

Knowledge, Attitudes, and Practices of Rural Communities Regarding Antimicrobial Resistance and Climate Change in Adadle District, Somali Region, Ethiopia: A Mixed-Methods Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Quantitative Results
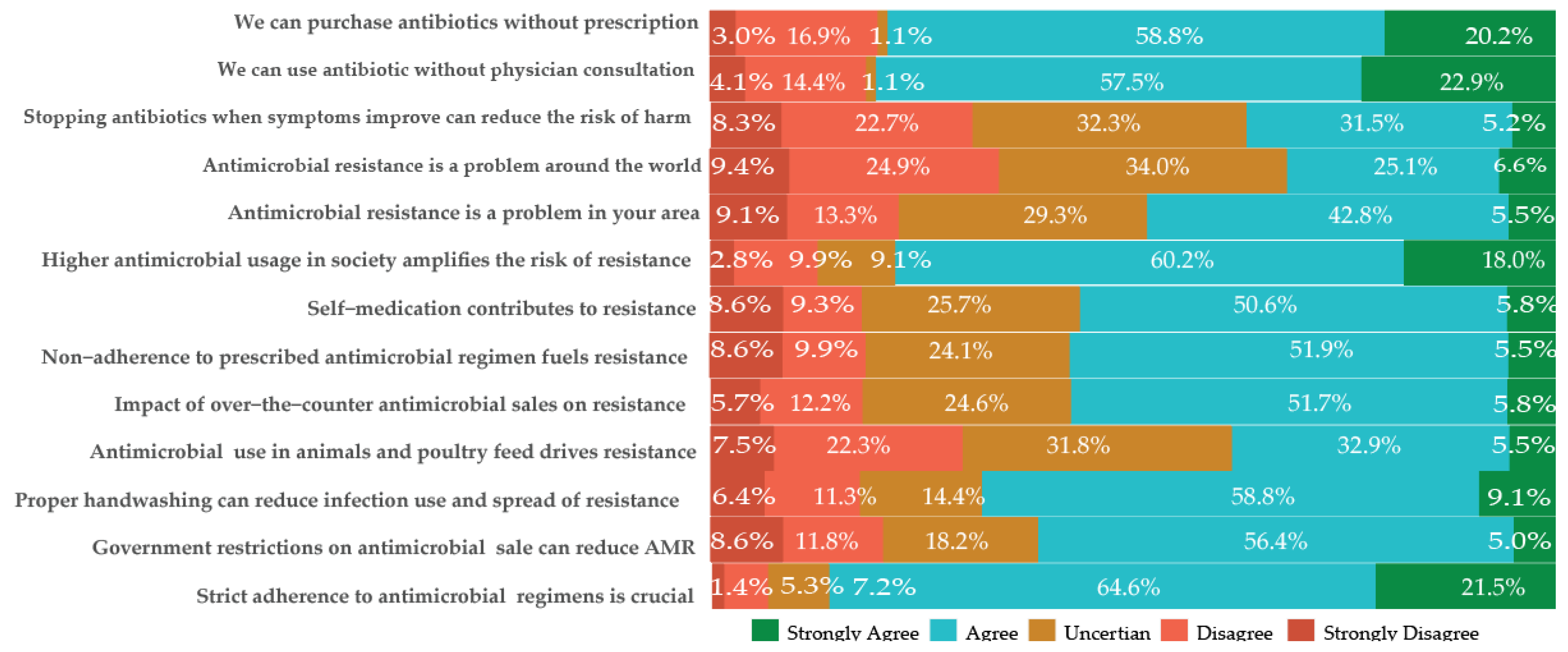
2.2. Knowledge and Attitude on Antimicrobials and AMR
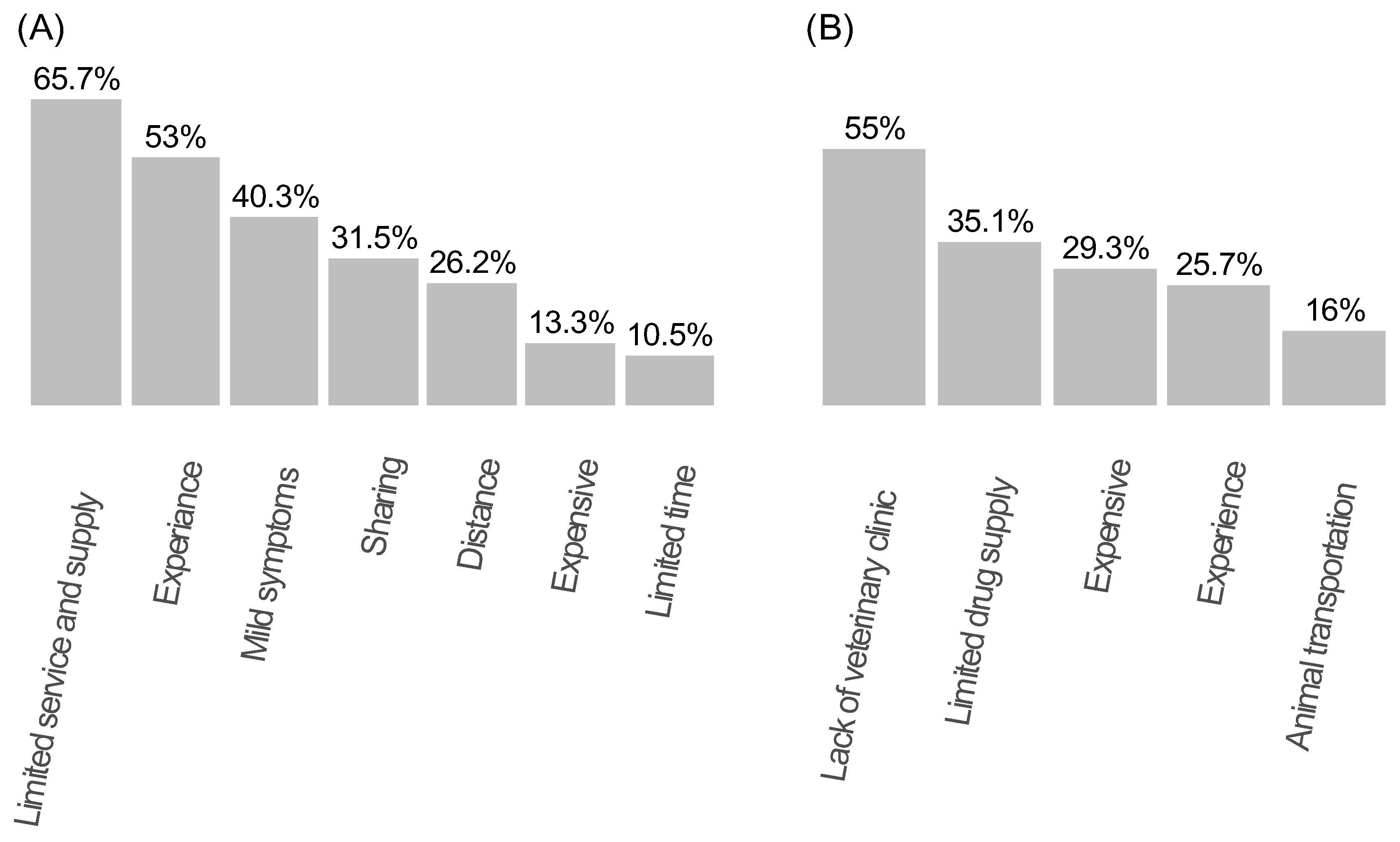
2.3. Practice on Antimicrobial Use
2.4. Knowledge and Attitude on Climate Change
2.5. Knowledge, Attitudes, and Practices Scores of Study Participants in Different Settings
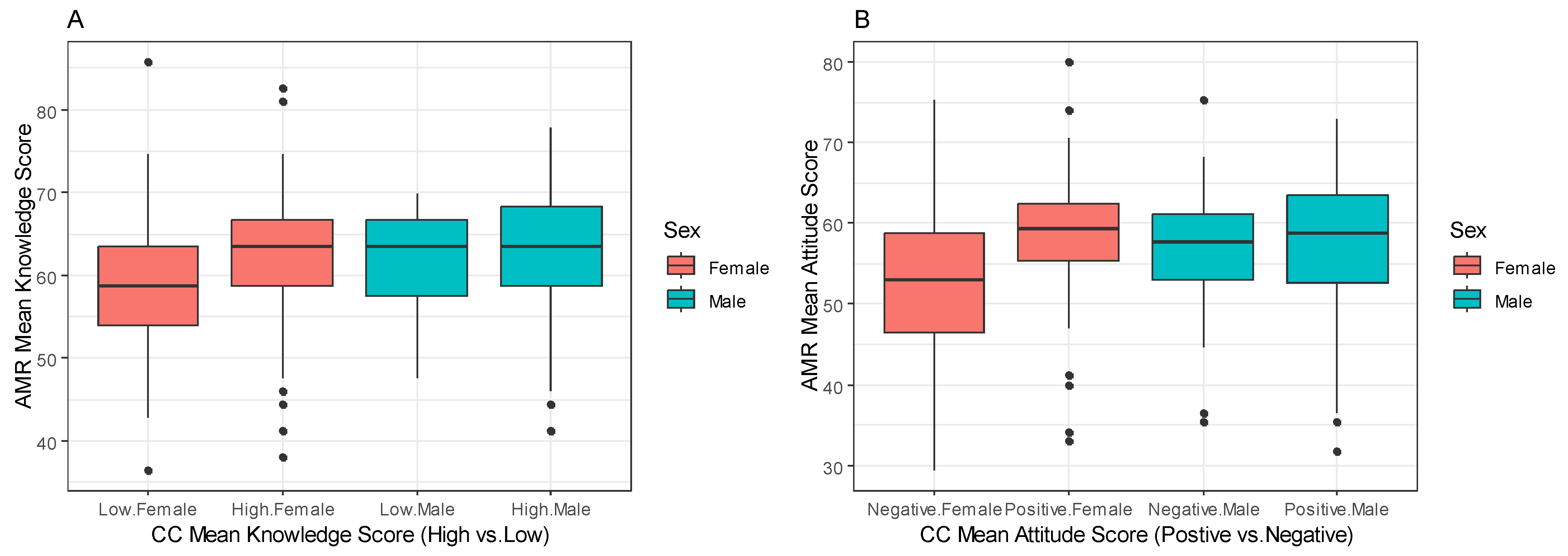
2.6. Mean Knowledge and Attitude Scores of Participants Regarding AMR and CC across Demographics
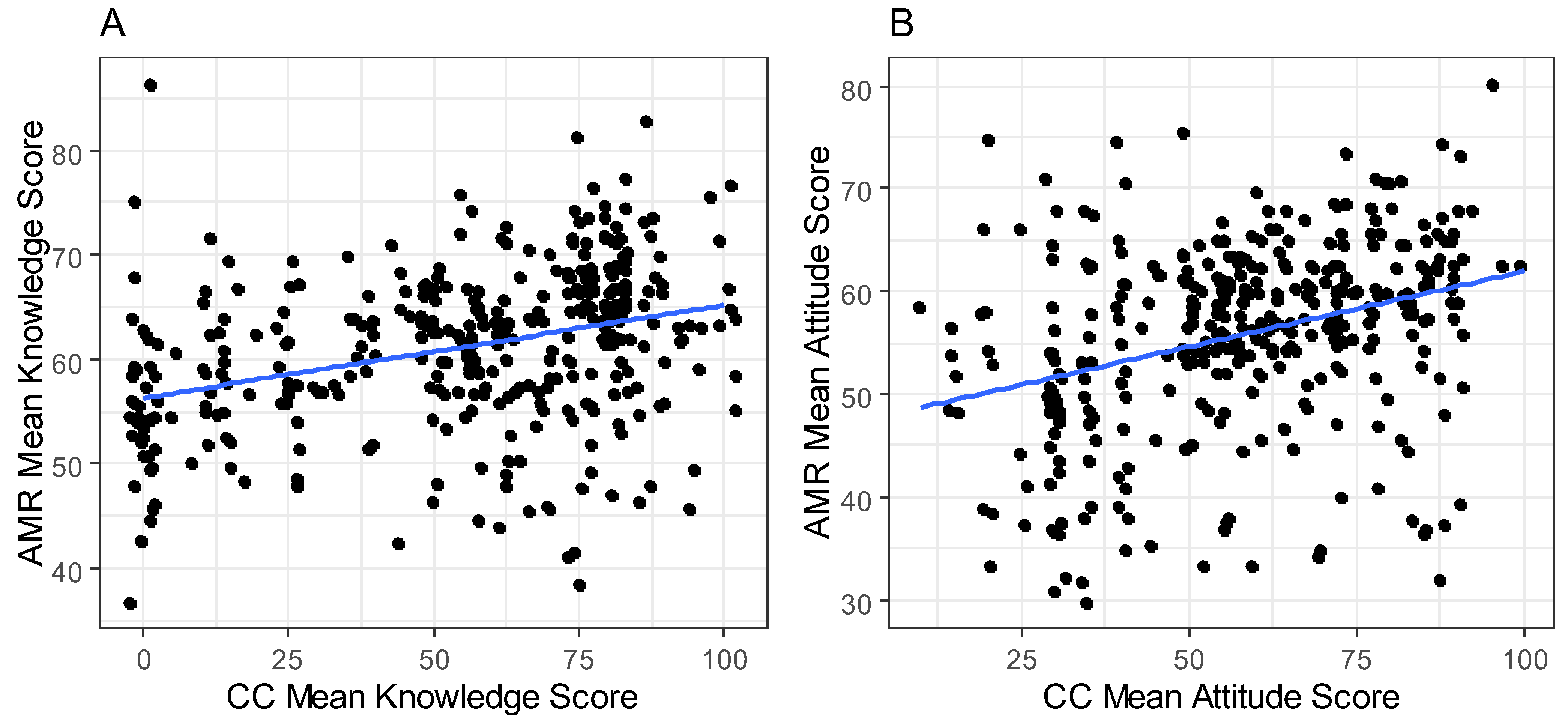
2.7. Comparing the Mean Knowledge and Attitude Scores of AMR and CC
2.8. Factors Associated with Knowledge and Attitudes (Multivariable Analysis)
2.9. Qualitative Results
2.10. Knowledge on Antimicrobials and Antimicrobial Use
Aaah’ whenever we go to the health facility or pharmacy, they always say it is an infection and give us Amoxicillin, which I believe is not as effective as Ampicillin (qoormdoobe, or black neck). The two most common antibiotics that we use are amoxicillin and ampicillin (qoormadoobe, or black neck)[CM: Woman: Age: 42 years]
They are drugs that can treat any diseases or alleviate pain, and without them, I believe life would have been very difficult for us.[CM: Man: Age: 54 years]
2.11. Knowledge on AMR
Yeah, we often hear that, if we do not take the medication correctly or misuse it, our bodies can adapt to it, which means it may not work in the future.[CM: Man: Age: 52 years]
