Surgical Treatment for the Ankle and Foot in Patients with Rheumatoid Arthritis: A Systematic Review

 , , and
, , and 
Abstract
:1. Introduction
2. Methods
2.1. Design
2.2. Search Strategy
2.3. Eligibility Criteria
- -
- Study population composed of adults aged at least 18 years, diagnosed with RA, and who underwent surgery to the ankle and/or foot.
- -
- Study design: Randomised controlled clinical trials (RCTs) and non-randomised controlled clinical trials (NRCTs) in which surgical treatment to the ankle or foot was performed for patients with RA who experienced pain and were disabled were assessed during the follow-up period
- -
- Cohort studies of patients with RA and/or without RA to evaluate one or more surgical treatments to the foot and/or ankle, with a follow-up period.
- -
- Studies which assessed pain and disability by the following outcomes: Foot Function Index [27], American Orthopaedic Foot and Ankle Score [28], Japanese Society of Surgery of the Foot ankle/hindfoot scale [29,30], Ankle Osteoarthritis Scale [31], Kofoed ankle score, Salford Rheumatoid Arthritis Foot Evaluation- Questionnaire [32], American College of Foot and Ankle Surgeons scoring scale [29], Short-Form 36 Questionnaire [33], or Stanford Health Assessment Questionnaire disability index [34]
- -
- Studies that examined surgical treatments to the foot or ankle in individual patients with RA (case studies).
- -
- Studies combining conservative and surgical treatment to the foot or ankle in patients with RA, including those describing a relevant post-operative rehabilitation programme.
- -
- Studies assessing pain or disability in juvenile arthritis.
- -
- Studies where the first treatment options were alternatives such as orthopaedic shoes, foot or physiotherapy, not surgery.
2.4. Study Selection
2.5. Data Extraction
2.6. Quality Assessment of the Studies Included
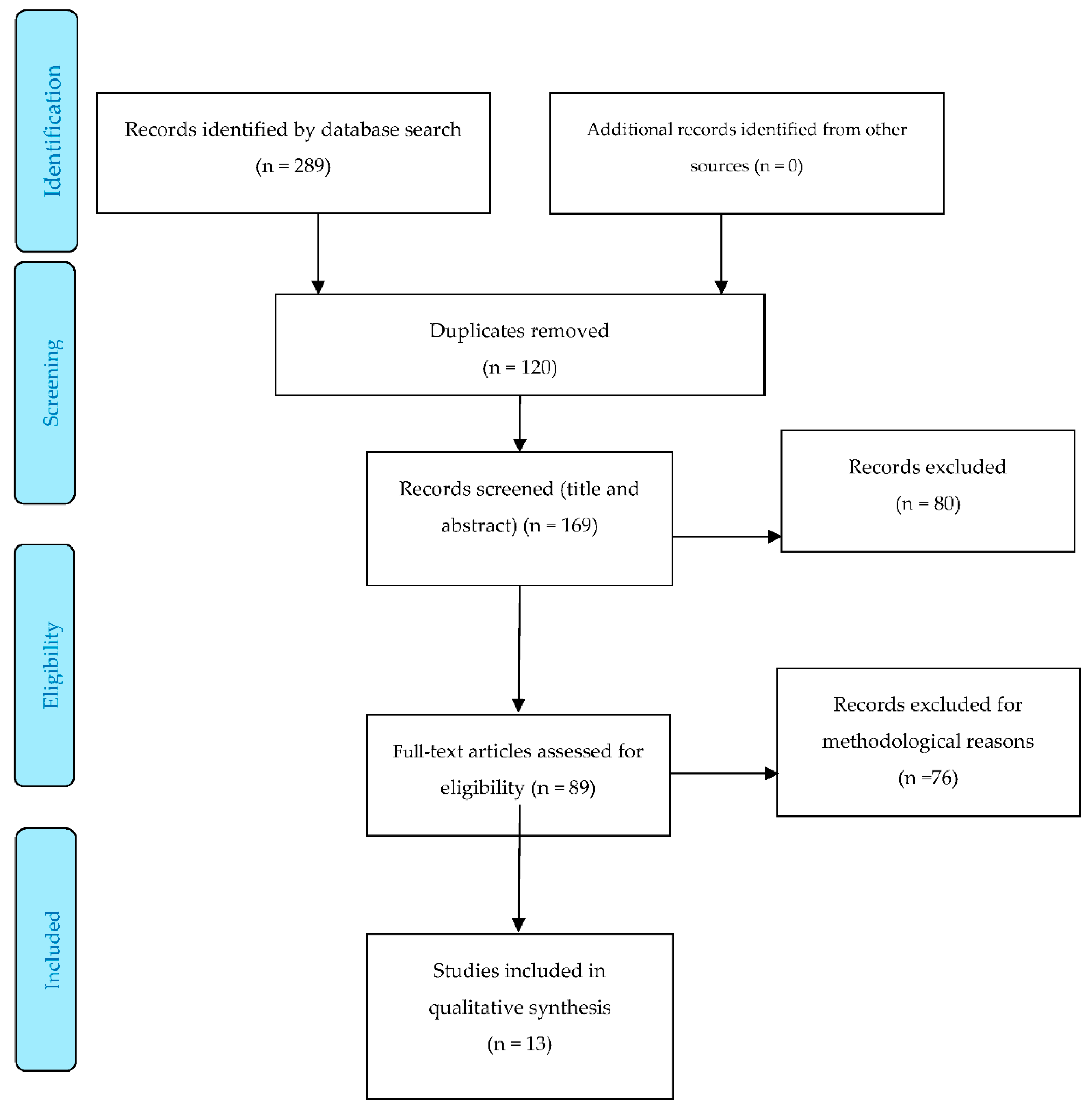
3. Results
3.1. Study Characteristics
3.2. Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
Appendix A
Appendix A.1. Searching Strategy

{kind=link}
| 1 | Rheumatoid Arthritis |
| 2 | Foot |
| 3 | Feet |
| 4 | Ankle |
| 5 | Bones of lower extremity |
| 6 | Hallux |
| 7 | First Metatarsophalang* |
| 8 | 2 OR 3 OR 4 OR 5 OR 6 OR 7 |
| 9 | 1 AND (2 OR 3 OR 4 OR 5 OR 6 OR 7) |
| 10 | Surgic* |
| 11 | “Non-conservative treatment” |
| 12 | 10 OR 11 |
| 13 | 9 AND 12 |
| 14 | “Pain” |
| 15 | Disab* |
| 16 | Funct* |
| 17 | 14 OR 15 OR 16 |
| 18 | 13 AND 17 |
Appendix A.2. Scopus Search Strategy
Appendix A.3. CINAHL Search Strategy
| 1 | Rheumatoid Arthritis |
| 2 | Foot |
| 3 | Feet |
| 4 | Ankle |
| 5 | Bones of lower extremity |
| 6 | 2 OR 3 OR 4 OR 5 |
| 7 | 1 AND (2 OR 3 OR 4 OR 5) |
| 8 | Surgic* |
| 9 | “Non-conservative treatment” |
| 10 | 8 OR 9 |
| 11 | 7 AND 10 |
| 12 | “Pain” |
| 13 | Disab* |
| 14 | Funct* |
| 15 | 12 OR 13 OR 14 |
| 16 | 11 AND 15 |
Appendix A.4. PROSPERO Search Strategy
References
- Otter, S.J.; Lucas, K.; Springett, K.; Moore, A.; Davies, K.; Cheek, L.; Young, A.; Walker-Bone, K. Foot pain in rheumatoid arthritis prevalence, risk factors and management: An epidemiological study. Clin. Rheumatol. 2010, 29, 255–271. [Google Scholar] [CrossRef]
