Acute Kidney Injury and In-Hospital Mortality: A Retrospective Analysis of a Nationwide Administrative Database of Elderly Subjects in Italy

 ,
, 
 ,
, 
Abstract
:1. Introduction
2. Experimental Section
2.1. Patient Selection and Eligibility
2.2. Data Analysis
2.3. Statistical Analysis
2.4. Ethical Issues
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fabbian, F.; De Giorgi, A.; Maietti, E.; Gallerani, M.; Pala, M.; Cappadona, R.; Manfredini, R.; Fedeli, U. A modified Elixhauser score for predicting in-hospital mortality in internal medicine admissions. Eur. J. Intern. Med. 2017, 40, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Hounkpatin, H.O.; Fraser, S.D.S.; Glidewell, L.; Blakeman, T.; Lewington, A.; Roderick, P.J. Predicting risk of recurrent acute kidney injury: A systematic review. Nephron 2019, 142, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Mishra, G.D.; Jones, M. Evidence on multimorbidity from definition to intervention: An overview of systematic reviews. Ageing Res. Rev. 2017, 37, 53–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klompstra, L.; Ekdahl, A.W.; Krevers, B.; Milberg, A.; Eckerblad, J. Factors related to health-related quality of life in older people with multimorbidity and high health care consumption over a two-year period. BMC Geriatr. 2019, 19, 187. [Google Scholar] [CrossRef] [PubMed]
- Millá-Perseguer, M.; Guadalajara-Olmeda, N.; Vivas-Consuelo, D.; Usó-Talamantes, R. Measurement of health-related quality by multimorbidity groups in primary health care. Health Qual. Life Outcomes 2019, 17, 8. [Google Scholar] [CrossRef] [PubMed]
- Fabbian, F.; Pala, M.; De Giorgi, A.; Manfredini, F.; Mallozzi Menegatti, A.; Salmi, R.; Portaluppi, F.; Gallerani, M.; Manfredini, R. In-hospital mortality in patients with renal dysfunction admitted for myocardial infarction: The Emilia-Romagna region of Italy database of hospital admissions. Int. Urol. Nephrol. 2013, 45, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Fabbian, F.; Gallerani, M.; Pala, M.; De Giorgi, A.; Salmi, R.; Manfredini, F.; Portaluppi, F.; Dentali, F.; Ageno, W.; Mikhailidis, D.P.; et al. In-hospital mortality for pulmonary embolism: Relationship with chronic kidney disease and end-stage renal disease. The hospital admission and discharge database of the Emilia Romagna region of Italy. Intern. Emerg. Med. 2013, 8, 735–740. [Google Scholar]
- Fabbian, F.; Gallerani, M.; Pala, M.; De Giorgi, A.; Salmi, R.; Dentali, F.; Ageno, W.; Manfredini, R. Association between in-hospital mortality and renal dysfunction in 186 219 patients hospitalized for acute stroke in the Emilia-Romagna region of Italy. Angiology 2014, 65, 906–910. [Google Scholar] [CrossRef]
- Fabbian, F.; De Giorgi, A.; Manfredini, F.; Lamberti, N.; Forcellini, S.; Storari, A.; Gallerani, M.; Caramori, G.; Manfredini, R. Impact of renal dysfunction on in-hospital mortality of patients with severe chronic obstructive pulmonary disease: A single-center Italian study. Int. Urol. Nephrol. 2016, 48, 1121–1127. [Google Scholar] [CrossRef]
- Chertow, G.M.; Burdick, E.; Honour, M.; Bonventre, J.V.; Bates, D.W. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J. Am. Soc. Nephrol. 2005, 16, 3365–7330. [Google Scholar] [CrossRef] [PubMed]
