Urinary Excretion of N1-methyl-2-pyridone-5-carboxamide and N1-methylnicotinamide in Renal Transplant Recipients and Donors

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection and Measurements
2.3. Assessment of 2Py and N1-MN Excretion
2.4. Statistical Analysis
3. Results
3.1. Excretion of 2Py in Kidney Donors and RTR
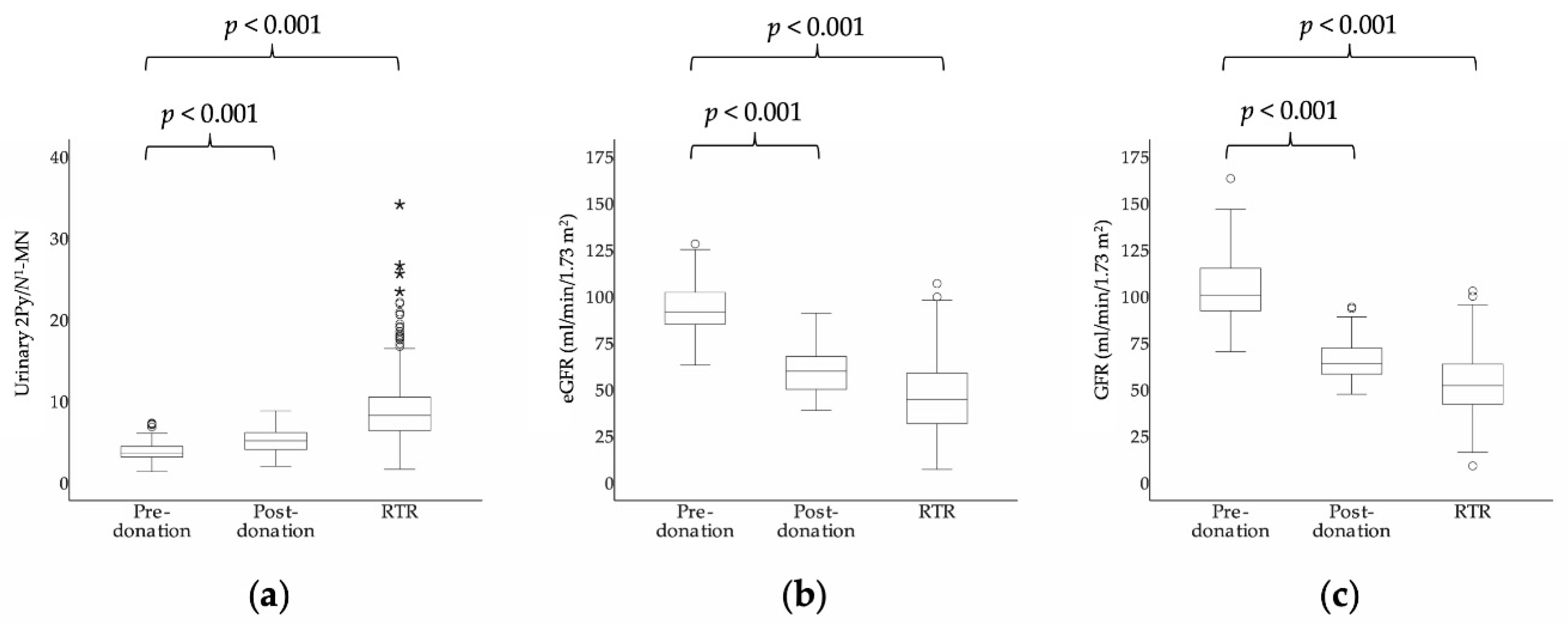
3.2. Excretion of 2Py and N1-MN before and after Kidney Donation in Kidney Donors
3.3. Associations of Urinary 2Py/N1-MN with Kidney Function
3.4. Characteristics and Associations with Urinary 2Py/N1-MN in RTR
3.5. Determinants of Urinary 2Py/N1-MN in RTR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bogan, K.L.; Brenner, C. Nicotinic acid, nicotinamide, and nicotinamide riboside: A molecular evaluation of NAD+ precursor vitamins in human nutrition. Annu. Rev. Nutr. 2008, 28, 115–130. [Google Scholar] [CrossRef] [Green Version]
- Soldi, L.R.; Maltos, A.L.; da Cunha, D.F.; Portari, G.V. Correlation Between First Morning Single Void and 24-Hour Urines: The Reliability to Quantify Niacin Status. Med. Sci. Monit. Basic Res. 2018, 24, 206–209. [Google Scholar] [CrossRef] [PubMed]
- EFSA NDA Panel. Scientific Opinion on Dietary Reference Values for niacin. EFSA J. 2014, 12, 3759. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization and United Nations High Commissions for Refugees. Pellagra and Its Prevention and Control in Major Emergencies; WHO/NHD/00.10.2000. Available online: http://apps.who.int/iris/bitstream/handle/10665/66704/WHO_NHD_00.10.pdf?sequence=1&isAllowed=y (accessed on 26 March 2018).
