Buddhists Care: Examining the Impact of Religious Elements on Reducing Discriminatory Attitudes toward People Living with HIV/AIDS


Abstract
1. Introduction
2. Literature Review
2.1. HIV/AIDS-Related Discrimination and Advertising
2.2. Buddhist Compassion and HIV/AIDS-Related Discrimination
2.3. Buddhist Symbolic Elements in Advertising
2.4. Attitude Formation Model and Advertising against HIV/AIDS-Related Discrimination
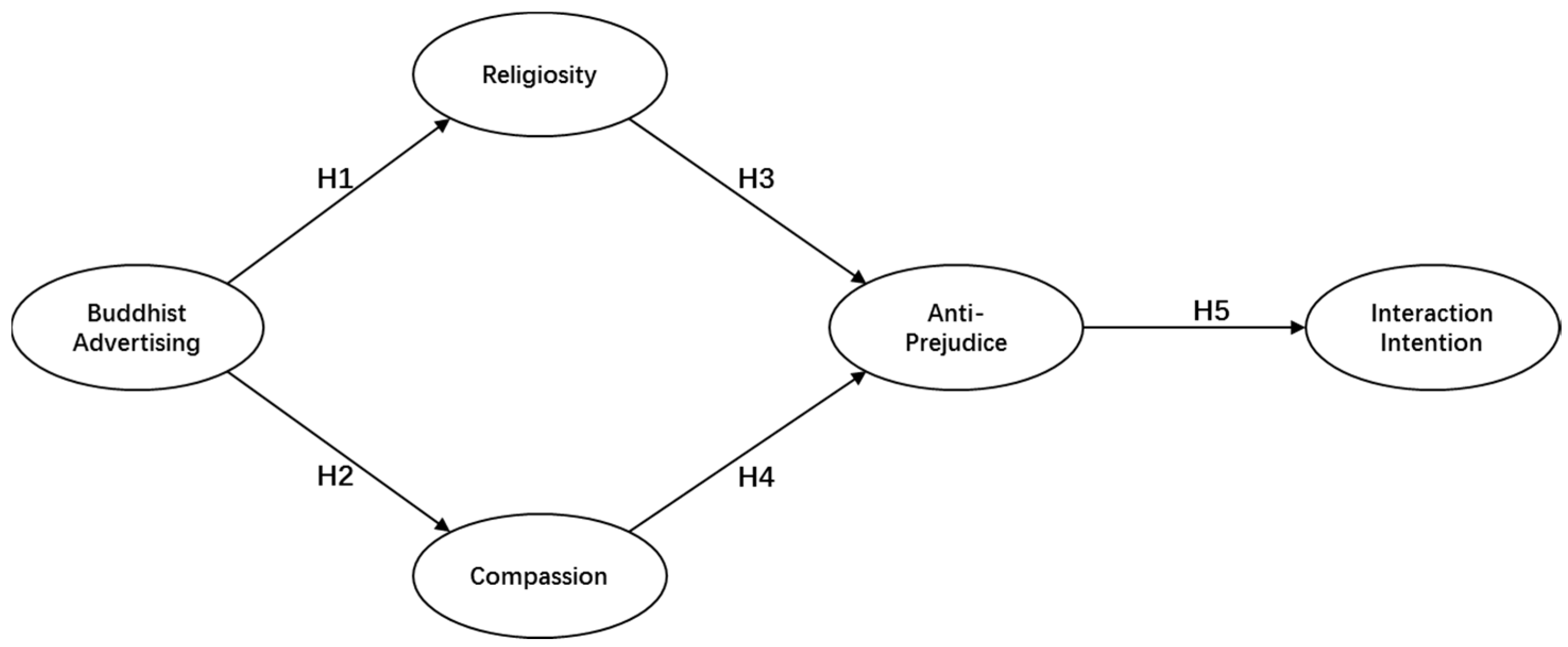
3. Hypotheses and Research Framework
4. Research Methods
4.1. Measurement Items
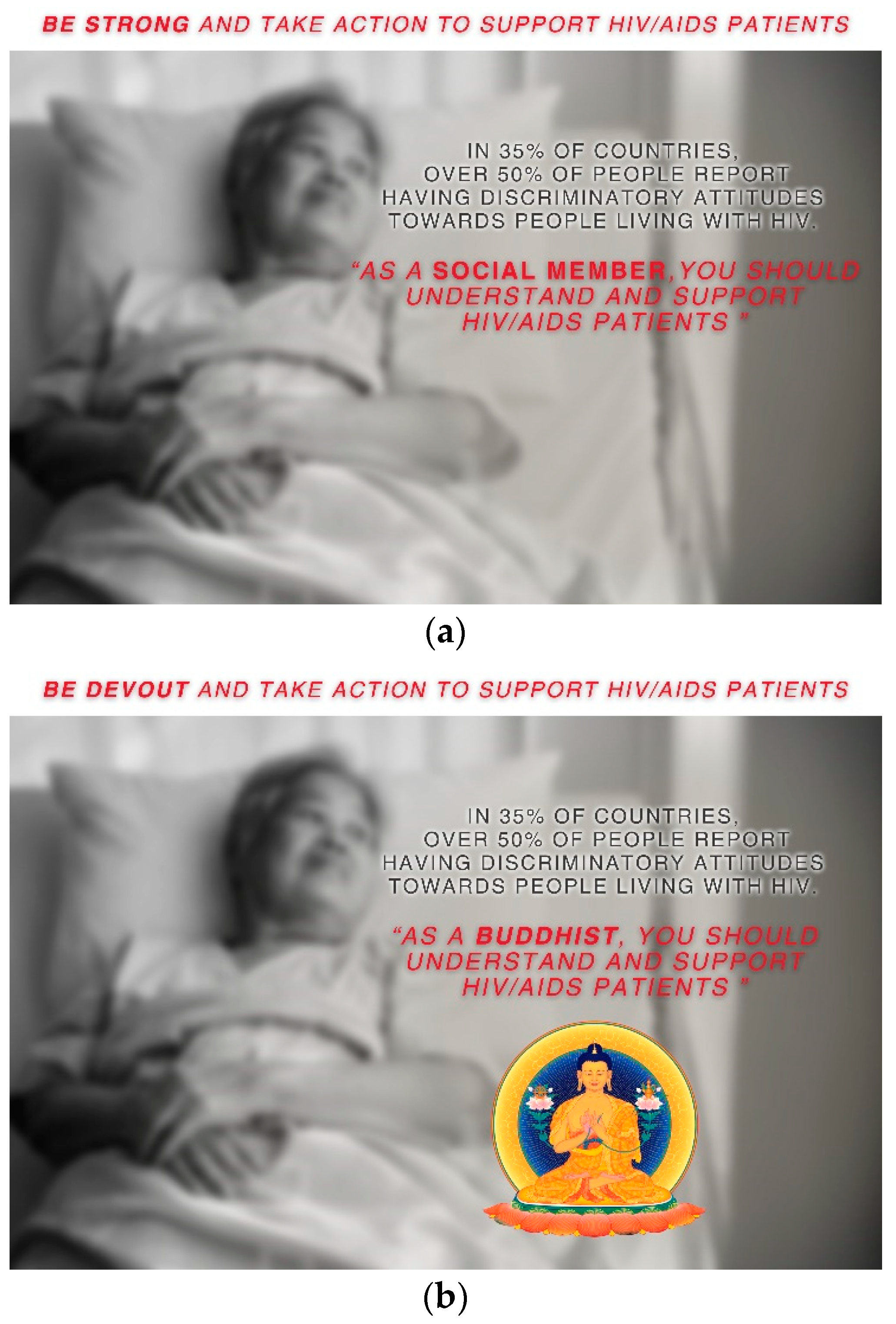
4.2. Stimuli and Pilot Study
4.3. Experiment Procedure
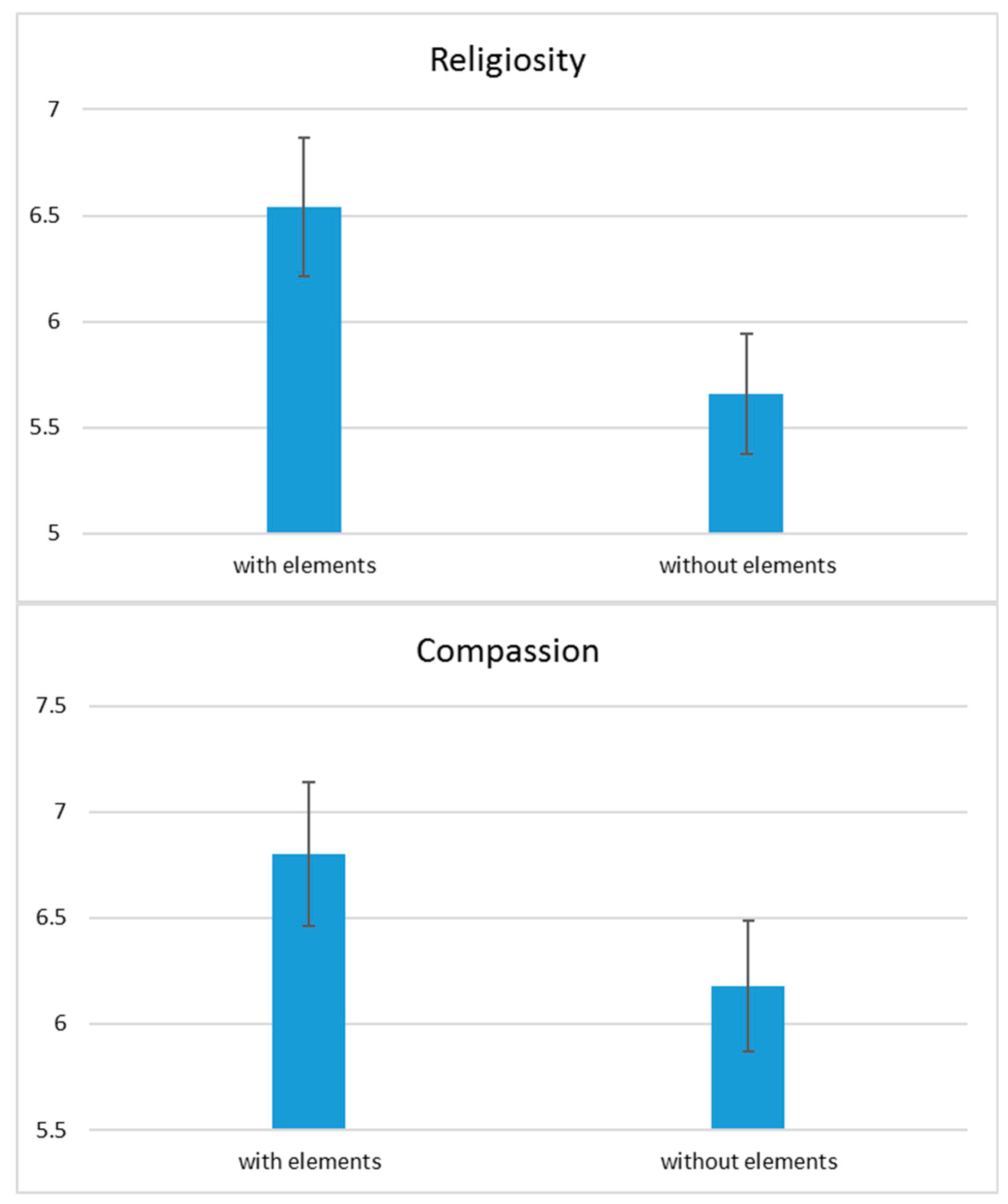
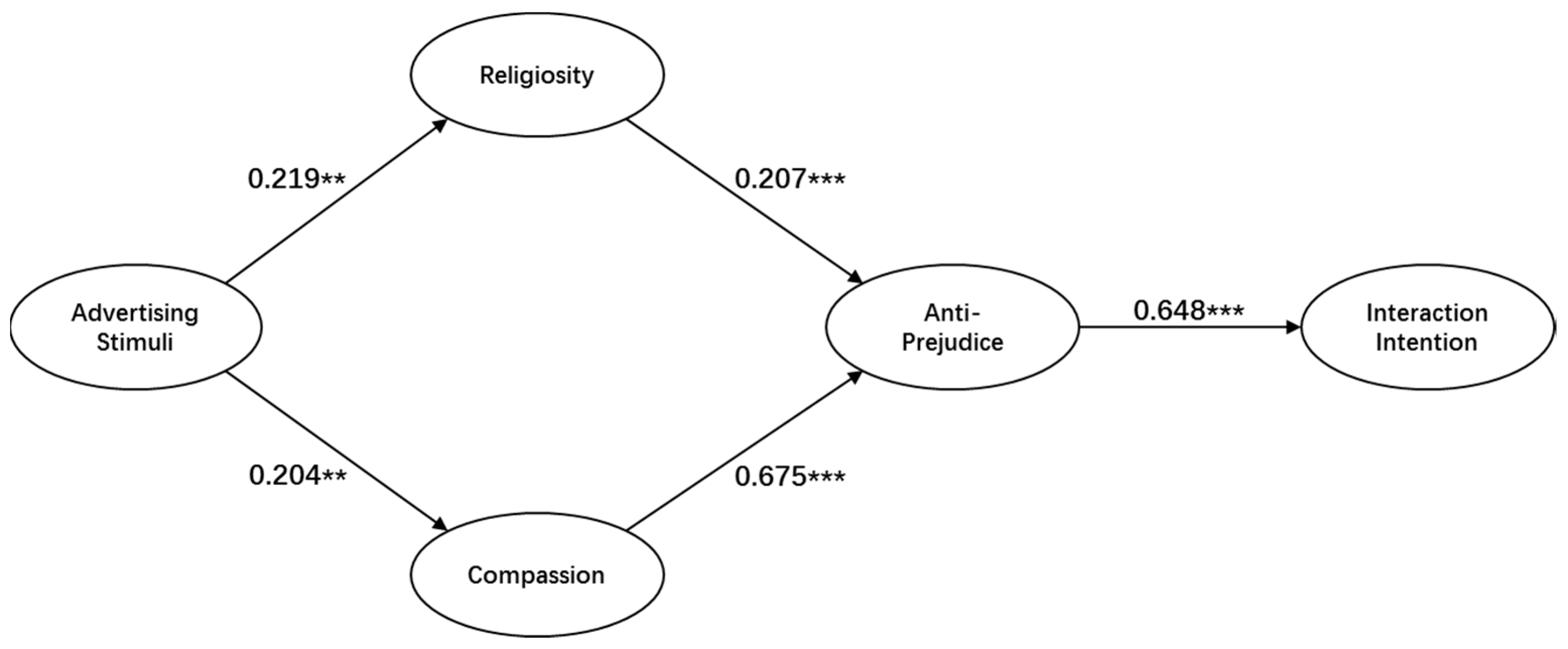
5. Findings
6. Discussion, Limitations and Future Research
Author Contributions
Funding
Conflicts of Interest
References
- Ackerson, Leland K., Shoba Ramanadhan, Monisha Arya, and Kasisomayajula Viswanath. 2012. Social Disparities, Communication Inequalities, and HIV/AIDS-Related Knowledge and Attitudes in India. AIDS and Behavior 16: 2072–81. [Google Scholar] [CrossRef] [PubMed]
- Alam, Syed Shah, Rohani Mohd, and Badrul Hisham. 2011. Is Religiosity an Important Determinant on Muslim Consumer Behaviour in Malaysia? Journal of Islamic Marketing 2: 83–96. [Google Scholar] [CrossRef]
- Anderson, Norman H. 1971. Integration Theory and Attitude Change. Psychological Review 78: 171–206. [Google Scholar] [CrossRef]
- Anderson, Moji, Gillian Elam, Sarah Gerver, Ijeoma Solarin, Kevin Fenton, and Philippa Easterbrook. 2008. HIV/AIDS-Related Stigma and Discrimination: Accounts of HIV-Positive Caribbean People in the United Kingdom. Social Science and Medicine 67: 790–98. [Google Scholar] [CrossRef] [PubMed]
- Aung, Steven K. H. 1996. Loving Kindness: The Essential Buddhist Contribution to Primary Care. Humane Health Care International 12: E12. [Google Scholar] [PubMed]
- Bagozzi, Richard P. 2006. A Field Investigation of Causal Relations among Cognitions, Affect, Intentions, and Behavior. Journal of Marketing Research 19: 562–83. [Google Scholar] [CrossRef]
- Blevins, John. 2015. Are Faith-Based Organizations Assets or Hindrances for Adolescents Living with HIV? They Are Both. Brown Journal of World Affairs 22: 25–38. [Google Scholar]