- Voshaar, M.A.O.; ten Klooster, P.M.; Taal, E.; van de Laar, M.A. Measurement properties of physical function scales validated for use in patients with rheumatoid arthritis: A systematic review of the literature. Health Qual. Life Outcomes 2011, 9, 99. [Google Scholar] [CrossRef] [Green Version]
- Riskowski, J.L.; Hagedorn, T.J.; Hannan, M.T. Measures of foot function, foot health, and foot pain: American Academy of Orthopedic Surgeons Lower Limb Outcomes Assessment: Foot and Ankle Module (AAOS-FAM), Bristol Foot Score (BFS), Revised Foot Function Index (FFI-R), Foot Health Status Questionnair. Arthritis Care Res. 2011, 63, S229–S239. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, M.; Owaki, H.; Takahi, K.; Fuji, T. Disease activity, knee function, and walking ability in patients with rheumatoid arthritis 10 years after primary total knee arthroplasty. J. Orthop. Surg. 2014. [Google Scholar] [CrossRef]
- Jaakkola, J.I.; Mann, R.A. A review of rheumatoid arthritis affecting the foot and ankle. Foot Ankle Int. 2004. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, S.E.; Michaud, K. Epidemiological studies in incidence, prevalence, mortality, and comorbidity of the rheumatic diseases. Arthritis Res. Ther. 2009, 11, 229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siddle, H.J.; Hodgson, R.J.; Hensor, E.M.A.; Grainger, A.J.; Redmond, A.C.; Wakefield, R.J.; Helliwell, P.S. Plantar plate pathology is associated with erosive disease in the painful forefoot of patients with rheumatoid arthritis. BMC Musculoskelet. Disord. 2017. [Google Scholar] [CrossRef] [Green Version]
- Stolt, M.; Suhonen, R.; Leino-Kilpi, H. Foot health in patients with rheumatoid arthritis—A scoping review. Rheumatol. Int. 2017, 37, 1413–1422. [Google Scholar] [CrossRef]
- Van Der Leeden, M.; Steultjens, M.P.M.; Ursum, J.; Dahmen, R.; Roorda, L.D.; Van Schaardenburg, D.; Dekker, J. Prevalence and course of forefoot impairments and walking disability in the first eight years of rheumatoid arthritis. Arthritis Care Res. 2008, 59, 1596–1602. [Google Scholar] [CrossRef]
- Van der Leeden, M.; Steultjens, M.; Dekker, J.H.M.; Prins, A.P.A.; Dekker, J. Forefoot joint damage, pain and disability in rheumatoid arthritis patients with foot complaints: The role of plantar pressure and gait characteristics. Rheumatology 2006, 45, 465–469. [Google Scholar] [CrossRef] [Green Version]
- Grondal, L.; Tengstrand, B.; Nordmark, B.; Wretenberg, P.; Stark, A. The foot: Still the most important reason for walking incapacity in rheumatoid arthritis—Distribution of symptomatic joints in 1000 RA patients. Acta Orthop. 2008, 79, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C.; Lee, S.H.; Lin, H.Y.; Liu, F.W.; Chiou, H.J.; Chan, R.C.; Chou, C.L. Short-term effect of ultrasound-guided low-molecular-weight hyaluronic acid injection on clinical outcomes and imaging changes in patients with rheumatoid arthritis of the ankle and foot joints. A randomized controlled pilot trial. Mod. Rheumatol. 2017, 27, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Gijon-Nogueron, G.; Ramos-Petersen, L.; Ortega-Avila, A.B.; Morales-Asencio, J.M.; Garcia-Mayor, S. Effectiveness of foot orthoses in patients with rheumatoid arthritis related to disability and pain: A systematic review and meta-analysis. Qual. Life Res. 2018, 27, 3059–3069. [Google Scholar] [CrossRef] [PubMed]