- Menon, R.M.; Gonzalez, M.A.; Adams, M.H.; Tolbert, D.S.; Leu, J.H.; Cefali, E.A. Effect of the rate of niacin administration on the plasma and urine pharmacokinetics of niacin and its metabolites. J. Clin. Pharmacol. 2007, 47, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Pissios, P. Nicotinamide N-Methyltransferase: More Than a Vitamin B3 Clearance Enzyme. Trends Endocrinol. Metab. 2017, 28, 340–353. [Google Scholar] [CrossRef] [Green Version]
- Jacob, R.A.; Swendseid, M.E.; McKee, R.W.; Fu, C.S.; Clemens, R.A. Biochemical markers for assessment of niacin status in young men: Urinary and blood levels of niacin metabolites. J. Nutr. 1989, 119, 591–598. [Google Scholar] [CrossRef]
- Delange, D.J.; Joubert, C.P. Assessment of Nicotinic Acid Status of Population Groups. Am. J. Clin. Nutr. 1964, 15, 169–174. [Google Scholar] [CrossRef]
- Hegyi, J.; Schwartz, R.A.; Hegyi, V. Pellagra: Dermatitis, dementia, and diarrhea. Int. J. Dermatol. 2004, 43, 1–5. [Google Scholar] [CrossRef]
- Strohm, D.; Bechthold, A.; Isik, N.; Leschik-Bonnet, E.; Heseker, H. Revised reference values for the intake of thiamin (vitamin B1), riboflavin (vitamin B2), and niacin. NFS J. 2016, 3, 20–24. [Google Scholar] [CrossRef] [Green Version]
- Shibata, K.; Matsuo, H. Correlation between niacin equivalent intake and urinary excretion of its metabolites, N’-methylnicotinamide, N’-methyl-2-pyridone-5-carboxamide, and N’-methyl-4-pyridone-3-carboxamide, in humans consuming a self-selected food. Am. J. Clin. Nutr. 1989, 50, 114–119. [Google Scholar] [CrossRef]
- Deen, C.P.J.; van der Veen, A.; van Faassen, M.; Minovic, I.; Gomes-Neto, A.W.; Geleijnse, J.M.; Borgonjen-van den Berg, K.J.; Kema, I.P.; Bakker, S.J.L. Urinary Excretion of N(1)-Methylnicotinamide, as a Biomarker of Niacin Status, and Mortality in Renal Transplant Recipients. J. Clin. Med. 2019, 8, 1948. [Google Scholar] [CrossRef] [Green Version]
- Maiza, A.; Waldek, S.; Ballardie, F.W.; Daley-Yates, P.T. Estimation of renal tubular secretion in man, in health and disease, using endogenous N-1-methylnicotinamide. Nephron 1992, 60, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Muller, F.; Sharma, A.; Konig, J.; Fromm, M.F. Biomarkers for In Vivo Assessment of Transporter Function. Pharmacol. Rev. 2018, 70, 246–277. [Google Scholar] [CrossRef] [Green Version]
- van den Berg, E.; Engberink, M.F.; Brink, E.J.; van Baak, M.A.; Joosten, M.M.; Gans, R.O.; Navis, G.; Bakker, S.J. Dietary acid load and metabolic acidosis in renal transplant recipients. Clin. J. Am. Soc. Nephrol. 2012, 7, 1811–1818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Berg, E.; Engberink, M.F.; Brink, E.J.; van Baak, M.A.; Gans, R.O.; Navis, G.; Bakker, S.J. Dietary protein, blood pressure and renal function in renal transplant recipients. Br. J. Nutr. 2013, 109, 1463–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Berg, E.; Pasch, A.; Westendorp, W.H.; Navis, G.; Brink, E.J.; Gans, R.O.; van Goor, H.; Bakker, S.J. Urinary sulfur metabolites associate with a favorable cardiovascular risk profile and survival benefit in renal transplant recipients. J. Am. Soc. Nephrol. 