Vitamin D Deficiency is Associated with Increased Disease Activity in Patients with Inflammatory Bowel Disease


Abstract
1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Quantification of 25-hydroxyvitamin D (25(OH)D3) Serum Levels and Other Laboratory Parameters
2.3. Disease Activity and IBD-related Medication
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. 25(OH)D3 Serum Concentrations and Associated Seasonal Variations
3.3. IBD-related Medication
3.4. Logistic Regression Analysis for Parameters Associated with Vitamin D Deficiency
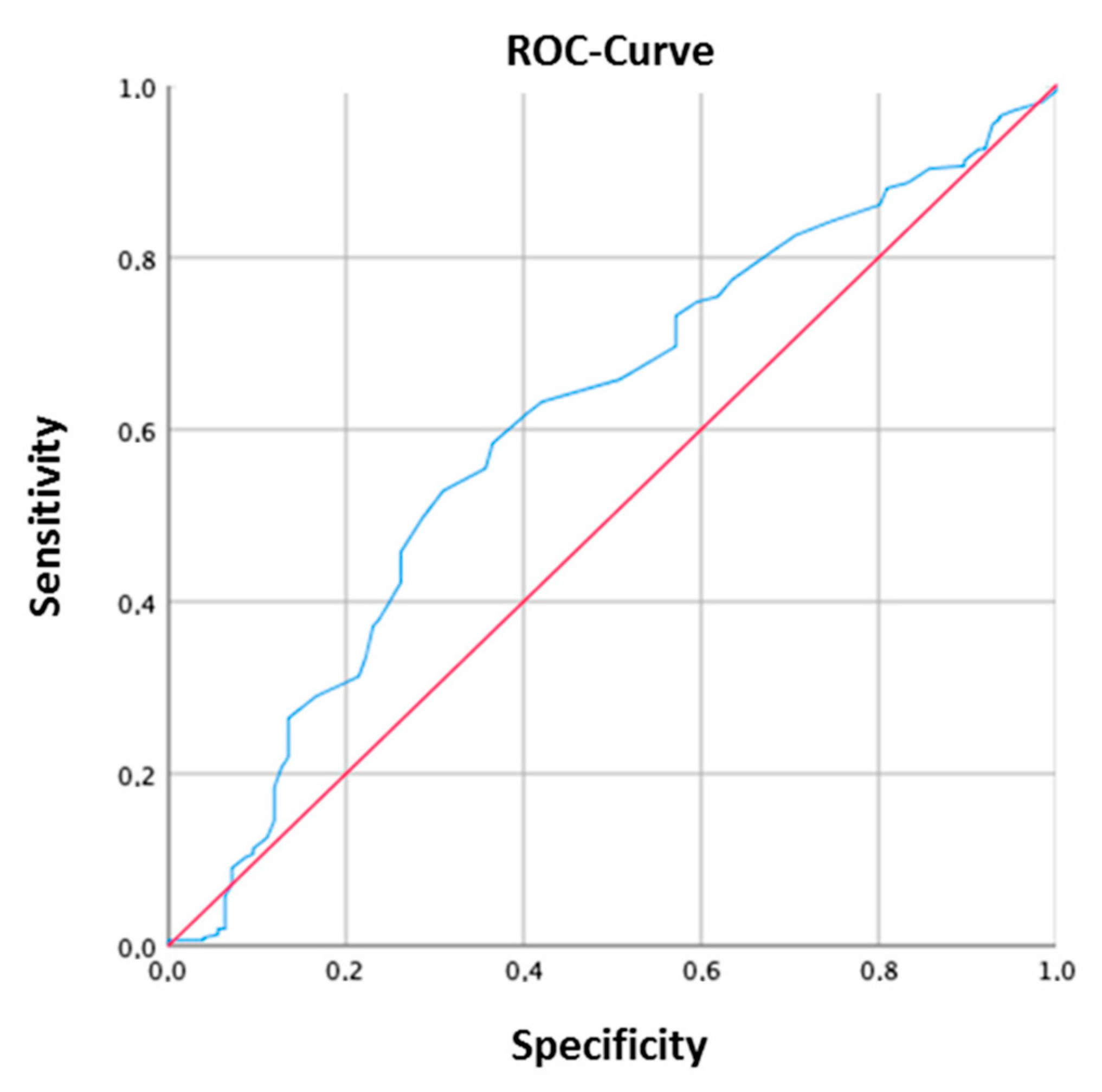
3.5. ROC Analysis to Determine 25(OH)D3 Serum Concentration CutOff
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Shih, D.Q.; Targan, S.R. Immunopathogenesis of inflammatory bowel disease. World J. Gastroenterol. 2008, 14, 390–400. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.T.; Stenger, S.; Li, H.; Wenzel, L.; Tan, B.H.; Krutzik, S.R.; Ochoa, M.T.; Schauber, J.; Wu, K.; Meinken, C.; et al. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science 2006, 311, 1770–1773. [Google Scholar] [CrossRef] [PubMed]
- Gombart, A.F.; Borregaard, N.; Koeffler, H.P. Human cathelicidin antimicrobial peptide (CAMP) gene is a direct target of the vitamin D receptor and is strongly up-regulated in myeloid cells by 1,25-dihydroxyvitamin D3. FASEB J. 2005, 19, 1067–1077. [Google Scholar] [CrossRef] [PubMed]
- Ramagopalan, S.V.; Heger, A.; Berlanga, A.J.; Maugeri, N.J.; Lincoln, M.R.; Burrell, A.; Handunnetthi, L.; Handel, A.E.; Disanto, G.; Orton, S.-M.; et al. A ChIP-seq defined genome-wide map of vitamin D receptor binding: Associations with disease and evolution. Genome Res. 2010, 20, 1352–1360. [Google Scholar] [CrossRef] [PubMed]
- De Souza, H.S.P.; Fiocchi, C. Immunopathogenesis of IBD: Current state of the art. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.; Cooper, S.C.; Ghosh, S.; Hewison, M. The Role of Vitamin D in Inflammatory Bowel Disease: Mechanism to Management. Nutrients 2019, 11, 1019. [Google Scholar] [CrossRef]
- Schaffler, H.; Herlemann, D.P.; Klinitzke, P.; Berlin, P.; Kreikemeyer, B.; Jaster, R.; Lamprecht, G. Vitamin D administration leads to a shift of the intestinal bacterial composition in Crohn’s disease patients, but not in healthy controls. J. Dig. Dis. 2018, 19, 225–234. [Google Scholar] [CrossRef]
- Liu, W.; Chen, Y.; Golan, M.A.; Annunziata, M.L.; Du, J.; Dougherty, U.; Kong, J.; Musch, M.; Huang, Y.; Pekow, J.; et al. Intestinal epithelial vitamin D receptor signaling inhibits experimental colitis. J. Clin. Investig. 2013, 123, 3983–3996. [Google Scholar] [CrossRef]
- Kong, J.; Zhang, Z.; Musch, M.W.; Ning, G.; Sun, J.; Hart, J.; Bissonnette, M.; Li, Y.C. Novel role of the vitamin D receptor in maintaining the integrity of the intestinal mucosal barrier. Am. J. Physiol. Gastrointest. Liver Physiol. 2008, 294, G208–G216. [Google Scholar] [CrossRef]
