Trajectories of Biological Values and Vital Parameters: An Observational Cohort Study of Adult Patients with Sickle Cell Disease Hospitalized for a Non-Complicated Vaso-Occlusive Crisis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
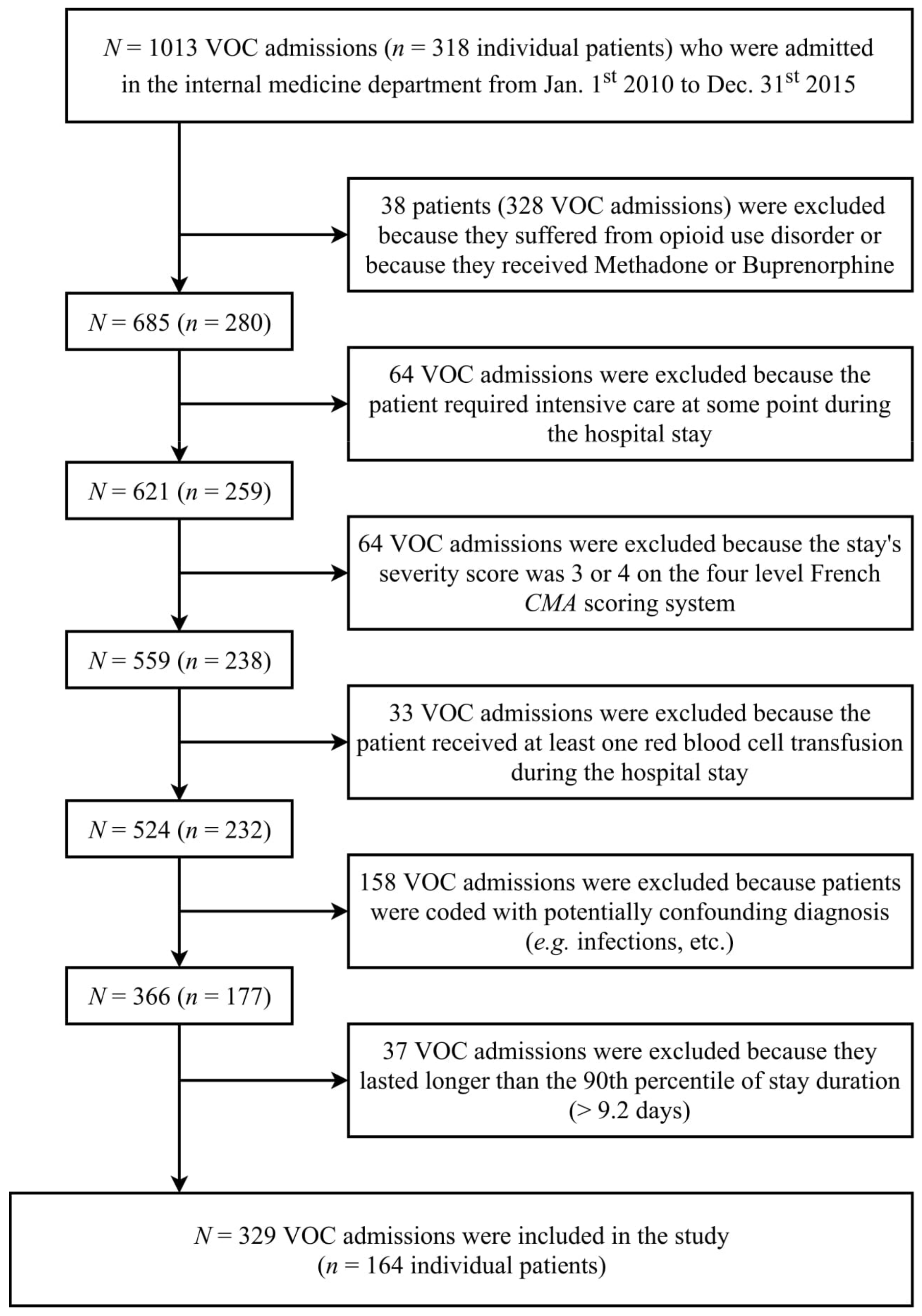
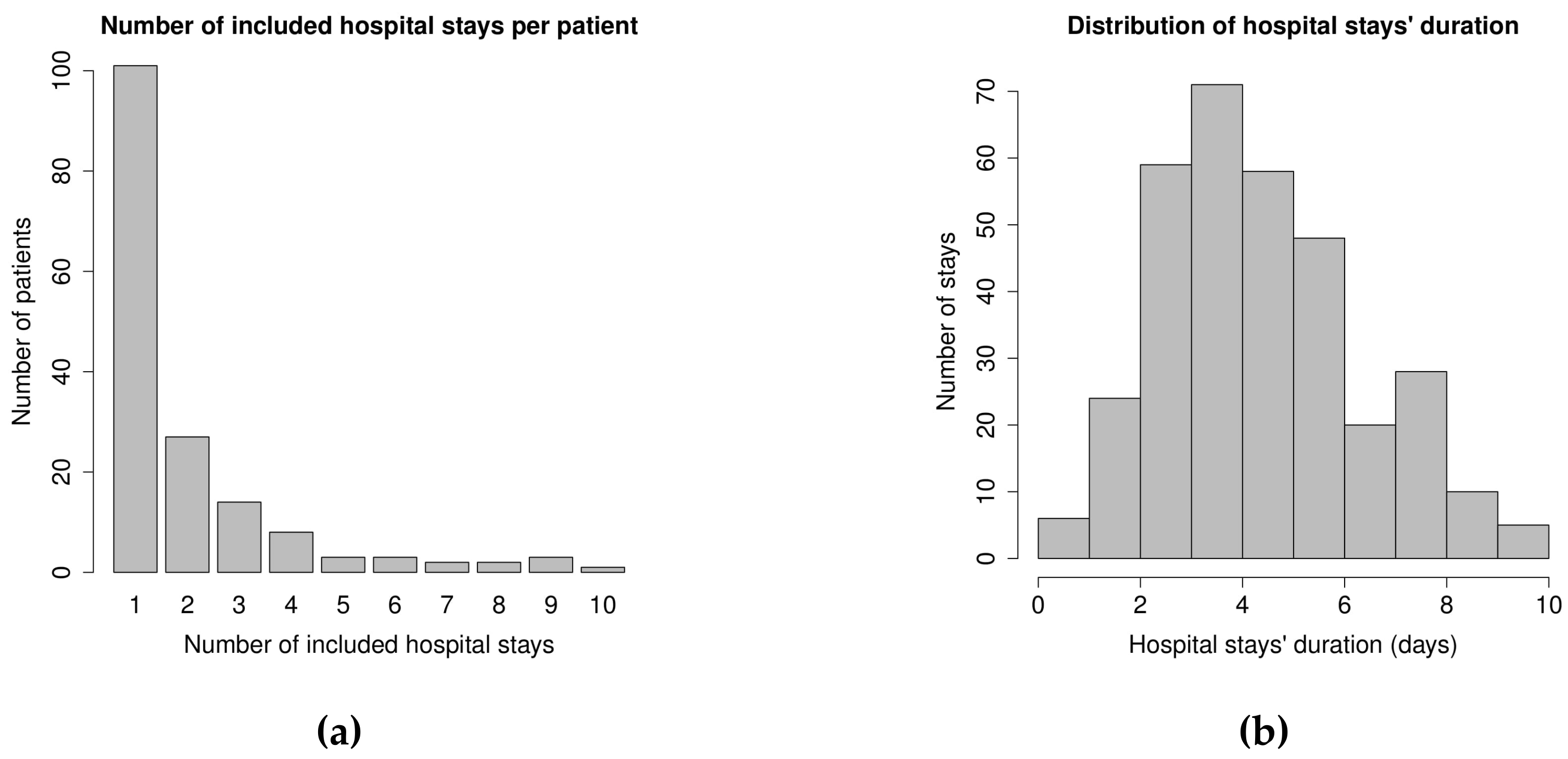
3.1. Population Description
3.2. Trends in Laboratory Results
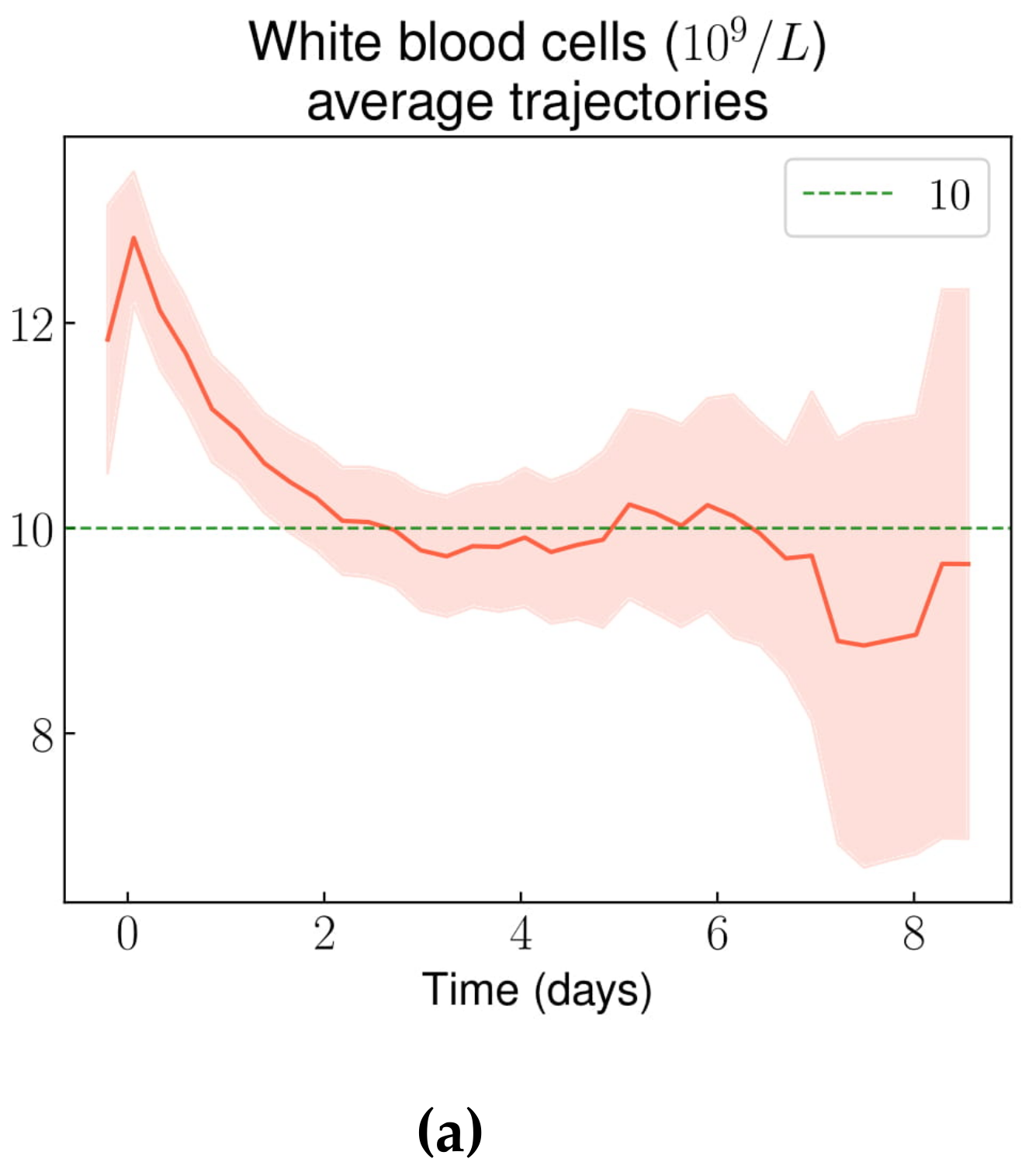
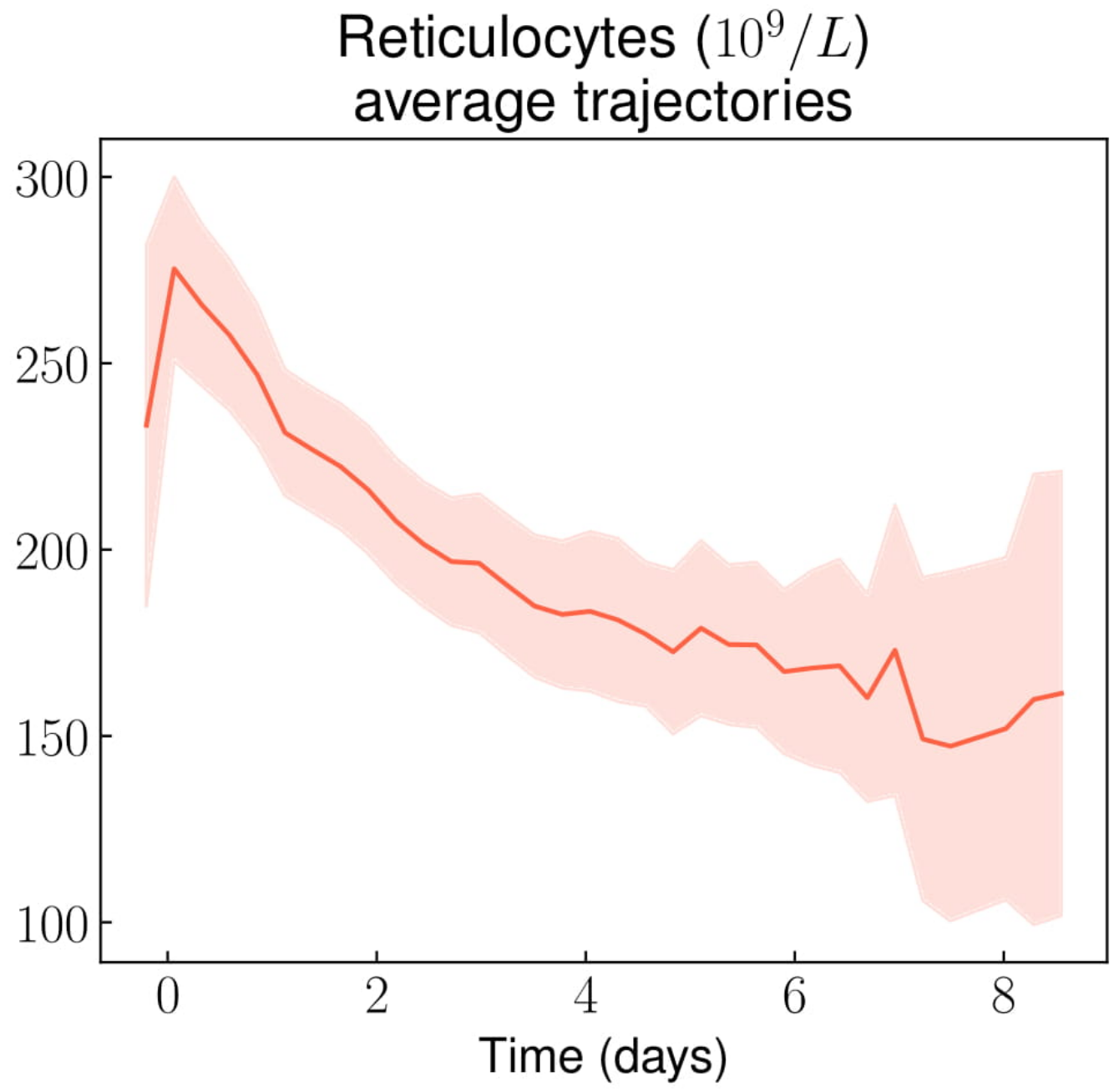
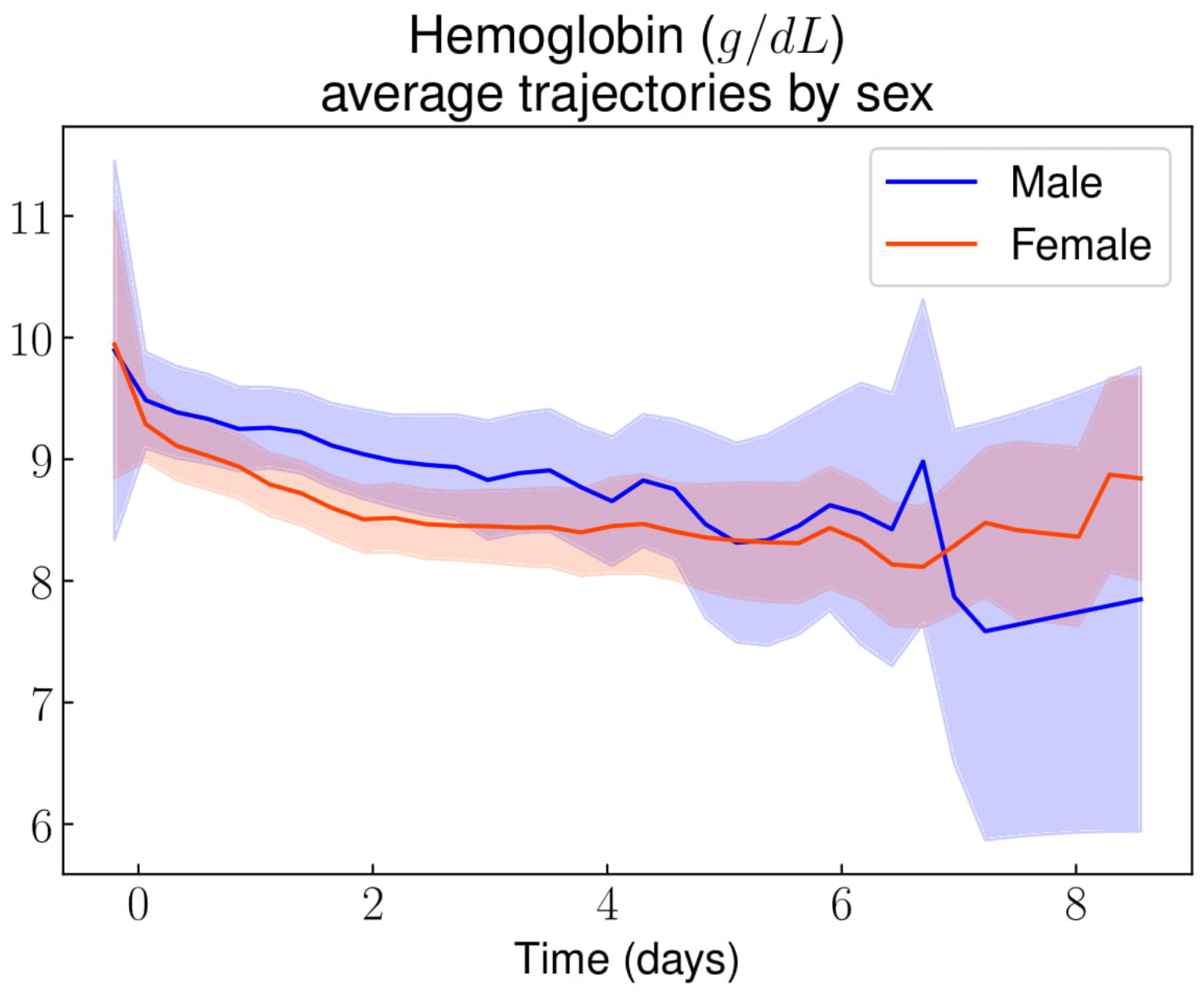
