A Prognostic Model for the Outcome of Nobel Biocare Dental Implants with Peri-Implant Disease after One Year

 ,
,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Follow-Up and Interventions
2.2. Predictors and Model Development
2.3. Bias
2.4. Study Size
2.5. Statistical Methods
2.6. Internal and External Validation
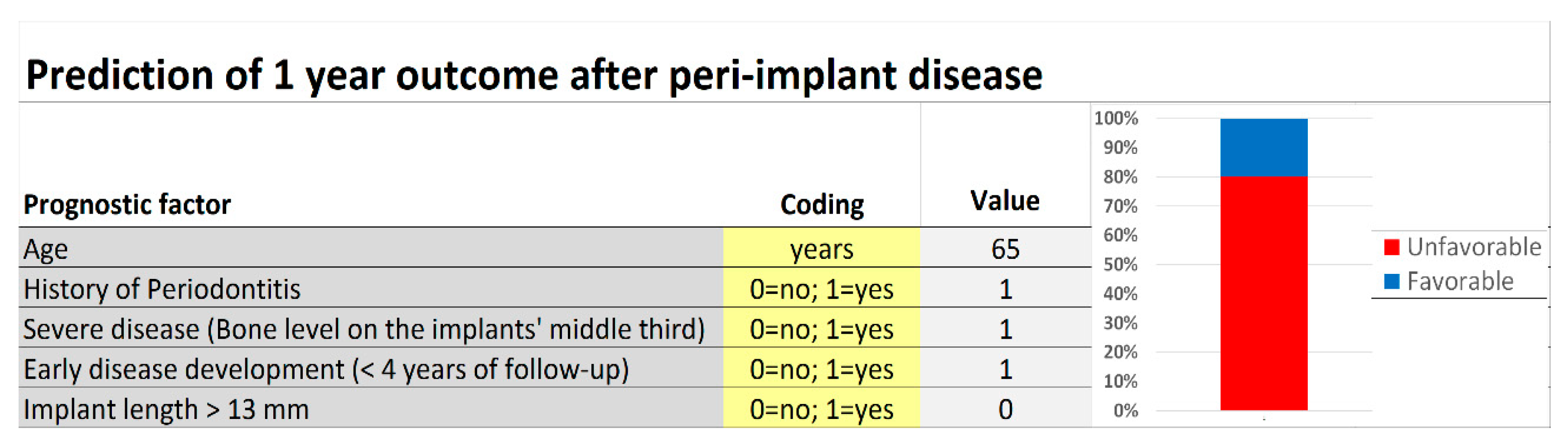
2.7. Model Presentation
3. Results
3.1. Participants
3.2. Results Reported According to Disease Severity
3.3. Treatment Protocols
3.4. Prognostic Factors
3.5. Model Presentation
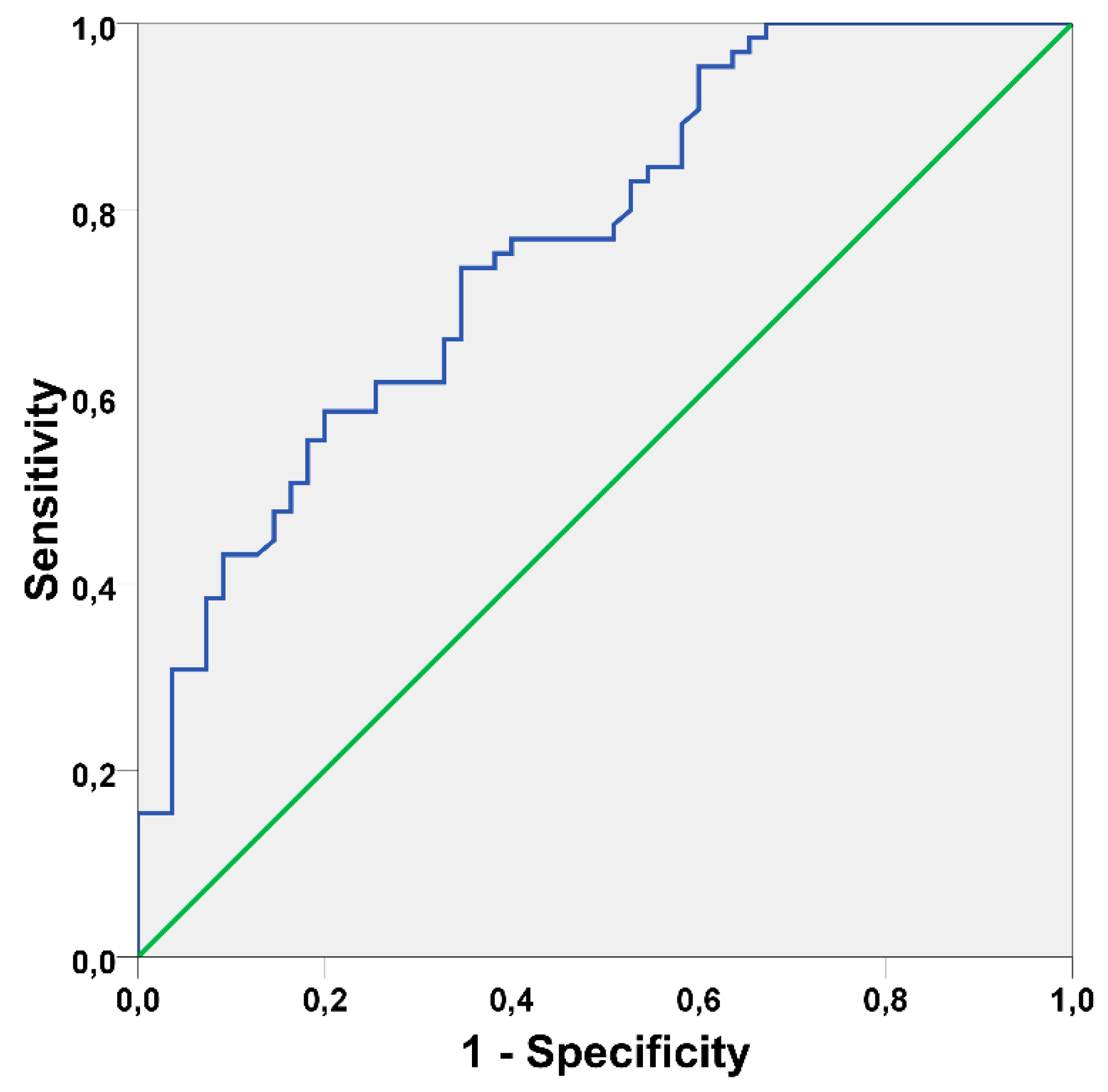
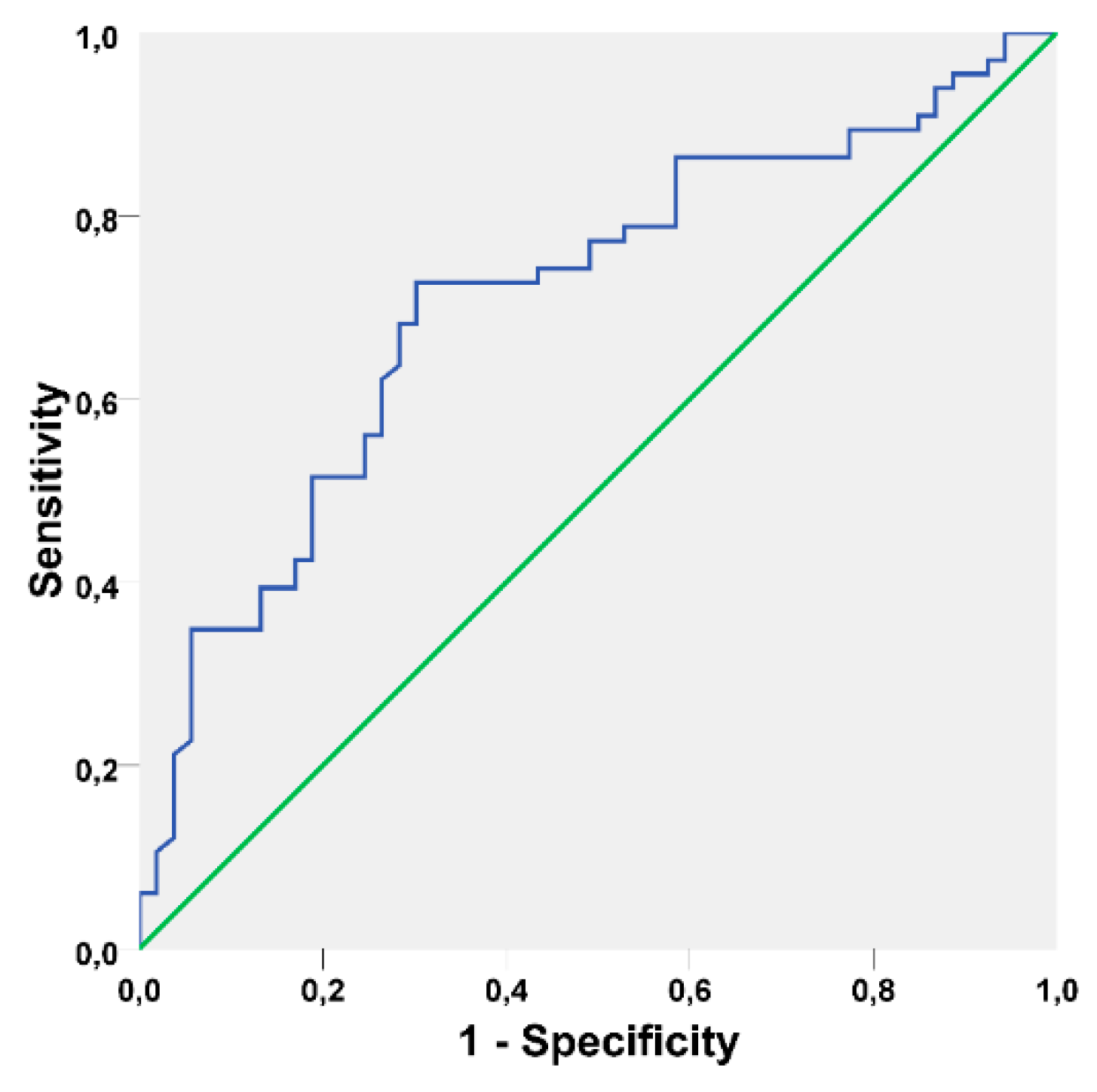
3.6. Prognostic Model Validation
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Pjetursson, B.E.; Tan, K.; Lang, N.P.; Brägger, U.; Egger, M.; Zwahlen, M. A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years. Clin. Oral Implant Res. 2004, 15, 625–642. [Google Scholar] [CrossRef]
- Kwon, T.; Bain, P.A.; Levin, L. Systematic review of short-(5–10 years) and long-term (10 years or more) survival and success of full-arch fixed dental hybrid prostheses and supporting implants. J. Dent. 2014, 42, 1228–1241. [Google Scholar] [CrossRef]
- Hjalmarsson, L.; Gheisarifar, M.; Jemt, T. A systematic review of survival of single implants as presented in longitudinal studies with a follow-up of at least 10 years. Eur. J. Oral Implantol. 2016, 9, S155–S162. [Google Scholar]
- Albrektsson, T. Consensus Report of Session IV. In Proceedings of the First European Workshop on Periodontology, 1st ed.; Lang, N.P., Ed.; Quintessence: London, UK, 1984; pp. 365–369. [Google Scholar]
- Esposito, M.; Grusovin, M.G.; Worthington, H.V. Interventions for replacing missing teeth: Treatment of peri-implantitis. Cochrane Database. Syst. Rev. 2012. [Google Scholar] [CrossRef]
- De Araújo Nobre, M.; Mano Azul, A.; Rocha, E.; Maló, P.; Salvado, F. Attributable fractions, modifiable risk factors and risk stratification using a risk score for peri-implant pathology. J. Prosthodont. Res. 2017, 61, 43–53. [Google Scholar] [CrossRef]
- Zitzmann, N.U.; Berglundh, T. Definition and prevalence of peri-implant diseases. J. Clin. Periodontol. 2008, 35, S286–S291. [Google Scholar] [CrossRef]
- Atieh, M.A.; Alsabeeha, N.H.; Faggion, C.M. Jr.; Duncan, W.J. The frequency of peri-implant diseases: A systematic review and meta-analysis. J. Periodontol. 2013, 84, 1586–1598. [Google Scholar] [CrossRef]
- Marcantonio, C.; Nicoli, L.G.; Marcantonio Junior, E.; Zandim-Barcelos, D.L. Prevalence and Possible Risk Factors of Peri-implantitis: A Concept Review. J. Contemp. Dent. Pract. 2015, 16, 750–757. [Google Scholar] [CrossRef]
- Derks, J.; Tomasi, C. Peri-implant health and disease. A systematic review of current epidemiology. J. Clin. Periodontol. 2015, 42, S158–S171. [Google Scholar] [CrossRef]