- Zhao, H.; Zhang, H.; Wu, H.; Li, H.; Liu, L.; Guo, J.; Li, C.; Shih, D.Q.; Zhang, X. Protective role of 1,25(OH)2 vitamin D3 in the mucosal injury and epithelial barrier disruption in DSS-induced acute colitis in mice. BMC Gastroenterol. 2012, 12, 57. [Google Scholar] [CrossRef] [PubMed]
- Barbalho, S.M.; Goulart, R.D.A.; Batista, G.L.D.S.A. Vitamin A and inflammatory bowel diseases: From cellular studies and animal models to human disease. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, A.N.; Khalili, H.; Higuchi, L.M.; Bao, Y.; Korzenik, J.R.; Giovannucci, E.L.; Richter, J.M.; Fuchs, C.S.; Chan, A.T. Higher predicted vitamin D status is associated with reduced risk of Crohn’s disease. Gastroenterology 2012, 142, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Ulitsky, A.; Ananthakrishnan, A.N.; Naik, A.; Skaros, S.; Zadvornova, Y.; Binion, D.G.; Issa, M. Vitamin D deficiency in patients with inflammatory bowel disease: Association with disease activity and quality of life. JPEN J. Parenter. Enteral Nutr. 2011, 35, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Del Pinto, R.; Pietropaoli, D.; Chandar, A.K.; Ferri, C.; Cominelli, F. Association between Inflammatory Bowel Disease and Vitamin D Deficiency: A Systematic Review and Meta-analysis. Inflamm. Bowel Dis. 2015, 21, 2708–2717. [Google Scholar] [CrossRef] [PubMed]
- Blanck, S.; Aberra, F. Vitamin d deficiency is associated with ulcerative colitis disease activity. Dig. Dis. Sci. 2013, 58, 1698–1702. [Google Scholar] [CrossRef] [PubMed]
- Forbes, A.; Escher, J.; Hebuterne, X.; Klek, S.; Krznaric, Z.; Schneider, S.; Shamir, R.; Stardelova, K.; Wierdsma, N.; Wiskin, A.E.; et al. ESPEN guideline. Clinical nutrition in inflammatory bowel disease. Clin. Nutr. 2007, 36, 321–347. [Google Scholar] [CrossRef]
- Vermeire, S.; Schreiber, S.; Sandborn, W.J.; Dubois, C.; Rutgeerts, P. Correlation between the Crohn’s disease activity and Harvey-Bradshaw indices in assessing Crohn’s disease severity. Clin. Gastroenterol. Hepatol. 2010, 8, 357–363. [Google Scholar] [CrossRef]
- Harvey, R.F.; Bradshaw, J.M. A simple index of Crohn’s-disease activity. Lancet 1980, 1, 514. [Google Scholar] [CrossRef]
- Walmsley, R.S.; Ayres, R.C.; Pounder, R.E.; Allan, R.N. A simple clinical colitis activity index. Gut 1998, 43, 29–32. [Google Scholar] [CrossRef]
- Jowett, S.L.; Seal, C.J.; Phillips, E.; Gregory, W.; Barton, J.R.; Welfare, M.R. Defining relapse of ulcerative colitis using a symptom-based activity index. Scand. J. Gastroenterol. 2003, 38, 164–171. [Google Scholar] [CrossRef]
- Rosen, C.J. Clinical practice. Vitamin D insufficiency. N. Engl. J. Med. 2011, 364, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Chetcuti Zammit, S.; Ellul, P.; Girardin, G.; Valpiani, D.; Nielsen, K.R.; Olsen, J.; Goldis, A.; Lazar, D.; Shonova, O.; Novakova, M.; et al. Vitamin D deficiency in a European inflammatory bowel disease inception cohort: An Epi-IBD study. Eur. J. Gastroenterol. Hepatol. 2018, 30, 1297–1303. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, A.N.; Cagan, A.; Gainer, V.S.; Cai, T.; Cheng, S.-C.; Savova, G.; Chen, P.; Szolovits, P.; Xia, Z.; de Jager, P.L.; et al. Normalization of plasma 25-hydroxy vitamin D is associated with reduced risk of surgery in Crohn’s disease. Inflamm. Bowel Dis. 2013, 19, 1921–1927. [Google Scholar] [CrossRef] [PubMed]
