
2015 versus 2021: Self-Reported Preparedness to Prescribe Antibiotics Prudently among Final Year Medical Students in Sweden

 , and
, and
Abstract
:1. Introduction
1.1. Antimicrobial Stewardship in Sweden
1.2. Aim
2. Results
2.1. Participation
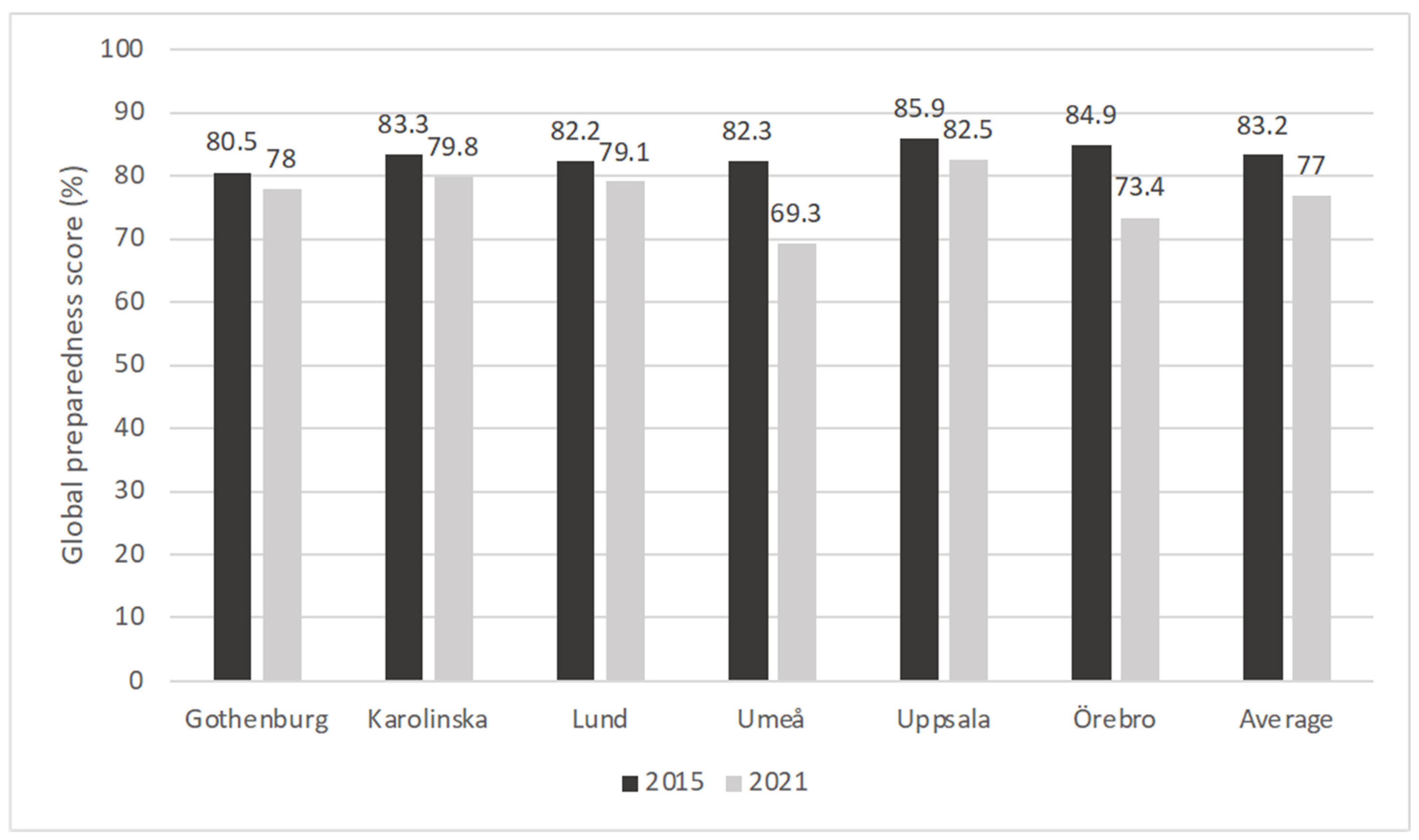
2.2. Global Preparedness Scores
2.3. Topic Preparedness Scores
2.4. Expressed Need for Further Education
2.5. Impacts of COVID-19 on Education
2.6. Perceived Usefulness of Teaching Methods
3. Discussion
3.1. Overall Preparedness Levels and Needs for Further Education
3.2. Consistency in Relative Topic Preparedness Scores and Teaching Methods
3.3. Variations between and within Medical Schools
3.4. Methodological Considerations
4. Materials and Methods
4.1. Study Design
4.2. Medical Schools in Sweden
4.3. Survey Development
4.4. Survey Distribution and Participants
4.5. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maxwell, S.R.; Cascorbi, I.; Orme, M.; Webb, D.J. Educating European (junior) doctors for safe prescribing. Basic Clin. Pharmacol. Toxicol. 2007, 101, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Brinkman, D.J.; Tichelaar, J.; Schutte, T.; Benemei, S.; Böttiger, Y.; Chamontin, B.; Christiaens, T.; Likic, R.; Maˇiulaitis, R.; Marandi, T.; et al. Essential competencies in prescribing: A first European cross-sectional study among 895 final-year medical students. Clin. Pharmacol. Ther. 2017, 101, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Brinkman, D.J.; Tichelaar, J.; Graaf, S.; Otten, R.H.J.; Richir, M.C.; van Agtmael, M.A. Do final-year medical students have sufficient prescribing competencies? A systematic literature review. Br. J. Clin. Pharmacol. 2018, 84, 615–635. [Google Scholar] [CrossRef]
- Dyar, O.J.; Nathwani, D.; Monnet, D.L.; Gyssens, I.C.; Stålsby Lundborg, C.; Pulcini, C.; Wechsler-Fördös, A.; Kostyanev, T.; Vlahović-Palčevski, V.; Kolar, M.; et al. Do medical students feel prepared to prescribe antibiotics responsibly? Results from a cross-sectional survey in 29 European countries. J. Antimicrob. Chemother. 2018, 73, 2236–2242. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Lago, J.M.; Montes-Villalba, R.A.; Vázquez-Cancela, O.; Otero-Santiago, M.; López-Durán, A.; Figueiras, A. Knowledge, Perceptions, and Perspectives of Medical Students Regarding the Use of Antibiotics and Antibiotic Resistance: A Qualitative Research in Galicia, Spain. Antibiotics 2023, 12, 558. [Google Scholar] [CrossRef] [PubMed]
- Palčevski, D.; Belančić, A.; Mikuličić, I.; Oštarijaš, E.; Likić, R.; Dyar, O.; Vlahović-Palčevski, V. Antimicrobial Prescribing Preparedness of Croatian Medical Students—Did It Change between 2015 and 2019? Medicines 2023, 10, 39. [Google Scholar] [CrossRef]
- Ferri, M.; Ranucci, E.; Romagnoli, P.; Giaccone, V. Antimicrobial resistance: A global emerging threat to public health systems. Crit. Rev. Food Sci. Nutr. 2017, 57, 2857–2876. [Google Scholar] [CrossRef]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, C.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial Consumption in the EU/EEA (ESAC-Net)—Annual Epidemiological Report for 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobialconsumption-europe-2021 (accessed on 12 February 2024).
- 2022 WHO Regional Office for Europe/European Centre for Disease Prevention and Control. Antimicrobial Resistance Surveillance in Europe 2022–2020 Data. Available online: https://www.ecdc.europa.eu/en/publications-data/antimicrobial-resistancesurveillance-europe-2022-2020-data (accessed on 12 February 2024).
- Dyar, O.J.; Huttner, B.; Schouten, J.; Pulcini, C.; ESGAP (ESCMID Study Group for Antimicrobial stewardshiP). What is antimicrobial stewardship? Clin. Microbiol. Infect. 2017, 23, 793–798. [Google Scholar] [CrossRef]
- Davey, P.; Marwick, C.A.; Scott, C.L.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst. Rev. 2017, 2, CD003543. [Google Scholar] [CrossRef]
- Pulcini, C.; Gyssens, I.C. How to educate prescribers in antimicrobial stewardship practices. Virulence 2013, 4, 192–202. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Action Plan on Antimicrobial Resistance. 2015. Available online: https://www.who.int/publications/i/item/9789241509763 (accessed on 12 February 2024).
