Impact of Quantitative Feedback via High-Fidelity Airway Management Training on Success Rate in Endotracheal Intubation in Undergraduate Medical Students—A Prospective Single-Center Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. The High-Fidelity Airway Management Simulator
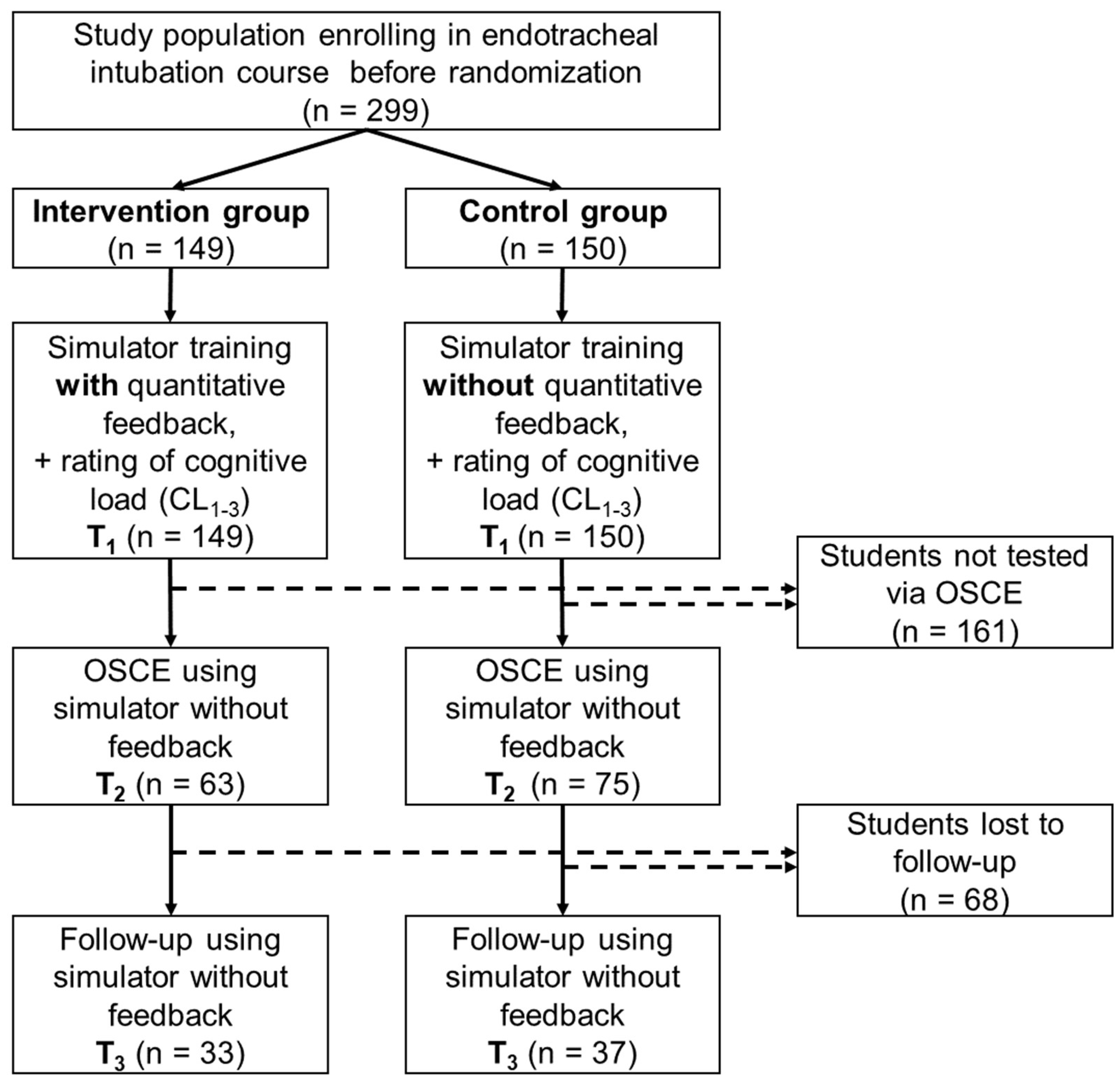
2.2. Study Design
2.3. Data Documentation and Statistical Analysis
3. Results
3.1. Analysis of Average Pressure on Upper Row of Teeth
3.2. Analysis of Correct Pressure Point of the Laryngoscope Spatula on the Tongue
3.3. Analysis of the Correct Position of the Tube after Intubation
3.4. Analysis of Cognitive Load in the Training Session
4. Discussion
4.1. Quality Criteria of Endotracheal Intubation
4.2. Cognitive Load
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CL | Cognitive Load |
| OSCE | Objective Structured Clinical Examination |
| PBL | Problem Based Learning |
References
- Soar, J.; Nolan, J.P.; Böttiger, B.W.; Perkins, G.D.; Lott, C.; Carli, P.; Pellis, T.; Sandroni, C.; Skrifvars, M.B.; Smith, G.B.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 3. Adult advanced life support. Resuscitation 2015, 95, 100–147. [Google Scholar] [CrossRef] [PubMed]
- Higgs, A.; McGrath, B.A.; Goddard, C.; Rangasami, J.; Suntharalingam, G.; Gale, R.; Cook, T.M. Guidelines for the management of tracheal intubation in critically ill adults. Br. J. Anaesth. 2018, 120, 323–352. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, M.; Mohr, S.; Weigand, M.A.; Martin, E.; Walther, A. Developing the skill of endotracheal intubation: Implication for emergency medicine. Acta Anaesthesiol. Scand. 2012, 56, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Buis, M.L.; Maissan, I.M.; Hoeks, S.E.; Klimek, M.; Stolker, R.J. Defining the learning curve for endotracheal intubation using direct laryngoscopy: A systematic review. Resuscitation 2016, 99, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Park, S.O.; Kim, J.W.; Sung, J.; Lee, K.R.; Lee, Y.H.; Hong, D.Y.; Baek, K.J. How much experience do rescuers require to achieve successful tracheal intubation during cardiopulmonary resuscitation? Resuscitation 2018, 133, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Mulcaster, J.T.; Mills, J.; Hung, O.R.; MacQuarrie, K.; Law, J.A.; Pytka, S.; Imrie, D.; Field, C. Laryngoscopic intubation: Learning and performance. Anesthesiology 2003, 98, 23–27. [Google Scholar] [CrossRef]
- Bernhard, M.; Bax, S.N.; Hartwig, T.; Yahiaoui-Doktor, M.; Petros, S.; Bercker, S.; Ramshorn-Zimmer, A.; Gries, A. Airway Management in the Emergency Department (The OcEAN-Study)-a prospective single centre observational cohort study. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 20. [Google Scholar] [CrossRef]
- Wang, E.E.; Quinones, J.; Fitch, M.T.; Dooley-Hash, S.; Griswold-Theodorson, S.; Medzon, R.; Korley, F.; Laack, T.; Robinett, A.; Clay, L. Developing technical expertise in emergency medicine--the role of simulation in procedural skill acquisition. Acad. Emerg. Med. 2008, 15, 1046–1057. [Google Scholar] [CrossRef]