- De Araújo Nobre, M.; Maló, P. Prevalence of periodontitis, dental caries, and peri-implant pathology and their relation with systemic status and smoking habits: Results of an open-cohort study with 22009 patients in a private rehabilitation center. J. Dent. 2017, 67, 36–42. [Google Scholar] [CrossRef]
- Lee, C.T.; Huang, Y.W.; Zhu, L.; Weltman, R. Prevalences of peri-implantitis and peri-implant mucositis: Systematic review and meta-analysis. J. Dent. 2017, 62, 1–12. [Google Scholar] [CrossRef]
- Uribe, R.; Peñarrocha, M.; Sanchis, J.M.; Garcia, O. Marginal periimplantitis due to occlusal overload. A case report. Med. Oral 2004, 9, 159–162. [Google Scholar]
- Renvert, S.; Persson, G.R. Periodontitis as a potential risk factor for peri-implantitis. J. Clin. Periodontol. 2009, 36, S9–S14. [Google Scholar] [CrossRef]
- Qian, J.; Wennerberg, A.; Albrektsson, T. Reasons for marginal bone loss around oral implants. Clin. Implant Dent. Relat. Res. 2012, 14, 792–807. [Google Scholar] [CrossRef]
- Fu, J.H.; Hsu, Y.T.; Wang, H.L. Identifying occlusal overload and how to deal with it to avoid marginal bone loss around implants. Eur. J. Oral Implantol. 2012, 5, S91–S103. [Google Scholar]
- Monje, A.; Catena, A.; Borgnakke, W.S. Association between diabetes mellitus/hyperglycaemia and peri-implant diseases: Systematic review and meta-analysis. J. Clin. Periodontol. 2017, 44, 636–648. [Google Scholar] [CrossRef]
- De Araújo Nobre, M.; Maló, P.; Gonçalves, Y.; Sabas, A.; Salvado, F. Dental implants in diabetic patients: Retrospective cohort study reporting on implant survival and risk indicators for excessive marginal bone loss at 5 years. J. Oral Rehabil. 2016, 43, 863–870. [Google Scholar] [CrossRef]
- Jepsen, S.; Berglundh, T.; Genco, R.; Aass, A.M.; Demirel, K.; Derks, J.; Figuero, E.; Giovannoli, J.L.; Goldstein, M.; Lambert, F.; et al. Peri-implant disease in subjects with and without preventive maintenance: A 5-year follow-up. J. Clin. Periodontol. 2012, 39, 173–181. [Google Scholar]
- Esposito, M.; Grusovin, M.G.; De Angelis, N.; Camurati, A.; Campailla, M.; Felice, P. The adjunctive use of light-activated disinfection (LAD) with FotoSan is ineffective in the treatment of peri-implantitis: 1-year results from a multicentre pragmatic randomised controlled trial. Eur. J. Oral Implantol. 2013, 6, 109–119. [Google Scholar]
- Magliocchetti, N.; Torchio, P.; Corrao, G.; Aricò, S.; Favilli, S. Prognostic factors for long-term survival in cirrhotic patients after the first episode of liver decompensation. Ital. J. Gastroenterol. Hepatol. 1997, 29, 38–46. [Google Scholar]
- Kemeny, N.; Braun, D.W., Jr. Prognostic factors in advanced colorectal carcinoma. Importance of lactic dehydrogenase level, performance status, and white blood cell count. Am. J. Med. 1983, 74, 786–794. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Koka, S.; Zarb, G. On osseointegration: The healing adaptation principle in the context of osseosufficiency, osseoseparation, and dental implant failure. Int. J. Prosthodont. 2012, 25, 48–52. [Google Scholar]
