Performance of 18F-FDG PET/CT in Selecting Thyroid Nodules with Indeterminate Fine-Needle Aspiration Cytology for Surgery. A Systematic Review and a Meta-Analysis

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Data Extraction
2.3. Quality Assessment
2.4. Data Analysis
3. Results
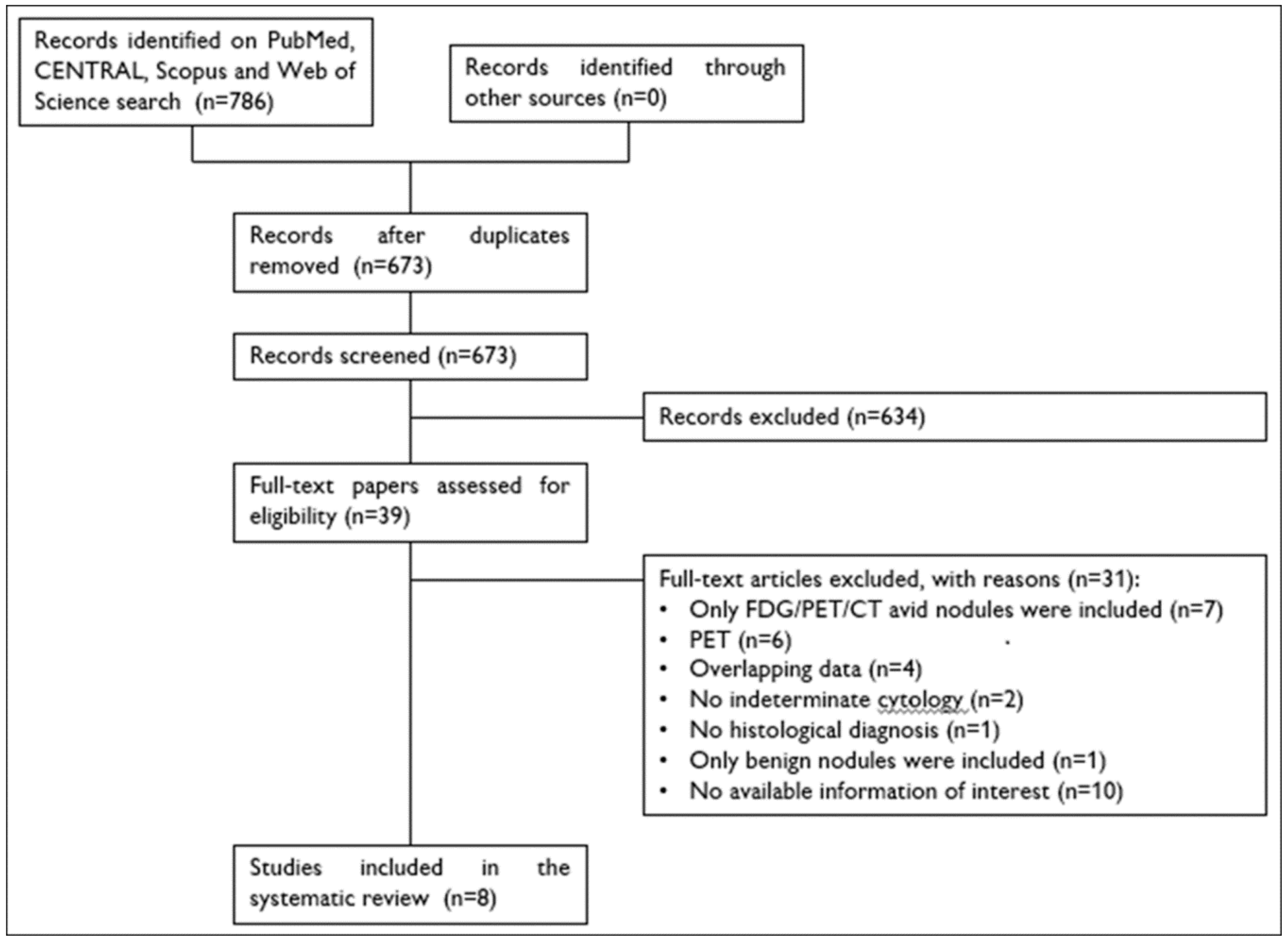
3.1. Literature Search
3.2. Qualitative Analysis (Systematic Review)
3.3. Quality Assessment
3.4. Quantitative Analysis (Meta-Analysis)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A
References
- Guth, S.; Theune, U.; Aberle, J.; Galach, A.; Bamberger, C.M. Very high prevalence of thyroid nodules detected by high frequency (13 MHz) ultrasound examination. Eur. J. Clin. Investig. 2009, 39, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Trimboli, P.; Treglia, G.; Guidobaldi, L.; Saggiorato, E.; Nigri, G.; Crescenzi, A.; Romanelli, F.; Orlandi, F.; Valabrega, S.; Sadeghi, R.; et al. Clinical characteristics as predictors of malignancy in patients with indeterminate thyroid cytology: A meta-analysis. Endocrine 2014, 46, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yassa, L.; Cibas, E.S.; Benson, C.B.; Frates, M.C.; Doubilet, P.M.; Gawande, A.A.; Moore, F.D., Jr.; Kim, B.W.; Nosé, V.; Marqusee, E.; et al. Long-term assessment of a multidisciplinary approach to thyroid nodule diagnostic evaluation. Cancer 2007, 111, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Cibas, E.S.; Ali, S.Z. The Bethesda System for Reporting Thyroid Cytopathology. Thyroid 2009, 19, 1159–1165. [Google Scholar] [CrossRef] [Green Version]
- Cibas, E.S.; Ali, S.Z. The 2017 Bethesda System for Reporting Thyroid Cytopathology. Thyroid 2017, 27, 1341–1346. [Google Scholar] [CrossRef] [PubMed]
- Fadda, G.; Basolo, F.; Bondi, A.; Bussolati, G.; Crescenzi, A.; Nappi, O.; Nardi, F.; Papotti, M.; Taddei, G.; Palombini, L.; et al. Cytological classification of thyroid nodules. Proposal of the SIAPEC-IAP Italian Consensus Working Group. Pathologica 2010, 102, 405–408. [Google Scholar]
- Nardi, F.; Basolo, F.; Crescenzi, A.; Fadda, G.; Frasoldati, A.; Orlandi, F.; Palombini, L.; Papini, E.; Zini, M.; Pontecorvi, A.; et al. Italian consensus for the classification and reporting of thyroid cytology. J. Endocrinol. Investig. 2014, 37, 593–599. [Google Scholar] [CrossRef]
- Perros, P.; Boelaert, K.; Colley, S.; Evans, C.; Evans, R.M.; Gerrard, B.G.; Gilbert, J.; Harrison, B.; Johnson, S.J.; Giles, T.E.; et al. Guidelines for the management of thyroid cancer. Clin. Endocrinol. 2014, 81 (Suppl. 1), 1–122. [Google Scholar] [CrossRef]