- Silver, S.A.; Long, J.; Zheng, Y.; Chertow, G.M. Cost of Acute Kidney Injury in Hospitalized Patients. J. Hosp. Med. 2017, 12, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Gijsen, R.; Hoeymans, N.; Schellevis, F.G.; Ruwaard, D.; Satariano, W.A.; van den Bos, G.A. Causes and consequences of comorbidity: A review. J. Clin. Epidemiol. 2001, 54, 661–674. [Google Scholar] [CrossRef]
- Elixhauser, A.; Steiner, C.; Harris, D.R.; Coffey, R.M. Comorbidity measures for use with administrative data. Med. Care 1998, 36, 8–27. [Google Scholar] [CrossRef] [PubMed]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Randall, G.K.; Martin, P.; Bishop, A.J.; Poon, L.W.; Johnson, M.A. Age differences and changes in resources essential to aging well: A comparison of sexagenarians, octogenarians, and centenarians. Curr. Gerontol. Geriatr. Res. 2011, 2011, 357896. [Google Scholar] [CrossRef] [PubMed]
- Santoni, G.; Angleman, S.; Welmer, A.K.; Mangialasche, F.; Marengoni, A.; Fratiglioni, L. Age-related variation in health status after age 60. PLoS ONE 2015, 10, e0120077. [Google Scholar]
- Ge, S.; Nie, S.; Liu, Z.; Chen, C.; Zha, Y.; Qian, J.; Liu, B.; Teng, S.; Xu, A.; Bin, W.; et al. Epidemiology and outcomes of acute kidney injury in elderly Chinese patients: A subgroup analysis from the EACH study. BMC Nephrol. 2016, 17, 136. [Google Scholar] [CrossRef]
- Chao, C.T.; Tsai, H.B.; Wu, C.Y.; Lin, Y.F.; Hsu, N.C.; Chen, J.S.; Hung, K.Y. Cumulative cardiovascular polypharmacy is associated with the risk of acute kidney injury in elderly patients. Medicine 2015, 94, e1251. [Google Scholar] [CrossRef]
- Gong, Y.; Zhang, F.; Ding, F.; Gu, Y. Elderly patients with acute kidney injury (AKI): Clinical features and risk factors for mortality. Arch. Gerontol. Geriatr. 2012, 54, e47–e51. [Google Scholar] [CrossRef]
- Fabbian, F.; De Giorgi, A.; Boari, B.; Misurati, E.; Gallerani, M.; Cappadona, R.; Cultrera, R.; Manfredini, R.; Rodrìguez Borrego, M.A.; Lopez-Soto, P.J. Infections and internal medicine patients: Could a comorbidity score predict in-hospital mortality? Medicine 2018, 97, e12818. [Google Scholar] [CrossRef] [PubMed]
- Grimes, D.A. Epidemiologic research using administrative databases—Garbage in, garbage out. Obstet. Gynecol. 2010, 116, 1018–1019. [Google Scholar] [CrossRef] [PubMed]
- Lameire, N.H.; Bagga, A.; Cruz, D.; De Maeseneer, J.; Endre, Z.; Kellum, J.A.; Liu, K.D.; Mehta, R.L.; Pannu, N.; Van Biesen, W.; et al. Acute kidney injury: An increasing global concern. Lancet 2013, 382, 170–179. [Google Scholar] [CrossRef]
- Moore, P.K.; Hsu, R.K.; Liu, K.D. Management of acute kidney injury: Core curriculum 2018. Am. J. Kidney Dis. 2018, 72, 136–148. [Google Scholar] [CrossRef] [PubMed]
- Joannidis, M.; Metnitz, B.; Bauer, P.; Schusterschitz, N.; Moreno, R.; Druml, W.; Metnitz, P.G. Acute kidney injury in critically ill patients classified by AKIN versus RIFLE using the SAPS 3 database. Intensive Care Med. 2009, 35, 1692–1702. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, J.; Fonseca, J.A.; Jorge, S.; Lopes, J.A. Acute Kidney Injury Definition and Diagnosis: A Narrative Review. J. Clin. Med. 2018, 7, 307. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.-C.; Shiao, C.-C.; Chi, N.-H.; Wang, C.-H.; Chueh, S.-C.J.; Liou, H.-H.; Spapen, H.D.; Honore, P.M.; Chu, T.-S. Outcome Prediction of Acute Kidney Injury Biomarkers at Initiation of Dialysis in Critical Units. J. Clin. Med. 2018, 7, 202. [Google Scholar] [CrossRef]