- Sanz, M.; Chapple, I.L.; Working Group 4 of the VIII European Workshop on Periodontology. Clinical research on peri-implant diseases: Consensus report of Working Group 4. J. Clin. Periodontol. 2012, 39, S202–S206. [Google Scholar] [CrossRef]
- Charalampakis, G.; Rabe, P.; Leonhardt, A.; Dahlén, G. A follow-up study of peri-implantitis cases after treatment. J. Clin. Periodontol. 2011, 38, 864–871. [Google Scholar] [CrossRef]
- De Waal, Y.C.; Raghoebar, G.M.; Meijer, H.J.; Winkel, E.G.; van Winkelhoff, A.J. Prognostic indicators for surgical peri-implantitis treatment. Clin. Oral Implants Res. 2016, 27, 1485–1491. [Google Scholar] [CrossRef]
- Chuang, S.K.; Wei, L.J.; Douglass, C.W.; Dodson, T.B. Risk factors for dental implant failure: A strategy for the analysis of clustered failure-time observations. J. Dent. Res. 2002, 81, 572–577. [Google Scholar] [CrossRef]
- Moy, P.K.; Medina, D.; Shetty, V.; Aghaloo, T.L. Dental implant failure rates and associated risk factors. Int. J. Oral Maxillofac. Implant 2005, 20, 569–577. [Google Scholar]
- Ramanauskaite, A.; Baseviciene, N.; Wang, H.L.; Tözüm, T.F. Effect of History of Periodontitis on Implant Success: Meta-Analysis and Systematic Review. Implant Dent. 2014, 23, 687–696. [Google Scholar] [CrossRef]
- De Araújo Nobre, M.A.; Maló, P.; Oliveira, S.H. The influence of implant location and position characteristics on periimplant pathology. Eur. J. Prosthodont. Restor. Dent. 2014, 3, 125–129. [Google Scholar]
- De Araújo Nobre, M.A.; Maló, P. The influence of rehabilitation characteristics in the incidence of peri-implant pathology: A case-control study. J. Prosthodont. 2014, 23, 21–30. [Google Scholar] [CrossRef]
- De Araújo Nobre, M.A.; Maló, P.S.; Oliveira, S.H. Associations of clinical characteristics and interval between maintenance visits with peri-implant pathology. J. Oral Sci. 2014, 56, 143–150. [Google Scholar] [CrossRef][Green Version]
- Fedak, K.M.; Bernal, A.; Capshaw, Z.A.; Gross, S. Applying the Bradford Hill criteria in the 21st century: How data integration has changed causal inference in molecular epidemiology. Emerg. Themes Epidemiol. 2015, 12, 14. [Google Scholar] [CrossRef]
- Mombelli, A.; van Oosten, M.A.; Schurch, E. Jr.; Land, N.P. The microbiota associated with successful or failing osseointegrated titanium implants. Oral Microbiol. Immunol. 1987, 2, 145–151. [Google Scholar] [CrossRef]
- Dupont, W.D.; Plummer, W.D. Power and Sample Size Calculations for Studies Involving Linear Regression. Controll. Clin. Trials 1998, 19, 589–601. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Zarb, G.; Koka, S.; Albrektsson, T. Hyperbole, clinical dissonance, and scratching the surface: Complication or disease? Int. J. Prosthodont. 2013, 26, 311. [Google Scholar]