- Baloch, Z.W.; Fleisher, S.; LiVolsi, V.A.; Gupta, P.K. Diagnosis of “follicular neoplasm”: A gray zone in thyroid fine-needle aspiration cytology. Diagn. Cytopathol. 2002, 26, 41–44. [Google Scholar] [CrossRef]
- Straccia, P.; Rossi, E.D.; Bizzarro, T.; Brunelli, C.; Cianfrini, F.; Damiani, D.; Fadda, G. A meta-analytic review of the Bethesda System for Reporting Thyroid Cytopathology: Has the rate of malignancy in indeterminate lesions been underestimated? Cancer Cytopathol. 2015, 123, 713–722. [Google Scholar] [PubMed]
- Trimboli, P.; Crescenzi, A.; Castellana, M.; Giorgino, F.; Giovanella, L.; Bongiovanni, M. Italian consensus for the classification and reporting of thyroid cytology: the risk of malignancy between indeterminate lesions at low or high risk. A systematic review and meta-analysis. Endocrine 2019, 63, 430–438. [Google Scholar] [PubMed]
- Trimboli, P.; Condorelli, E.; Catania, A.; Sorrenti, S. Clinical and ultrasound parameters in the approach to thyroid nodules cytologically classified as indeterminate neoplasm. Diagn. Cytopathol. 2009, 37, 783–785. [Google Scholar] [CrossRef] [PubMed]
- Sciacchitano, S.; Lavra, L.; Ulivieri, A.; Magi, F.; De Francesco, G.P.; Bellotti, C.; Salehi, L.B.; Trovato, M.; Drago, C.; Bartolazzi, A. Comparative analysis of diagnostic performance, feasibility and cost of different test-methods for thyroid nodules with indeterminate cytology. Oncotarget 2017, 8, 49421–49442. [Google Scholar] [CrossRef] [PubMed]
- Bongiovanni, M.; Trimboli, P.; Rossi, E.D.; Fadda, G.; Nobile, A.; Giovanella, L. DIAGNOSIS OF ENDOCRINE DISEASE: High-yield thyroid fine-needle aspiration cytology: An update focused on ancillary techniques improving its accuracy. Eur. J. Endocrinol. 2016, 174, R53–R63. [Google Scholar] [CrossRef] [PubMed]
- Trimboli, P.; Treglia, G.; Condorelli, E.; Romanelli, F.; Crescenzi, A.; Bongiovanni, M.; Giovanella, L. BRAF-mutated carcinomas among thyroid nodules with prior indeterminate FNA report: A systematic review and meta-analysis. Clin. Endocrinol. 2016, 84, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Treglia, G.; Caldarella, C.; Saggiorato, E.; Ceriani, L.; Orlandi, F.; Salvatori, M.; Giovanella, L. Diagnostic performance of (99m)Tc-MIBI scan in predicting the malignancy of thyroid nodules: A meta-analysis. Endocrine 2013, 44, 70–78. [Google Scholar] [PubMed]
