Analogical and Digital Workflow in the Design and Preparation of the Emergence Profile of Biologically Oriented Preparation Technique (BOPT) Crowns over Implants in the Working Model

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Description of the Technique
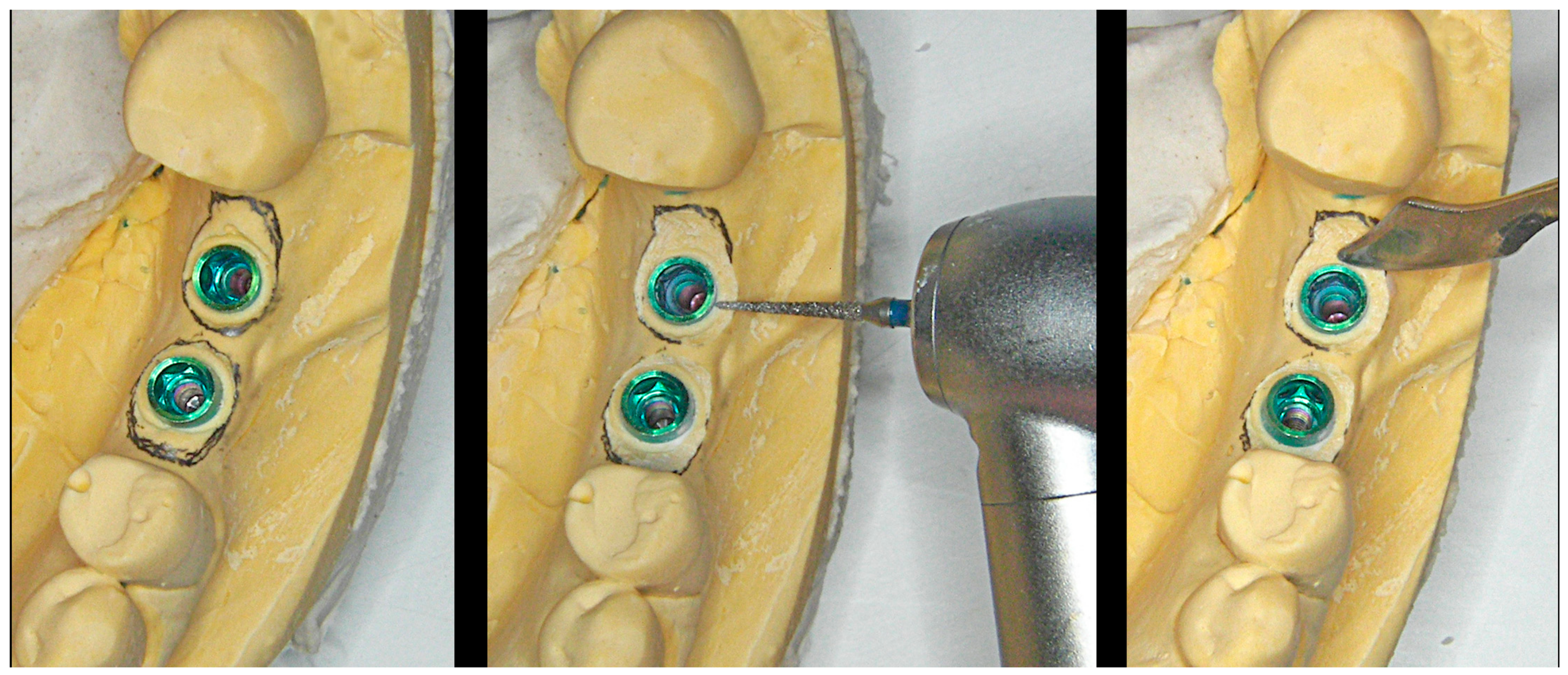
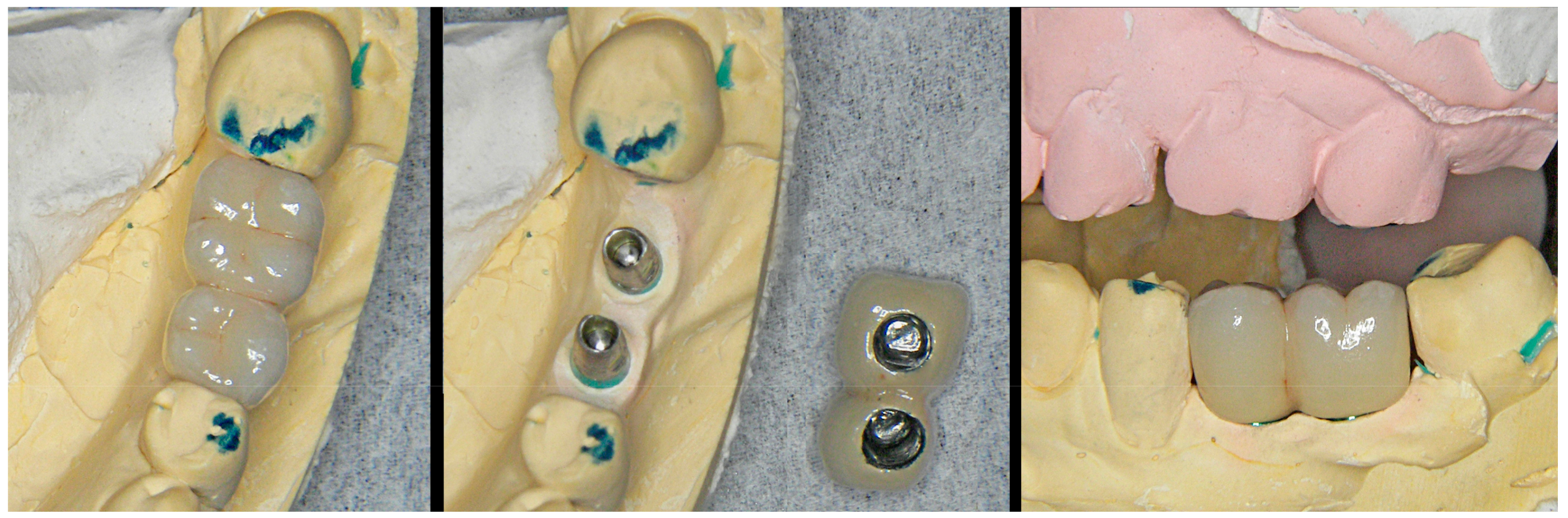