- Becker, S.T.; Beck-Broichsitter, B.E.; Graetz, C.; Dörfer, C.E.; Wiltfang, J.; Häsler, R. Peri-implantitis versus periodontitis: Functional differences indicated by transcriptome profiling. Clin. Implant Dent. Relat. Res. 2014, 16, 401–411. [Google Scholar] [CrossRef]
- Carcuac, O.; Berglundh, T. Composition of human peri-implantitis and periodontal lesions. J. Dent. Res. 2014, 93, 1083–1088. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J. Peri-implant diseases: Diagnosis and risk indicators. J. Clin. Periodontol. 2008, 35, S292–S304. [Google Scholar] [CrossRef]
- Albrektsson, T.; Buser, D.; Chen, S.T.; Cochran, D.; DeBruyn, H.; Jemt, T.; Koka, S.; Nevins, M.; Sennerby, L.; Simion, M. Statements from the Estepona Consensus Meeting on Peri-implantitis, February 2–4, 2012. Clin. Implant Dent. Relat. Res. 2012, 14, 781–782. [Google Scholar] [CrossRef]
- De Araújo Nobre, M.; Mano Azul, A.; Rocha, E.; Maló, P. Risk factors of peri-implant pathology. Eur. J. Oral Sci. 2015, 123, 131–139. [Google Scholar] [CrossRef]
- Konstantinidis, I.K.; Kotsakis, G.A.; Gerdes, S.; Walter, M.H. Cross-sectional study on the prevalence and risk indicators of peri-implant diseases. Eur. J. Oral Implantol. 2018, 8, 75–88. [Google Scholar]
- Karlsson, K.; Derks, J.; Håkansson, J.; Wennström, J.L.; Petzold, M.; Berglundh, T. Interventions for peri-implantitis and their effects on further bone loss. A retrospective analysis of a registry-based cohort. J. Clin. Periodontol. 2019. [Google Scholar] [CrossRef]
- Riley, R.D.; Hayden, J.A.; Steyerberg, E.W.; Moons, K.G.; Abrams, K.; Kyzas, P.A.; Malats, N.; Briggs, A.; Schroter, S.; Altman, D.G.; et al. Prognosis Research Strategy (PROGRESS) 2: Prognostic factor research. PLoS Med. 2013, 10, e1001380. [Google Scholar] [CrossRef]
- Moons, K.G.; Royston, P.; Vergouwe, Y.; Grobbee, D.E.; Altman, D.G. Prognosis and prognostic research: What, why, and how? BMJ 2009, 338, b375. [Google Scholar] [CrossRef]
- Hansebout, R.R.; Cornacchi, S.D.; Haines, T.; Goldsmith, C.H. How to use an article about prognosis. Can. J. Surg. 2009, 52, 328–336. [Google Scholar]
- Webster, J.D.; Dennis, M.M.; Dervisis, N.; Heller, J.; Bacon, N.J.; Bergman, P.J.; Bienzle, D.; Cassali, G.; Castagnaro, M.; Cullen, J.; et al. American College of Veterinary Pathologists Oncology Committee. Recommended guidelines for the conduct and evaluation of prognostic studies in veterinary oncology. Vet. Pathol. 2011, 48, 7–18. [Google Scholar] [CrossRef]
- Lagervall, M.; Jansson, L.E. Treatment outcome in patients with peri-implantitis in a periodontal clinic: A retrospective study. J. Periodontol. 2013, 84, 1365–1373. [Google Scholar] [CrossRef]
- Hultin, M.; Gustafsson, A.; Hallstrom, H.; Johansson, L.A.; Ekfeldt, A.; Klinge, B. Microbiological findings and host response in patients with periimplantitis. Clin. Oral Implants Res. 2002, 13, 349–358. [Google Scholar] [CrossRef]