I have heard several times that people complain about antibiotics like amoxicillin not working. I have experienced this myself—I took another antibiotic, and it did not work either. However, I never considered it might be due to resistance; I simply thought maybe the disease and the medicine didn’t match. There are many such cases.[CM: Woman: Age: 49 years]
Yes, it can be transmitted, for example, if one person is infected with TB, he/she can transmit it to the other family members who live with them or share food or are in close proximity to them. We used to take them outside the house and keep them away from the family. Because we know that, they can transmit to the other family member. If he gets close to the family member.[CM: Female: Age: 49 years]
2.12. Attitude and Practices on Antimicrobial Use
Yes, we ask and share medicine within ourselves. For example, if we share the same signs and symptoms with a family member or neighbor, like coughing, I will share the antibiotic with them. Sometimes, I keep it for future use in case somebody gets sick.[CM: Woman: Age: 51 years]
I would like to go to the health facility, but I have to take care of the children, the house, and other family activities. Therefore, it is easier and quicker to get the drugs from the pharmacy instead of going to the hospital, which takes all morning.[CM: Female: Age: 45 years].
We prefer the health center because the medications there are cheaper and of good quality compared to outside pharmacies. However, insufficient drug supply, inappropriate diagnosis, lack of laboratory services, and a limited number of health professionals often compel us to go to the pharmacy instead. This is because pharmacies may have a better drug supply than the health center. Additionally, the health professionals who work in the health center often own the pharmacy. The services they provide are essentially the same since both lack basic investigation.[CM: Female: Age: 37 years].