- Yang, D.; Wei, Y.-K.; Xue, F.-S.; Deng, X.-M.; Zhi, J. Simulation-based airway management training: Application and looking forward. J. Anesth. 2016, 30, 284–289. [Google Scholar] [CrossRef]
- Herrmann-Werner, A.; Nikendei, C.; Keifenheim, K.; Bosse, H.M.; Lund, F.; Wagner, R.; Celebi, N.; Zipfel, S.; Weyrich, P. “Best practice” skills lab training vs. a “see one, do one” approach in undergraduate medical education: An RCT on students’ long-term ability to perform procedural clinical skills. PLoS ONE 2013, 8, e76354. [Google Scholar] [CrossRef]
- Kardash, K.; Tessler, M.J. Videotape feedback in teaching laryngoscopy. Can. J. Anaesth. 1997, 44, 54–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.H.; Kim, Y.-M.; Chung, H.S.; Cho, J.; Lee, H.-M.; Kang, G.-H.; Kim, E.-C.; Lim, T.; Cho, Y.S. Comparison of four manikins and fresh frozen cadaver models for direct laryngoscopic orotracheal intubation training. Emerg. Med. J. 2010, 27, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.; Kedarisetty, S.; Delson, N.; Glaser, D.; Moitoza, J.; Davis, D.P.; Hastings, R.H. The effect of cross-training with adjustable airway model anatomies on laryngoscopy skill transfer. Anesth. Analg. 2011, 113, 862–868. [Google Scholar] [CrossRef] [PubMed]
- Ende, J. Feedback in clinical medical education. JAMA 1983, 250, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Hattie, J. Visible Learning. A Synthesis of over 800 Meta-Analyses Relating to Achievement, 1st ed.; Routledge Taylor & Francis: London, UK, 2009; ISBN 9780203887332. [Google Scholar]
- Van der Leeuw, R.M.; Slootweg, I.A. Twelve tips for making the best use of feedback. Med. Teach. 2013, 35, 348–351. [Google Scholar] [CrossRef] [PubMed]
- Ramani, S.; Krackov, S.K. Twelve tips for giving feedback effectively in the clinical environment. Med. Teach. 2012, 34, 787–791. [Google Scholar] [CrossRef] [PubMed]
- Sweller, J. Cognitive Load During Problem Solving: Effects on Learning. Cogn. Sci. 1988, 12, 257–285. [Google Scholar] [CrossRef]
- Leppink, J.; van Heuvel, A.D. The evolution of cognitive load theory and its application to medical education. Perspect. Med. Educ. 2015, 4, 119–127. [Google Scholar] [CrossRef] [Green Version]
- Van Merrienboer, J.J.G.; Sweller, J. Cognitive load theory in health professional education: Design principles and strategies. Med. Educ. 2010, 44, 85–93. [Google Scholar] [CrossRef]
- Ayres, P.; Paas, F. Interdisciplinary Perspectives Inspiring a New Generation of Cognitive Load Research. Educ Psychol. Rev. 2009, 21, 1–9. [Google Scholar] [CrossRef]
- Paas, F.G. Training strategies for attaining transfer of problem-solving skill in statistics: A cognitive-load approach. J. Educ. Psychol. 1992, 84, 429–434. [Google Scholar] [CrossRef]
- Hibbeler, B.; Korziliusmk, H. Die Medizin wird weiblich. Dtsch. Arztebl. 2008, 105, 609–612. [Google Scholar]
- Yasny, J.S. Perioperative dental considerations for the anesthesiologist. Anesth. Analg. 2009, 108, 1564–1573. [Google Scholar] [CrossRef] [PubMed]