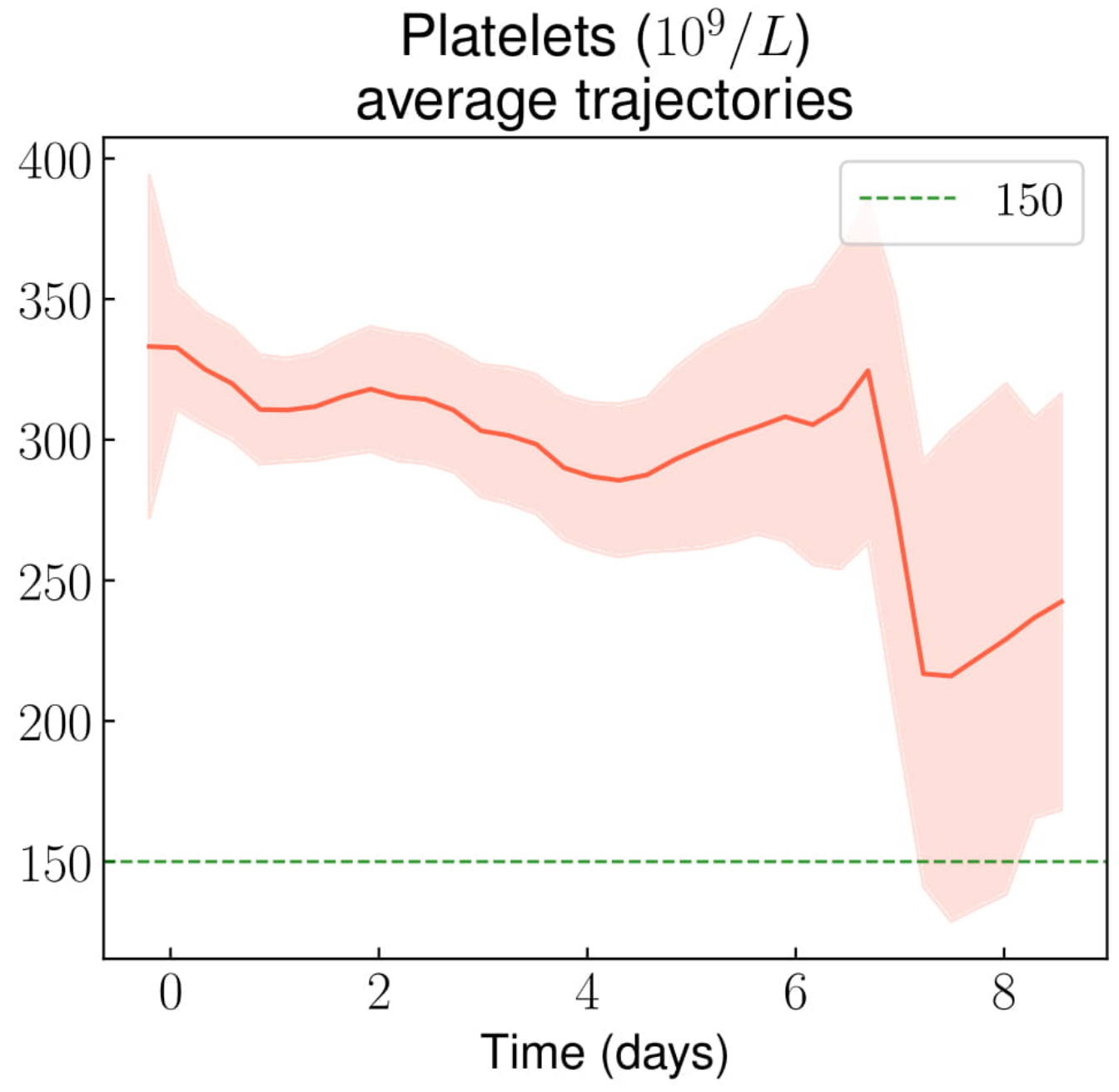
3.2.1. Complete Blood Count
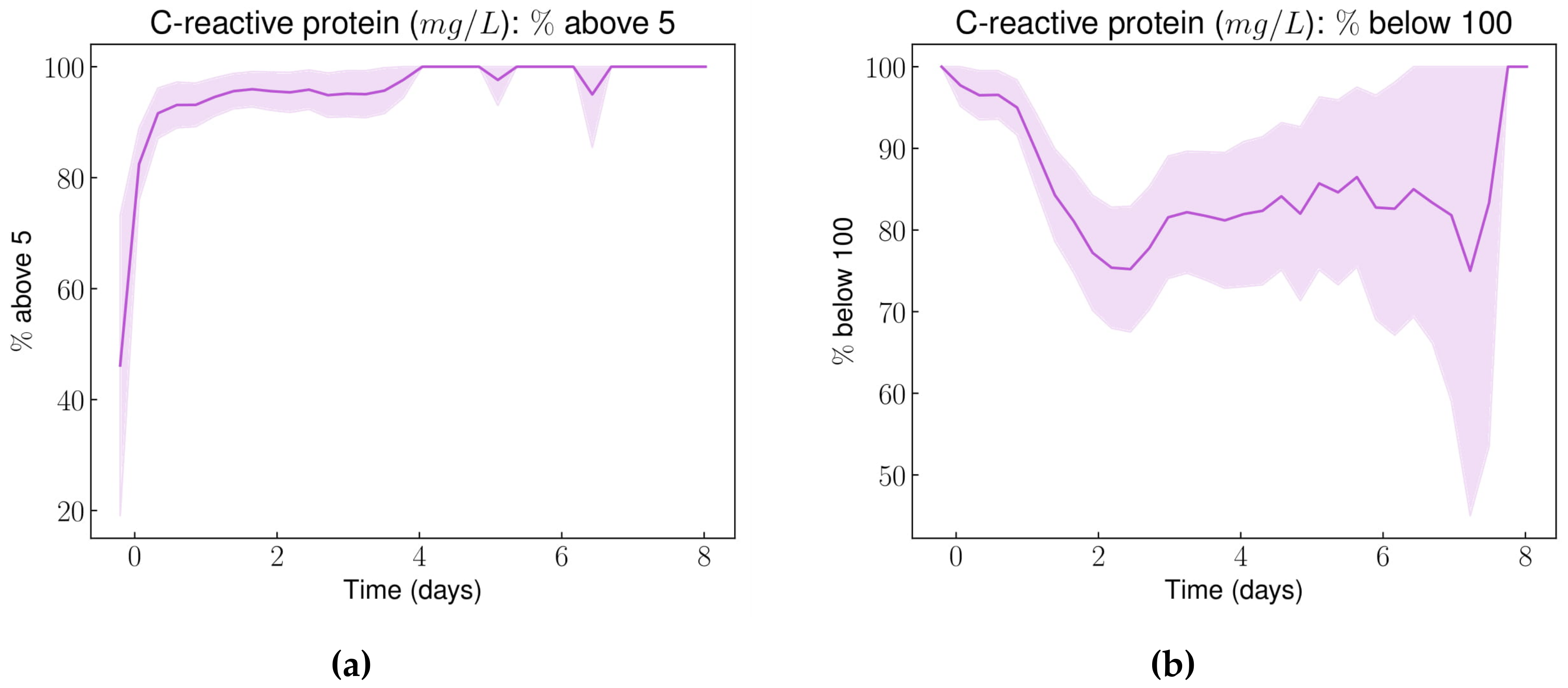
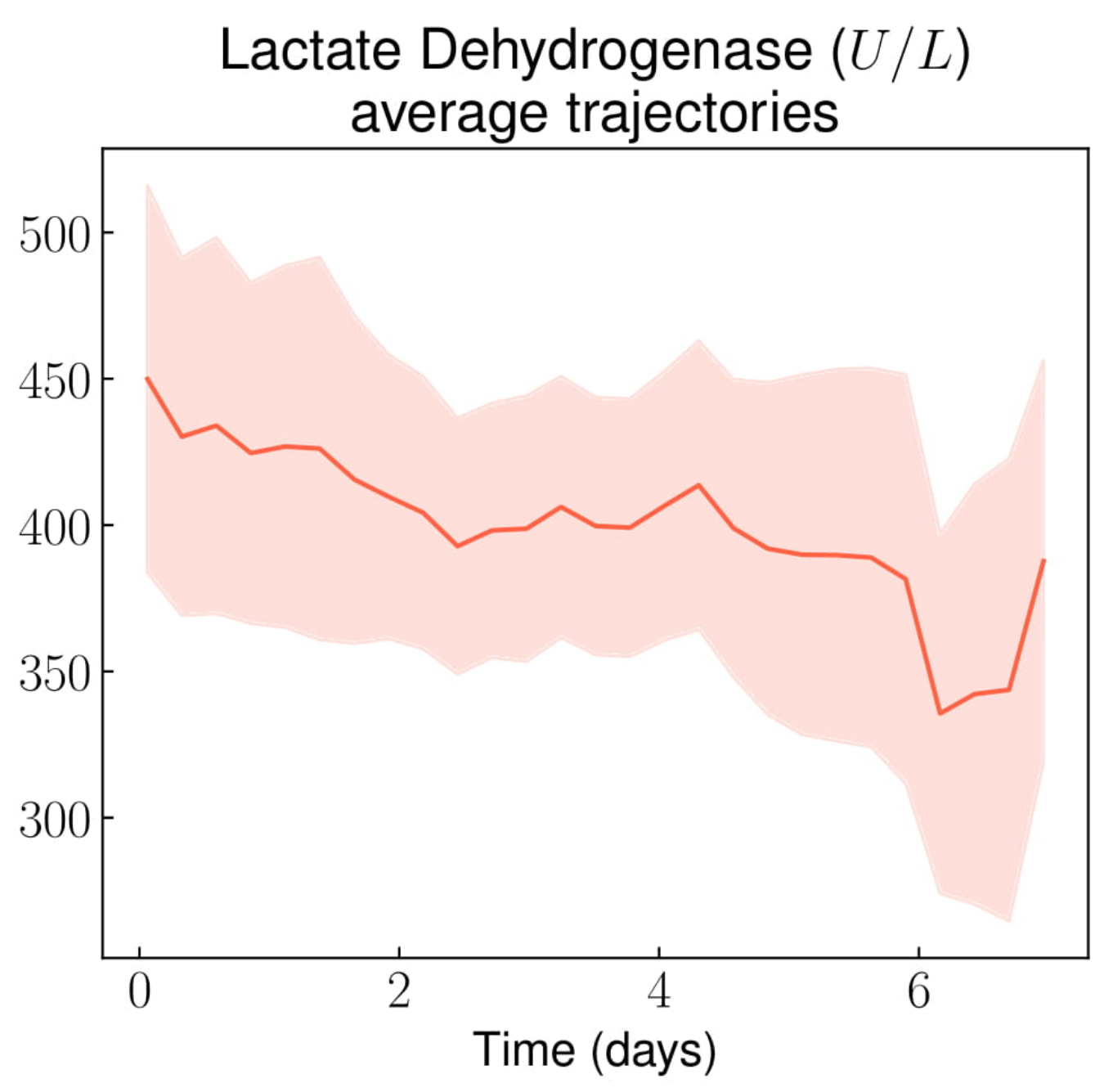
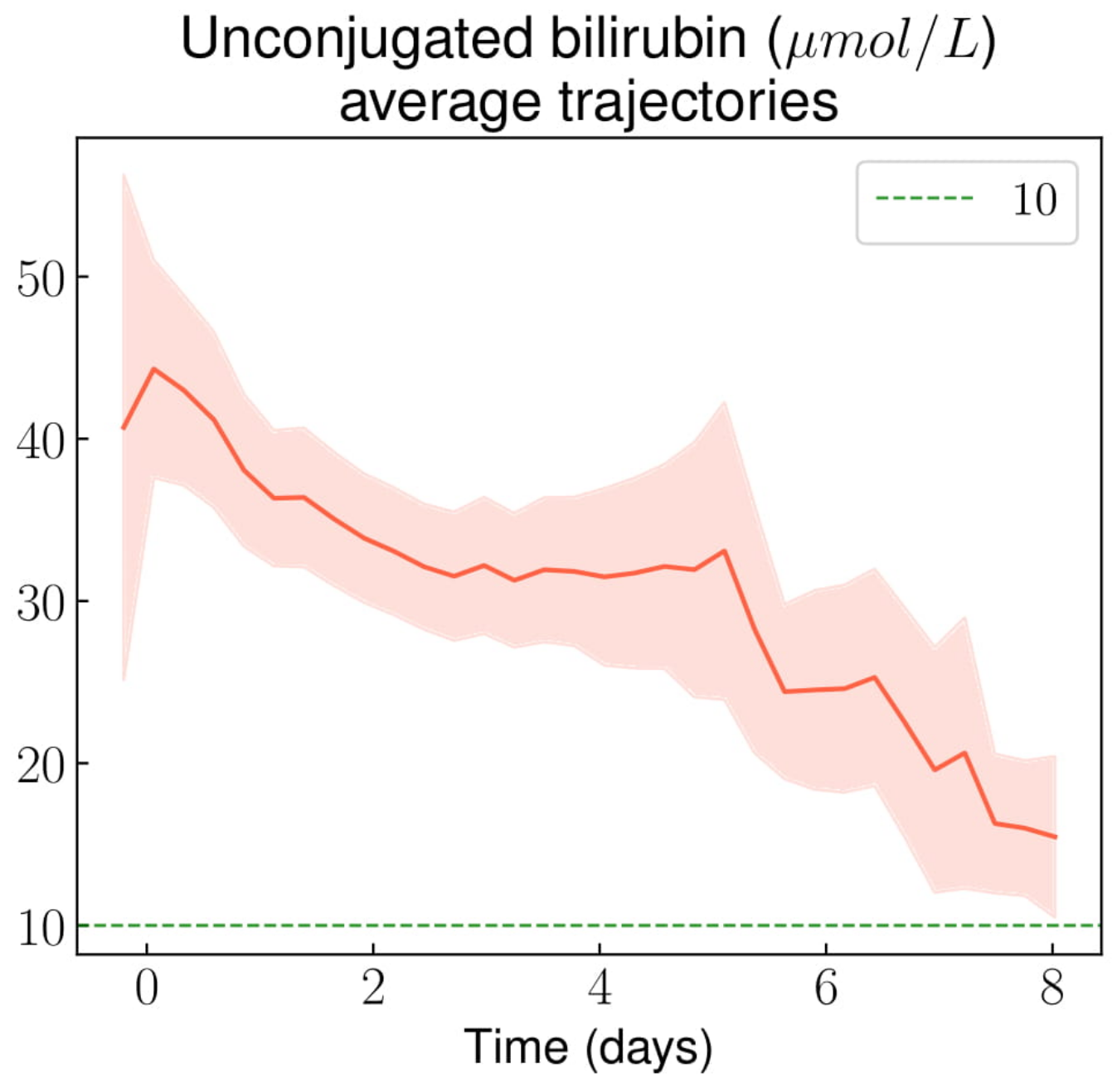
3.2.2. Other Laboratory Results
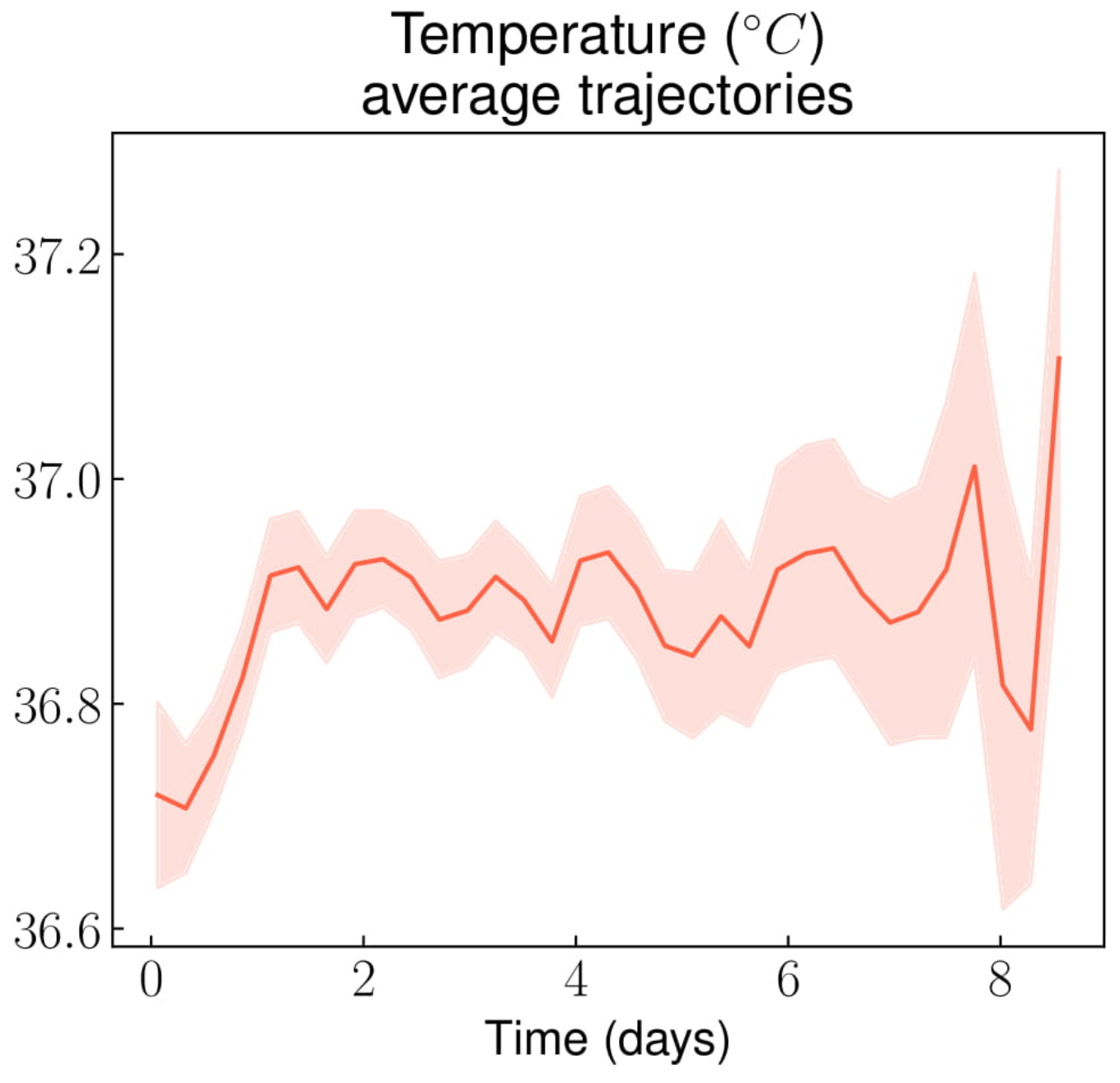
3.3. Trends in Vital Parameters
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
Appendix A
Appendix B
- A15–A19: Tuberculosis
- A30–A49: Other bacterial diseases
- A80–A89: Viral infections of the central nervous system
- B50–B64: Protozoal diseases