2.13. Livestock Antimicrobial Use and Practice
One of the challenges we face is the limited availability of medication for livestock in our area. Throughout the year, we receive only a small number of vials of tetracycline and penstrep. Tetracycline is the only drug accessible for treating livestock, and we utilize it whenever it is available or when there are remaining doses. In situations involving severe conditions, we consult animal health workers. However, their capacity to provide comprehensive assistance is constrained by the limited availability of animal health services. Regardless of whether we consult with professionals or not, the situation remains unchanged. Consequently, we continue to rely on our experiences to address the health needs of our livestock.[CM: Community animal health worker: Age: 45 years].
2.14. Climate Change and Antimicrobial Resistance
The weather is getting worse year after year. Well… let me tell you. In the past eight to ten years, we have been tussling with severe droughts. For ten years now, we used to name the droughts because they occurred one at a time for extended periods. However, in the last eight years, droughts have been happening consecutively. Due to their recurrence, we no longer give them names.[CM: Female: Age: 41 years].
Over the past eight years, we have lost most of our livestock to drought rather than diseases. To save the remaining livestock, most of the community migrated from the Kebele in search of water and food. Whenever we face severe drought, we usually migrate to find water and food, but during these migrations, we lose some of our livestock due to hunger and diseases.[CM: Male: Age: 54 years].
Well … we do not have the technology or materials to measure the weather, only God knows the change of the weather.[CM: Female: Age: 43 years].