- Giovanella, L.; Campenni, A.; Treglia, G.; Verburg, F.A.; Trimboli, P.; Ceriani, L.; Bongiovanni, M. Molecular imaging with (99m)Tc-MIBI and molecular testing for mutations in differentiating benign from malignant follicular neoplasm: A prospective comparison. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1018–1026. [Google Scholar] [CrossRef]
- Rager, O.; Radojewski, P.; Dumont, R.A.; Treglia, G.; Giovanella, L.; Walter, M.A. Radioisotope imaging for discriminating benign from malignant cytologically indeterminate thyroid nodules. Gland Surg. 2019. [Google Scholar] [CrossRef]
- de Koster, E.J.; de Geus-Oei, L.F.; Dekkers, O.M.; van Engen-van Grunsven, I.; Hamming, J.; Corssmit, E.P.M.; Morreau, H.; Schepers, A.; Smit, J.; Oyen, W.J.G.; et al. Diagnostic Utility of Molecular and Imaging Biomarkers in Cytological Indeterminate Thyroid Nodules. Endocr. Rev. 2018, 39, 154–191. [Google Scholar]
- Piccardo, A.; Trimboli, P.; Foppiani, L.; Treglia, G.; Ferrarazzo, G.; Massollo, M.; Bottoni, G.; Giovanella, L. PET/CT in thyroid nodule and differentiated thyroid cancer patients. The evidence-based state of the art. Rev. Endocr. Metab. Disord. 2019, 20, 47–64. [Google Scholar]
- Treglia, G.; Kroiss, A.S.; Piccardo, A.; Lococo, F.; Santhanam, P.; Imperiale, A. Role of positron emission tomography in thyroid and neuroendocrine tumors. Minerva Endocrinol. 2018, 43, 341–355. [Google Scholar] [PubMed]
- Treglia, G.; Muoio, B.; Giovanella, L.; Salvatori, M. The role of positron emission tomography and positron emission tomography/computed tomography in thyroid tumours: An overview. Eur. Arch. Otorhinolaryngol. 2013, 270, 1783–1787. [Google Scholar] [CrossRef] [PubMed]
- Treglia, G.; Giovanella, L.; Rufini, V. PET and PET/CT imaging in thyroid and adrenal diseases: An update. Hormones 2013, 12, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Vriens, D.; de Wilt, J.H.; van der Wilt, G.J.; Netea-Maier, R.T.; Oyen, W.J.; de Geus-Oei, L.F. The role of [18F]-2-fluoro-2-deoxy-d-glucose-positron emission tomography in thyroid nodules with indeterminate fine-needle aspiration biopsy: Systematic review and meta-analysis of the literature. Cancer 2011, 117, 4582–4594. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Zhai, H.; Lu, Y. Is fluorine-18 fluorodeoxyglucose positron emission tomography useful for the thyroid nodules with indeterminate fine needle aspiration biopsy? A meta-analysis of the literature. J. Otolaryngol. Head. Neck. Surg. 2013, 42, 38. [Google Scholar] [CrossRef] [PubMed]