- Casado, P.L.; Pereira, M.C.; Duarte, M.E.; Granjeiro, J.M. History of chronic periodontitis is a high risk indicator for peri-implant disease. Braz. Dent. J. 2013, 24, 136–141. [Google Scholar] [CrossRef]
- Marrone, A.; Lasserre, J.; Bercy, P.; Brecx, M.C. Prevalence and risk factors for peri-implant disease in Belgian adults. Clin. Oral Implants Res. 2013, 24, 934–940. [Google Scholar] [CrossRef]
- Poli, P.P.; Beretta, M.; Grossi, G.B.; Maiorana, C. Risk indicators related to peri-implant disease: An observational retrospective cohort study. J. Periodontal. Implant Sci. 2016, 46, 266–276. [Google Scholar] [CrossRef]
- Renvert, S.; Aghazadeh, A.; Hallström, H.; Persson, G.R. Factors related to peri-implantitis—A retrospective study. Clin. Oral Implants Res. 2014, 25, 522–529. [Google Scholar] [CrossRef]
- Cecchinato, D.; Parpaiola, A.; Lindhe, J. Mucosal inflammation and incidence of crestal bone loss among implant patients: A 10-year study. Clin. Oral Implants Res. 2014, 25, 791–796. [Google Scholar] [CrossRef]
- Fransson, C.; Wennstrom, J.; Berglundh, T. Clinical characteristics at implants with a history of progressive bone loss. Clin. Oral Implants Res. 2008, 19, 142–147. [Google Scholar] [CrossRef]
- Cooney, M.T.; Dudina, A.L.; Graham, I.M. Value and limitations of existing scores for the assessment of cardiovascular risk: A review for clinicians. J. Am. Coll. Cardiol. 2009, 54, 1209–1227. [Google Scholar] [CrossRef]
- Selvarajah, S.; Kaur, G.; Haniff, J.; Cheong, K.C.; Hiong, T.G.; van der Graaf, Y.; Bots, M.L. Comparison of the Framingham Risk Score, SCORE and WHO/ISH cardiovascular risk prediction models in an Asian population. Int. J. Cardiol. 2014, 176, 211–218. [Google Scholar] [CrossRef]
- Ramírez-Prado, D.; Palazón-Bru, A.; Folgado-de la Rosa, D.M.; Carbonell-Torregrosa, M.A.; Martínez-Díaz, A.M.; Martínez-St John, D.R.; Gil-Guillén, V.F. A four-year cardiovascular risk score for type 2 diabetic inpatients. Peer J. 2015, 3, e984. [Google Scholar] [CrossRef][Green Version]
- Esposito, M.; Grusovin, M.G.; Worthington, H.V. Treatment of peri-implantitis: What interventions are effective? A Cochrane systematic review. Eur. J. Oral Implantol. 2012, 5, S21–S41. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Derivation Set (%) | Validation Set (%) | ||||
|---|---|---|---|---|---|---|
| Total Sample | Moderate Disease | Severe Disease | Total Sample | Moderate Disease | Severe Disease | |
| Demographics | ||||||
| Number of patients | 120 (100%) | 54 (45%) | 66 (55%) | 120 (100%) | 62 (51.7%) | 58 (48.3%) |
| Average age (standard deviation) | 58.6 (10.5) | 56.7 (9.8) | 60 (10.9) | 58.6 (10.8) | 58.6 (11.5) | 58.6 (10.1) |
| Gender | ||||||
| Female | 73 (60.8%) | 31 (57.4%) | 42 (63.6%) | 69 (57.5%) | 28 (45.2%) | 41 (70.7%) |
| Male | 47 (39.2%) | 23 (42.6%) | 24 (36.4%) | 51 (42.5%) | 34 (54.8%) | 17 (29.3%) |