3. Discussion
4. Materials and Methods
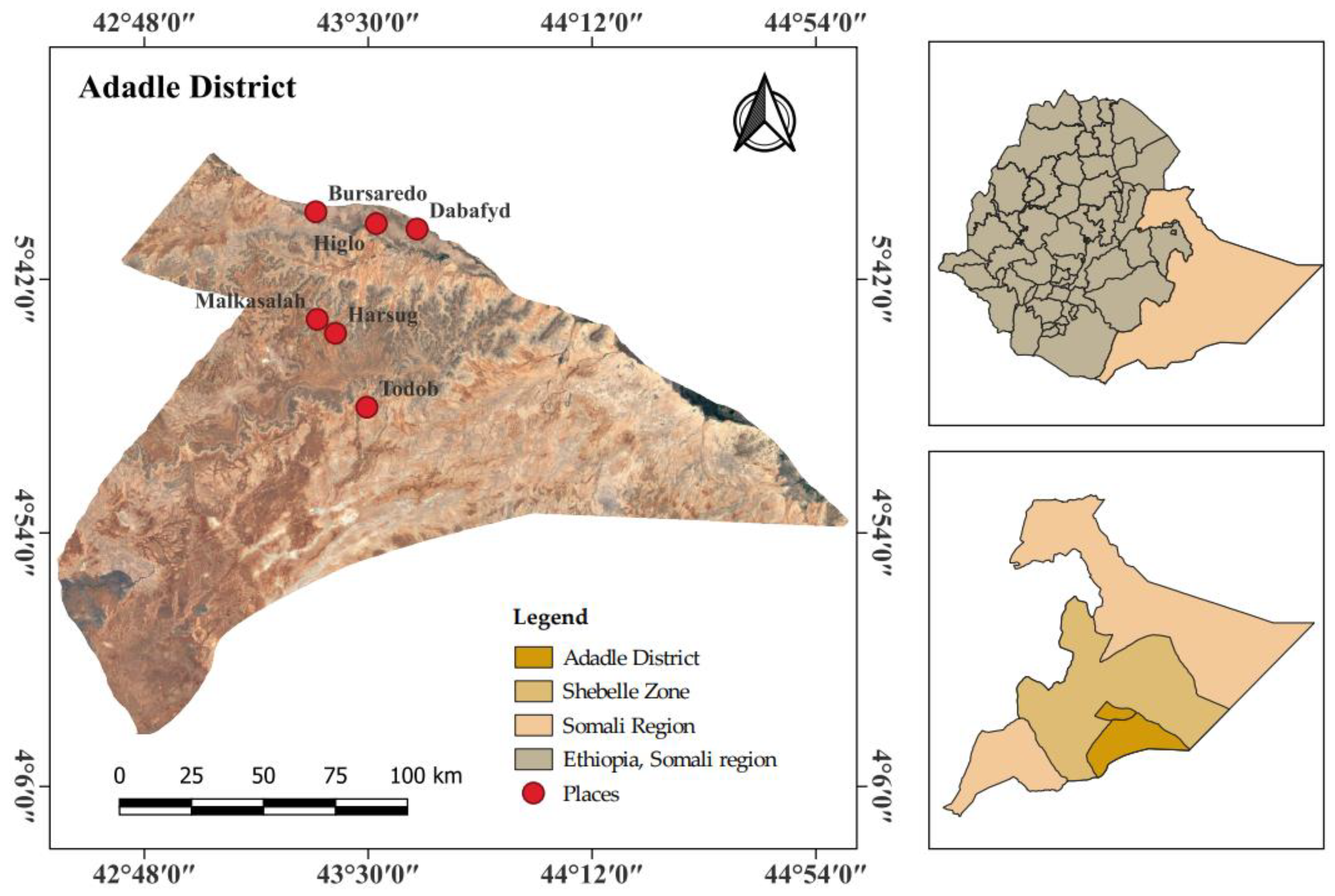
4.1. Study Area
4.2. Study Desing
4.3. Sample Size Calculation
4.4. Data Collection Instrument
4.5. Sampling Technique and Data Collection
4.6. Data Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lio, R.M.S.; Favara, G.; Maugeri, A.; Barchitta, M.; Agodi, A. How antimicrobial resistance is linked to climate change: An overview of two intertwined global challenges. Int. J. Environ. Res. Public Health 2023, 20, 1681. [Google Scholar]
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. 19 May 2016, Government of the United Kingdom. p. 84. Available online: https://apo.org.au/node/63983 (accessed on 24 February 2024).
