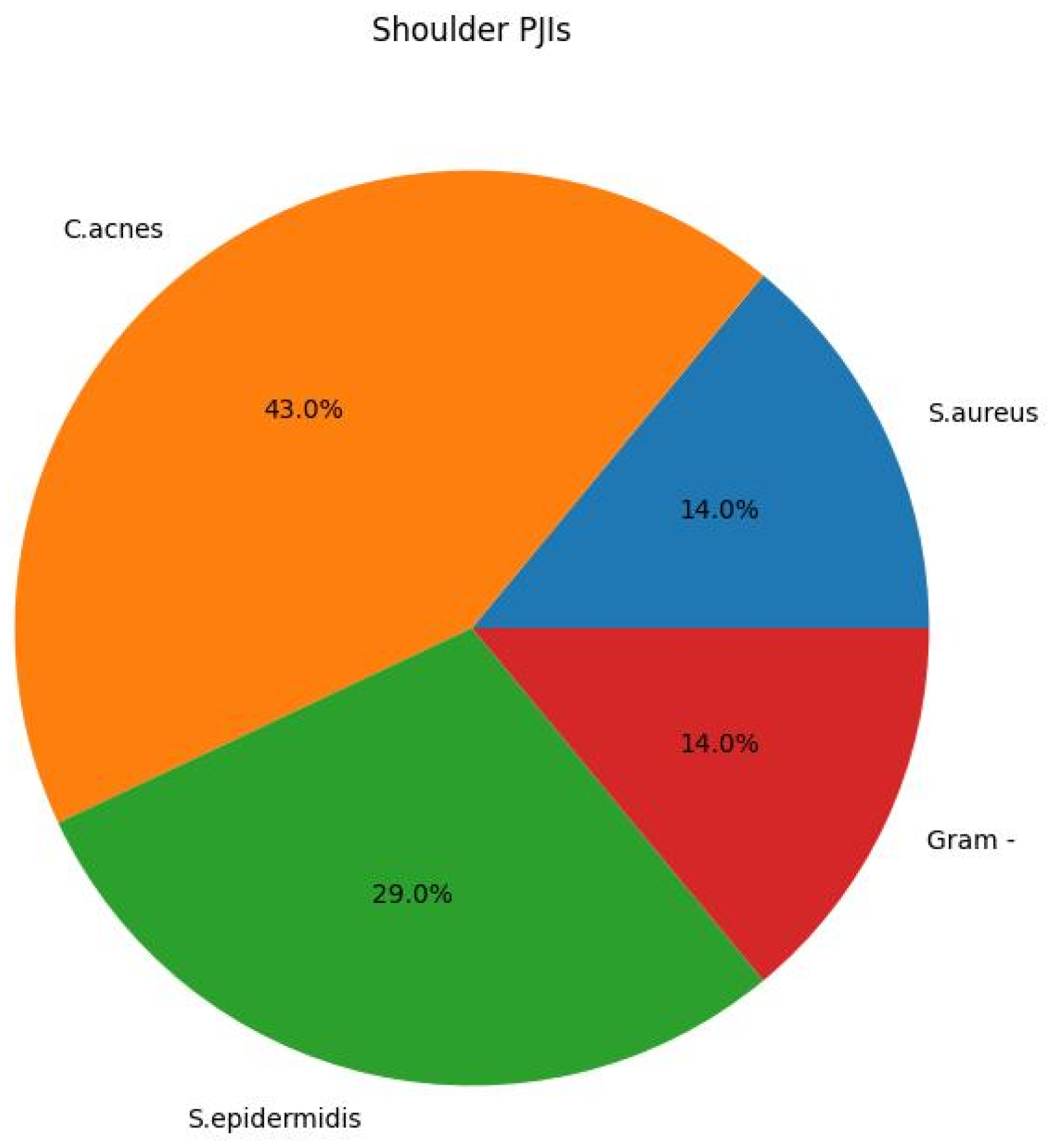
| C. acnes | 5 | 1 | 4 | 2 | 3 | |
| F. magna | 2 | 2 | 2 | |||
| Gram− | E. cloacae | 2 | 1 | 1 | 1 | 1 |
| P. mirabilis | 2 | 2 | 2 | |||
| E. coli | 1 | 1 | 1 | |||
| P. aeruginosa | 1 | 1 | 1 | |||
| M. morganii | 1 | 1 | 1 | |||
| Total | 65 | 33 | 32 | 58 | 7 |
| Antibiotic | S. aureus | S. epidermidis | Others CoNS |
|---|---|---|---|
| Oxacillin | 3/16 | 13/15 | 3/10 |
| Levofloxacin | 2/16 | 9/15 | 1/10 |
| Daptomycin | 0/16 | 2/15 | 0/10 |
| Rifampicin | 1/16 | 3/15 | 0/10 |
| Vancomycin | 0/16 | 0/15 | 0/10 |
| Teicoplanin | 0/16 | 0/15 | 0/10 |
| Tetracycline | 0/16 | 9/15 | 0/10 |
| Linezolid | 0/16 | 0/15 | 0/10 |
| Gentamicin | 1/16 | 7/15 | 1/10 |
| Cotrimoxazole | 0/16 | 5/15 | 0/10 |
| Clindamycin | 3/16 | 8/15 | 2/10 |
| Cefazolin | 3/16 | 13/15 | 3/10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suardi, V.; Baroni, D.; Shahein, A.H.A.; Morena, V.; Logoluso, N.; Mangiavini, L.; Pellegrini, A.V. Microbiology of Prosthetic Joint Infections: A Retrospective Study of an Italian Orthopaedic Hospital. Antibiotics 2024, 13, 399. https://doi.org/10.3390/antibiotics13050399
Suardi V, Baroni D, Shahein AHA, Morena V, Logoluso N, Mangiavini L, Pellegrini AV. Microbiology of Prosthetic Joint Infections: A Retrospective Study of an Italian Orthopaedic Hospital. Antibiotics. 2024; 13(5):399. https://doi.org/10.3390/antibiotics13050399
Chicago/Turabian StyleSuardi, Virginia, Daniele Baroni, Abdelrahman Hosni Abdelhamid Shahein, Valentina Morena, Nicola Logoluso, Laura Mangiavini, and Antonio Virgilio Pellegrini. 2024. "Microbiology of Prosthetic Joint Infections: A Retrospective Study of an Italian Orthopaedic Hospital" Antibiotics 13, no. 5: 399. https://doi.org/10.3390/antibiotics13050399