- Blevins, John. 2018. Christianity’s Role in United States Global Health and Development Policy. Christianity’s Role in United States Global Health and Development Policy. London: Routledge. [Google Scholar] [CrossRef]
- Blevins, John, Christoph Benn, and Sandra Thurman. 2016. Reflections on HIV-Related Experiences of Two Global Funding Mechanisms Supporting Religious Health Providers. The Review of Faith & International Affairs 14: 110–17. [Google Scholar] [CrossRef]
- Blevins, John B., Mohamed F. Jalloh, and David A. Robinson. 2019. Faith and Global Health Practice in Ebola and HIV Emergencies. American Journal of Public Health 109: 379–84. [Google Scholar] [CrossRef]
- Breckler, Steven J. 1984. Empirical Validation of Affect, Behavior, and Cognition as Distinct Components of Attitude. Journal of Personality and Social Psychology 47: 1191–205. [Google Scholar] [CrossRef]
- Bychkov, Oleg. 2019. ‘He Who Sees Does Not Desire to Imagine’: The Shifting Role of Art and Aesthetic Observation in Medieval Franciscan Theological Discourse in the Fourteenth Century. Religions 10: 205. [Google Scholar] [CrossRef]
- Chatters, Linda M. 2002. Religion and Health: Public Health Research and Practice. Annual Review of Public Health 21: 335–67. [Google Scholar] [CrossRef] [PubMed]
- Clobert, Magali, Vassilis Saroglou, and Kwang Kuo Hwang. 2015. Buddhist Concepts as Implicitly Reducing Prejudice and Increasing Prosociality. Personality and Social Psychology Bulletin 41: 513–25. [Google Scholar] [CrossRef] [PubMed]
- Clobert, Magali, Vassilis Saroglou, and Kwang Kuo Hwang. 2017. East Asian Religious Tolerance versus Western Monotheist Prejudice: The Role of (in)Tolerance of Contradiction. Group Processes and Intergroup Relations 20: 216–32. [Google Scholar] [CrossRef]
- Coursey, David H., and Sanjay K. Pandey. 2007. Public service motivation measurement: Testing an abridged version of Perry’s proposed scale. Administration & Society 39: 547–68. [Google Scholar] [CrossRef]
- Daly, Timothy M., and Rajan Nataraajan. 2015. Swapping Bricks for Clicks: Crowdsourcing Longitudinal Data on Amazon Turk. Journal of Business Research 68: 2603–9. [Google Scholar] [CrossRef]
- Davidson, Richard J., and Anne Harrington. 2002. Visions of Compassion: Western Scientists and Tibetan Buddhists Examine Human Nature. Oxford: Oxford University Press. [Google Scholar]