- B95–B97: Bacterial, viral and other infectious agents
- G00–G09: Inflammatory diseases of the central nervous system
- I70–I79: Diseases of arteries, arterioles and capillaries
- I80.0–I80.2: Phlebitis and thrombophlebitis
- I82: Other venous embolism and venous thrombosis
- J01: Sinusitis
- J02: Pharyngitis
- J14–J18: Bacterial pneumonia (includes the code used for acute chest syndromes)
- J20: Acute bronchitis
- J32: Chronic sinusitis
- J69: Pneumonitis due to solids and liquids
- K04: Diseases of pulp and periapical tissues
- K12.2: Cellulitis
- K81: Cholecystitis
- K83: Other diseases of biliary tracts
- K85: Acute pancreatitis
- M10: Gout
- M11: Other crystal arthropathies
- M86: Osteomyelitis
- N10: Acute tubulo-interstitial nephritis
- N41.0: Acute prostatitis
- R57.2: Septic shock
- R65.0–R65.1: Systemic Inflammatory Response Syndrome [SIRS] of infectious origin
- Infectious items from T80–T88: Infectious complications of surgical and medical care
Appendix C
- Demographic data (sex, date of birth);
- Dates and timestamps for hospital admission (which occurs after the patient has been evaluated by the emergency department), as well as hospital discharge;
- Laboratory tests measured at least once for over 75% of patients from both the emergency department (prior to hospital admission) and the subsequent hospital stay;
- Vital parameters measured at least once for over 75% of patients after admission (vital parameters from the emergency department could not be retrieved);
- Opioid prescriptions (molecule, starting and ending timestamps, posology and pharmaceutical form);
- Using all available free text reports from the patients’ EHR regardless of the source department and the stay, we also extracted the following patient-related variables:
- ○
- Steady state hemoglobin level (i.e., hemoglobin level measured at a routine evaluation, outside any VOC or infectious episode);
- ○
- Sickle cell disease genotype (either SS or other SCD genotypes);
- ○
- Comorbidities and complications.