- Douvris, A.; Zeid, K.; Hiremath, S.; Brown, P.A.; Sood, M.M.; Abou Arkoub, R.; Malhi, G.; Clark, E.G. Safety Lapses Prior to Initiation of Hemodialysis for Acute Kidney Injury in Hospitalized Patients: A Patient Safety Initiative. J. Clin. Med. 2018, 7, 317. [Google Scholar] [CrossRef]
- Hsu, R.K.; McCulloch, C.E.; Dudley, R.A.; Lo, L.J.; Hsu, C.Y. Temporal changes in incidence of dialysis-requiring AKI. J. Am. Soc. Nephrol. 2013, 24, 37–42. [Google Scholar] [CrossRef]
- Waikar, S.S.; Curhan, G.C.; Wald, R.; McCarthy, E.P.; Chertow, G.M. Declining mortality in patients with acute renal failure, 1988 to 2002. J. Am. Soc. Nephrol. 2006, 17, 1143–1150. [Google Scholar] [CrossRef]
- Liangos, O.; Wald, R.; O’Bell, J.W.; Price, L.; Pereira, B.J.; Jaber, B.L. Epidemiology and outcomes of acute renal failure in hospitalized patients: A national survey. Clin. J. Am. Soc. Nephrol. 2006, 1, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Thakar, C.V.; Arrigain, S.; Worley, S.; Yared, J.P.; Paganini, E.P. A clinical score to predict acute renal failure after cardiac surgery. J. Am. Soc. Nephrol. 2005, 16, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.A.; Himmelfarb, J.; Tolkoff-Rubin, N.; Chandran, P.; Wingard, R.L.; Hakim, R.M. Prognosis of patients with acute renal failure requiring dialysis: Results of a multicenter study. Am. J. Kidney Dis. 1998, 32, 432–443. [Google Scholar] [CrossRef]
- Fiaccadori, E.; Maggiore, U.; Lombardi, M.; Leonardi, S.; Rotelli, C.; Borghetti, A. Predicting patient outcome from acute renal failure comparing three general severity of illness scoring systems. Kidney Int. 2000, 58, 283–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, J.L.; Daniels, F.; Star, R.A.; Kimmel, P.L.; Eggers, P.W.; Molitoris, B.A.; Himmelfarb, J.; Collins, A.J. Incidence and mortality of acute renal failure in Medicare beneficiaries, 1992 to 2001. J. Am. Soc. Nephrol. 2006, 17, 1135–1142. [Google Scholar] [CrossRef]
- Coca, S.G.; Peixoto, A.J.; Garg, A.X.; Krumholz, H.M.; Parikh, C.R. The prognostic importance of a small acute decrement in kidney function in hospitalized patients: A systematic review and meta-analysis. Am. J. Kidney Dis. 2007, 50, 712–720. [Google Scholar] [CrossRef]
- Liaño, F.; Pascual, J. Epidemiology of acute renal failure: A prospective, multicenter, community-based study. Madrid Acute Renal Failure Study Group. Kidney Int. 1996, 50, 811–818. [Google Scholar] [CrossRef]
- Chertow, G.M.; Soroko, S.H.; Paganini, E.P.; Cho, K.C.; Himmelfarb, J.; Ikizler, T.A.; Mehta, R.L. Mortality after acute renal failure: Models for prognostic stratification and risk adjustment. Kidney Int. 2006, 70, 1120–1126. [Google Scholar] [CrossRef] [Green Version]
- Bouchard, J.; Soroko, S.B.; Chertow, G.M.; Himmelfarb, J.; Ikizler, T.A.; Paganini, E.P.; Mehta, R.L. Fluid accumulation, survival and recovery of kidney function in critically ill patients with acute kidney injury. Kidney Int. 2009, 76, 422–427. [Google Scholar] [CrossRef] [Green Version]
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO. clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138.