- Dlamini, Priscilla S., Thecla W. Kohi, Leana R. Uys, René Deliwe Phetlhu, Maureen L. Chirwa, Joanne R. Naidoo, William L. Holzemer, Minrie Greeff, and Lucy N. Makoae. 2007. Verbal and Physical Abuse and Neglect as Manifestations of HIV/AIDS Stigma in Five African Countries. Public Health Nursing 24: 389–99. [Google Scholar] [CrossRef] [PubMed]
- Dorić, Dragan, Emilija Nikolić-Dorić, Vesna Jevremović, and Jovan Mališić. 2009. On Measuring Skewness and Kurtosis. Quality and Quantity 43: 481–93. [Google Scholar] [CrossRef]
- Dotson, Michael J., and Eva M. Hyatt. 2002. Religious Symbols as Peripheral Cues in Advertising. Journal of Business Research 48: 63–68. [Google Scholar] [CrossRef]
- Engstrom, David. 2005. The Roles of Buddhist Temples in the Treatment of HIV/AIDS in Thailand. Journal of Sociology and Social Welfare 32: 5–22. [Google Scholar]
- Feldman, David B., Ian C. Fischer, and Robert A. Gressis. 2016. Does Religious Belief Matter for Grief and Death Anxiety? Experimental Philosophy Meets Psychology of Religion. Journal for the Scientific Study of Religion 55: 531–39. [Google Scholar] [CrossRef]
- Fishbein, Martin, and Icek Ajzen. 2011. Predicting and Changing Behavior. London: Psychology Press. [Google Scholar] [CrossRef]
- Fuqua, Joy V. 2002. Religion as a Social Determinant of Public Health. Cultural Studies 16: 650–72. [Google Scholar] [CrossRef]
- Genberg, Becky L., Surinda Kawichai, Alfred Chingono, Memory Sendah, Suwat Chariyalertsak, Kelika A. Konda, and David D. Celentano. 2008. Assessing HIV/AIDS Stigma and Discrimination in Developing Countries. AIDS and Behavior 12: 772–80. [Google Scholar] [CrossRef] [PubMed]
- Genberg, Becky L., Zdenek Hlavka, Kelika A. Konda, Suzanne Maman, Suwat Chariyalertsak, Alfred Chingono, Jessie Mbwambo, Precious Modiba, Heidi Van Rooyen, and David D. Celentano. 2009. A Comparison of HIV/AIDS-Related Stigma in Four Countries: Negative Attitudes and Perceived Acts of Discrimination towards People Living with HIV/AIDS. Social Science and Medicine 68: 2279–87. [Google Scholar] [CrossRef] [PubMed]
- Hackney, Charles H., and Glenn S. Sanders. 2003. Religiosity and Mental Health: A Meta–Analysis of Recent Studies: EBSCOhost. Journal for the Scientific Study of Religion 42: 43–56. [Google Scholar] [CrossRef]
- Hassan Fathelrahman Mansour, Ilham, and Dalia Mohammed Elzubier Diab. 2016. The Relationship between Celebrities’ Credibility and Advertising Effectiveness: The Mediation Role of Religiosity. Journal of Islamic Marketing 7: 148–66. [Google Scholar] [CrossRef]