- Mölstad, S.; Erntell, M.; Hanberger, H.; Melander, E.; Norman, C.; Skoog, G.; Lundborg, C.S.; Söderström, A.; Torell, E.; Cars, O. Sustained reduction of antibiotic use and low bacterial resistance: 10-year follow-up of the Swedish Strama programme. Lancet Infect. Dis. 2008, 8, 125–132. [Google Scholar] [CrossRef]
- Government Offices of Sweden. Swedish Strategy to Combat Antibiotic Resistance. 2016. Available online: https://www.vr.se/download/18.19df7fb916622e206d81e5/1538575613387/Swedish-strategy-to-combat-antibiotic-resistance.pdf (accessed on 5 March 2024).
- Pulcini, C.; Wencker, F.; Frimodt-Møller, N.; Kern, W.V.; Nathwani, D.; Rodríguez-Baño, J.; Simonsen, G.S.; Vlahović-Palčevski, V.; Gyssens, I.C.; Gyssens, I.; et al. European survey on principles of prudent antibiotic prescribing teaching in undergraduate students. Clin. Microbiol. Infect. 2015, 21, 354–361. [Google Scholar] [CrossRef]
- Dyar, O.J.; Lund, M.; Lindsjö, C.; Stålsby Lundborg, C.; Pulcini, C. Preparedness to prescribe antibiotics responsibly: A comparison between final year medical students in France and Sweden. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Abbo, L.M.; Cosgrove, S.E.; Pottinger, P.S.; Pereyra, M.; Sinkowitz-Cochran, R.; Srinivasan, A.; Webb, D.J.; Hooton, T.M. Medical students’ perceptions and knowledge about antimicrobial stewardship: How are we educating our future prescribers. Clin. Infect. Dis. 2013, 57, 631–638. [Google Scholar] [CrossRef]
- Rose, S. Medical Student Education in the Time of COVID-19. JAMA 2020, 323, 2131–2132. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Srivastav, S.; Bhardwaj, A.; Dixit, A.; Misra, S. Medical Education During the COVID-19 Pandemic: A Single Institution Experience. Indian Pediatr. 2020, 57, 678–679. [Google Scholar] [CrossRef]
- Theoret, C.; Ming, X. Our education, our concerns: The impact on medical student education of COVID-19. Med. Educ. 2020, 54, 591–592. [Google Scholar] [CrossRef]
- Schouten, J.; De Waele, J.; Lanckohr, C.; Koulenti, D.; Haddad, N.; Rizk, N.; Sjövall, F.; Kanj, S.S.; Alliance for the Prudent Use of Antibiotics. Antimicrobial stewardship in the ICU in COVID-19 times: The known unknowns. Int. J. Antimicrob. Agents 2021, 58, 106409. [Google Scholar] [CrossRef]
- Malli, I.A.; Mohamud, M.S.; Al-Nasser, S. Enhancing Medical Students’ Confidence and Knowledge in Antibiotic Prescription and Administration through Virtual Education: A Quasi-Experimental Study. Antibiotics 2023, 12, 1546. [Google Scholar] [CrossRef]
- Shahrvini, B.; Baxter, S.L.; Coffey, C.S.; MacDonald, B.V.; Lander, L. Pre-clinical remote undergraduate medical education during the COVID-19 pandemic: A survey study. BMC Med. Educ. 2021, 21, 13. [Google Scholar] [CrossRef] [PubMed]
- Biggs, J.; Tang, C. Teaching for Quality Learning at University, 4th ed.; Open University Press: Maidenhead, UK, 2011. [Google Scholar]


{kind=link}
| Topic | 2015 (n = 239) | 2021 (n = 309) | |||||
|---|---|---|---|---|---|---|---|
| Sufficiently Prepared | Sufficiently Prepared | Difference 1 | p | Trend | |||
| % | Range | % | Range | (Range) | |||
| To recognise the clinical signs of infection | 99.2 | 97–100 | 99.4 | 97–100 | 0.2 (−0.3–0.8) | 0.7 | ↗ |
| To assess the clinical severity of infection (e.g., using criteria such as the septic shock criteria) | 95.0 | 92–100 | 92.2 | 89–98 | −2.8 (−7.5–5.9) | 0.2 | ↘ |