- Treglia, G.; Sadeghi, R. Meta-analyses and systematic reviews on PET and PET/CT in oncology: The state of the art. Clin. Transl. Imaging 2013, 1, 73–75. [Google Scholar] [CrossRef]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; The PRISMA-DTA Group. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Sadeghi, R.; Treglia, G. Systematic reviews and meta-analyses of diagnostic studies: A practical guideline. Clin. Transl. Imaging 2017, 5, 83–87. [Google Scholar] [CrossRef]
- Eusebi, P. Diagnostic accuracy measures. Cerebrovasc. Dis. 2013, 36, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Glas, A.S.; Lijmer, J.G.; Prins, M.H.; Bonsel, G.J.; Bossuyt, P.M. The diagnostic odds ratio: A single indicator of test performance. J. Clin. Epidemiol. 2003, 56, 1129–1135. [Google Scholar] [CrossRef]
- European Network for Health Technology Assessment. Meta-analysis of Diagnostic Test Accuracy Studies. Available online: https://www.eunethta.eu/methodological-guideline-on-meta-analysis-of-diagnostic-test-accuracy-studies/ (accessed on 1 July 2019).
- Mitchell, J.C.; Grant, F.; Evenson, A.R.; Parker, J.A.; Hasselgren, P.O.; Parangi, S. Preoperative evaluation of thyroid nodules with 18FDG-PET/CT. Surgery 2005, 138, 1166–1174. [Google Scholar] [CrossRef] [PubMed]
- Hales, N.W.; Krempl, G.A.; Medina, J.E. Is there a role for fluorodeoxyglucose positron emission tomography/computed tomography in cytologically indeterminate thyroid nodules? Am. J. Otolaryngol. 2008, 29, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Deandreis, D.; Al Ghuzlan, A.; Auperin, A.; Vielh, P.; Caillou, B.; Chami, L.; Lumbroso, J.; Travagli, J.P.; Hartl, D.; Baudin, E.; et al. Is (18)F-fluorodeoxyglucose-PET/CT useful for the presurgical characterization of thyroid nodules with indeterminate fine needle aspiration cytology? Thyroid 2012, 22, 165–172. [Google Scholar] [CrossRef]
- Muñoz Pérez, N.; Villar del Moral, J.M.; Muros Fuentes, M.A.; López de la Torre, M.; Arcelus Martínez, J.I.; Becerra Massare, P.; Esteva Martínez, D.; Cañadas Garre, M.; Coll Del Rey, E.; Bueno Laraño, P.; et al. Could 18F-FDG-PET/CT avoid unnecessary thyroidectomies in patients with cytological diagnosis of follicular neoplasm? Langenbecks. Arch. Surg. 2013, 398, 709–716. [Google Scholar] [CrossRef]