| Implant status | ||||||
| Survival | 55 (45.8%) | 31 (57.4%) | 24 (36.4%) | 53 (44.2%) | 31 (50.8% | 22 (37.9%) |
| Failure | 65 (54.2%) | 23 (42.6%) | 42 (63.6%) | 66 (55.0%) | 30 (49.2%) | 36 (62.1%) |
| History of Periodontitis | ||||||
| Absence | 29 (24.2%) | 14 (25.9%) | 15 (22.7%) | 30 (25.0%) | 16 (25.8%) | 14 (24.1%) |
| Presence | 91 (75.8%) | 40 (74.1%) | 51 (77.3%) | 90 (75.0%) | 46 (74.2%) | 44 (75.9%) |
| Systemic comorbidities | ||||||
| Absence | 79 (65.8%) | 35 (64.8%) | 44 (66.7%) | 80 (66.7%) | 41 (66.1%) | 39 (67.2%) |
| Presence | 41 (34.2%) | 19 (35.2%) | 22 (33.3%) | 40 (33.3%) | 21 (33.9%) | 19 (32.8%) |
| Smoking | ||||||
| Non-smoker | 77 (64.2%) | 37 (68.5%) | 40 (60.6%) | 81 (67.5%) | 42 (67.7%) | 39 (67.5%) |
| Smoker | 43 (35.8%) | 17 (31.5%) | 26 (39.4%) | 39 (32.5%) | 20 (32.3%) | 19 (32.8%) |
| Proximity of implants/teeth | ||||||
| Absence | 86 (71.7%) | 42 (77.8%) | 44 (66.7%) | 93 (77.5%) | 48 (77.4%) | 45 (77.6%) |
| Presence | 34 (28.3%) | 12 (22.2%) | 22 (33.3%) | 27 (22.5%) | 14 (22.6%) | 13 (22.4%) |
| Type of implant surface | ||||||
| Machined | 5 (4.2%) | 2 (3.7%) | 3 (4.5%) | 7 (5.8%) | 4 (6.5%) | 3 (5.2%) |
| Anodically oxidized | 115 (95.8%) | 52 (96.3%) | 63 (95.5%) | 113 (94.2%) | 58 (93.5%) | 55 (94.8%) |
| Implant position per arch | ||||||
| Maxilla | 66 (55%) | 29 (53.7%) | 37 (56.1%) | 65 (54.2%) | 21 (33.9%) | 34 (58.6%) |
| Mandible | 54 (45%) | 25 (46.3%) | 29 (43.9%) | 55 (45.8%) | 41 (66.1%) | 24 (41.4%) |
| Implant position in the arch | ||||||
| Anterior | 49 (40.8%) | 21 (38.9%) | 28 (42.4%) | 42 (35.0%) | 22 (35.5%) | 20 (34.5%) |
| Posterior | 71 (59.2%) | 33 (61.1%) | 38 (57.6%) | 78 (65.0%) | 40 (64.5%) | 38 (65.5%) |
| Time of follow-up at diagnosis * | ||||||
| ≥4 years | 69 (57.5%) | 28 (51.9%) | 41 (62.1%) | 65 (54.2%) | 37 (59.7%) | 28 (48.3%) |
| <4 years | 51 (42.5%) | 26 (48.1%) | 25 (37.9%) | 55 (45.8%) | 25 (40.3%) | 30 (51.7%) |
| Implant length | ||||||
| ≤13 mm | 62 (51.7%) | 27 (50%) | 35 (53%) | 58 (48.3%) | 28 (45.2%) | 30 (51.7%) |
| >13 mm | 58 (48.3%) | 27 (50%) | 31 (47%) | 62 (51.7%) | 34 (54.8%) | 28 (48.3%) |
| Abutment height | ||||||
| No abutment | 11 (9.2%) | 8 (14.8%) | 3 (4.5%) | 7 (5.8%) | 2 (3.2%) | 5 (8.6%) |
| 1 mm | 27 (22.5%) | 13 (24.1%) | 14 (21.2%) | 26 (21.7%) | 12 (19.4%) | 14 (24.1%) |
| 2 mm | 36 (30.0%) | 13 (24.1%) | 23 (34.8%) | 36 (30.0%) | 22 (35.5%) | 14 (24.1%) |
| 3 mm | 27 (22.5%) | 10 (18.5%) | 17 (25.8%) | 23 (19.2%) | 7 (11.3%) | 16 (27.6%) |
| 4 mm | 15 (12.5%) | 6 (11.1%) | 9 (13.6%) | 24 (20.0%) | 17 (27.4%) | 7 (12.1%) |
| 5 mm | 3 (2.5%) | 3 (5.6%) | 0 (0%) | 4 (3.3%) | 2 (3.2%) | 2 (3.4%) |
| 6 mm | 1 (0.8%) | 1 (1.9%) | 0 (0%) | 0 (0.0%) | 0 (0%) | 0 (0%) |
| Type of rehabilitation | ||||||
| Single tooth | 35 (29.2%) | 18 (33.3%) | 17 (25.8%) | 37 (30.8%) | 16 (25.8%) | 21 (36.2%) |