- Blanco García, F.J. Manual SER de las Enfermedades Reumáticas; Alonso Ruíz, A., Gracia Álvaro, J.M.Á., Andreu Sánchez, J.L., Blanch, I., Rubió, J., Collantes Estévez, E., Cruz Martínez, J., Gratacós Masmitja, A., Laffón Roca, A., Martín Mola, E., Eds.; Buenos Aires: Madrid, Spain, 2004; ISBN 8479038594. [Google Scholar]
- Simon, M.J.K.; Strahl, A.; Mussawy, H.; Rolvien, T.; Schumacher, R.F.; Seller, M.; Rüther, W. Forefoot Reconstruction Following Metatarsal Head Resection Arthroplasty With a Plantar Approach—A 20-Year Follow-Up. Foot Ankle Int. 2019, 40, 769–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tootle, K.; Hollnagel, J. Lou; Kinmon, K. Surgical Treatment of Severe Hallux Abductovalgus With Dislocation of the First Metatarsophalangeal Joint: A Case Presentation and Surgical Technique. Foot Ankle Spec. 2019, 12, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.; Carroll, M.; Brenton-Rule, A.; Keys, M.; Bell, L.; Dalbeth, N.; Rome, K. Region-specific foot pain and plantar pressure in people with rheumatoid arthritis: A cross-sectional study. Clin. Biomech. 2018, 55, 14–27. [Google Scholar] [CrossRef]
- Triolo, P.; Rosso, F.; Rossi, R.; Cerlon, R.; Cottino, U.; Bonasia, D.E. Fusion of the First Metatarsophalangeal Joint and Second to Fifth Metatarsal Head Resection for Rheumatoid Forefoot Deformity. J. Foot Ankle Surg. 2017, 56, 263–270. [Google Scholar] [CrossRef]
- Rosenbaum, D.; Timte, B.; Schmiegel, A.; Miehlke, R.K.; Hilker, A. First Ray Resection Arthroplasty versus Arthrodesis in the Treatment of the Rheumatoid Foot. Foot Ankle Int. 2011, 32, 589–594. [Google Scholar] [CrossRef]
- Fazal, M.A.; Wong, J.H.M.; Rahman, L. First metatarsophalangeal joint arthrodesis with two orthogonal two hole plates. Acta Orthop. Traumatol. Turc. 2018, 52, 363–366. [Google Scholar] [CrossRef]
- Su, E.P.; Kahn, B.; Figgie, M.P. Total ankle replacement in patients with rheumatoid arthritis. Clin. Orthop. Relat. Res. 2004, 424, 32–38. [Google Scholar] [CrossRef]
- Pedersen, E.; Pinsker, E.; Younger, A.S.; Penner, M.J.; Wing, K.J.; Dryden, P.J.; Glazebrook, M.; Daniels, T.R. Outcome of Total Ankle Arthroplasty in Patients with Rheumatoid Arthritis and Noninflammatory Arthritis. J. Bone Jt. Surg. 2014, 96, 1768–1775. [Google Scholar] [CrossRef] [PubMed]
- Gong, J.; Zhou, B.; Tao, X.; Yuan, C.; Tang, K. Tibiotalocalcaneal arthrodesis with headless compression screws. J. Orthop. Surg. Res. 2016, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Hoogen, F.H.; de Waal Malefijt, M.C. Total ankle prostheses in rheumatoid arthropathy Outcome in 52 patients followed for 1–9 years. Acta Orthop. 2009, 80, 440–444. [Google Scholar] [CrossRef]
- Dodd, L.; Atinga, M.; Foote, J.; Palmer, S. Outcomes after the Stainsby Procedure in the Lesser Toes: An Alternative Procedure for the Correction of Rigid Claw Toe Deformity. J. Foot Ankle Surg. 2011, 50, 522–524. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, 1–34. [Google Scholar] [CrossRef] [Green Version]