- Mazzali, C.; Duca, P. Use of administrative data in healthcare research. Intern. Emerg. Med. 2015, 10, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Waikar, S.S.; Wald, R.; Chertow, G.M.; Curhan, G.C.; Winkelmayer, W.C.; Liangos, O.; Sosa, M.A.; Jaber, B.L. Validity of International Classification of Diseases, Ninth Revision, Clinical Modification Codes for Acute Renal Failure. J. Am. Soc. Nephrol. 2006, 17, 1688–1694. [Google Scholar] [CrossRef] [PubMed]
- Vlasschaert, M.E.; Bejaimal, S.A.; Hackam, D.G.; Quinn, R.; Cuerden, M.S.; Oliver, M.J.; Iansavichus, A.; Sultan, N.; Mills, A.; Garg, A.X. Validity of administrative database coding for kidney disease: A systematic review. Am. J. Kidney Dis. 2011, 57, 29–43. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, L.A.; Riding, A.M.; Payne, R.A.; Abel, G.A.; Tomson, C.R.; Wilkinson, I.B.; Roland, M.O.; Chaudhry, A.N. The accuracy of diagnostic coding for acute kidney injury in England—A single centre study. BMC Nephrol. 2013, 14, 58. [Google Scholar] [CrossRef] [PubMed]
- Grams, M.E.; Waikar, S.S.; MacMahon, B.; Whelton, S.; Ballew, S.H.; Coresh, J. Performance and limitations of administrative data in the identification of AKI. Clin. J. Am. Soc. Nephrol. 2014, 9, 682–689. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Items | Score |
|---|---|
| Age 0–60 (years) | 0 |
| Age 61–70 (years) | 3 |
| Age 71–80 (years) | 7 |
| Age 81–90 (years) | 11 |
| Age 91+ (years) | 16 |
| Chronic kidney disease | 1 |