- The age of the patient at hospital admission, determined from the patient’s date of birth and the timestamp for the admission;
- The duration of the stay, based on the admission and discharge timestamps. Note that the duration of the stay does not include the time the patient spent in the emergency department prior to admission to the internal medicine department;
- The hemoglobin gap to steady state (i.e., for each punctual hemoglobin measure, we derived the difference between this measure and the patient’s steady state hemoglobin value). For the 13 patients (7.9%) whose steady state hemoglobin value was missing, we imputed it using the last hemoglobin value measured prior to discharge, following their first included stay.
Appendix D
- We created a uniform time grid from the overall first measure to the last one. Zero time mark was set at the timestamp of the stay’s admission. For specific variables with known day/night cycles (e.g., temperature and blood pressure), zero time mark was arbitrarily set at 6pm on the day of the admission to take into account day/night cycle.
- We fitted a first order smoothing spline on each stay’s individual trajectory.
- From the fitted individual stays trajectories, we computed a mean trajectory with its confidence interval. For this final step, we followed a specific procedure to enhance precision and performance:
- We calculated for each stay the variable’s value at every time mark on the grid. If an individual trajectory’s time span was shorter than the overall time grid, we considered the missing time mark’s values as NA. That means that individual trajectories were not imputed with spline extrapolations neither before the first available value nor after the last.
- We then obtained a matrix were each row is a stay, each column is a time mark, and each cell is a measured or spline imputed value.
- We assumed that for each time mark, the values are drawn from a Gaussian distribution. Thus, for each time mark, we calculate the mean value with its 95% Gaussian confidence interval.
- Additionally, we stratified this procedure by sex.
- Finally, for some selected variables whose average trajectories suggested that they could potentially discriminate between non-complicated and complicated VOCs, we calculated the proportion of patients all along the hospital stay whose values were above or below specific thresholds. The thresholds were chosen based on both clinical relevance and graphical description of the averaged trajectory.
- Given the fact that this procedure relies on individual stay’s smoothed trajectories to draw an average trajectory, we applied it on a limited selection of biomarkers and vital parameters, for which we had values measured for at least 75% of the included stays. This explains why only the most routinely monitored variables are analyzed in our study, even though some included patients might have benefitted from less common laboratory tests.
Appendix E










References
- Weatherall, D.; Akinyanju, O.; Fucharoen, S.; Olivieri, N.; Musgrove, P. Disease Control Priorities in Developing Countries; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Modell, B.; Darlison, M. Global epidemiology of haemoglobin disorders and derived service indicators. Bull. World Health Organ. 2008, 86, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Wastnedge, E.; Waters, D.; Patel, S.; Morrison, K.; Goh, M.Y.; Adeloye, D.; Rudan, I. The global burden of sickle cell disease in children under five years of age: A systematic review and meta-analysis. J. Glob. Health 2018. [Google Scholar] [CrossRef] [PubMed]
- Piel, F.B.; Patil, A.P.; Howes, R.E.; Nyangiri, O.A.; Gething, P.W.; Dewi, M.; Temperley, W.H.; Williams, T.N.; Weatherall, D.J.; Hay, S.I. Global epidemiology of sickle haemoglobin in neonates: A contemporary geostatistical model-based map and population estimates. Lancet 2013, 381, 142–151. [Google Scholar] [CrossRef]
- Rees, D.C.; Williams, T.N.; Gladwin, M.T. Sickle-cell disease. Lancet 2010, 376, 2018–2031. [Google Scholar] [CrossRef]
- Pauling, L.; Itano, H.A.; Singer, S.J.; Wells, I.C. Sickle Cell Anemia, a Molecular Disease. Science 1949, 110, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Bunn, H.F. Pathogenesis and Treatment of Sickle Cell Disease. N. Engl. J. Med. 1997, 337, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Stuart, M.J.; Nagel, R.L. Sickle-cell disease. Lancet 2004, 364, 1343–1360. [Google Scholar] [CrossRef]
- Diggs, L.W. Sickle Cell Crises: Ward Burdick Award Contribution. Am. J. Clin. Pathol. 1965, 44, 1–19. [Google Scholar] [CrossRef]
- Platt, O.S.; Thorington, B.D.; Brambilla, D.J.; Milner, P.F.; Rosse, W.F.; Vichinsky, E.; Kinney, T.R. Pain in Sickle Cell Disease. N. Engl. J. Med. 1991, 325, 11–16. [Google Scholar] [CrossRef]
- Platt, O.S.; Brambilla, D.J.; Rosse, W.F.; Milner, P.F.; Castro, O.; Steinberg, M.H.; Klug, P.P. Mortality In Sickle Cell Disease—Life Expectancy and Risk Factors for Early Death. N. Engl. J. Med. 1994, 330, 1639–1644. [Google Scholar] [CrossRef]
- Prasad, R.; Hasan, S.; Castro, O.; Perlin, E.; Kim, K. Long-Term Outcomes in Patients with Sickle Cell Disease and Frequent Vaso-Occlusive Crises. Am. J. Med. Sci. 2003, 325, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Darbari, D.S.; Wang, Z.; Kwak, M.; Hildesheim, M.; Nichols, J.; Allen, D.; Seamon, C.; Peters-Lawrence, M.; Conrey, A.; Hall, M.K.; et al. Severe Painful Vaso-Occlusive Crises and Mortality in a Contemporary Adult Sickle Cell Anemia Cohort Study. PLoS ONE 2013, 8, e79923. [Google Scholar] [CrossRef] [PubMed]
- Vichinsky, E.P.; Neumayr, L.D.; Earles, A.N.; Williams, R.; Lennette, E.T.; Dean, D.; Nickerson, B.; Orringer, E.; McKie, V.; Bellevue, R.; et al. Causes and Outcomes of the Acute Chest Syndrome in Sickle Cell Disease. N. Engl. J. Med. 2000, 342, 1855–1865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, W.R.; Penberthy, L.T.; Bovbjerg, V.E.; McClish, D.K.; Roberts, J.D.; Dahman, B.; Aisiku, I.P.; Levenson, J.L.; Roseff, S.D. Daily assessment of pain in adults with sickle cell disease. Ann. Intern. Med. 2008, 148, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Van Tuijn, C.F.J.; Sins, J.W.R.; Fijnvandraat, K.; Biemond, B.J. Daily pain in adults with sickle cell disease-a different perspective. Am. J. Hematol. 2017, 92, 179–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zapletal, E.; Rodon, N.; Grabar, N.; Degoulet, P. Methodology of integration of a clinical data warehouse with a clinical information system: the HEGP case. Stud. Health Technol. Inform. 2010, 160, 193–197. [Google Scholar] [PubMed]
- Uzuner, Ö.; South, B.R.; Shen, S.; DuVall, S.L. 2010 i2b2/VA challenge on concepts, assertions, and relations in clinical text. J. Am. Med. Inform. Assoc. 2011, 18, 552–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, S.N.; Weber, G.; Mendis, M.; Gainer, V.; Chueh, H.C.; Churchill, S.; Kohane, I. Serving the enterprise and beyond with informatics for integrating biology and the bedside (i2b2). J. Am. Med. Inform. Assoc. 2010, 17, 124–130. [Google Scholar] [CrossRef] [Green Version]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sørensen, H.T.; von Elm, E.; Langan, S.M.; RECORD Working Committee. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef]
- Trajectories of Biological Values and Vital Parameters: An Observational Cohort Study of Adult Patients with Sickle Cell Disease Hospitalized for a Non-Complicated Vaso-Occlusive Crisis-Python Code, Notebook Tutorials, and All Generated Figures. Available online: https://github.com/SimonBussy/redcvo (accessed on 19 September 2019).