- Merten, M.M.; Castro, M.R.; Zhang, J.; Durski, J.; Ryder, M. Examining the Role of Preoperative Positron Emission Tomography/Computerized Tomography in Combination with Ultrasonography in Discriminating Benign from Malignant Cytologically Indeterminate Thyroid Nodules. Thyroid 2017, 27, 95–102. [Google Scholar] [CrossRef]
- Pathak, K.A.; Goertzen, A.L.; Nason, R.W.; Klonisch, T.; Leslie, W.D. A prospective cohort study to assess the role of FDG-PET in differentiating benign and malignant follicular neoplasms. Ann. Med. Surg. 2016, 12, 27–31. [Google Scholar] [CrossRef]
- Piccardo, A.; Puntoni, M.; Treglia, G.; Foppiani, L.; Bertagna, F.; Paparo, F.; Massollo, M.; Dib, B.; Paone, G.; Arlandini, A.; et al. Thyroid nodules with indeterminate cytology: prospective comparison between 18F-FDG-PET/CT, multiparametric neck ultrasonography, 99mTc-MIBI scintigraphy and histology. Eur. J. Endocrinol. 2016, 174, 693–703. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.T.; Lange, N.G.E.; Nielsen, A.L.; Thomassen, A.; Døssing, H.; Godballe, C.; Rohde, M. PET/CT and prediction of thyroid cancer in patients with follicular neoplasm or atypia. Eur. Arch. Otorhinolaryngol. 2018, 275, 2109–2117. [Google Scholar] [CrossRef]
- Gharib, H.; Papini, E.; Garber, J.R.; Duick, D.S.; Harrell, R.M.; Hegedüs, L.; Paschke, R.; Valcavi, R.; Vitti, P.; AACE/ACE/AME Task Force on Thyroid Nodules. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi Medical Guidelines for clinical practice for the diagnosis and management of thyroid nodules – 2016 update. Endocr. Pract. 2016, 22, 622–639. [Google Scholar] [PubMed]
- Bergenfelz, A.; Jansson, S.; Kristoffersson, A.; Mårtensson, H.; Reihnér, E.; Wallin, G.; Lausen, I. Complications to thyroid surgery: Results as reported in a database from a multicenter audit comprising 3,660 patients. Langenbecks. Arch. Surg. 2008, 393, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Vriens, D.; Adang, E.M.; Netea-Maier, R.T.; Smit, J.W.; de Wilt, J.H.; Oyen, W.J.; de Geus-Oei, L.F. Cost-effectiveness of FDG-PET/CT for cytologically indeterminate thyroid nodules: A decision analytic approach. J. Clin. Endocrinol. Metab. 2014, 99, 3263–3274. [Google Scholar] [CrossRef] [PubMed]
- Hegedüs, L.; Bonnema, S.J.; Bennedbaek, F.N. Management of simple nodular goiter: Current status and future perspectives. Endocr. Rev. 2003, 24, 102–132. [Google Scholar] [PubMed]