- Budiman-Mak, E.; Conrad, K.J.; Roach, K.E. The Foot Function Index: A Measure of Foot Pain and Disability. J. Clin. Epidemiol. 1991, 44, 561–570. [Google Scholar] [CrossRef]
- Kitaoka, H.B.; Alexander, I.J.; Adelaar, R.S.; A. Nunley, J.; Myerson, M.S.; Sanders, M.; Lutter, L.D. Clinical Rating Systems for the Ankle-Hindfoot, Midfoot, Hallux, and Lesser Toes. Foot Ankle Int. 1997, 18, 187–188. [Google Scholar] [CrossRef]
- Niki, H.; Aoki, H.; Inokuchi, S.; Ozeki, S.; Kinoshita, M.; Kura, H.; Tanaka, Y.; Noguchi, M.; Nomura, S.; Hatori, M.; et al. Development and reliability of a standard rating system for outcome measurement of foot and ankle disorders I: Development of standard rating system. J. Orthop. Sci. 2005, 10, 457–465. [Google Scholar] [CrossRef] [Green Version]
- Niki, H.; Aoki, H.; Inokuchi, S.; Ozeki, S.; Kinoshita, M.; Kura, H.; Tanaka, Y.; Noguchi, M.; Nomura, S.; Hatori, M.; et al. Development and reliability of a standard rating system for outcome measurement of foot and ankle disorders II: Interclinician and intraclinician reliability and validity of the newly established standard rating scales and Japanese Orthopaedic Association. J. Orthop. Sci. 2005, 10, 466–474. [Google Scholar] [CrossRef] [Green Version]
- Domsic, R.T.; Saltzman, C.L. Ankle osteoarthritis scale. Foot Ankle Int. 1998. [Google Scholar] [CrossRef]
- Walmsley, S.; Ravey, M.; Graham, A.; Teh, L.S.; Williams, A.E. Development of a patient-reported outcome measure for the foot affected by rheumatoid arthritis. J. Clin. Epidemiol. 2012, 65, 413–422. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Fries, J.F.; Spitz, P.; Kraines, R.G.; Holman, H.R. Measurement of patient outcome in arthritis. Arthritis Rheum. 1980, 23, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (Minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2014. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group PRISMA 2009 Flow Diagram. PLoS Med. 2009. [Google Scholar] [CrossRef]
- Horita, M.; Nishida, K.; Hashizume, K.; Nasu, Y.; Saiga, K.; Nakahara, R.; Machida, T.; Ohashi, H.; Ozaki, T. Outcomes of Resection and Joint-Preserving Arthroplasty for Forefoot Deformities for Rheumatoid Arthritis. Foot Ankle Int. 2018, 39, 292–299. [Google Scholar] [CrossRef]
- Ebina, K.; Hirao, M.; Hashimoto, J.; Nampei, A.; Shi, K.; Tomita, T.; Futai, K.; Kunugiza, Y.; Noguchi, T.; Yoshikawa, H. Comparison of a self-administered foot evaluation questionnaire (SAFE-Q) between joint-preserving arthroplasty and resection-replacement arthroplasty in forefoot surgery for patients with rheumatoid arthritis. Mod. Rheumatol. 2017, 27, 795–800. [Google Scholar] [CrossRef]
- Fukushi, J.I.; Nakashima, Y.; Okazaki, K.; Yamada, H.; Mawatari, T.; Ohishi, M.; Oyamada, A.; Akasaki, Y.; Iwamoto, Y. Outcome of joint-preserving arthroplasty for rheumatoid forefoot deformities. Foot Ankle Int. 2016, 37, 262–268. [Google Scholar] [CrossRef]
- Bhavikatti, M.; Sewell, M.D.; Al-Hadithy, N.; Awan, S.; Bawarish, M.A. Joint preserving surgery for rheumatoid forefoot deformities improves pain and corrects deformity at midterm follow-up. Foot 2012. [Google Scholar] [CrossRef]