2014, 25, 1303–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siebelink, E.; Geelen, A.; de Vries, J.H. Self-reported energy intake by FFQ compared with actual energy intake to maintain body weight in 516 adults. Br. J. Nutr. 2011, 106, 274–281. [Google Scholar] [CrossRef] [Green Version]
- Streppel, M.T.; de Vries, J.H.; Meijboom, S.; Beekman, M.; de Craen, A.J.; Slagboom, P.E.; Feskens, E.J. Relative validity of the food frequency questionnaire used to assess dietary intake in the Leiden Longevity Study. Nutr. J. 2013, 12, 75. [Google Scholar] [CrossRef] [Green Version]
- Dutch Nutrient Databank. NEVO Table 2006; Voorlichtingsbureau Voor de Voeding: The Hague, The Netherlands, 2006. [Google Scholar]
- Eisenga, M.F.; Kieneker, L.M.; Soedamah-Muthu, S.S.; van den Berg, E.; Deetman, P.E.; Navis, G.J.; Gans, R.O.; Gaillard, C.A.; Bakker, S.J.; Joosten, M.M. Urinary potassium excretion, renal ammoniagenesis, and risk of graft failure and mortality in renal transplant recipients. Am. J. Clin. Nutr. 2016, 104, 1703–1711. [Google Scholar] [CrossRef]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef] [Green Version]
- Salvador, C.L.; Hartmann, A.; Asberg, A.; Bergan, S.; Rowe, A.D.; Morkrid, L. Estimating Glomerular Filtration Rate in Kidney Transplant Recipients: Comparing a Novel Equation with Commonly Used Equations in this Population. Transplant. Direct 2017, 3, e332. [Google Scholar] [CrossRef] [PubMed]
- Apperloo, A.J.; de Zeeuw, D.; Donker, A.J.; de Jong, P.E. Precision of glomerular filtration rate determinations for long-term slope calculations is improved by simultaneous infusion of 125I-iothalamate and 131I-hippuran. J. Am. Soc. Nephrol. 1996, 7, 567–572. [Google Scholar] [PubMed]
- Bouma, G.; van Faassen, M.; Kats-Ugurlu, G.; de Vries, E.G.; Kema, I.P.; Walenkamp, A.M. Niacin (Vitamin B3) Supplementation in Patients with Serotonin-Producing Neuroendocrine Tumor. Neuroendocrinology 2016, 103, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, B.E.; Sharif, T.; Martell, E.; Dai, C.; Kim, Y.; Lee, P.W.; Gujar, S.A. NAD(+) salvage pathway in cancer metabolism and therapy. Pharmacol. Res. 2016, 114, 274–283. [Google Scholar] [CrossRef]
- Badawy, A.A. Kynurenine Pathway of Tryptophan Metabolism: Regulatory and Functional Aspects. Int. J. Tryptophan Res. 2017, 10, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Wozniacka, A.; Wieczorkowska, M.; Gebicki, J.; Sysa-Jedrzejowska, A. Topical application of 1-methylnicotinamide in the treatment of rosacea: A pilot study. Clin. Exp. Dermatol. 2005, 30, 632–635. [Google Scholar] [CrossRef]
- Kremer, J.I.; Gompel, K.; Bakuradze, T.; Eisenbrand, G.; Richling, E. Urinary Excretion of Niacin Metabolites in Humans after Coffee Consumption. Mol. Nutr. Food Res. 2018, 62, e1700735. [Google Scholar] [CrossRef] [Green Version]