| Male gender | 2 |
| Neurological disorders | 3 |
| Lymphoma | 4 |
| Solid tumor without metastasis | 4 |
| Ischemic heart disease | 5 |
| Congestive heart failure | 5 |
| Coagulopathy | 8 |
| Fluid and electrolyte disorders | 8 |
| Liver disease | 10 |
| Cachexia | 11 |
| Metastatic cancer | 12 |
| Total Number of Records | 760,664 |
|---|---|
| Men, (n (%)) | 397,174 (52.2) |
| Women, (n (%)) | 363,490 (47.8) |
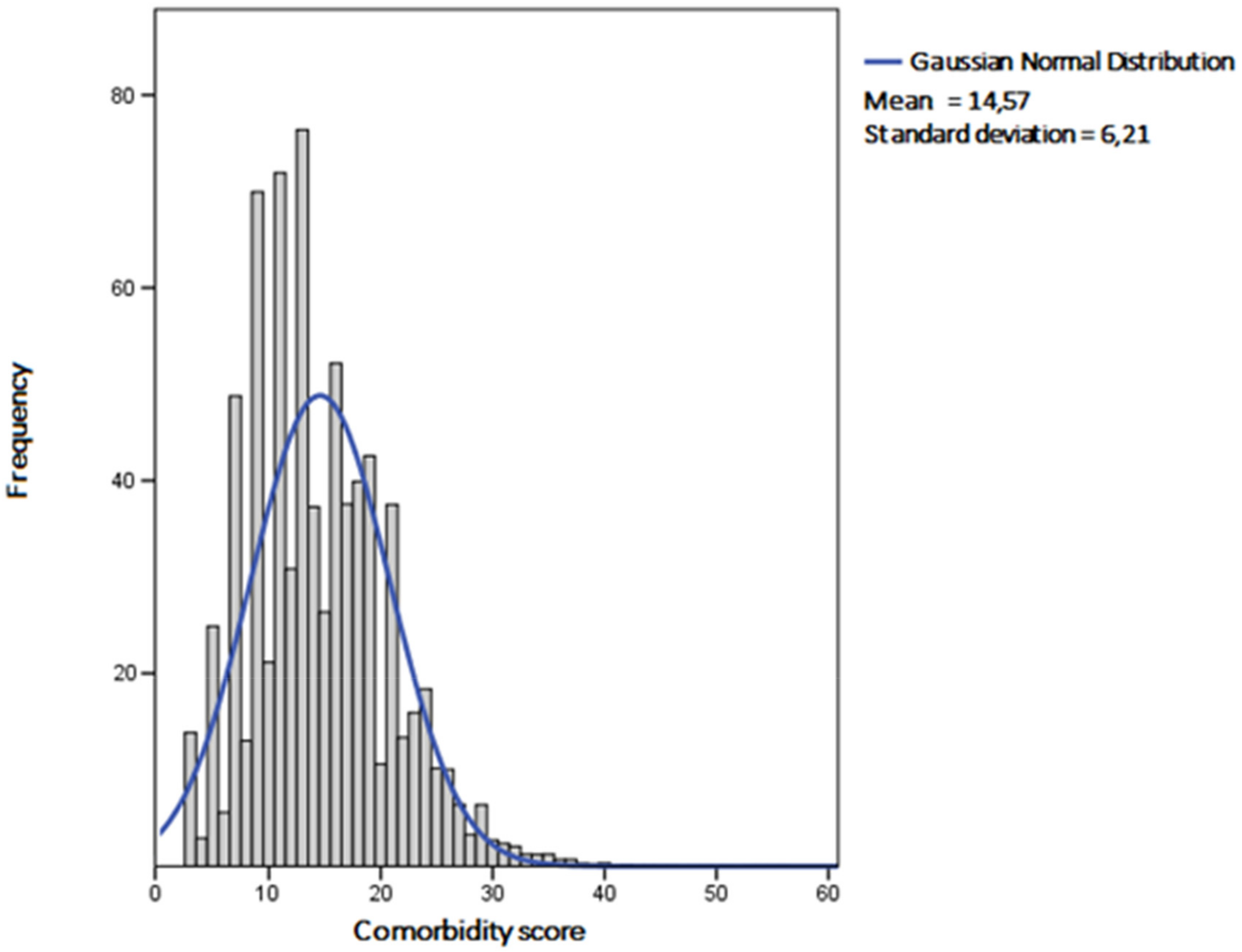
| Age (years) | 80.5 ± 7.8 |
| Comorbidity score | 14.57 ± 6.21 |
| Dialysis-dependent acute kidney injury (AKI), (n (%)) | 68,653 (9) |
| Diabetes, (n (%)) | 115,238 (15.6) |
| Sepsis, (n (%)) | 39,144 (5.1) |
| Length-of-stay (LOS) (days) | 13.72 ± 15.49 |
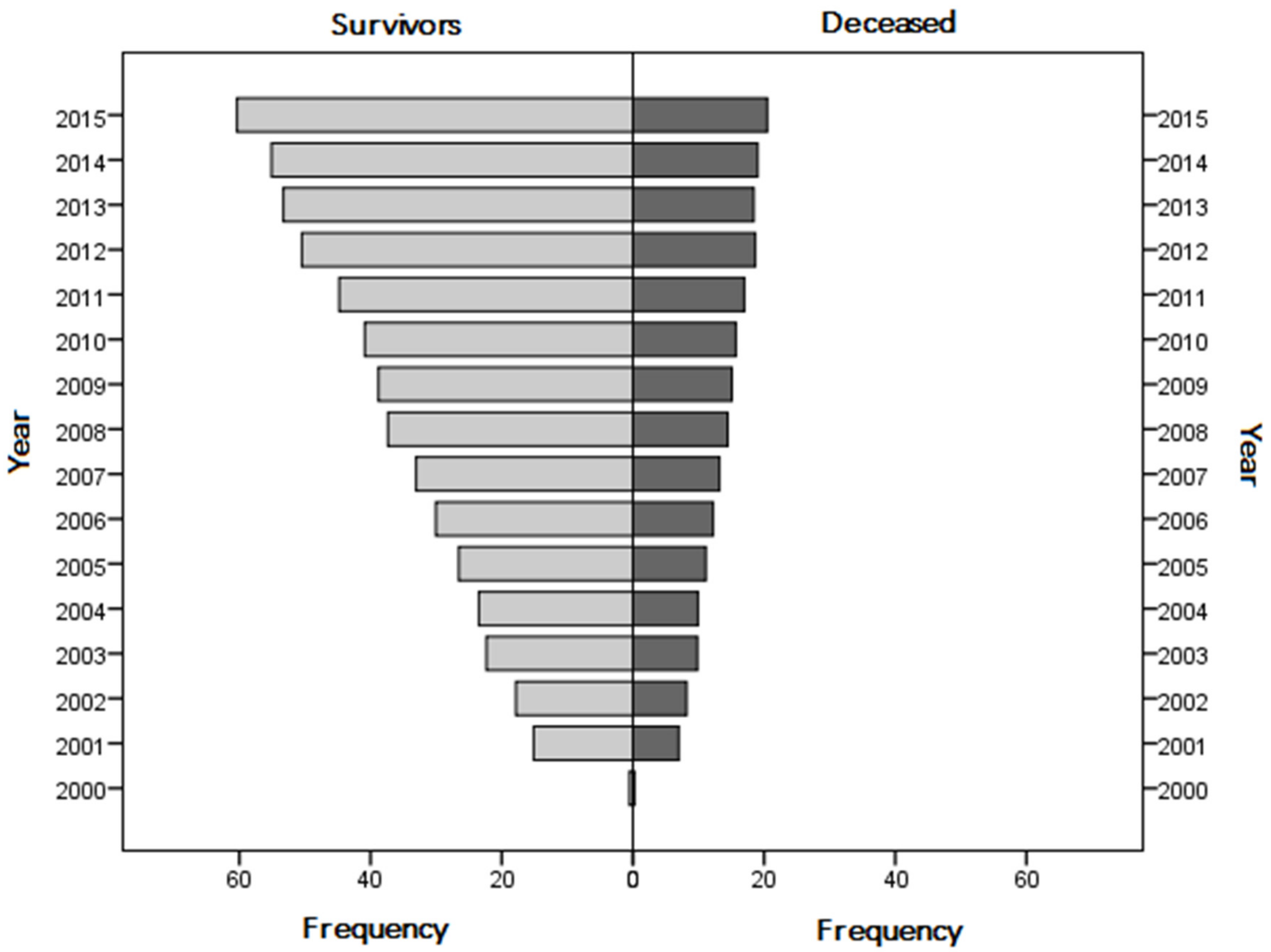
| Deceased subjects, (n (%)) | 210,661 (27.7) |
| Parameters | Survivors | Deceased | p |
|---|---|---|---|
| n = 550,003 | n = 210,661 | ||
| Men, (n (%)) | 288,120 (52.4) | 109,054 (51.8) | <0.001 |
| Women, (n (%)) | 261,883 (47.6) | 101,607 (48.2) | |
| Age (years) | 80 ± 7.72 | 81.9 ± 7.9 | <0.001 |
| Comorbidity score | 14.04 ± 6.02 | 15.96 ± 6.48 | <0.001 |
| Dialysis-dependent AKI, (n (%)) | 37,598 (6.8) | 31,055 (14.7) | <0.001 |
| Diabetes, (n (%)) | 95,433 (17.4) | 22,866 (10.9) | <0.001 |
| Sepsis, (n (%)) | 23,230 (4.2) | 15,914 (7.6) | <0.001 |
| Parameters | First Tertile (Score < 11) | Second Tertile (11 ≤ Score ≤ 17) | Third Tertile (Score > 17) | p |
|---|---|---|---|---|