| To use point-of-care tests (e.g., urine dipstick, rapid diagnostic tests for streptococcal pharyngitis) | 89.9 | 80–94 | 87.3 | 72–98 | −2.6 (−14.8–4.4) | 0.3 | ↘ |
| To interpret biochemical markers of inflammation (e.g., CRP) | 97.1 | 92–100 | 98.0 | 94–100 | 0.9 (−1.7–4.3) | 0.5 | ↗ |
| To decide when it is important to take microbiological samples before starting antibiotic therapy | 95.4 | 92–97 | 94.1 | 85–98 | −1.3 (−6.9–1.0) | 0.5 | ↘ |
| To interpret basic microbiological investigations (e.g., blood cultures, antibiotic susceptibility reporting) | 93.7 | 86–97 | 92.8 | 85–100 | −0.9 (−6.8–6.0) | 0.7 | ↘ |
| To identify clinical situations when not to prescribe an antibiotic | 93.7 | 92–97 | 84.4 | 64–90 | −9.3 (−30.2–−2.6) | <0.001 | ↘ |
| To differentiate between bacterial colonisation and infection (e.g., asymptomatic bacteriuria) | 91.2 | 89–97 | 87.3 | 75–95 | −3.9 (−19.1–2.1) | 0.1 | ↘ |
| To differentiate between bacterial and viral upper respiratory tract infections | 93.3 | 86–100 | 81.9 | 75–88 | −11.4 (−25.0–−2.6) | <0.001 | ↘ |
| To select initial empirical therapy based on the most likely pathogen(s) and antibiotic resistance patterns without using guidelines | 71.4 | 64–82 | 61.8 | 49–78 | −9.6 (−26.6–2.6) | 0.02 | ↘ |
| To decide the urgency of antibiotic administration in different situations (e.g., <1 h for severe sepsis, non-urgent for chronic bone infections) | 87.9 | 76–94 | 82.8 | 77–90 | −5.1 (−17.7–9.4) | 0.1 | ↘ |
| To prescribe antibiotic therapy according to national/local guidelines | 92.4 | 82–97 | 87.3 | 75–94 | −5.1 (−11.6–3.6) | 0.05 | ↘ |
| To assess antibiotic allergies (e.g., differentiating between anaphylaxis and hypersensitivity) | 76.1 | 66–94 | 72.3 | 60–91 | −3.8 (−18.5–25.5) | 0.3 | ↘ |
| To identify indications for combination antibiotic therapy | 61.4 | 48–70 | 48.3 | 32–62 | −13.1 (−25.8–−5.4) | 0.002 | ↘ |
| To decide the shortest possible adequate duration of antibiotic therapy for a specific infection | 62.2 | 46–76 | 48.2 | 36–57 | −14.0 (−31.7–0.4) | 0.001 | ↘ |
| To prescribe using principles of surgical antibiotic prophylaxis | 53.8 | 35–62 | 44.0 | 32–51 | −9.8 (−25.8–−5.4) | 0.02 | ↘ |
| To review the need to continue or change antibiotic therapy after 48–72 h, based on clinical evolution and laboratory results | 81.2 | 71–94 | 75.4 | 62–89 | −5.8 (−25.6–11.9) | 0.1 | ↘ |
| To assess clinical outcomes and possible reasons for the failure of antibiotic treatment | 83.1 | 76–88 | 77.5 | 66–87 | −5.6 (−12.3–−1.2) | 0.1 | ↘ |
| To decide when to switch from intravenous (IV) to oral antibiotic therapy | 75.1 | 68–82 | 65.2 | 51–75 | −9.9 (−22.0–−4.2) | 0.01 | ↘ |
| To measure/audit antibiotic use in a clinical setting and to interpret the results of such studies | 64.4 | 44–57 | 50.2 | 21–43 | −14.2 (−30.6–−7.8) | <0.001 | ↘ |
| To work within the multi-disciplinary team in managing antibiotic use in hospitals | 69.3 | 54–70 | 71.5 | 42–71 | 2.2 (−17.2–5.4) | 0.6 | ↗ |
| To discuss antibiotic use with patients who are asking for antibiotics when I feel they are not necessary | 95.3 | 88–97 | 93.4 | 81–98 | −1.9 (−7.7–3.9) | 0.3 | ↘ |
| To communicate with senior doctors in situations where I feel antibiotics are not necessary, but I feel I am being inappropriately pressured into prescribing antibiotics by senior doctors | 60.9 | 46–71 | 47.3 | 22–47 | −13.6 (−48.4–−0.4) | 0.002 | ↘ |