| Partial | 15 (12.5%) | 7 (13%) | 8 (12.1%) | 10 (8.3%) | 6 (9.7%) | 4 (6.9%) |
| Full-arch | 70 (58.3%) | 29 (53.7%) | 41 (62.1%) | 73 (60.8%) | 40 (64.5%) | 33 (56.9%) |
| Type of material used in the restoration | ||||||
| Full-ceramic | 12 (10.0%) | 9 (16.7%) | 3 (4.5%) | 8 (6.7%) | 6 (9.7%) | 2 (3.4%) |
| Metal-ceramic | 52 (43.3%) | 19 (35.2%) | 33 (50.0%) | 48 (40.0%) | 25 (40.3%) | 23 (39.7%) |
| Metal-acrylic resin | 44 (36.7%) | 17 (31.5%) | 27 (40.9%) | 44 (36.7%) | 22 (35.5%) | 22 (37.9%) |
| Full-acrylic resin | 12 (10.0%) | 9 (16.7%) | 3 (4.5%) | 20 (16.7%) | 9 (14.5%) | 11 (19.0%) |
| Type of opposing dentition | ||||||
| Removable prosthesis | 1 (0.8%) | 0 (0%) | 1 (1.5%) | 2 (1.7%) | 2 (3.2%) | 0 (0%) |
| Natural teeth | 57 (47.5%) | 29 (53.7%) | 28 (42.4%) | 61 (50.8%) | 34 (54.8%) | 27 (46.6%) |
| Fixed prosthesis over natural teeth | 1 (0.8%) | 0 (0%) | 1 (1.5%) | 3 (2.5%) | 2 (3.2%) | 1 (1.7%) |
| Implant supported fixed prosthesis | 61 (50.8%) | 25 (46.3%) | 36 (54.5%) | 54 (45.0%) | 24 (38.7%) | 30 (51.7%) |
| Biofilm | ||||||
| Absence | 24 (20%) | 16 (29.6%) | 8 (12.1%) | 24 (20%) | 9 (14.5%) | 15 (25.9%) |
| Presence | 96 (80%) | 38 (70.4%) | 58 (87.9%) | 96 (80%) | 53 (85.5%) | 43 (74.1%) |
| Bleeding | ||||||
| Absence | 17 (14.2%) | 8 (14.8%) | 9 (13.6%) | 20 (16.7%) | 8 (12.9%) | 12 (20.7%) |
| Presence | 103 (85.8%) | 46 (85.2%) | 57 (86.4%) | 100 (83.3%) | 54 (87.1%) | 46 (79.3%) |
| Probing pocket depth in millimeters | ||||||
| ≤6 mm | 108 (90%) | 51 (94.4%) | 57 (86.4%) | 107 (89.2%) | 53 (85.5%) | 54 (93.1%) |
| >6 mm | 12 (10%) | 3 (5.6%) | 9 (13.6%) | 13 (10.8%) | 9 (14.5%) | 4 (6.9%) |
| Bone level at diagnosis | ||||||
| Implants’ coronal third | 54 (45%) | 54 (100%) | 0 (0%) | 62 (51.7%) | 62 (100%) | 0 (0%) |
| Implants’ middle third | 66 (55%) | 0 (0%) | 66 (100%) | 58 (48.3%) | 0 (0%) | 58 (100%) |
| Mechanical complications | ||||||
| Absence | 115 (95.8%) | 52 (96.3%) | 63 (95.5%) | 115 (95.8%) | 59 (95.2%) | 56 (96.6%) |
| Presence | 5 (4.2%) | 2 (3.7%) | 3 (4.5%) | 5 (4.2%) | 3 (4.8%) | 2 (3.4%) |
| Therapeutic approach | ||||||
| Non-surgical | 100 (83.3%) | 48 (88.9%) | 52 (78.8%) | 97 (80.8%) | 55 (88.7%) | 42 (72.4%) |
| Surgical | 20 (16.7%) | 6 (11.1%) | 14 (21.2%) | 23 (19.2%) | 7 (11.3%) | 16 (27.6%) |
| Variables | Relative Risk (RR) Crude Values (95% CI) | p-Value | Relative Risk (RR) Adjusted Values (95% CI) a | p-Value | Beta Value |
|---|---|---|---|---|---|
| Age | 1.04 (1.01; 1.08) | p = 0.030 | 1.04 (0.99; 1.08) | p = 0.105 | 0.035 |
| Gender (male) | 0.71 (0.34; 1.48) | p = 0.357 | |||
| History of Periodontitis | 3.56 (1.46; 8.68) | p = 0.005 | 3.13 (1.15; 8.55) | p = 0.026 | 1.142 |
| Systemic complications | 1.13 (0.53; 2.40) | p = 0.760 | |||
| Smoking | 1.49 (0.70; 3.18) | p = 0.302 | |||
| Proximity of implants/teeth | 0.67 (0.30; 1.49) | p = 0.327 | |||