| Number of subjects | 200,131 (26.3%) | 332,533 (43.7%) | 228,000 (30%) | |
| Length-of-stay (days) | 15.6 ± 19 | 13.59 ± 14.5 | 12.28 ± 13.1 | <0.001 |
| Comorbidity score | 7.48 ± 1.99 | 13.67 ± 2,04 | 22.12 ± 4.13 | <0.001 |
| Males, (n (%)) | 119,798 (59.9%) | 144,464 (43.4%) | 132,912 (58.3%) | <0.001 |
| Females, (n (%)) | 80,333 (40.1%) | 188,069 (56.6%) | 95,088 (41.7%) | |
| Deceased, (n (%)) | 38,740 (19.4%) | 92,987 (28%) | 78,934 (34.6%) | <0.001 |
| Dialysis-dependent AKI, (n (%)) | 26,901 (13.4%) | 29,054 (8.7%) | 12,698 (5.6%) | <0.001 |
| Sepsis, (n (%)) | 12,652 (6.3%) | 17,944 (5.4%) | 8,548 (3.7%) | <0.001 |
| Chronic kidney disease (n (%)) | 32,217 (16.1%) | 49,308 (14.8%) | 33,713 (14.8%) | <0.001 |
| Neurological disorders (n (%)) | 2609 (1.3%) | 8661 (2.6%) | 6642 (2.9%) | <0.001 |
| Lymphoma (n (%)) | 2856 (1.4%) | 9145 (2.8%) | 4442 (1.9%) | <0.001 |
| Solid tumor without metastasis (n (%)) | 5888 (2.9%) | 29,907 (9%) | 35,829 (15.7%) | <0.001 |
| Ischemic heart disease (n (%)) | 2042 (1%) | 14,001 (4.2%) | 18,900 (8.3%) | <0.001 |
| Congestive heart failure (n (%)) | 7109 (3.6%) | 67,211 (20.2%) | 72,039 (31.6%) | <0.001 |
| Coagulopathy (n (%)) | 0 | 2780 (0.8%) | 5486 (2.4%) | <0.001 |
| Fluid and electrolyte disorders (n (%)) | 0 | 33,322 (10%) | 93,380 (41%) | <0.001 |
| Liver disease (n (%)) | 0 | 8578 (2.6%) | 25,437 (11.2%) | <0.001 |
| Cachexia (n (%)) | 0 | 441 (0.1%) | 14,922 (6.5%) | <0.001 |