- World Health Organization. Quantitative Risk Assessment of the Effects of Climate Change on Selected Causes of Death, 2030s and 2050s; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Harring, N.; Krockow, E.M. The social dilemmas of climate change and antibiotic resistance: An analytic comparison and discussion of policy implications. Humanit. Soc. Sci. Commun. 2021, 8, 125. [Google Scholar] [CrossRef]
- Kaba, H.E.; Kuhlmann, E.; Scheithauer, S. Thinking outside the box: Association of antimicrobial resistance with climate warming in Europe–A 30 country observational study. Int. J. Hyg. Environ. Health 2020, 223, 151–158. [Google Scholar] [CrossRef]
- Lelieveld, J.; Klingmüller, K.; Pozzer, A.; Burnett, R.T.; Haines, A.; Ramanathan, V. Effects of fossil fuel and total anthropogenic emission removal on public health and climate. Proc. Natl. Acad. Sci. USA 2019, 116, 7192–7197. [Google Scholar] [CrossRef]
- MacFadden, D.R.; McGough, S.F.; Fisman, D.; Santillana, M.; Brownstein, J.S. Antibiotic resistance increases with local temperature. Nat. Clim. Chang. 2018, 8, 510–514. [Google Scholar] [CrossRef] [PubMed]
- Patz, J.A.; Olson, S.H. Climate change and health: Global to local influences on disease risk. Ann. Trop. Med. Parasitol. 2006, 100, 535–549. [Google Scholar] [CrossRef] [PubMed]
- Zinsstag, J.; Crump, L.; Schelling, E.; Hattendorf, J.; Maidane, Y.O.; Ali, K.O.; Muhummed, A.; Umer, A.A.; Aliyi, F.; Nooh, F.; et al. Climate change and one health. FEMS Microbiol. Lett. 2018, 365, fny085. [Google Scholar] [CrossRef]
- Cissé, G. Food-borne and water-borne diseases under climate change in low- and middle-income countries: Further efforts needed for reducing environmental health exposure risks. Acta Trop. 2019, 194, 181–188. [Google Scholar] [CrossRef]
- Lake, I.R.; Hooper, L.; Abdelhamid, A.; Bentham, G.; Boxall, A.B.; Draper, A.; Fairweather-Tait, S.; Hulme, M.; Hunter, P.R.; Nichols, G.; et al. Climate change and food security: Health impacts in developed countries. Environ. Health Perspect. 2012, 120, 1520–1526. [Google Scholar] [CrossRef]
- Springmann, M.; Mason-D’Croz, D.; Robinson, S.; Garnett, T.; Godfray, H.C.J.; Gollin, D.; Rayner, M.; Ballon, P.; Scarborough, P. Global and regional health effects of future food production under climate change: A modelling study. Lancet 2016, 387, 1937–1946. [Google Scholar] [CrossRef]
- Wassie, S.B. Natural resource degradation tendencies in Ethiopia: A review. Environ. Syst. Res. 2020, 9, 1–29. [Google Scholar]
- Simane, B.; Beyene, H.; Deressa, W.; Kumie, A.; Berhane, K.; Samet, J. Review of Climate Change and Health in Ethiopia: Status and Gap Analysis. Ethiop. J. Health Dev. 2016, 30, 28–41. [Google Scholar] [PubMed]
- Simegn, W.; Moges, G. Awareness and knowledge of antimicrobial resistance and factors associated with knowledge among adults in Dessie City, Northeast Ethiopia: Community-based cross-sectional study. PLoS ONE 2022, 17, e0279342. [Google Scholar] [CrossRef] [PubMed]
- Tesfaye, Z. Patient knowledge and practice on antimicrobial use and resistance in Felege Hiwot hospital, Bahir Dar, Ethiopia. J. Basic Clin. Pharm. 2017, 8, S010–S015. [Google Scholar]
- Belay, A.; Oludhe, C.; Mirzabaev, A.; Recha, J.W.; Berhane, Z.; Osano, P.M.; Demissie, T.; Olaka, L.A.; Solomon, D. Knowledge of climate change and adaptation by smallholder farmers: Evidence from southern Ethiopia. Heliyon 2022, 8, e12089. [Google Scholar] [CrossRef]
- Amare, Z.Y.; Ayoade, J.O.; Adelekan, I.O.; Zeleke, M.T. Rural communities’ perception of climate change and its determinants in Dejen district, Nile basin of Ethiopia. Asian J. Agric. Rural. Dev. 2017, 7, 102–114. [Google Scholar] [CrossRef]
- Abrham, T.; Mekuyie, M. Effects of climate change on pastoral households in the Harshin District of the Somali Region, Ethiopia. Jàmbá 2022, 14, 1202. [Google Scholar]
- Nyoni, N.M.B.; Grab, S.; Archer, E.R.M. Heat stress and chickens: Climate risk effects on rural poultry farming in low-income countries. Clim. Dev. 2019, 11, 83–90. [Google Scholar] [CrossRef]
- Ayukekbong, J.A.; Ntemgwa, M.; Atabe, A.N. The threat of antimicrobial resistance in developing countries: Causes and control strategies. Antimicrob. Resist. Infect. Control. 2017, 6, 47. [Google Scholar]
- Woldegeorgis, B.Z.; Kerbo, A.A.; Obsa, M.S.; Mokonnon, T.M. A systematic review and meta-analysis of antimicrobial resistance knowledge, attitudes, and practices: Current evidence to build a strong national antimicrobial drug resistance narrative in Ethiopia. PLoS ONE 2023, 18, e0287042. [Google Scholar] [CrossRef]
- Andersen, J.G.; Kallestrup, P.; Karekezi, C.; Yonga, G.; Kraef, C. Climate change and health risks in Mukuru informal settlement in Nairobi, Kenya-knowledge, attitudes and practices among residents. BMC Public Health 2023, 23, 393. [Google Scholar]
- Melore, T.W.; Nel, V. Resilience of informal settlements to climate change in the mountainous areas of Konso, Ethiopia and QwaQwa, South Africa. Jàmbá 2020, 12, 778. [Google Scholar] [CrossRef] [PubMed]
- Musoke, D.; Namata, C.; Lubega, G.B.; Kitutu, F.E.; Mugisha, L.; Amir, S.; Brandish, C.; Gonza, J.; Ikhile, D.; Niyongabo, F.; et al. Access, use and disposal of antimicrobials among humans and animals in Wakiso district, Uganda: A qualitative study. J. Pharm. Policy Pract. 2021, 14, 69. [Google Scholar] [CrossRef]
- Ndaki, P.M.; Mushi, M.F.; Mwanga, J.R.; Konje, E.T.; Mugassa, S.; Manyiri, M.W.; Mwita, S.M.; Ntinginya, N.E.; Mmbaga, B.T.; Keenan, K.; et al. Non-prescribed antibiotic dispensing practices for symptoms of urinary tract infection in community pharmacies and accredited drug dispensing outlets in Tanzania: A simulated clients approach. BMC Prim. Care 2022, 23, 287. [Google Scholar] [CrossRef]