- Hendriksen, Ellen Setsuko, Daniel Hlubinka, Suwat Chariyalertsak, Alfred Chingono, Glenda Gray, Jessie Mbwambo, Linda Richter, Michal Kulich, and Thomas J. Coates. 2009. Keep Talking about It: HIV/AIDS-Related Communication and Prior HIV Testing in Tanzania, Zimbabwe, South Africa, and Thailand. AIDS and Behavior 13: 1213–21. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hutchinson, Paul Lawrence, Xoli Mahlalela, and Josh Yukich. 2007. Mass Media, Stigma, and Disclosure of HIV Test Results: Multilevel Analysis in the Eastern Cape, South Africa. AIDS Education and Prevention 19: 489–510. [Google Scholar] [CrossRef] [PubMed]
- Idler, Ellen L. 2015. Religion as a Social Determinant of Public Health. New York: Oxford University Press. [Google Scholar] [CrossRef]
- Jensen-Fangel, Søren, Lars Pedersen, Court Pedersen, Carsten S. Larsen, Palle Tauris, Axel Møller, Henrik T. Sørensen, and Niels Obel. 2004. Low Mortality in HIV-Infected Patients Starting Highly Active Antiretroviral Therapy: A Comparison with the General Population. Aids 18: 89–97. [Google Scholar] [CrossRef]
- Johnny, Leanne, and Claudia Mitchell. 2006. ‘live and Let Live’: An Analysis of HIV/AIDS-Related Stigma and Discrimination in International Campaign Posters. Journal of Health Communication 11: 755–67. [Google Scholar] [CrossRef]
- Khuat, Thu Hong, Thi Van Anh Nguyen, and Jessica Ogden. 2004. Understanding HIV and AIDS-Related Stigma and Discrimination in Vietnam. Hanoi: Institute for Social Development Studies and International Center for Research on Women. [Google Scholar]
- Kitara, David Lagoro, and Judith Aloyo. 2012. HIV/AIDS Stigmatization, the Reason for Poor Access to HIV Counseling and Testing (HCT) among the Youths in Gulu (Uganda). African Journal of Infectious Diseases 6: 12–20. [Google Scholar] [CrossRef] [PubMed]
- Kittikorn, Nilmanat, Annette F. Street, and Jeanine Blackford. 2006. Managing Shame and Stigma: Case Studies of Female Carers of People with AIDS in Southern Thailand. Qualitative Health Research 16: 1286–301. [Google Scholar] [CrossRef] [PubMed]
- Li, Li, Zunyou Wu, Yu Zhao, Chunqing Lin, Roger Detels, and Sheng Wu. 2006. Using case vignettes to measure HIV-related stigma among health professionals in China. International Journal of Epidemiology 36: 178–84. [Google Scholar] [CrossRef] [PubMed]