- Nasseri, K.; Daley-Yates, P.T. A comparison of N-1-methylnicotinamide clearance with 5 other markers of renal function in models of acute and chronic renal failure. Toxicol. Lett. 1990, 53, 243–245. [Google Scholar] [CrossRef]
- Weber, W.; Toussaint, S.; Looby, M.; Nitz, M.; Kewitz, H. System analysis in multiple dose kinetics: Evidence for saturable tubular reabsorption of the organic cation N1-methylnicotinamide in humans. J. Pharm. Biopharm. 1991, 19, 553–574. [Google Scholar] [CrossRef]
- Duranton, F.; Cohen, G.; De Smet, R.; Rodriguez, M.; Jankowski, J.; Vanholder, R.; Argiles, A.; European Uremic Toxin Work Group. Normal and pathologic concentrations of uremic toxins. J. Am. Soc. Nephrol. 2012, 23, 1258–1270. [Google Scholar] [CrossRef] [Green Version]
- Vanholder, R.; Van Laecke, S.; Glorieux, G. What is new in uremic toxicity? Pediatr. Nephrol. 2008, 23, 1211–1221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenglet, A.; Liabeuf, S.; Bodeau, S.; Louvet, L.; Mary, A.; Boullier, A.; Lemaire-Hurtel, A.S.; Jonet, A.; Sonnet, P.; Kamel, S.; et al. N-methyl-2-pyridone-5-carboxamide (2PY)-Major Metabolite of Nicotinamide: An Update on an Old Uremic Toxin. Toxins 2016, 8, 339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tayama, Y.; Sugihara, K.; Sanoh, S.; Miyake, K.; Kitamura, S.; Ohta, S. Developmental changes of aldehyde oxidase activity and protein expression in human liver cytosol. Drug Metab. Pharm. 2012, 27, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Garattini, E.; Terao, M. The role of aldehyde oxidase in drug metabolism. Expert Opin. Drug Metab. Toxicol. 2012, 8, 487–503. [Google Scholar] [CrossRef] [PubMed]
- Pryde, D.C.; Dalvie, D.; Hu, Q.; Jones, P.; Obach, R.S.; Tran, T.D. Aldehyde oxidase: An enzyme of emerging importance in drug discovery. J. Med. Chem. 2010, 53, 8441–8460. [Google Scholar] [CrossRef]
- Chen, C.H.; Ferreira, J.C.; Gross, E.R.; Mochly-Rosen, D. Targeting aldehyde dehydrogenase 2: New therapeutic opportunities. Physiol. Rev. 2014, 94, 1–34. [Google Scholar] [CrossRef] [Green Version]
- Xu, F.; Chen, Y.G.; Xue, L.; Li, R.J.; Zhang, H.; Bian, Y.; Zhang, C.; Lv, R.J.; Feng, J.B.; Zhang, Y. Role of aldehyde dehydrogenase 2 Glu504lys polymorphism in acute coronary syndrome. J. Cell Mol. Med. 2011, 15, 1955–1962. [Google Scholar] [CrossRef] [Green Version]
- Pan, C.; Xing, J.H.; Zhang, C.; Zhang, Y.M.; Zhang, L.T.; Wei, S.J.; Zhang, M.X.; Wang, X.P.; Yuan, Q.H.; Xue, L.; et al. Aldehyde dehydrogenase 2 inhibits inflammatory response and regulates atherosclerotic plaque. Oncotarget 2016, 7, 35562–35576. [Google Scholar] [CrossRef] [Green Version]
- Graessler, J.; Fischer, S. The dual substrate specificity of aldehyde oxidase 1 for retinal and acetaldehyde and its role in ABCA1 mediated efflux. Horm. Metab. Res. 2007, 39, 775–776. [Google Scholar] [CrossRef]