- Sindato, C.; Mboera, L.E.G.; Katale, B.Z.; Frumence, G.; Kimera, S.; Clark, T.G.; Legido-Quigley, H.; Mshana, S.E.; Rweyemamu, M.M.; Matee, M. Knowledge, attitudes and practices regarding antimicrobial use and resistance among communities of Ilala, Kilosa and Kibaha districts of Tanzania. Antimicrob. Resist. Infect. Control 2020, 9, 194. [Google Scholar] [CrossRef] [PubMed]
- Tafa, B.; Endale, A.; Bekele, D. Paramedical staffs knowledge and attitudes towards antimicrobial resistance in Dire Dawa, Ethiopia: A cross sectional study. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 64. [Google Scholar] [CrossRef]
- Amaha, M.H.; Alemu, B.M.; Atomsa, G.E. Self-medication practice and associated factors among adult community members of Jigjiga town, Eastern Ethiopia. PLoS ONE 2019, 14, e0218772. [Google Scholar] [CrossRef] [PubMed]
- Ayalew, M.B. Self-medication practice in Ethiopia: A systematic review. Patient Prefer. Adherence 2017, 11, 401–413. [Google Scholar] [CrossRef]
- Zheng, Z.; Feng, Z.; Zhang, D.; Sun, X.; Dong, D.; Luo, Y.; Feng, D. Does self-medication reduce medical expenditure among the middle-aged and elderly population? A four-wave longitudinal study in China. Front. Public Health 2023, 10, 1047710. [Google Scholar] [CrossRef]
- Cambaco, O.; Menendez, Y.A.; Kinsman, J.; Sigaúque, B.; Wertheim, H.; Do, N.; Gyapong, M.; John-Langba, J.; Sevene, E.; Munguambe, K. Community knowledge and practices regarding antibiotic use in rural Mozambique: Where is the starting point for prevention of antibiotic resistance? BMC Public Health 2020, 20, 1183. [Google Scholar] [CrossRef]
- Ayele, Y.; Mamu, M. Assessment of knowledge, attitude and practice towards disposal of unused and expired pharmaceuticals among community in Harar city, Eastern Ethiopia. J. Pharm. Policy Pract. 2018, 11, 27. [Google Scholar] [CrossRef]
- Gebeyehu, E.; Bantie, L.; Azage, M. Inappropriate use of antibiotics and its associated factors among urban and rural communities of Bahir Dar City Administration, Northwest Ethiopia. PLoS ONE 2015, 10, e0138179. [Google Scholar] [CrossRef] [PubMed]
- Muhie, O.A. Antibiotic use and resistance pattern in Ethiopia: Systematic review and meta-analysis. Int. J. Microbiol. 2019, 2019, 2489063. [Google Scholar] [CrossRef] [PubMed]
- Hussein, H.A.; Abdi, S.M.; Ahad, A.A. Factors and challenges contributing to antimicrobial resistance in East African pastoral settings and importance of One Health approach. CABI One Health 2023, 2023, ohcs202300025. [Google Scholar] [CrossRef]
- Shackleton, S.; Ziervogel, G.; Sallu, S.; Gill, T.; Tschakert, P. Why is socially-just climate change adaptation in sub-Saharan Africa so challenging? A review of barriers identified from empirical cases. Wiley Interdiscip. Rev. Clim. Chang. 2015, 6, 321–344. [Google Scholar] [CrossRef]
- Bryan, E.; Deressa, T.T.; Gbetibouo, G.A.; Ringler, C. Adaptation to climate change in Ethiopia and South Africa: Options and constraints. Environ. Sci. Policy 2009, 12, 413–426. [Google Scholar] [CrossRef]
- Gandure, S.; Walker, S.; Botha, J. Farmers’ perceptions of adaptation to climate change and water stress in a South African rural community. Environ. Dev. 2013, 5, 39–53. [Google Scholar]
- Mandleni, B.; Anim, F. Perceptions of cattle and sheep farmers on climate change and adaptation in the Eastern Cape Province of South Africa. J. Hum. Ecol. 2011, 34, 107–112. [Google Scholar]
- Artur, L.; Hilhorst, D. Everyday realities of climate change adaptation in Mozambique. Glob. Environ. Chang. 2012, 22, 529–536. [Google Scholar] [CrossRef]
- Rouleau, T.; Stuart, J.; Call, M.; Yozell, S.; Yoshioka, N.; Maekawa, M.; Fiertz, N. The climate and ocean risk vulnerability index: Measuring coastal city resilience to inform action. Front. Sustain. Cities 2022, 4, 884212. [Google Scholar] [CrossRef]
- Berger-Gonzalez, M.; Stauffacher, M.; Zinsstag, J.; Edwards, P.; Krütli, P. Transdisciplinary research on cancer-healing systems between biomedicine and the Maya of Guatemala: A tool for reciprocal reflexivity in a multi-epistemological setting. Qual. Health Res. 2016, 26, 77–91. [Google Scholar] [CrossRef]
- Hadorn, G.H.; Bradley, D.; Pohl, C.; Rist, S.; Wiesmann, U. Implications of transdisciplinarity for sustainability research. Ecol. Econ. 2006, 60, 119–128. [Google Scholar] [CrossRef]
- Stålne, K.; Pedersen, E. Transdisciplinary research on indoor environment and health as a social process. Int. J. Environ. Res. Public Health 2021, 18, 4379. [Google Scholar] [CrossRef] [PubMed]
- Asekun-Olarinmoye, E.O.; Bamidele, J.O.; Odu, O.O.; Olugbenga-Bello, A.I.; Abodurin, O.L.; Adebimpe, W.O.; Oladele, E.A.; Adeomi, A.A.; Adeoye, O.A.; Ojofeitimi, E.O. Public perception of climate change and its impact on health and environment in rural southwestern Nigeria. Res. Rep. Trop. Med. 2014, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kabir, M.I.; Rahman, M.B.; Smith, W.; Lusha, M.A.F.; Azim, S. Knowledge and perception about climate change and human health: Findings from a baseline survey among vulnerable communities in Bangladesh. BMC Public Health 2016, 16, 266. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.-Y.; Skandalos, N.; Braslina, L.; Kapsalis, V.; Karamanis, D. Integrating Solar Energy and Nature-Based Solutions for Climate-Neutral Urban Environments. Solar 2023, 3, 382–415. [Google Scholar] [CrossRef]
- Dorosh, P.; Rashid, S. Food and Agriculture in Ethiopia: Progress and Policy Challenges; University of Pennsylvania Press: Philadelphia, PA, USA, 2013; Available online: https://ideas.repec.org/p/fpr/issbrf/74.html (accessed on 24 February 2024).