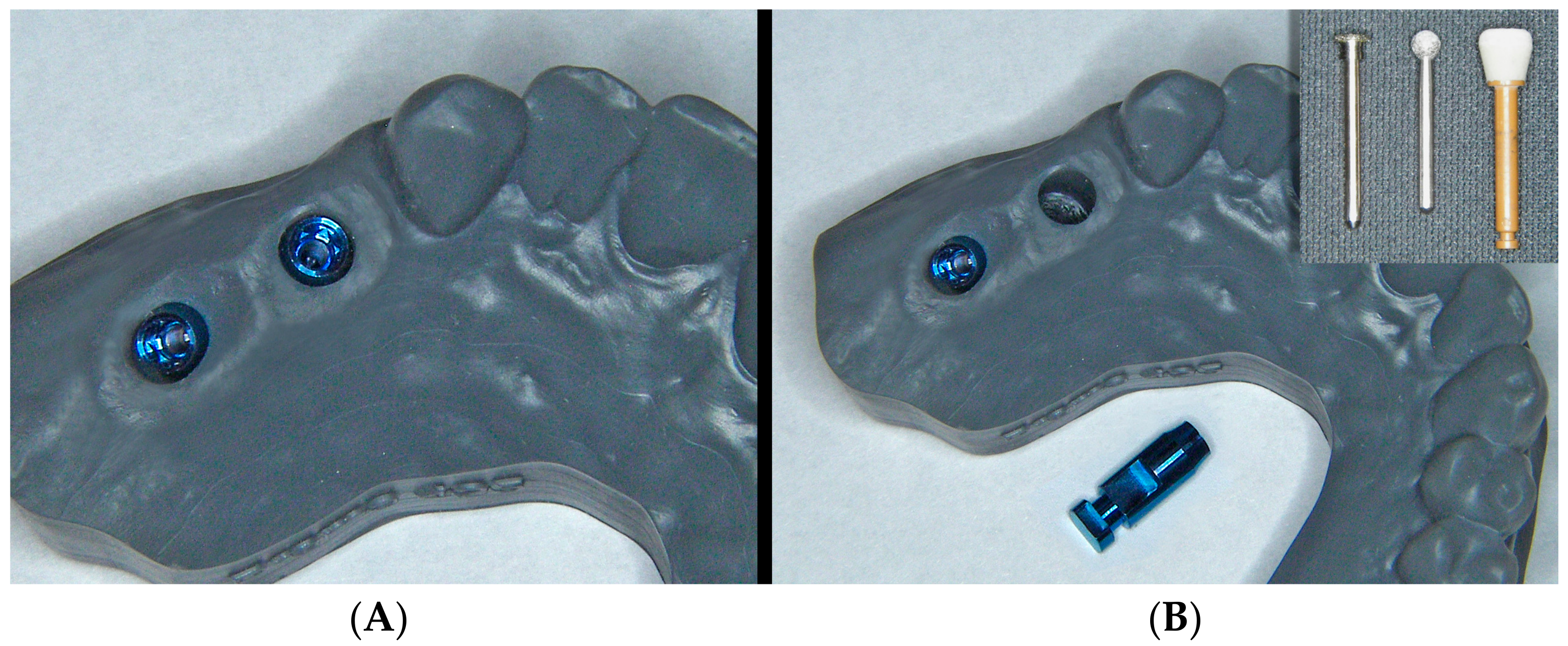
3. Analogical Workflow
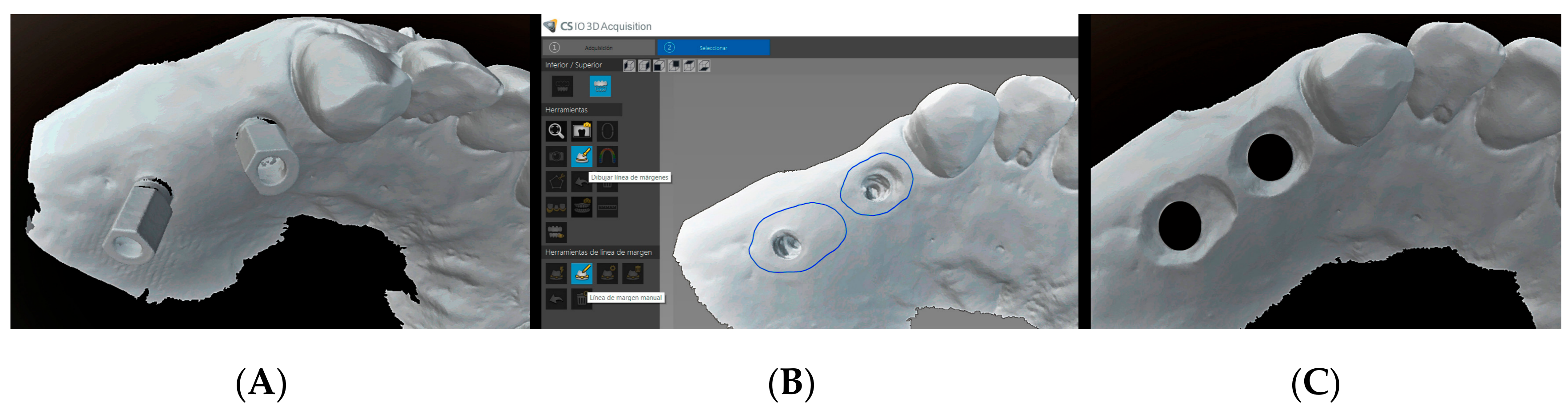
4. Digital Workflow
5. Discussion
6. Conclusions
Author Contributions
Conflicts of Interest
References
- Loi, I.; Scutellà, F.; Galli, F. Tecnica di preparazione orientata biologicamente (BOPT). Un nuovo approccio nella preparazione protesica in odontostomatologia. Quintessenza Internazionale 2008, 5, 69–75. Available online: https://www.researchgate.net/publication/285243228_Tecnica_di_preparazione_orientata_biologicamente_BOPT_Un_nuovo_approccio_nella_preparazione_protesica_in_odontostomatologia (accessed on 9 August 2019).