- Benoni, A.C.; Bremander, A.; Nilsdotter, A. Patient-reported outcome after rheumatoid arthritis-related surgery in the lower extremities: A report from the Swedish National Register of Rheuma Surgery (RAKIR). Acta Orthop. 2012, 83, 179–184. [Google Scholar] [CrossRef] [Green Version]
- Donegan, R.J.; Blume, P.A. Functional Results and Patient Satisfaction of First Metatarsophalangeal Joint Arthrodesis Using Dual Crossed Screw Fixation. J. Foot Ankle Surg. 2017, 56, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Kinninmonth, A.W.G.; Kumar, C.S. Long-term results of the modified Hoffman procedure in the rheumatoid forefoot. J. Bone Jt. Surg. Ser. A 2005, 87, 748–752. [Google Scholar] [CrossRef] [PubMed]
- Reize, P.; Leichtle, C.I.; Leichtle, U.G.; Schanbacher, J. Long-term results after metatarsal head resection in the treatment of rheumatoid arthritis. Foot Ankle Int. 2006, 27, 586–590. [Google Scholar] [CrossRef]
- Hirao, M.; Ebina, K.; Tsuboi, H.; Nampei, A.; Kushioka, J.; Noguchi, T.; Tsuji, S.; Owaki, H.; Hashimoto, J.; Yoshikawa, H. Outcomes of modified metatarsal shortening offset osteotomy for forefoot deformity in patients with rheumatoid arthritis: Short to mid-term follow-up. Mod. Rheumatol. 2017, 27, 981–989. [Google Scholar] [CrossRef]

| Author Year | Patients (n) | Age (Years) | Sex | Foot/Ankle | Follow up | Surgical Site | Surgical Technique | Outcome | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | Male | Left | Right | Bilat | |||||||
| Horita et al., 2018 [38] | 29 RA | 64.2 ± 22 | 29 | 0 | 34 feet | 5 | 34.75 months (min. 24 months) | MTP joints | Arthroplasty Resection group (n = 14) | JSSF | |
| Osteotomy Joint preservation group (n = 15) | |||||||||||
| Ebina et al., 2017 [39] | 49 RA | 63.45 | 46 | 3 | 63 feet | 14 | 45 months | MTP joints | Arthroplasty or osteotomy Resection-replacement (n = 28) Preserving (n = 35) | SAFE-Q | |
| Fukushi et al., 2016 [40] | 17 RA | 62 | 16 | 1 | 12 | 11 | 5 | 68 months | MTP joints | Arthrodesis of the 1st MTP joint and arthroplasty of the remaining target areas. Resection arthroplasty (RA) (n = 13) | JSSF, Hallux and lesser toes scale |
| Osteotomy of all the toes Joint preservation (n = 10) | |||||||||||
| Bhavikatti et al., 2012 [41] | 49 RA | 56.1 ± 26 | 44 | 5 | 66 feet | 17 | 51 months (40–65) | MTP joints | Osteotomy | AOFAS | |
| Benoni et al., 2012 [42] | 258 (193 RA) | 64 ± 33 | 212 | 65 | 162 feet and 31 ankles | - | 12 months | Ankle and foot | Arthrodesis or osteotomy of the forefoot. Stainsby ankle group (n = 31) | SF-36 HAQ | |
| Arthrodesis of the hindfoot. Arthrodesis or arthroplasty of the ankle. Feet group (n = 162) | |||||||||||
| Rosenbaum et al., 2011 [19] | 53 RA | 53 ± 9 | 43 | 10 | 58 feet | 5 | 41 ± 12 months | MTP joints | Arthrodesis of the 1st MTP joint. Arthrodesis (n = 33) | HAQ FFI | |
| Arthroplasty of all target areas. Arthroplasty (n = 25) | |||||||||||
| Van der Heide et al., 2009 [24] | 58 (54 RA) | 55 ± 27 | 48 | 10 | 58 ankles | 4 | 31 months | Ankle | Total arthroplasty of the ankle STAR (n = 37) BP (n = 21) | Kofoed score | |
| Su et al., 2004 [21] | 17 RA | 50 ± 31 | 14 | 2 | 27 ankles | 10 | 76 months | Ankle | Total arthroplasty of the ankle HSS Custom (n = 7) Endotec (n = 19) | AOFAS | |