| To use knowledge of the common mechanisms of antibiotic resistance in pathogens | 84.0 | 78–100 | 78.8 | 62–90 | −5.2 (−30.9–5.9) | 0.1 | ↘ |
| To use knowledge of the epidemiology of bacterial resistance, including local/regional variations | 75.5 | 69–82 | 62.1 | 38–78 | −13.4 (−40.6–−3.5) | <0.001 | ↘ |
| To practise effective Infection control and hygiene (to prevent the spread of bacteria) | 97.9 | 95–100 | 95.5 | 89–98 | −2.4 (−6.6–−0.3) | 0.1 | ↘ |
| To use knowledge of the negative consequences of antibiotic use (bacterial resistance, toxic/adverse effects, cost, Clostridium difficile infections) | 97.9 | 94–100 | 95.8 | 89–98 | −2.1 (−8.6–3.1) | 0.2 | ↘ |
| Highest Preparedness | Lowest Preparedness | Greatest Variation between Medical Schools |
|---|---|---|
| To recognize the clinical signs of infection (99.4%) | To prescribe using principles of surgical antibiotic prophylaxis (44.0%) | To use knowledge of the negative consequences of antibiotic use (bacterial resistance, toxic/adverse effects, cost, Clostridium difficile infections) (37.7–78.3%) |
| To interpret biochemical markers of inflammation (e.g., CRP) (98.0%) | To communicate with senior doctors in situations where I feel antibiotics are not necessary but I feel I am being inappropriately pressured into prescribing antibiotics by senior doctors (47.3%) | To use knowledge of the common mechanisms of antibiotic resistance in pathogens (60.4–91.5%) |
| To use knowledge of the negative consequences of antibiotic use (bacterial resistance, toxic/adverse effects, cost, Clostridium difficile infections) (95.8%) | To decide the shortest possible adequate duration of antibiotic therapy for a specific infection (48.2%) | To interpret basic microbiological investigations (e.g., blood cultures, antibiotic susceptibility reporting) (41.7–71.4%) |
| To practise effective Infection control and hygiene (to prevent the spread of bacteria) (95.5%) | To identify indications for combination antibiotic therapy (48.3%) | To differentiate between bacterial and viral upper respiratory tract infections (32.1–61.7%) |
| To decide when it is important to take microbiological samples before starting antibiotic therapy (94.1%) | To measure/audit antibiotic use in a clinical setting and to interpret the results of such studies (50.2%) | To assess antibiotic allergies (e.g., differentiating between anaphylaxis and hypersensitivity) (49.1–78.3%) |
| Gothenburg | Karolinska | Lund | Umeå | Uppsala | Örebro |
|---|---|---|---|---|---|
| To prescribe using principles of surgical antibiotic prophylaxis (36.2%) | To communicate with senior doctors in situations where I feel antibiotics are not necessary but I feel I am being inappropriately pressured into prescribing antibiotics by senior doctors (34.7%) | To measure/audit antibiotic use in a clinical setting and to interpret the results of such studies (40.6%) | To measure/audit antibiotic use in a clinical setting and to interpret the results of such studies (20.8%) | To prescribe using principles of surgical antibiotic prophylaxis (40.0%) | To communicate with senior doctors in situations where I feel antibiotics are not necessary but I feel I am being inappropriately pressured into prescribing antibiotics by senior doctors (22.2%) |