- Cochrane, L.; Singh, R. Climate Services for Resilience: The Changing Roles of NGOs in Ethiopia; BRACED: London, UK, 2017. [Google Scholar]
- Seiler, C.; Berendonk, T.U. Berendonk, Heavy metal driven co-selection of antibiotic resistance in soil and water bodies impacted by agriculture and aquaculture. Front. Microbiol. 2012, 3, 18889. [Google Scholar] [CrossRef]
- Singer, A.C.; Shaw, H.; Rhodes, V.; Hart, A. Review of antimicrobial resistance in the environment and its relevance to environmental regulators. Front. Microbiol. 2016, 7, 219380. [Google Scholar] [CrossRef]
- Cissé, G.; McLeman, R.; Adams, H.; Aldunce, P.; Bowen, K.; Campbell-Lendrum, D.; Clayton, S.; Ebi, K.L.; Hess, J.; Huang, C.; et al. 2022: Health, Wellbeing, and the Changing Structure of Communities; Cambridge University Press: Cambridge, UK, 2022. [Google Scholar]
- Malik, B.; Bhattacharyya, S. Antibiotic drug-resistance as a complex system driven by socio-economic growth and antibiotic misuse. Sci. Rep. 2019, 9, 9788. [Google Scholar] [CrossRef]
- Cecchini, S.; Scott, C. Can information and communications technology applications contribute to poverty reduction? Lessons from rural India. Inf. Technol. Dev. 2003, 10, 73–84. [Google Scholar]
- Simegn, W.; Dagnew, B.; Weldegerima, B.; Dagne, H. Knowledge of antimicrobial resistance and associated factors among health professionals at the University of Gondar specialized hospital: Institution-based cross-sectional study. Front. Public Health 2022, 10, 790892. [Google Scholar] [CrossRef]
- Maja, M.M.; Idiris, A.A.; Terefe, A.T.; Fashe, M.M. Gendered vulnerability, perception and adaptation options of smallholder farmers to climate change in eastern Ethiopia. Earth Syst. Environ. 2023, 7, 189–209. [Google Scholar] [CrossRef]
- Pham-Duc, P.; Sriparamananthan, K. Exploring gender differences in knowledge and practices related to antibiotic use in Southeast Asia: A scoping review. PLoS ONE 2021, 16, e0259069. [Google Scholar] [CrossRef]
- Erku, D.A.; Mekuria, A.B.; Belachew, S.A. Inappropriate use of antibiotics among communities of Gondar town, Ethiopia: A threat to the development of antimicrobial resistance. Antimicrob. Resist. Infect. Control 2017, 6, 112. [Google Scholar] [CrossRef]
- Wibeck, V. Enhancing learning, communication and public engagement about climate change–some lessons from recent literature. Environ. Educ. Res. 2014, 20, 387–411. [Google Scholar] [CrossRef]
- Ojomo, E.; Elliott, M.; Amjad, U.; Bartram, J. Climate change preparedness: A knowledge and attitudes study in southern Nigeria. Environments 2015, 2, 435–448. [Google Scholar] [CrossRef]
- Gebeyehu, D.T.; Bekele, D.; Mulate, B.; Gugsa, G.; Tintagu, T. Knowledge, attitude and practice of animal producers towards antimicrobial use and antimicrobial resistance in Oromia zone, north eastern Ethiopia. PLoS ONE 2021, 16, e0251596. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Tackling Antimicrobial Resistance (AMR) Together: Working Paper 5.0: Enhancing the Focus on Gender and Equity; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Zhang, Y.; Huang, L.; Chao, Q.; Yang, Q.; Chen, C. Analysis of gender equality in climate governance. Chin. J. Popul. Resour. Environ. 2021, 19, 98–103. [Google Scholar] [CrossRef]
- Deressa, T.T.; Hassan, R.M.; Ringler, C. Perception of and adaptation to climate change by farmers in the Nile basin of Ethiopia. J. Agric. Sci. 2011, 149, 23–31. [Google Scholar] [CrossRef]
- Rouusounides, A.; Papaevangelou, V.; Hadjipanayis, A.; Panagakou, S.; Theodoridou, M.; Syrogiannopoulos, G.; Hadjichristodoulou, C. Descriptive Study on Parents’ Knowledge, Attitudes and Practices on Antibiotic Use and Misuse in Children with Upper Respiratory Tract Infections in Cyprus. Int. J. Environ. Res. Public Health 2011, 8, 3246–3262. [Google Scholar] [CrossRef] [PubMed]
- Alduhaimi, G.S.; Alabdulkareem, M.E.; Alhussin, G.I.; Alhumaid, L.A.; Basudan, S.K.; Masud, N.; Alhatmi, H.A.; Bosaeed, M.A. Awareness of Antimicrobial Resistance: Surveillance among Visitors of a Tertiary Care Center, Riyadh, Saudi Arabia. Saudi J. Health Syst. Res. 2022, 2, 128–135. [Google Scholar] [CrossRef]
- Wiernik, B.M.; Ones, D.S.; Dilchert, S. Age and environmental sustainability: A meta-analysis. J. Manag. Psychol. 2013, 28, 826–856. [Google Scholar] [CrossRef]
- Yang, X.; Wei, L.; Su, Q. How Is Climate Change Knowledge Distributed among the Population in Singapore? A Demographic Analysis of Actual Knowledge and Illusory Knowledge. Sustainability 2020, 12, 3782. [Google Scholar] [CrossRef]
- Hess, D.J.; Collins, B.M. Climate change and higher education: Assessing factors that affect curriculum requirements. J. Clean. Prod. 2018, 170, 1451–1458. [Google Scholar] [CrossRef]
- Destaw, F.; Fenta, M. Climate change adaptation strategies and their predictors amongst rural farmers in Ambassel district, Northern Ethiopia. Jamba 2021, 13, 974. [Google Scholar]
- Alston, M. Gender mainstreaming and climate change. Women’s Stud. Int. Forum 2014, 47, 287–294. [Google Scholar]