| Author Year | Patients (n) | Age (Years) | Sex | Foot/Ankle | Follow up | Surgical Site | Surgical Technique | Outcome | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | Male | Left | Right | Bilat | |||||||
| Fazal et al., 2018 [20] | 26 (10RA) | 64 ± 15 | 23 | 3 | 32 feet | 6 | 49 months (40–62 months) | 1st MTP joint | Arthrodesis: fixation with 2 orthogonal plates | AOFAS FADI | |
| Donegan et al., 2017 [43] | 228 (29RA) | 55.8 ± 3.2 | 178 | 50 | 122 | 140 | 22 | 7.6 ± 1.64 months | 1st MTP joint, small toes. | Arthrodesis of the 1st MTP joint with double screw fixation and arthroplasty of the small toes | ACFAS scoring scale and SF-36 |
| Pedersen et al., 2014 [22] | 100 (50RA) | 60 | 64 (35 RA) | 36 (15 RA) | 58 RA ankles 54 NRA ankles | 12 | 64.7 ± 22.1 | Ankle | Total arthroplasty of the ankle | AOS SF-36 | |
| Dodd et al., 2011 [25] | 16 (4RA) | 56 ± 21 | 12 (3 RA) | 3 (1RA) | 24 (6 RA) | 14 months (min. 6 months) | Small toes | Standby | Manchester Oxford Foot and Ankle Score | ||
| Thomas et al., 2006 [44] | 23RA | 60.9 ± 22 | 19 | 4 | 21 | 22 | 20 | 64.9 months (22–108) | MTP joints | Arthroplasty | AOFAS VAS |
| Author | Surgical Site | Outcome | Surgical Technique | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Horita et al. [38] | MTP Joints | Arthroplasty resection group | Osteotomy joint-preservation group | |||||||
| JSSF (0–100 points) | Pre | Post | p-Value | Pre | Post | p-Value | ||||
| Pain | 22.5 ± 10 | 28.1 ± 10 | 0.003 | 20.0 ± 20 | 28.9 ± 10 | 0.001 | ||||
| Deformity | 12.2 ± 12 | 19.9 ± 13 | 0.001 | 14.7 ± 6 | 22.0 ± 6 | 0.001 | ||||
| Range of motion | 10.1 ± 15 | 12.0 ± 15 | 0.023 | 10.9 ± 7 | 14.3 ± 2 | 0.004 | ||||
| Walking ability | 13..1 ± 10 | 18.8 ± 10 | 0.003 | 11.4 ± 7 | 18.9 ± | 0.003 | ||||
| Activities of daily life (ADL) | 3.3 ± 8 | 5.4 ± 8 | 0.015 | 5.2 ± 3 | 7.1 ± 2 | 0.012 | ||||
| JSSF-RA scale (total) | 61.3 ± 19 | 83.9 ± 27 | 0.001 | 62.2 ± 15 | 90.8 ± 8 | 0.001 | ||||
| Ebina et al. [39] | MTP Joints | Resection-replacement group | Preserving group | |||||||
| SAFE-Q (0–100 points) | Pre | Post | Change | Pre | Post | Change | ||||
| Pain | 36.8 | 75.0 | 38.2 | 42.2 | 82.6 | 44.4 | ||||
| Physical functioning and daily living | 43.2 | 68.8 | 25.6 | 52.7 | 78.1 | 25.4 | ||||
| Social functioning | 44.3 | 72.0 | 27.7 | 52.5 | 81.9 | 29.4 | ||||
| General health and well-being | 48.4 | 68.4 | 20.0 | 45.5 | 84.4 | 38.9 | ||||
| Shoe-related | 30.1 | 50.3 | 20.2 | 30.6 | 64.4 | 33.8 | ||||
| Fukushi et al. [40] | MTP Joints | Joint-preserving | Resection arthroplasty | p-Value | ||||||
| JSSF (0–100 points) | Pre | Post | Pre | Post | Pre | Post | ||||
| Hallux | Total | 61.4 ± 16.3 | 88.2 ± 8.1 | 54.5 ± 8.3 | 79.4 ± 9.6 | 0.196 | 0.035 | |||
| Pain | 27.0 ± 11.6 | 37.0 ± 4.8 | 26.9 ± 4.8 | 36.4 ± 6.7 | 0.982 | 0.808 | ||||
| Function | 32.8 ± 5.3 | 36.2 ± 6.0 | 27.5 ± 5.5 | 28.0 ± 3.6 | 0.032 | 0.001 | ||||
| Alignment | 3.1 ± 5.3 | 15.0 ± 0.0 | 0.0 ± 0.0 | 15.0 ± 0.0 | 0.047 | - | ||||
| Lesser toes | Total | 57.4 ± 19.2 | 87.7 ± 8.3 | 45.2 ± 12.3 | 73.6 ± 13.9 | 0.091 | 0.015 | |||