- Loi, I. Protesi su denti naturali nei settori di rilevanza estetica con tecnica BOPT: Case series report. Dental Cadmos. 2008, 76, 51–59. [Google Scholar]
- Loi, I.; Galli, F.; Scutellà, F.; Felice, A. Il contorno coronale protesico con tecnica di preparazione BOPT (Biologically Oriented Preparation Technique): Considerazioni tecniche. Quintessenza Internazionale 2009, 25, 4–19. Available online: https://www.researchgate.net/publication/285361620_Il_contorno_coronale_protesico_con_tecnica_di_preparazione_BOPT_Biologically_Oriented_Preparation_Technique_Considerazioni_tecniche (accessed on 9 August 2019).
- Loi, I.; Felice, A. Biologically oriented preparation technique (BOPT): A new approach for prosthetic restoration of periodontically halthy teeth. Eur. J. Esthet. Dent. 2013, 8, 10–23. [Google Scholar] [PubMed]
- Serra-Pastor, B.; Loi, I.; Fons-Font, A.; Solá-Ruíz, M.F.; Agustín-Panadero, R. Periodontal and prosthetic outcomes on teeth prepared with biologically oriented preparation technique: A 4-year follow-up prospective clinical study. J. Prosthodont. Res. 2019. [Google Scholar] [CrossRef]
- Cabanes-Gumbau, G.; Pascual-Moscardo, A.; Penarrocha-Oltra, D.; Garcia-Mira, B.; Aizcorbe-Vicente, J.; Penarrocha-Diago, M. Volumetric variation of peri-implant soft tissues in convergent collar implants and crowns using the biologically oriented preparation technique (BOPT). Med. Oral Patol. Oral Cir. Bucal 2019, 24, e643–e651. [Google Scholar] [CrossRef]
- Su, H.; Gonzalez-Martin, O.; Weisgold, A.; Lee, E. Considerations of implant abutment and crown contour: Critical contour and subcritical contour. Int. J. Periodontics Restor. Dent. 2010, 30, 335–343. [Google Scholar]
- Díaz-Sánchez, M.; Soto-Peñaloza, D.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M. Influence of supracrestal tissue attachment thickness on radiographic bone level around dental implants: A systematic review and meta-analysis. J. Periodontal. Res. 2019. [Google Scholar] [CrossRef]
- Rodriguez, X.; Vela, X.; Segalà, M.; Perez, J.; Pons, L.; Loi, I. Examen histológico humano de la respuesta de los tejidos al tallado vertical y provisionalización inmediata (BOPT). Fundamento biológico. Periodoncia Clínica 2019, 12, 47–58. [Google Scholar]
- Testori, T.; Weinstein, T.; Scutellà, F.; Wang, H.L.; Zucchelli, G. Implant placement in the esthetic area: Criteria for positioning single and multiple implants. Periodontology 2000, 2018, 176–196. [Google Scholar] [CrossRef]
- Cabanes, G. Perfil de emergencia y sellado mucoso en coronas BOPT sobre implantes PRAMA. Available online: http://www.cooecs.es/perfil-de-emergencia-y-sellado-mucoso-en-coronas-b-o-p-t-sobre-implantes-prama/ (accessed on 9 August 2019).
- Cabanes, G.; Alapont, V. Rehabilitación oral con implantes transmucosos de cabeza convergente. Available online: https://gacetadental.com/2018/02/rehabilitacion-oral-implantes-transmucosos-cabeza-convergente-69979/ (accessed on 9 August 2019).