- Sigruener, A.; Buechler, C.; Orso, E.; Hartmann, A.; Wild, P.J.; Terracciano, L.; Roncalli, M.; Bornstein, S.R.; Schmitz, G. Human aldehyde oxidase 1 interacts with ATP-binding cassette transporter-1 and modulates its activity in hepatocytes. Horm. Metab. Res. 2007, 39, 781–789. [Google Scholar] [CrossRef]
- Chini, C.C.S.; Tarrago, M.G.; Chini, E.N. NAD and the aging process: Role in life, death and everything in between. Mol. Cell Endocrinol. 2017, 455, 62–74. [Google Scholar] [CrossRef] [PubMed]
- Canto, C.; Menzies, K.J.; Auwerx, J. NAD(+) Metabolism and the Control of Energy Homeostasis: A Balancing Act between Mitochondria and the Nucleus. Cell Metab. 2015, 22, 31–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slominska, E.M.; Smolenski, R.T.; Szolkiewicz, M.; Leaver, N.; Rutkowski, B.; Simmonds, H.A.; Swierczynski, J. Accumulation of plasma N-methyl-2-pyridone-5-carboxamide in patients with chronic renal failure. Mol. Cell Biochem. 2002, 231, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, B.; Slominska, E.; Szolkiewicz, M.; Smolenski, R.T.; Striley, C.; Rutkowski, P.; Swierczynski, J. N-methyl-2-pyridone-5-carboxamide: A novel uremic toxin? Kidney Int. 2003, 63, S19–S21. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, H.; Ishikawa, A.; Yoshitake, Y.; Kodama, N.; Nishimuta, M.; Fukuwatari, T.; Shibata, K. Diurnal variations in human urinary excretion of nicotinamide catabolites: Effects of stress on the metabolism of nicotinamide. Am. J. Clin. Nutr. 2003, 77, 406–410. [Google Scholar] [CrossRef] [Green Version]
- Orlando, R.; Floreani, M.; Napoli, E.; Padrini, R.; Palatini, P. Renal clearance of N(1)-methylnicotinamide: A sensitive marker of the severity of liver dysfunction in cirrhosis. Nephron 2000, 84, 32–39. [Google Scholar] [CrossRef]
- Fu, C.S.; Swendseid, M.E.; Jacob, R.A.; McKee, R.W. Biochemical markers for assessment of niacin status in young men: Levels of erythrocyte niacin coenzymes and plasma tryptophan. J. Nutr. 1989, 119, 1949–1955. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| RTR | Kidney Donors | Population | Kidney Donors | Paired | ||
|---|---|---|---|---|---|---|
| Variable | n = 660 | n = 275 | Difference | n = 85 | Difference | |
| Total Cohort | Total Cohort | p-Value 2 | Pre-Donation | Post-Donation | p-Value 3 | |
| Age, years | 53.0 ± 12.7 | 53.3 ± 10.7 | 0.68 | 52.2 ± 10.5 | 52.6 ± 10.4 | <0.001 |
| Male, n (%) | 379 (57) | 112 (41) | 0.001 | 43 (51) | 43 (51) | - |
| Body surface area, m2 | 1.9 ± 0.2 | 1.9 ± 0.2 | 0.90 | 2.0 ± 0.2 | 1.9 ± 0.2 | 0.01 |
| BMI, kg/m2 | 26.6 ± 4.8 | 25.9 ± 3.4 | 0.01 | 26.0 ± 3.4 | 25.7 ± 3.2 | 0.03 |
| Urinary excretion | ||||||
| 2Py, μmol/day | 178.1 (130.3–242.8) | 155.6 (119.6–217.6) | 0.001 | 152.8 (124.4–215.1) | 161.7 (116.6–227.8) | 0.31 |
| N1-MN, μmol/day | 22.0 (15.8–31.8) | 41.4 (31.6–57.2) | <0.001 | 40.9 (31.0–58.2) | 32.5 (23.4–44.0) | <0.001 |