- Moreno-Reyes, R.; Kyrilli, A.; Lytrivi, M.; Bourmorck, C.; Chami, R.; Corvilain, B. Is there still a role for thyroid scintigraphy in the workup of a thyroid nodule in the era of fine needle aspiration cytology and molecular testing? F1000Res 2016, 5, 763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treglia, G.; Trimboli, P.; Verburg, F.A.; Luster, M.; Giovanella, L. Prevalence of normal TSH value among patients with autonomously functioning thyroid nodule. Eur. J. Clin. Investig. 2015, 45, 739–744. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| First Author [ref] | Country | Study Design | Thyroid Nodules (n) | Selection Criteria |
|---|---|---|---|---|
| Mitchell [34] | USA | NR | 24 | Microfollicular pattern |
| Hales [35] | USA | PCS | 16 | Follicular or Hürthle cell lesion |
| Deandreis [36] | France | RCS | 56 | Indeterminate cytology or AUS/FLUS and FN/SFN, > 10 mm, TSH 0.5–4 mUI L−1 |
| Muñoz Pérez [37] | Spain | PCS | 46 | Follicular or Hürthle cell neoplasm, euthyroid. Exclusion criteria: autonomous nodules, contraindication for 18F-FDG PET/CT or FNA, and the history or presence of another extrathyroidal cancer |
| Merten [38] | USA | RCS | 51 | Suspicious for Hürthle cell neoplasm or follicular neoplasm |
| Pathak [39] | Canada | PCS | 50 | Follicular or Hürthle cell neoplasms, > 5 mm |
| Piccardo [40] | Italy, Switzerland | PCS | 87 | Indeterminate cytology, > 10 mm, TSH 1–4 mUI L−1, undetectable thyroperoxidase and thyroglobulin autoantibodies |
| Nguyen [41] | Denmark | PCS | 108 | AUS/FLUS or FN/SFN. Exclusion criteria: (a) B symptoms (e.g., weight, night sweats); (b) suspicious ultrasound examination (lymph node metastasis, suspicious thyroid tumor); (c) suspicious clinical examinations (e.g., recurrent laryngeal nerve palsy); (d) lymph node metastasis and/or distant metastasis on 18F-FDG PET/CT, histology other than of thyroid origin |
| First Author, [ref] | PET/CT Scanner | 18F-FDG Injected Activity (MBq) | Time between 18F-FDG Injection and Image Acquisitions (min) | SUVmax Cut-Off Value for Benign and Malignant Lesions |
|---|---|---|---|---|
| Mitchell [34] | Discovery LS (General Electric Healthcare, Chalfont St. Giles, UK) | 740 | 60 | 5 |
| Hales [35] | REVEAL XVI HiREZ (Cti Molecular Imaging, Knoxville, Tennessee, USA) | 444–518 | 60 | 2 |
| Deandreis [36] | Biograph (Siemens, Knoxville, Tennessee, USA) | 118–189 | 60 | NR |
| Muñoz Pérez [37] | Biograph 16 (Siemens, Knoxville, Tennessee, USA) | 210–370 | 45–60 | 4.2 |
| Merten [38] | Discovery (General Electric Healthcare, Chalfont St. Giles, UK) | 444–519 | 60–70 | 5 |