- Canalli, A.A.; Conran, N.; Fattori, A.; Saad, S.T.O.; Costa, F.F. Increased adhesive properties of eosinophils in sickle cell disease. Exp. Hematol. 2004, 32, 728–734. [Google Scholar] [CrossRef]
- Aloisi, A.M.; Aurilio, C.; Bachiocco, V.; Biasi, G.; Fiorenzani, P.; Pace, M.C.; Paci, V.; Pari, G.; Passavanti, G.; Ravaioli, L.; et al. Endocrine consequences of opioid therapy. Psychoneuroendocrinology 2009, 34, S162–S168. [Google Scholar] [CrossRef] [PubMed]
- Brennan, M.J. The effect of opioid therapy on endocrine function. Am. J. Med. 2013, 126, S12–S18. [Google Scholar] [CrossRef] [PubMed]
- Bargoma, E.M.; Mitsuyoshi, J.K.; Larkin, S.K.; Styles, L.A.; Kuypers, F.A.; Test, S.T. Serum C-reactive protein parallels secretory phospholipase A2 in sickle cell disease patients with vasoocclusive crisis or acute chest syndrome. Blood 2005, 105, 3384–3385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballas, S.K.; Smith, E.D. Red blood cell changes during the evolution of the sickle cell painful crisis. Blood 1992, 79, 2154–2163. [Google Scholar] [PubMed]
- Rogovik, A.L.; Li, Y.; Kirby, M.A.; Friedman, J.N.; Goldman, R.D. Admission and length of stay due to painful vasoocclusive crisis in children. Am. J. Med. Sci. 2009, 27, 797–801. [Google Scholar] [CrossRef] [PubMed]
- Pain Frequency, Severity and QT Dispersion in Adult Patients with Sickle Cell Anemia: Correlation with Inflammatory Markers. Available online: https://www.dovepress.com/pain-frequency-severity-and-qt-dispersion-in-adult-patients-with-sickl-peer-reviewed-article-JBM (accessed on 11 July 2018).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Whole Sample | SS Genotype | Other SCD Genotype 4 | p-Value 2 | |
|---|---|---|---|---|
| All included patients | n3 = 164 | n3 = 121 (74.8%) | n3 = 43 (26.2%) | |
| Females | 87 (53.1%) | 63 (52.1%) | 24 (55.8%) | 0.724 |
| Age at first hospital admission | 27 [22; 34] | 26 [22; 32] | 33 [21; 39] | 0.041 |
| Steady state hemoglobin (g/dL) | 9 [8; 10] | 8 [8; 9] | 10 [9.5; 11] | <0.001 |
| Acute chest syndrome 1 | 111 (67.7%) | 93 (76.9%) | 18 (41.9%) | <0.001 |
| Avascular bone necrosis 1 | 37 (22.6%) | 23 (19%) | 14 (32.6%) | 0.089 |
| Retinopathy 1 | 19 (11.6%) | 12 (9.9%) | 7 (16.3%) | 0.275 |
| Leg skin ulceration 1 | 10 (6.1%) | 9 (7.4%) | 1 (2.3%) | 0.457 |
| Ischemic stroke 1 | 6 (3.7%) | 3 (2.5%) | 3 (7%) | 0.186 |
| Dialysis 1 | 2 (1.2%) | 1 (0.8%) | 1 (2.3%) | 0.457 |
| Pulmonary hypertension 1 | 3 (1.8%) | 2 (1.6%) | 1 (2.3%) | 1 |
| Male patients only | m3 = 77 | m3 = 58 (75.3%) | m3 = 19 (24.7%) | |
| Priapism 1 | 13 (16.9%) | 13 (22.4%) | 0 (0%) | 0.030 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veil, R.; Bussy, S.; Looten, V.; Arlet, J.-B.; Pouchot, J.; Jannot, A.-S.; Ranque, B. Trajectories of Biological Values and Vital Parameters: An Observational Cohort Study of Adult Patients with Sickle Cell Disease Hospitalized for a Non-Complicated Vaso-Occlusive Crisis. J. Clin. Med. 2019, 8, 1502. https://doi.org/10.3390/jcm8091502
Veil R, Bussy S, Looten V, Arlet J-B, Pouchot J, Jannot A-S, Ranque B. Trajectories of Biological Values and Vital Parameters: An Observational Cohort Study of Adult Patients with Sickle Cell Disease Hospitalized for a Non-Complicated Vaso-Occlusive Crisis. Journal of Clinical Medicine. 2019; 8(9):1502. https://doi.org/10.3390/jcm8091502
Chicago/Turabian StyleVeil, Raphael, Simon Bussy, Vincent Looten, Jean-Benoît Arlet, Jacques Pouchot, Anne-Sophie Jannot, and Brigitte Ranque. 2019. "Trajectories of Biological Values and Vital Parameters: An Observational Cohort Study of Adult Patients with Sickle Cell Disease Hospitalized for a Non-Complicated Vaso-Occlusive Crisis" Journal of Clinical Medicine 8, no. 9: 1502. https://doi.org/10.3390/jcm8091502