| Metastatic cancer (n (%)) | 0 | 2009 (0.6%) | 28,416 (12.5%) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fabbian, F.; Savriè, C.; De Giorgi, A.; Cappadona, R.; Di Simone, E.; Boari, B.; Storari, A.; Gallerani, M.; Manfredini, R. Acute Kidney Injury and In-Hospital Mortality: A Retrospective Analysis of a Nationwide Administrative Database of Elderly Subjects in Italy. J. Clin. Med. 2019, 8, 1371. https://doi.org/10.3390/jcm8091371
Fabbian F, Savriè C, De Giorgi A, Cappadona R, Di Simone E, Boari B, Storari A, Gallerani M, Manfredini R. Acute Kidney Injury and In-Hospital Mortality: A Retrospective Analysis of a Nationwide Administrative Database of Elderly Subjects in Italy. Journal of Clinical Medicine. 2019; 8(9):1371. https://doi.org/10.3390/jcm8091371
Chicago/Turabian StyleFabbian, Fabio, Caterina Savriè, Alfredo De Giorgi, Rosaria Cappadona, Emanuele Di Simone, Benedetta Boari, Alda Storari, Massimo Gallerani, and Roberto Manfredini. 2019. "Acute Kidney Injury and In-Hospital Mortality: A Retrospective Analysis of a Nationwide Administrative Database of Elderly Subjects in Italy" Journal of Clinical Medicine 8, no. 9: 1371. https://doi.org/10.3390/jcm8091371
APA StyleFabbian, F., Savriè, C., De Giorgi, A., Cappadona, R., Di Simone, E., Boari, B., Storari, A., Gallerani, M., & Manfredini, R. (2019). Acute Kidney Injury and In-Hospital Mortality: A Retrospective Analysis of a Nationwide Administrative Database of Elderly Subjects in Italy. Journal of Clinical Medicine, 8(9), 1371. https://doi.org/10.3390/jcm8091371