- Mair, Victor H. 2006. Buddhism and the Rise of the Written Vernacular in East Asia: The Making of National Languages. The Journal of Asian Studies 53: 707. [Google Scholar] [CrossRef]
- Mair, Victor H., and John Blofeld. 2006. Bodhisattva of Compassion: The Mystical Tradition of Kuan Yin. The Journal of Asian Studies 39: 161. [Google Scholar] [CrossRef]
- Malamuth, Neil M., Scott Haber, and Seymour Feshbach. 1980. Testing Hypotheses Regarding Rape: Exposure to Sexual Violence, Sex Differences, and the ‘Normality’ of Rapists. Journal of Research in Personality 14: 121–37. [Google Scholar] [CrossRef]
- Manoj, Sharma. 2015. Measuring Advertising Effectiveness (3 Methods). Hillsdale: L. Erlbaum Associates. [Google Scholar]
- Mcgrath, Pam. 2007. Buddhist Spirituality—a Compassionate Perspective on Hospice Care. Mortality 3: 251–63. [Google Scholar] [CrossRef]
- Miller, Tracy. 2015. Of Palaces and Pagodas: Palatial Symbolism in the Buddhist Architecture of Early Medieval Cave as Infinite Palace: South Asian Precedents and East. Frontiers of History in China 10: 222–63. [Google Scholar] [CrossRef]
- Min Han, Chen. 2004. Testing the Role of Country Image in Consumer Choice Behaviour. European Journal of Marketing 24: 24–40. [Google Scholar] [CrossRef]
- Morwitz, Vicki G., and Gavan J. Fitzsimons. 2004. The mere-measurement effect: Why does measuring intentions change actual behavior? Journal of Consumer Psychology 14: 64–74. [Google Scholar] [CrossRef]
- Moyo, Philani, and Charlene Keir Ying-Ling. 2014. An Assessment of the Role of Faith-Based Organisations in HIV/AIDS Mitigation, Treatment and Care: The Case of Buddhist Compassion Relief in KwaZulu Natal, South Africa. Mediterranean Journal of Social Sciences 5: 345–51. [Google Scholar] [CrossRef]
- Muralidharan, Sidharth, Carrie La Ferle, and Sanjukta Pookulangara. 2018. Studying the Impact of Religious Symbols on Domestic Violence Prevention in India: Applying the Theory of Reasoned Action to Bystanders’ Reporting Intentions. International Journal of Advertising 37: 609–32. [Google Scholar] [CrossRef]
- Nardella, Carlo. 2012. Religious Symbols in Italian Advertising: Symbolic Appropriation and the Management of Consent. Journal of Contemporary Religion 27: 217–40. [Google Scholar] [CrossRef]