- Cabanes, G. Experiencia en clínica de la técninca BOPT sobre implantes: preparación vertical de pilares y conformación de la emergencia coronaria. In Protocolo clínico-protésico de la técnica BOPT; Agustín, R., Chust, C., Eds.; Ediciones Especializadas Europeas: Barcelona, Spain, 2016; pp. 205–213. [Google Scholar]
- Rattanapanich, P.; Aunmeungtong, W.; Chaijareenont, P.; Khongkhunthian, P. Comparative Study between an Immediate Loading Protocol Using the Digital Workflow and a Conventional Protocol for Dental Implant Treatment: A Randomized Clinical Trial. J. Clin. Med. 2019, 8, 622. [Google Scholar] [CrossRef] [PubMed]
- Lo Russo, L.; Caradonna, G.; Biancardino, M.; De Lillo, A.; Troiano, G.; Guida, L. Digital versus conventional workflow for the fabrication of multiunit fixed prostheses: A systematic review and meta-analysis of vertical marginal fit in controlled in vitro studies. J. Prosthet. Dent. 2019. [Google Scholar] [CrossRef] [PubMed]
- Rebong, R.E.; Stewart, K.T.; Utreja, A.; Ghoneima, A.A. Accuracy of three-dimensional dental resin models created by fused deposition modeling, stereolithography, and Polyjet prototype technologies: A comparative study. Angle Orthod. 2018, 88, 363–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Javaid, M.; Haleem, A. Current status and applications of additive manufacturing in dentistry: A literature-based review. J. Oral Biol. Craniofacial Res. 2019, 9, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Mackay, M.M.; Fallah, M.; Danyal, T. Acquisition of a Digital Intraoral Scanning Device: An Examination of Practice Volume Changes and the Economic Impact via an Interrupted Time Series Analysis. J. Clin. Dent. 2017, 28, S1–S5. [Google Scholar] [PubMed]
- Patzelt, S.B.; Lamprinos, C.; Stampf, S.; Att, W. The time efficiency of intraoral scanners: an in vitro comparative study. J. Am. Dent. Assocc. 2014, 145, 542–551. [Google Scholar] [CrossRef]
- Resnick, C.M.; Doyle, M.; Calabrese, C.E.; Sanchez, K.; Padwa, B.L. Is It Cost Effective to Add an Intraoral Scanner to an Oral and Maxillofacial Surgery Practice? J. Oral Maxillofac. Surg. 2019, 77, 1687–1694. [Google Scholar] [CrossRef]
- Canullo, L.; Di Domenico, A.; Marinotti, F.; Menini, M.; Pesce, P. Soft Tissue Contour Impression with Analogic or Digital Work Flow: A Case Report. Int. J. Environ. Res. Public Heal. 2018, 15, 2623. [Google Scholar] [CrossRef]
- Chopra, A.; Sivaraman, K.; Narayan, A.I.; Balakrishnan, D. Etiology and classification of food impaction around implants and implant-retained prosthesis. Clin. Implant. Dent. Relat. Res. 2019, 21, 391–397. [Google Scholar] [CrossRef]
- Bidra, A.S. Nonsurgical management of inflammatory periimplant disease caused by food impaction: A clinical report. J. Prosthet. Dent. 2014, 111, 96–100. [Google Scholar] [CrossRef]
- Hirschfeld, I. Food impaction. J. Am. Dent. Assoc. 1930, 17, 1504–1511. [Google Scholar]














© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabanes-Gumbau, G.; Soto-Peñaloza, D.; Peñarrocha-Diago, M.; Peñarrocha-Diago, M. Analogical and Digital Workflow in the Design and Preparation of the Emergence Profile of Biologically Oriented Preparation Technique (BOPT) Crowns over Implants in the Working Model. J. Clin. Med. 2019, 8, 1452. https://doi.org/10.3390/jcm8091452
Cabanes-Gumbau G, Soto-Peñaloza D, Peñarrocha-Diago M, Peñarrocha-Diago M. Analogical and Digital Workflow in the Design and Preparation of the Emergence Profile of Biologically Oriented Preparation Technique (BOPT) Crowns over Implants in the Working Model. Journal of Clinical Medicine. 2019; 8(9):1452. https://doi.org/10.3390/jcm8091452
Chicago/Turabian StyleCabanes-Gumbau, Guillermo, David Soto-Peñaloza, Miguel Peñarrocha-Diago, and María Peñarrocha-Diago. 2019. "Analogical and Digital Workflow in the Design and Preparation of the Emergence Profile of Biologically Oriented Preparation Technique (BOPT) Crowns over Implants in the Working Model" Journal of Clinical Medicine 8, no. 9: 1452. https://doi.org/10.3390/jcm8091452