| 2Py/N1-MN | 8.7 ± 3.8 | 4.0 ± 1.4 | <0.001 | 4.0 ± 1.4 | 5.2 ± 1.5 | <0.001 |
| Sum of 2Py and N1-MN, μmol/day | 198.3 (155.9–269.4) | 203.7 (149.4–274.7) | 0.98 | 198.3 (162.3–270.8) | 189.7 (141.9–271.6) | 0.90 |
| 2Py fraction, % 4 | 89.1 (86.4–91.3) | 79.0 (75.6–82.1) | <0.001 | 78.3 (75.5–81.8) | 83.5 (80.0–86.0) | <0.001 |
| N1-MN fraction, % 4 | 10.9 (8.7–13.6) | 21.0 (17.9–24.4) | <0.001 | 21.7 (18.2–24.5) | 16.5 (14.0–20.0) | <0.001 |
| Kidney function | ||||||
| eGFR, mL/min/1.73 m2 | 45.8 ± 18.7 | 91.0 ± 14.2 | <0.001 | 92.8 ± 13.9 | 60.1 ± 12.1 | <0.001 |
| GFR, mL/min/1.73 m2 | 52.4 ± 17.4 | 82.3 ± 29.7 | <0.001 | 103.7 ± 16.7 | 65.3 ± 10.4 | <0.001 |
| Variable | RTR | Kidney Donors | ||
|---|---|---|---|---|
| Total Cohort | Pre-Donation | Post-Donation | ||
| n = 660 | n = 275 | n = 85 | n = 85 | |
| eGFR, mL/min/1.73 m2 | ||||
| Standardized β | −0.40 | −0.17 | −0.01 | −0.11 |
| p-value | <0.001 | 0.03 | 0.94 | 0.42 |
| GFR, mL/min/1.73 m2 | ||||
| Standardized β | −0.39 | −0.20 | −0.02 | 0.15 |
| p-value | <0.001 | 0.003 | 0.89 | 0.27 |
| Variable | Value | Standardized β | p-Value |
|---|---|---|---|
| Urinary 2Py/N1-MN | 8.7 ± 3.8 | - | - |
| 2Py excretion, μmol/day | 178.1 (130.3–242.8) | - | - |
| N1-MN excretion, μmol/day | 22.0 (15.8–31.8) | - | - |
| Age, years | 53.0 ± 12.7 | 0.03 | 0.09 |
| Male, n (%) | 379 (57) | −0.004 | 0.92 |
| Body surface area, m2 | 1.9 ± 0.22 | 0.11 | 0.006 |
| BMI, kg/m2 | 26.6 ± 4.8 | 0.17 | <0.001 |
| Creatinine excretion, mmol/day | 11.7 ± 3.4 | −0.05 | 0.22 |
| Time since transplantation, years | 5.6 (2.0–12.0) | −0.07 | 0.07 |
| Lifestyle | |||
| Current smoker, n (%) | 78 (13) | −0.10 | 0.02 |
| Alcohol consumption, g/day | 3.1 (0.0–11.9) | −0.15 | <0.001 |
| Nutrition | |||
| Energy intake, kcal/day | 2182 ± 642 | −0.09 | 0.03 |
| Niacin equivalents intake, mg/day | 35.6 ± 9.2 | −0.06 | 0.14 |
| Vitamin B6 intake, mg/day | 1.8 ± 0.5 | −0.09 | 0.03 |
| Glucose homeostasis | |||
| Glucose, mmol/L | 5.3 (4.8–6.0) | 0.15 | <0.001 |
| HbA1c, % | 5.8 (5.5–6.2) | 0.12 | 0.002 |
| Diabetes, n (%) | 152 (23) | 0.16 | <0.001 |
| Lipid homeostasis | |||
| Total cholesterol, mmol/L | 5.1 ± 1.1 | 0.03 | 0.38 |
| LDL, mmol/L | 3.0 ± 0.9 | 0.07 | 0.10 |
| HDL, mmol/L | 1.3 (1.1–1.7) | −0.20 | <0.001 |
| Triglycerides, mmol/L | 1.7 (1.2–2.3) | 0.17 | <0.001 |
| Hemodynamic | |||
| Systolic blood pressure, mmHg | 135.8 ± 17.3 | 0.07 | 0.08 |
| Diastolic blood pressure, mmHg | 82.5 ± 11.0 | 0.08 | 0.05 |
| Mean arterial pressure, mmHg | 107.0 ± 15.0 | 0.10 | 0.02 |
| Inflammation | |||
| Hs-CRP, mg/L | 1.6 (0.7–4.6) | 0.19 | <0.001 |
| Kidney function | |||
| eGFR, mL/min/1.73 m2 | 45.8 ± 18.7 | −0.40 | <0.001 |
| Proteinuria, n (%) | 132 (20) | 0.08 | 0.04 |
| Nonimmunosuppressive medication | |||
| Antidiabetic, n (%) | 96 (15) | 0.14 | <0.001 |
| Statin, n (%) | 349 (53) | 0.06 | 0.15 |
| Antihypertensive, n (%) | 581 (88) | 0.09 | 0.02 |
| Acetylsalicylic acid, n (%) | 127 (19) | 0.09 | 0.03 |