- Naseri, Abbas, and Ezhar Tamam. 2012. Impact of Islamic Religious Symbol In Producing Favorable Attitude Toward Advertisement. Revista de Administratie Publica Si Politici Sociale 1: 61–77. [Google Scholar]
- Nyblade, Laura, and Kerry MacQuarrie. 2006. Can We Measure HIV/AIDS-Related Stigma and Discrimination? Current Knowledge about Quantifying Stigma in Developing Countries. Washington: Futures Group POLICY Project. [Google Scholar]
- Parker, Richard, and Peter Aggleton. 2003. HIV and AIDS-Related Stigma and Discrimination: A Conceptual Framework and Implications for Action. Social Science & Medicine 57: 13–24. [Google Scholar]
- Patry Leidy, Denise. 1252. The Art of Buddhism. An Introduction to Its History and Meaning. Boston: Shambhala. [Google Scholar]
- Peltzer, Karl, Warren Parker, Musawenkosi Mabaso, Elias Makonko, Khangelani Zuma, and Shandir Ramlagan. 2012. Impact of National HIV and AIDS Communication Campaigns in South Africa to Reduce HIV Risk Behaviour. The Scientific World Journal 2012: 384608. [Google Scholar] [CrossRef] [PubMed]
- Putney, Snell, and Russell Middleton. 1961. Dimensions and Correlates of Religious Ideologies. Social Forces 39: 285–90. [Google Scholar] [CrossRef]
- Rand, David G., Anna Dreber, Omar S. Haque, Rob J. Kane, Martin A. Nowak, and Sarah Coakley. 2014. Religious Motivations for Cooperation: An Experimental Investigation Using Explicit Primes. Religion, Brain and Behavior 4: 31–48. [Google Scholar] [CrossRef]
- Ritter, Ryan S., and Jesse Lee Preston. 2013. Representations of Religious Words: Insights for Religious Priming Research. Journal for the Scientific Study of Religion 52: 494–507. [Google Scholar] [CrossRef]
- Sayles, Jennifer N., Mitchell D. Wong, Janni J. Kinsler, David Martins, and William E. Cunningham. 2009. The Association of Stigma with Self-Reported Access to Medical Care and Antiretroviral Therapy Adherence in Persons Living with HIV/AIDS. Journal of General Internal Medicine 24: 1101. [Google Scholar] [CrossRef]
- Scalvini, Marco. 2010. Glamorizing Sick Bodies: How Commercial Advertising Has Changed the Representation of HIV/AIDS. Social Semiotics 20: 219–31. [Google Scholar] [CrossRef]
- Schroeder, John William. 2002. Visions of Compassion: Western Scientists Adn Tibetan BUddhists Examine Human Nature. New York: Oxford University Press. [Google Scholar]