- Irawati, L.; Alrasheedy, A.A.; Hassali, M.A.; Saleem, F. Low-income community knowledge, attitudes and perceptions regarding antibiotics and antibiotic resistance in Jelutong District, Penang, Malaysia: A qualitative study. BMC Public Health 2019, 19, 1292. [Google Scholar]
- Russom, M.; Bahta, M.; Debesai, M.; Bahta, I.; Kessete, A.; Afendi, A.; Fitsum, Y.; Nambozi, J.; Kidane, S.N.; Tesfamariam, E.H. Knowledge, attitude and practice of antibiotics and their determinants in Eritrea: An urban population-based survey. BMJ Open 2021, 11, e046432. [Google Scholar] [CrossRef]
- Rahman, M.S.; Karamehic-Muratovic, A.; Baghbanzadeh, M.; Amrin, M.; Zafar, S.; Rahman, N.N.; Shirina, S.U.; Haque, U. Climate change and dengue fever knowledge, attitudes and practices in Bangladesh: A social media–based cross-sectional survey. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.S.; Overgaard, H.J.; Pientong, C.; Mayxay, M.; Ekalaksananan, T.; Aromseree, S.; Phanthanawiboon, S.; Zafar, S.; Shipin, O.; Paul, R.E.; et al. Knowledge, attitudes, and practices on climate change and dengue in Lao People’s Democratic Republic and Thailand. Environ. Res. 2021, 193, 110509. [Google Scholar] [CrossRef]
- Chen, H.; Boore, J.R. Translation and back-translation in qualitative nursing research: Methodological review. J. Clin. Nurs. 2010, 19, 234–239. [Google Scholar] [CrossRef]
- Saunders, B.; Sim, J.; Kingstone, T.; Baker, S.; Waterfield, J.; Bartlam, B.; Burroughs, H.; Jinks, C. Saturation in qualitative research: Exploring its conceptualization and operationalization. Qual. Quant. 2018, 52, 1893–1907. [Google Scholar] [CrossRef]
- Curry, L.A.; Nembhard, I.M.; Bradley, E.H. Qualitative and mixed methods provide unique contributions to outcomes research. Circulation 2009, 119, 1442–1452. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- O’connor, C.; Joffe, H. Intercoder reliability in qualitative research: Debates and practical guidelines. Int. J. Qual. Methods 2020, 19, 1609406919899220. [Google Scholar]
- Castleberry, A.; Nolen, A. Thematic analysis of qualitative research data: Is it as easy as it sounds? Curr. Pharm. Teach. Learn. 2018, 10, 807–815. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N = 362 (%) |
|---|---|
| Settlement | |
| Pastoralist | 183 (50.6%) |
| Agro-pastoralist | 179 (49.4%) |
| Sex | |
| Female | 257 (71.0%) |
| Male | 105 (29.0%) |
| Age group (in years) | |
| <30 | 141 (39.0%) |
| 31–40 | 112 (30.9%) |
| >40 | 109 (30.1%) |
| Marital status | |
| Single | 25 (6.9%) |
| Married | 327 (90.3%) |
| Divorced | 3 (0.8%) |
| Widowed | 7 (1.9%) |
| Educational status | |
| Illiterate | 235 (64.9%) |
| Primary school | 58 (16.0%) |
| Religious learning | 63 (17.4%) |
| College and above | 6 (1.7%) |
| Occupation | |
| Housewife | 212 (58.6%) |
| Government employee | 19 (5.2%) |
| Pastoralist | 56 (15.5%) |
| Farmer | 23 (6.4%) |
| Business | 52 (14.4%) |
| Numbers of person per household | |
| <5 | 129 (35.6%) |
| 6–8 | 121 (33.4%) |
| >8 | 112 (30.9%) |
| How long they have lived in the area | |
| <10 years | 153 (42.3%) |
| >10 years | 209 (57.7%) |
| Variable | N = 96 (%) |
|---|---|
| Sex | |
| Female | 46 (47.9%) |
| Male | 50 (53.1%) |
| Age | |
| 18–25 | 22 (22.9%) |
| 26–35 | 35 (36.5%) |
| >36 | 39 (40.6%) |
| Level of education | |
| Illiterate | 77 (80.2%) |
| Primary school | 2 (2.1%) |
| Secondary school | 6 (6.3%) |
| College and above | 11 (11.4%) |
| Occupation | |
| Farmer | 30 (31.2%) |
| Housewife | 22 (22.9%) |
| Government | 15 (15.6%) |
| Business owner | 12 (12.5%) |
| NGOs | 17 (17.8%) |
| Village of residence | |
| Bursaredo | 17 (17.7%) |
| Gabal | 16 (16.6%) |
| Malkasalah | 16 (16.6%) |
| Harsug | 15 (15.6%) |
| Dabafayd | 16 (16.6%) |
| Todob | 17 (17.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muhummed, A.M.; Alemu, A.; Maidane, Y.O.; Tschopp, R.; Hattendorf, J.; Vonaesch, P.; Zinsstag, J.; Cissé, G. Knowledge, Attitudes, and Practices of Rural Communities Regarding Antimicrobial Resistance and Climate Change in Adadle District, Somali Region, Ethiopia: A Mixed-Methods Study. Antibiotics 2024, 13, 292. https://doi.org/10.3390/antibiotics13040292
Muhummed AM, Alemu A, Maidane YO, Tschopp R, Hattendorf J, Vonaesch P, Zinsstag J, Cissé G. Knowledge, Attitudes, and Practices of Rural Communities Regarding Antimicrobial Resistance and Climate Change in Adadle District, Somali Region, Ethiopia: A Mixed-Methods Study. Antibiotics. 2024; 13(4):292. https://doi.org/10.3390/antibiotics13040292
Chicago/Turabian StyleMuhummed, Abdifatah Muktar, Ashenafi Alemu, Yahya Osman Maidane, Rea Tschopp, Jan Hattendorf, Pascale Vonaesch, Jakob Zinsstag, and Guéladio Cissé. 2024. "Knowledge, Attitudes, and Practices of Rural Communities Regarding Antimicrobial Resistance and Climate Change in Adadle District, Somali Region, Ethiopia: A Mixed-Methods Study" Antibiotics 13, no. 4: 292. https://doi.org/10.3390/antibiotics13040292