- Newland, M.C.; Ellis, S.J.; Peters, K.R.; Simonson, J.A.; Durham, T.M.; Ullrich, F.A.; Tinker, J.H. Dental injury associated with anesthesia: A report of 161,687 anesthetics given over 14 years. J. Clin. Anesth. 2007, 19, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Mourao, J.; Neto, J.; Luis, C.; Moreno, C.; Barbosa, J.; Carvalho, J.; Tavares, J. Dental injury after conventional direct laryngoscopy: A prospective observational study. Anaesthesia 2013, 68, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- Vogel, J.; Stubinger, S.; Kaufmann, M.; Krastl, G.; Filippi, A. Dental injuries resulting from tracheal intubation--a retrospective study. Dent. Traumatol. 2009, 25, 73–77. [Google Scholar] [CrossRef]
- Fukuda, T.; Sugimoto, Y.; Yamashita, S.; Toyooka, H.; Tanaka, M. Forces applied to the maxillary incisors during tracheal intubation and dental injury risks of intubation by beginners: A manikin study. Acta Anaesthesiol. Taiwan. 2011, 49, 12–15. [Google Scholar] [CrossRef]
- Garcia, J.; Coste, A.; Tavares, W.; Nuno, N.; Lachapelle, K. Assessment of competency during orotracheal intubation in medical simulation. Br. J. Anaesth. 2015, 115, 302–307. [Google Scholar] [CrossRef]
- Al Shawwa, L.; Abulaban, A.A.; Abulaban, A.A.; Merdad, A.; Baghlaf, S.; Algethami, A.; Abu-Shanab, J.; Balkhoyor, A. Factors potentially influencing academic performance among medical students. Adv. Med. Educ. Pract. 2015, 6, 65–75. [Google Scholar] [CrossRef] [Green Version]
- Bosse, H.M.; Mohr, J.; Buss, B.; Krautter, M.; Weyrich, P.; Herzog, W.; Junger, J.; Nikendei, C. The benefit of repetitive skills training and frequency of expert feedback in the early acquisition of procedural skills. BMC Med. Educ. 2015, 15, 22. [Google Scholar] [CrossRef]
- Fraser, K.L.; Ayres, P.; Sweller, J. Cognitive Load Theory for the Design of Medical Simulations. Simul. Healthc. 2015, 10, 295–307. [Google Scholar] [CrossRef] [PubMed]
- Wulf, G.; Shea, C.; Lewthwaite, R. Motor skill learning and performance: A review of influential factors. Med. Educ. 2010, 44, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Brydges, R.; Carnahan, H.; Safir, O.; Dubrowski, A. How effective is self-guided learning of clinical technical skills? It’s all about process. Med. Educ. 2009, 43, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Young, J.Q.; van Merrienboer, J.; Durning, S.; Cate, O. ten. Cognitive Load Theory: Implications for medical education: AMEE Guide No. 86. Med. Teach. 2014, 36, 371–384. [Google Scholar] [CrossRef] [PubMed]
- Leppink, J.; Duvivier, R. Twelve tips for medical curriculum design from a cognitive load theory perspective. Med. Teach. 2016. [Google Scholar] [CrossRef]
- Paas, F.; Tuovinen, J.E.; Tabbers, H.; Van Gerven, P.W.M. Cognitive Load Measurement as a Means to Advance Cognitive Load Theory. Educ. Psychol. 2003, 38, 63–71. [Google Scholar] [CrossRef]
- Paas, F.; Van Merriënboer, J. Instructional control of cognitive load in the training of complex cognitive tasks. Educ. Psychol. Rev. 1994, 6, 351–371. [Google Scholar] [CrossRef]