| Pain | 24.4 ± 7.3 | 36.6 ± 5.0 | 23.8 ± 2.3 | 36.4 ± 5.0 | 0.867 | 0.894 | ||||
| Function | 28.2 ± 11.3 | 36.1 ± 6.8 | 21.4 ± 2.4 | 30.3 ± 5.7 | 0.077 | 0.050 | ||||
| Alignment | 3.5 ± 4.2 | 15 ± 0.0 | 0.0 ± 0.7 | 7.0 ± 6.3 | 0.006 | 0.001 | ||||
| Bhavikatti et al. [41] | MTP Joints | Osteotomy group | ||||||||
| Pre | Post | Change | ||||||||
| AOFAS (0–100 points) | 39.8 (18–56) | 88.7 (48–92) | 48.9 | |||||||
| Benoni et al. [42] | Ankle and foot | Feet group | Stainsby ankle group | |||||||
| Pre | 12 months | p-Value | Pre | 12 months | p-Value | |||||
| HAQ (0–3points) | 1.0 | 0.96 | 0.8 | 1.4 | 1.4 | 0.8 | ||||
| SF-36 (0–100 points) | ||||||||||
| Physical functioning (PF) | 44 | 51 | <0.001 | 27 | 33 | 0.2 | ||||
| Social functioning (SF) | 73 | 75 | 0.4 | - | - | - | ||||
| Role limitations because of physical health problems (RP) | 34 | 42 | 0.03 | 19 | 27 | 0.4 | ||||
| Bodily pain (BP) | 40 | 48 | <0.001 | 34 | 46 | 0.03 | ||||
| General mental health (GH) | 51 | 49 | 0.4 | 51 | 46 | 0.2 | ||||
| Emotional problems (RE) | 64 | 67 | 0.5 | 51 | 55 | 0.7 | ||||
| Vitality (VT) | 51 | 50 | 0.5 | 38 | 45 | 0.2 | ||||
| Rosenbaum et al. [19] | MTP joints | Arthrodesis | Arthroplasty | p-Value | ||||||
| HAQ (0–3) | 1.0 ± 0.7 | 0.9 ± 0.6 | Ns | |||||||
| FFI (0–100) | 32 ± 19 | 30 ± 17 | Ns | |||||||
| van der Heide et al. [24] | Ankle | STAR | BP | |||||||
| Follow up (31 months) | ||||||||||
| Kofoed Score (0–100 points) | Mean Kofoed score73 points (SD16, range 21–92) | <50 points | 4 | 0 | ||||||
| Removal of implant | 4 | 1 | ||||||||
| >50 points | 29 | 20 | ||||||||
| Su et al. [21] | Ankle | HSS Custom | Endotec | p-value | ||||||
| AOFAS (0–100 points) | 85 | 79 | 0.12 | |||||||
| Fazal et al. [20] | 1st MTP joint | Arthrodesis group | ||||||||
| Pre | Post | Change | ||||||||
| AOFAS (0–100 points) | 37.1 ± 8.8 | 80.7 ± 8.8 | 43.6 (p < 0.0001) | |||||||
| FADI (0–100 points) | 40.3 ± 11.0 | 86.9 ± 14.2 | 46.6 (p < 0.0001) | |||||||
| Donegan et al. [43] | 1st MTP joint | Arthrodesis of the 1st MTP joint with double screw fixation and arthroplasty of the small toes | ||||||||
| Post | ||||||||||
| SF-36 (0–100 points) | Physical function | 79.5 ± 2.6 | ||||||||
| Energy | 72.3 ± 1.7 | |||||||||
| Painlessness | 79.4 ± 1.5 | |||||||||
| General health | 73.0 ± 1.9 | |||||||||
| ACFAS (0–68 points) | Subjective score | 37.2 ± 2.5 | ||||||||
| Objective score | 14.5 ± 1.7 | |||||||||
| Pedersen et al. [22] | Ankle | Arthroplasty group | ||||||||
| Pre | Post | Change | ||||||||
| AOS (0–100 points) | Pain | 63.3 ± 16.6 | 18.5 ± 17.8 | −44.8 ± 22.7 | ||||||
| Disability | 70.0 ± 14.6 | 30.0 ± 23.4 | −40.0 ± 23.0 | |||||||
| SF-36 (0–100 points) | Physical component | 27.4 ± 8.0 | 34.4 ± 8.8 | 6.9 ± 8.6 | ||||||
| Mental component | 59.0 ± 13.4 | 63.1 ± 9.5 | 4.1 ± 12.8 | |||||||
| Dodd et al. [25] | Small toes | Standby | ||||||||
| Pre | Post | Change | ||||||||
| Manchester and Oxford Foot and Ankle Score | Pain (0–20) | 13.75 ± 3 | 8.75 ± 3 | −5 | ||||||
| Social (0–16) | 11.5 ± 10 | 7.5 ± 11 | −4 | |||||||
| Walking (0–28) | 22.5 ± 8 | 14.75 ± 10 | −7.75 | |||||||
| Thomas et al. [44] | MTP Joints | Arthroplasty group | ||||||||