- Shiu, Henry, and Leah Stokes. 2008. Buddhist Animal Release Practices: Historic, Environmental, Public Health And Economic Concerns. Contemporary Buddhism 9: 181–96. [Google Scholar] [CrossRef]
- Songwathana, Praneed, and Lenore Manderson. 2001. Stigma and Rejection: Living with AIDS in Villages in Southern Thailand. Medical Anthropology: Cross Cultural Studies in Health and Illness 20: 1–23. [Google Scholar] [CrossRef] [PubMed]
- Song, Yao, and Zhenzhen Qin. 2019. Towards the Beauty of Buddhism: The Development and Validation of a Buddhist Aesthetics Scale. Religions 10: 343. [Google Scholar] [CrossRef]
- St Lawrence, Janet S., Brenda A. Husfeldt, Jeffrey A. Kelly, Harold V. Hood, and Steve Smith. 1990. The Stigma of AIDS. Journal of Homosexuality 19: 85–102. [Google Scholar] [CrossRef] [PubMed]
- Stewart, Neil, Christoph Ungemach, Adam J. L. Harris, Daniel M. Bartels, Gabriele Paolacci, and Jesse Chandler. 2015. The Average Laboratory Samples a Population of 7,300 Amazon Mechanical Turk Workers The Size of the MTurk Population. Judgment and Decision Making 10: 479–91. [Google Scholar]
- Suki, Norazah Mohd. 2013. Green Awareness Effects on Consumers’ Purchasing Decision: Some Insights from Malaysia. International Journal of Asia-Pacific Studies 9: 49–63. [Google Scholar]
- Taylor, Valerie A., Diane Halstead, and Paula J. Haynes. 2010. Consumer Responses to Christian Religious Symbols in Advertising. Journal of Advertising 39: 79–92. [Google Scholar] [CrossRef]
- Than, Phung Quoc Tat, Bach Xuan Tran, Cuong Tat Nguyen, Nu Thi Truong, Thao Phuong Thi Thai, Carl A. Latkin, Cyrus S. H. Ho, and Roger C. M. Ho. 2019. Understanding Global HIV Stigma and Discrimination: Are Contextual Factors Sufficiently Studied? International Journal of Environmental Research and Public Health 16: 1899. [Google Scholar]
- Tran, Bach Xuan, Hai Thanh Phan, Carl A. Latkin, Huong Lan Thi Nguyen, Chi Linh Hoang, Cyrus S. H. Ho, and Roger Ho. 2019. Stigma against patients with HIV/AIDS in the rapid expansion of antiretroviral treatment in large drug injection-driven HIV epidemics of Vietnam. Harm Reduction Journal 16: 6. [Google Scholar]
- UNAIDS. 2015. On the Fast-Track to End AIDS by 2030: Focus on Location and Population. Available online: https://www.unaids.org/sites/default/files/media_asset/WAD2015_report_en_part01.pdf (accessed on 1 May 2019).