- Sorbello, M.; Afshari, A.; de Hert, S. Device or target? A paradigm shift in airway management: Implications for guidelines, clinical practice and teaching. Eur. J. Anaesthesiol. 2018, 35, 811–814. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| n | Intervention Group | n | Control Group | Intervention vs. Control | |
|---|---|---|---|---|---|
| training (T1) | 149 | 57.47 (± 60.032) | 150 | 58.09 (± 62.915) | p = 0.941 |
| examination (T2) | 63 | 48.35 (± 52.344) | 75 | 47.64 (± 60.843) | p = 0.519 |
| follow-up (T3) | 33 | 58.85 (± 45.640) | 37 | 51.81 (± 46.449) | p = 0.469 |
| n | Intervention Group | n | Control Group | Intervention vs. Control | |
|---|---|---|---|---|---|
| training (T1) | 149 | 60.4% (n = 90) | 150 | 52.7% (n = 79) | p = 0.177 |
| examination (T2) | 63 | 85.7% (n = 54) | 75 | 76.0% (n = 57) | p = 0.152 |
| follow up (T3) | 33 | 63.6% (n = 21) | 37 | 89.2% (n = 33) | p = 0.011 |
| n | Intervention Group | n | Control Group | Intervention vs. Control | |
|---|---|---|---|---|---|
| training (T1) | 149 | 67.8% (n = 101) | 150 | 58.7% (n = 88) | p = 0.102 |
| examination (T2) | 63 | 55.6% (n = 35) | 75 | 54.7% (n = 41) | p = 0.917 |
| follow up (T3) | 33 | 42.4% (n = 14) | 37 | 43.2% (n = 16) | p = 0.945 |
| Intervention Group | Control Group | Intervention vs. Control | |
|---|---|---|---|
| cognitive load (CL1) | 2.79 (± 1.291) | 2.85 (± 1.353) | p = 0.688 |
| cognitive load (CL2) | 3.66 (± 1.441) | 3.43 (± 1.472) | p = 0.159 |
| cognitive load (CL3) | 4.75 (± 1.774) | 4.19 (± 1.860) | p = 0.008 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hempel, G.; Heinke, W.; Struck, M.F.; Piegeler, T.; Rotzoll, D. Impact of Quantitative Feedback via High-Fidelity Airway Management Training on Success Rate in Endotracheal Intubation in Undergraduate Medical Students—A Prospective Single-Center Study. J. Clin. Med. 2019, 8, 1465. https://doi.org/10.3390/jcm8091465
Hempel G, Heinke W, Struck MF, Piegeler T, Rotzoll D. Impact of Quantitative Feedback via High-Fidelity Airway Management Training on Success Rate in Endotracheal Intubation in Undergraduate Medical Students—A Prospective Single-Center Study. Journal of Clinical Medicine. 2019; 8(9):1465. https://doi.org/10.3390/jcm8091465
Chicago/Turabian StyleHempel, Gunther, Wolfgang Heinke, Manuel F. Struck, Tobias Piegeler, and Daisy Rotzoll. 2019. "Impact of Quantitative Feedback via High-Fidelity Airway Management Training on Success Rate in Endotracheal Intubation in Undergraduate Medical Students—A Prospective Single-Center Study" Journal of Clinical Medicine 8, no. 9: 1465. https://doi.org/10.3390/jcm8091465
APA StyleHempel, G., Heinke, W., Struck, M. F., Piegeler, T., & Rotzoll, D. (2019). Impact of Quantitative Feedback via High-Fidelity Airway Management Training on Success Rate in Endotracheal Intubation in Undergraduate Medical Students—A Prospective Single-Center Study. Journal of Clinical Medicine, 8(9), 1465. https://doi.org/10.3390/jcm8091465