| Final follow-up | ||||||||||
| VAS (0–10 points) | Pain at rest | 1.8 ± 6.1 | ||||||||
| Pain in motion | 4.1 ± 8.9 | |||||||||
| AOFAS (0–100 points) | 64.5 ± 27 | |||||||||
| Author | Clearly Stated Aim | Inclusion of Consecutive Patients | Prospective Collection of Data | Endpoints Appropriate to the Aim of the Study | Unbiased Assessment of the Study Endpoint: | Follow-up Period Appropriate to the Aim of the Study | Loss to Follow up Less than 5% | Prospective Calculation of the Study Size | An Adequate Control Group: | Contemporary Groups | Baseline Equivalence of Groups | Adequate Statistical Analyses | Score 24/24 Or 16/16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Horita et al. [38] | 2 | 1 | 2 | 1 | 0 | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 18/24 |
| Ebina et al. [39] | 2 | 1 | 2 | 2 | 0 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 20/24 |
| Fukushi et al. [40] | 2 | 1 | 1 | 2 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 18/24 |
| Rosenbaum et al. [19] | 2 | 1 | 1 | 1 | 0 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 18/24 |
| Su et al. [21] | 2 | 1 | 2 | 1 | 1 | 2 | 2 | 2 | 1 | 0 | 0 | 2 | 16/24 |
| Bhavikatti et al. [41] | 2 | 1 | 2 | 1 | 0 | 2 | 2 | 0 | 10/16 | ||||
| Benoni et al. [42] | 2 | 2 | 2 | 2 | 0 | 1 | 0 | 2 | 11/16 | ||||
| van der Heide et al. [24] | 2 | 1 | 1 | 1 | 0 | 1 | 2 | 1 | 9/16 |
| Author | Selection * | Comparability ** | Outcome *** | Score **** | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the exposed cohort 1 | Selection of the non-exposed cohort 2 | Ascertainment of exposure 3 | Demonstration that outcome of interest was not present at start of study 4 | Comparability of cohorts on the basis of the design or analysis 5 | Assessment of outcome 6 | Was follow-up long enough for outcomes to occur? 7 | Adequacy of follow up of cohorts 8 | ||
| Fazal et al. [20] | c | c | a * | a * | a * | d | a * | a * | 5 |
| Donegan et al. [43] | a * | c | a * | a * | a * | b * | b | b * | 6 |
| Pedersen et al. [22] | a * | b | a * | a * | a * | b * | a * | a * | 7 |
| Dodd et al. [25] | b * | b | a * | a * | a * | b * | c | b * | 6 |
| Thomas et al. [44] | b * | c | a * | a * | a * | b * | a * | b * | 7 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega-Avila, A.B.; Moreno-Velasco, A.; Cervera-Garvi, P.; Martinez-Rico, M.; Chicharro-Luna, E.; Gijon-Noqueron, G. Surgical Treatment for the Ankle and Foot in Patients with Rheumatoid Arthritis: A Systematic Review. J. Clin. Med. 2020, 9, 42. https://doi.org/10.3390/jcm9010042
Ortega-Avila AB, Moreno-Velasco A, Cervera-Garvi P, Martinez-Rico M, Chicharro-Luna E, Gijon-Noqueron G. Surgical Treatment for the Ankle and Foot in Patients with Rheumatoid Arthritis: A Systematic Review. Journal of Clinical Medicine. 2020; 9(1):42. https://doi.org/10.3390/jcm9010042
Chicago/Turabian StyleOrtega-Avila, Ana Belen, Antonio Moreno-Velasco, Pablo Cervera-Garvi, Magdalena Martinez-Rico, Esther Chicharro-Luna, and Gabriel Gijon-Noqueron. 2020. "Surgical Treatment for the Ankle and Foot in Patients with Rheumatoid Arthritis: A Systematic Review" Journal of Clinical Medicine 9, no. 1: 42. https://doi.org/10.3390/jcm9010042