| Proton pump inhibitor, n (%) | 326 (49) | 0.08 | 0.04 |
| Immunosuppressive medication | |||
| Prednisolon dose, mg/day | 3.0 (2.0–3.0) | 0.07 | 0.07 |
| Proliferation inhibitor, n (%) | 548 (83) | −0.02 | 0.71 |
| Tacrolimus, n (%) | 120 (18) | 0.11 | 0.007 |
| Cyclosporine, n (%) | 253 (38) | −0.01 | 0.72 |
| Variable | Univariable | Multivariable 1 | ||
|---|---|---|---|---|
| Standardized β | p-Value | Standardized β | p-Value | |
| Age, years | 0.03 | 0.09 | - | - |
| Male, n (%) | −0.004 | 0.92 | - | - |
| BMI, kg/m2 | 0.17 | <0.001 | - | - |
| Time since transplantation, years | −0.07 | 0.07 | - | - |
| Lifestyle | ||||
| Current smoker, n (%) | −0.10 | 0.02 | −0.13 | 0.001 |
| Alcohol consumption, g/day | −0.15 | <0.001 | −0.12 | 0.002 |
| Nutrition | ||||
| Energy intake, kcal/day | −0.09 | 0.03 | - | - |
| Niacin equivalents intake, mg/day | −0.06 | 0.14 | - | - |
| Vitamin B6 intake, mg/day | −0.09 | 0.03 | - | - |
| Glucose homeostasis | ||||
| Diabetes, n (%) | 0.16 | <0.001 | 0.10 | 0.01 |
| Lipid homeostasis | ||||
| LDL, mmol/L | 0.07 | 0.10 | - | - |
| HDL, mmol/L | −0.20 | <0.001 | −0.12 | 0.002 |
| Hemodynamic | ||||
| Mean arterial pressure, mmHg | 0.10 | 0.02 | - | - |
| Inflammation | ||||
| Hs-CRP, mg/L | 0.19 | <0.001 | 0.10 | 0.009 |
| Kidney function | ||||
| eGFR, mL/min/1.73 m2 | −0.40 | <0.001 | −0.38 | <0.001 |
| Proteinuria, n (%) | 0.08 | 0.04 | - | - |
| Nonimmunosuppressive medication | ||||
| Antihypertensive, n (%) | 0.09 | 0.02 | - | - |
| Acetylsalicylic acid, n (%) | 0.09 | 0.03 | - | - |
| Proton pump inhibitor, n (%) | 0.08 | 0.04 | - | - |
| Immunosuppressive medication | ||||
| Prednisolon dose, mg/day | 0.07 | 0.07 | - | - |
| Tacrolimus, n (%) | 0.11 | 0.007 | - | - |
| R2 | 0.28 | 0.26 | ||
| Adjusted R2 | 0.25 | 0.25 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deen, C.P.J.; van der Veen, A.; Gomes-Neto, A.W.; Geleijnse, J.M.; Borgonjen-van den Berg, K.J.; Heiner-Fokkema, M.R.; Kema, I.P.; Bakker, S.J.L. Urinary Excretion of N1-methyl-2-pyridone-5-carboxamide and N1-methylnicotinamide in Renal Transplant Recipients and Donors. J. Clin. Med. 2020, 9, 437. https://doi.org/10.3390/jcm9020437
Deen CPJ, van der Veen A, Gomes-Neto AW, Geleijnse JM, Borgonjen-van den Berg KJ, Heiner-Fokkema MR, Kema IP, Bakker SJL. Urinary Excretion of N1-methyl-2-pyridone-5-carboxamide and N1-methylnicotinamide in Renal Transplant Recipients and Donors. Journal of Clinical Medicine. 2020; 9(2):437. https://doi.org/10.3390/jcm9020437
Chicago/Turabian StyleDeen, Carolien P. J., Anna van der Veen, António W. Gomes-Neto, Johanna M. Geleijnse, Karin J. Borgonjen-van den Berg, M. Rebecca Heiner-Fokkema, Ido P. Kema, and Stephan J. L. Bakker. 2020. "Urinary Excretion of N1-methyl-2-pyridone-5-carboxamide and N1-methylnicotinamide in Renal Transplant Recipients and Donors" Journal of Clinical Medicine 9, no. 2: 437. https://doi.org/10.3390/jcm9020437