| To measure/audit antibiotic use in a clinical setting and to interpret the results of such studies (36.2%) | To measure/audit antibiotic use in a clinical setting and to interpret the results of such studies (38.8%) | To communicate with senior doctors in situations where I feel antibiotics are not necessary but I feel I am being inappropriately pressured into prescribing antibiotics by senior doctors (45.3%) | To prescribe using principles of surgical antibiotic prophylaxis (32.1%) | To measure/audit antibiotic use in a clinical setting and to interpret the results of such studies (43.3%) | To measure/audit antibiotic use in a clinical setting and to interpret the results of such studies (27.8%) |
| Percentage of Students Who Feel They Need More Education | 2015 | 2021 | p |
|---|---|---|---|
| Gothenburg University | 18% | 36% | 0.05 |
| Karolinska Institutet | 25% | 40% | 0.09 |
| Lund University | 19% | 32% | 0.18 |
| Umeå University | 32% | 37% | 0.63 |
| Uppsala University | 13% | 16% | 0.7 |
| Örebro University | 18% | 52% | 0.02 |
| Average | 21% | 36% | 0.003 |
| Teaching Method | Useful or Very Useful | Not Useful | Neutral | I Am Unsure | I Do Not Understand the Question | Teaching Method Was Not Used 1 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2015 | 2021 | 2015 | 2021 | 2015 | 2021 | 2015 | 2021 | 2015 | 2021 | 2015 | 2021 | |||
| % | Range | % | Range | % | % | % | % | % | % | % | % | % | % | |
| Lectures (with >15 people) | 88.1 | 77.1–97.0 | 77.7 | 57.8–86.7 | 0.4 | 0.0 | 10.2 | 19.1 | 1.3 | 3.2 | 0.0 | 0.0 | 0.4 | 2.1 |
| Small group teaching (with <15 people) | 95.0 | 70.6–93.9 | 91.0 | 55.6–90.6 | 0.9 | 0.7 | 2.7 | 3.7 | 1.4 | 4.5 | 0.0 | 0.0 | 5.5 | 7.9 |
| Discussions of clinical cases and vignettes | 92.2 | 82.4–92.5 | 90.9 | 66.7–92.2 | 0.4 | 0.3 | 4.8 | 5.9 | 2.2 | 2.1 | 0.4 | 0.7 | 1.3 | 1.0 |
| Active learning assignments | 51.9 | 35.1–52.0 | 54.1 | 25.0–47.2 | 7.4 | 6.4 | 35.4 | 32.7 | 5.3 | 6.8 | 0.0 | 0.0 | 18.9 | 23.9 |
| Infectious diseases clinical placement | 93.6 | 88.6–95.5 | 82.6 | 58.3–85.9 | 0.4 | 3.2 | 5.1 | 12.4 | 0.8 | 1.1 | 0.0 | 0.7 | 0.0 | 2.8 |
| Microbiology clinical placement | 47.1 | 8.6–52.9 | 38.8 | 8.3–29.8 | 10.1 | 6.2 | 30.4 | 39.5 | 11.6 | 14.7 | 0.7 | 0.8 | 41.5 | 55.2 |
| Peer or near-peer teaching | 68.5 | 27.3–48.6 | 67.5 | 22.2–42.2 | 1.5 | 1.3 | 17.7 | 20.5 | 10.8 | 9.9 | 1.5 | 0.7 | 44.7 | 47.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Nasir, J.; Belančić, A.; Palčevski, D.; Dyar, O.J.; on behalf of Student-PREPARE Sweden Working Group. 2015 versus 2021: Self-Reported Preparedness to Prescribe Antibiotics Prudently among Final Year Medical Students in Sweden. Antibiotics 2024, 13, 303. https://doi.org/10.3390/antibiotics13040303
Al-Nasir J, Belančić A, Palčevski D, Dyar OJ, on behalf of Student-PREPARE Sweden Working Group. 2015 versus 2021: Self-Reported Preparedness to Prescribe Antibiotics Prudently among Final Year Medical Students in Sweden. Antibiotics. 2024; 13(4):303. https://doi.org/10.3390/antibiotics13040303
Chicago/Turabian StyleAl-Nasir, Jasmine, Andrej Belančić, Dora Palčevski, Oliver J. Dyar, and on behalf of Student-PREPARE Sweden Working Group. 2024. "2015 versus 2021: Self-Reported Preparedness to Prescribe Antibiotics Prudently among Final Year Medical Students in Sweden" Antibiotics 13, no. 4: 303. https://doi.org/10.3390/antibiotics13040303