| Pathak [39] | Biograph-16 (Siemens, Malvern, Pennsylvania, USA) | 185 | NR | 3.25 |
| Piccardo [40] | Discovery LS (General Electric Medical Systems, Milwaukee, Wisconsin, USA) Biograph 16 (Siemens, Knoxville, Tennessee, USA) | 111 | 50 | NR |
| Nguyen [41] | Discovery 690 (General Electric Healthcare, Waukesha, Wisconsin, USA) Discovery VCT (General Electric Medical Systems, Milwaukee, Wisconsin, USA) Discovery RX (General Electric Medical Systems, Milwaukee, Wisconsin, USA) Discovery STE (General Electric Medical Systems, Milwaukee, Wisconsin, USA) | 200–400 | 60 | NR |
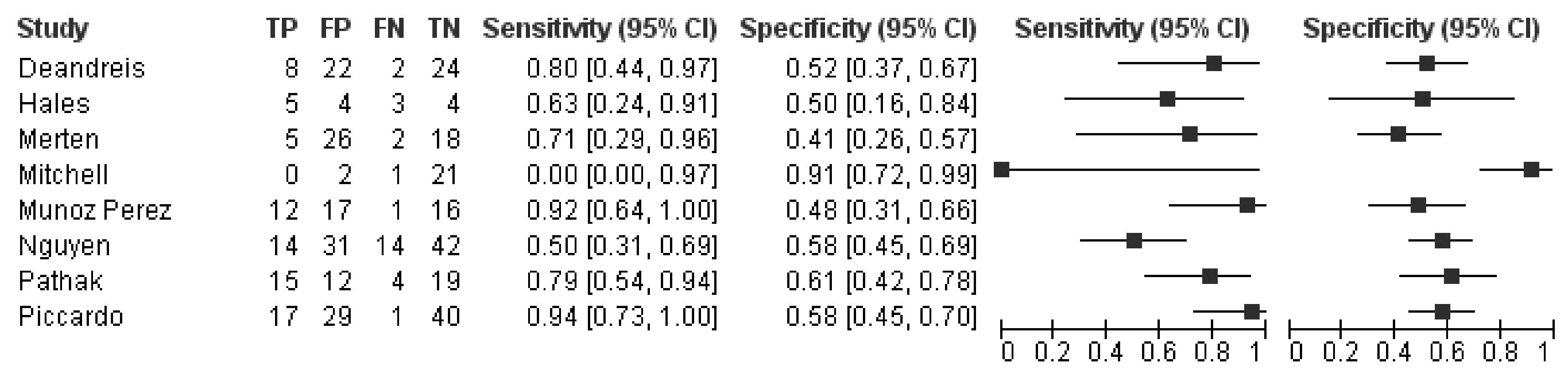
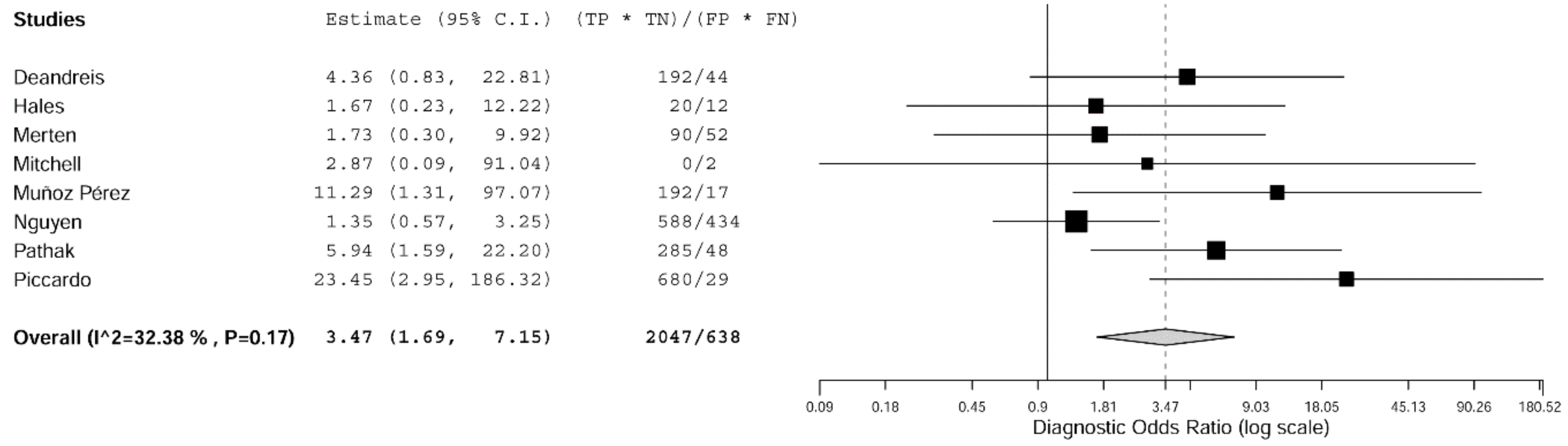
| Sensitivity (95% CI) | Specificity (95% CI) | Positive Predictive Value (95% CI) | Negative Predictive Value (95% CI) | Likelihood Ratio for Positive Results (95% CI) | Likelihood Ratio for Negative Results (95% CI) | Diagnostic Odds Ratio (95% CI) |
|---|---|---|---|---|---|---|
| 74% (55–87) | 58% (48–67) | 34% (25–44) | 74% (41–100) | 1.7 (1.4–2.0) | 0.4 (0.2–0.7) | 3.5 (1.7–7.1) |
| I2 = NA | I2 = NA | I2 = 57% | I2 = 99% | I2 = 17% | I2 = 93% | I2 = 32% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castellana, M.; Trimboli, P.; Piccardo, A.; Giovanella, L.; Treglia, G. Performance of 18F-FDG PET/CT in Selecting Thyroid Nodules with Indeterminate Fine-Needle Aspiration Cytology for Surgery. A Systematic Review and a Meta-Analysis. J. Clin. Med. 2019, 8, 1333. https://doi.org/10.3390/jcm8091333
Castellana M, Trimboli P, Piccardo A, Giovanella L, Treglia G. Performance of 18F-FDG PET/CT in Selecting Thyroid Nodules with Indeterminate Fine-Needle Aspiration Cytology for Surgery. A Systematic Review and a Meta-Analysis. Journal of Clinical Medicine. 2019; 8(9):1333. https://doi.org/10.3390/jcm8091333
Chicago/Turabian StyleCastellana, Marco, Pierpaolo Trimboli, Arnoldo Piccardo, Luca Giovanella, and Giorgio Treglia. 2019. "Performance of 18F-FDG PET/CT in Selecting Thyroid Nodules with Indeterminate Fine-Needle Aspiration Cytology for Surgery. A Systematic Review and a Meta-Analysis" Journal of Clinical Medicine 8, no. 9: 1333. https://doi.org/10.3390/jcm8091333
APA StyleCastellana, M., Trimboli, P., Piccardo, A., Giovanella, L., & Treglia, G. (2019). Performance of 18F-FDG PET/CT in Selecting Thyroid Nodules with Indeterminate Fine-Needle Aspiration Cytology for Surgery. A Systematic Review and a Meta-Analysis. Journal of Clinical Medicine, 8(9), 1333. https://doi.org/10.3390/jcm8091333