| Implant surface (machined) | 5.02 (0.54; 46.31) | p = 0.155 | |||
| Implant position (maxilla) | 1.36 (0.66; 2.80) | p = 0.408 | |||
| Implant position (posterior) | 1.08 (0.52; 2.24) | p = 0.840 | |||
| Early disease development (<4 years) | 2.45 (1.16; 5.20) | p = 0.019 | 3.99 (1.62; 9.82) | p = 0.003 | 1.383 |
| Implant length (>13 mm) | 2.84 (1.35; 5.99) | p = 0.006 | 3.52 (1.48; 8.37) | p = 0.004 | 1.258 |
| Abutment height | p = 0.539 | ||||
| No abutment | 1.0 (reference) | ||||
| 1 mm | 2.48 (0.54; 11.40) | ||||
| 2 mm | 2.98 (0.68; 13.09) | ||||
| 3 mm | 4.53 (0.97; 21.14) | ||||
| 4 mm | 5.33 (0.97; 29.39) | ||||
| 5 mm | - | ||||
| 6 mm | - | ||||
| Type of rehabilitation | p = 0.112 | ||||
| Full-arch | 1.0 (reference) | ||||
| Single tooth | 0.59 (0.26; 1.35) | ||||
| Partial | 0.31 (0.10; 1.02) | ||||
| Type of material used in restoration | p = 0.287 | ||||
| Full-ceramic | 1.0 (reference) | ||||
| Metal-ceramic | 0.57 (0.16; 2.02) | ||||
| Metal-acrylic resin | 1.25 (0.34; 4.59) | ||||
| Acrylic resin | 1.0 (0.20; 5.07) | ||||
| Type of opposing dentition | p = 0.660 | ||||
| Implant-supported prosthesis | 1.0 (reference) | ||||
| Removable prosthesis | - | ||||
| Natural teeth | 0.63 (0.30; 1.30) | ||||
| Fixed prosthesis natural teeth | - | ||||
| Biofilm | 2.33 (0.92; 5.86) | p = 0.071 | |||
| Bleeding | 2.46 (0.84; 7.16) | p = 0.099 | |||
| Probing pocket depth (>6 mm) | 2.79 (0.72; 10.85) | p = 0.140 | |||
| Disease severity (severe disease-bone level implants’ middle 1/3) | 2.36 (1.13; 4.93) | p = 0.022 | 3.26 (1.37; 7.81) | p = 0.008 | 1.183 |
| Mechanical complications | 1.28 (0.21; 7.97) | p = 0.790 | |||
| Therapeutic approach (surgical) | 1.71 (0.63; 4.66) | p = 0.290 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Araújo Nobre, M.; Salvado, F.; Nogueira, P.; Rocha, E.; Ilg, P.; Maló, P. A Prognostic Model for the Outcome of Nobel Biocare Dental Implants with Peri-Implant Disease after One Year. J. Clin. Med. 2019, 8, 1352. https://doi.org/10.3390/jcm8091352
de Araújo Nobre M, Salvado F, Nogueira P, Rocha E, Ilg P, Maló P. A Prognostic Model for the Outcome of Nobel Biocare Dental Implants with Peri-Implant Disease after One Year. Journal of Clinical Medicine. 2019; 8(9):1352. https://doi.org/10.3390/jcm8091352
Chicago/Turabian Stylede Araújo Nobre, Miguel, Francisco Salvado, Paulo Nogueira, Evangelista Rocha, Peter Ilg, and Paulo Maló. 2019. "A Prognostic Model for the Outcome of Nobel Biocare Dental Implants with Peri-Implant Disease after One Year" Journal of Clinical Medicine 8, no. 9: 1352. https://doi.org/10.3390/jcm8091352
APA Stylede Araújo Nobre, M., Salvado, F., Nogueira, P., Rocha, E., Ilg, P., & Maló, P. (2019). A Prognostic Model for the Outcome of Nobel Biocare Dental Implants with Peri-Implant Disease after One Year. Journal of Clinical Medicine, 8(9), 1352. https://doi.org/10.3390/jcm8091352