- UNAIDS. 2017. UNAIDS 2017. Available online: https://www.unaids.org/sites/default/files/media_asset/20170720_Data_book_2017_en.pdf (accessed on 1 May 2019).
- UNAIDS. 2018. UNAIDS DATA 2018. Available online: https://www.unaids.org/sites/default/files/media_asset/unaids-data-2018_en.pdf (accessed on 1 May 2019).
- Unger, Lynette S. 1995. Observations—A Cross-Cultural-Study on the Affect-Based Model of Humor in Advertising. Journal of Advertising Research 35: 66–71. [Google Scholar]
- van Dyk, Alta C. 2017. How Do Clergy in the Afrikaans-Speaking Churches Deal with Sexuality and HIV Prevention in Young People? Is the Message Clear? Verbum et Ecclesia 38: 1–9. [Google Scholar] [CrossRef][Green Version]
- Watts, Jonathan S., and Yoshiharu Tomatsu. 2012. Buddhist Care for the Dying and Bereaved. Needham Heights: Simon and Schuster. [Google Scholar]
- Winchester, Daniel. 2017. ‘A Part of Who I Am’: Material Objects as ‘Plot Devices’ in the Formation of Religious Selves. Journal for the Scientific Study of Religion 56: 83–103. [Google Scholar] [CrossRef]
- World Health Organization, and Unicef. 2015. GLOBAL HIV/AIDS RESPONSE Epidemic Update and Health Sector Progress towards Universal Access. [Google Scholar]
- Yeung, Gustav K. K., and Wai Yin Chow. 2010. ‘To Take up Your Own Responsibility’: The Religiosity of Buddhist Adolescents in Hong Kong. International Journal of Children’s Spirituality 15: 5–23. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sources | Items | Cronbach’s Alpha (α) |
|---|---|---|
| Religiosity (Putney and Middleton 1961) | Buddhism forms an important basis for the kind of person I want to be My ideas on Buddhism have a big influence on my view in other areas Were I to think about Buddhism differently, my whole life would be very different I often think about Buddhist matters Buddhism is one of the most important parts of my philosophy of life | 0.896 |
| Compassion (Coursey and Pandey 2007) | It is difficult for me to contain my feelings when I see people in illness I am often reminded by daily events about how dependent we are on one another I have compassion for people in need who are unwilling to take the first step to help themselves | 0.824 |
| Anti-Prejudice (Malamuth et al. 1980) | HIV people deserve sympathy and understanding HIV people deserve the best medical care possible HIV has been traumatic for affected people HIV people have a lot of pain and suffering HIV people are safe to others | 0.880 |
| Interaction Intention (Li et al. 2006) | If I met HIV people, I am willing to strike up a conversation with them I would continue the friendship with a HIV-affected friend I am willing to work in the same office with HIV people | 0.914 |
| Constructs | Mean | SD | RE | COM | ANT | INT |
|---|---|---|---|---|---|---|
| Religiosity (RE) | 6.10 | 1.92 | 1.000 | |||
| Compassion (COM) | 6.49 | 1.82 | 0.518 *** | 1.000 | ||
| Anti-Prejudice (ANT) | 7.10 | 1.86 | 0.505 *** | 0.779 *** | 1.000 | |
| Interaction Intention (INT) | 6.68 | 1.96 | 0.522 *** | 0.595 *** | 0.672 *** | 1.000 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, Y.; Qin, Z. Buddhists Care: Examining the Impact of Religious Elements on Reducing Discriminatory Attitudes toward People Living with HIV/AIDS. Religions 2019, 10, 409. https://doi.org/10.3390/rel10070409
Song Y, Qin Z. Buddhists Care: Examining the Impact of Religious Elements on Reducing Discriminatory Attitudes toward People Living with HIV/AIDS. Religions. 2019; 10(7):409. https://doi.org/10.3390/rel10070409
Chicago/Turabian StyleSong, Yao, and Zhenzhen Qin. 2019. "Buddhists Care: Examining the Impact of Religious Elements on Reducing Discriminatory Attitudes toward People Living with HIV/AIDS" Religions 10, no. 7: 409. https://doi.org/10.3390/rel10070409
APA StyleSong, Y., & Qin, Z. (2019). Buddhists Care: Examining the Impact of Religious Elements on Reducing Discriminatory Attitudes toward People Living with HIV/AIDS. Religions, 10(7), 409. https://doi.org/10.3390/rel10070409