- Kabbani, T.A.; Koutroubakis, I.E.; Schoen, R.E.; Ramos-Rivers, C.; Shah, N.; Swoger, J.; Regueiro, M.; Barrie, A.; Schwartz, M.; Hashash, J.G.; et al. Association of Vitamin D Level With Clinical Status in Inflammatory Bowel Disease: A 5-Year Longitudinal Study. Am. J. Gastroenterol. 2016, 111, 712–719. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Ko, K.H.; Kim, Y.S.; Lee, B.K.; Choi, J.H.; Woo, Y.M.; Kim, J.Y.; Moon, J.S. Vitamin D deficiency is associated with disease activity in patients with Crohn’s disease. Intest. Res. 2019, 17, 70–77. [Google Scholar] [CrossRef]
- Caviezel, D.; Maissen, S.; Niess, J.H.; Kiss, C.; Hruz, P. High Prevalence of Vitamin D Deficiency among Patients with Inflammatory Bowel Disease. Inflamm. Intest. Dis. 2018, 2, 200–210. [Google Scholar] [CrossRef]
- Frigstad, S.O.; Hoivik, M.; Jahnsen, J.; Dahl, S.R.; Cvancarova, M.; Grimstad, T.; Berset, I.P.; Huppertz-Hauss, G.; Hovde, O.; Torp, R.; et al. Vitamin D deficiency in inflammatory bowel disease: Prevalence and predictors in a Norwegian outpatient population. Scand. J. Gastroenterol. 2017, 52, 100–106. [Google Scholar] [CrossRef]
- Suibhne, T.N.; Cox, G.; Healy, M.; O’Morain, C.; O’Sullivan, M. Vitamin D deficiency in Crohn’s disease: Prevalence, risk factors and supplement use in an outpatient setting. J. Crohns. Colitis 2012, 6, 182–188. [Google Scholar] [CrossRef]
- Janssen, C.E.; Globig, A.M.; Busse Grawitz, A.; Bettinger, D.; Hasselblatt, P. Seasonal variability of vitamin D status in patients with inflammatory bowel disease—A retrospective cohort study. PLoS ONE 2019, 14, e0217238. [Google Scholar] [CrossRef] [PubMed]
- Garg, M.; Rosella, O.; Lubel, J.S.; Gibson, P.R. Association of circulating vitamin D concentrations with intestinal but not systemic inflammation in inflammatory bowel disease. Inflamm. Bowel Dis. 2013, 19, 2634–2643. [Google Scholar] [CrossRef] [PubMed]
- Mechie, N.-C.; Mavropoulou, E.; Ellenrieder, V.; Petzold, G.; Kunsch, S.; Neesse, A.; Amanzada, A. Serum vitamin D but not zinc levels are associated with different disease activity status in patients with inflammatory bowel disease. Medicine (Baltimore) 2019, 98, e15172. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameters | Entire Cohort n = 470 | Ulcerative Colitis n = 198 | Crohn’s Disease n = 272 | p Value |
|---|---|---|---|---|
| Female sex, n (%) | 257 (54.7) | 94 (47.5) | 163 (59.9) | |
| Age, median (range) | 41 (18–84) | 45 (18–84) | 39 (18–84) | p = 0.027 |
| Remission # | 312 (71.6) | 161 (83.9) | 151 (61.9) | p < 0.0001 |
| HBI, mean (SD) | N/A | N/A | 4.23 (3.56) | |
| SCCAI, mean (SD) | N/A | 2.15 (2.46) | N/A | |
| CRP mg/dL, mean (SD) | 0.66 (1.2) | 0.55 (0.9) | 0.74 (1.3) | p = 0.049 |
| Leukocytes/nL, mean (SD) | 8.17 (2.9) | 7.88 (2.9) | 8.38 (2.8) | p = 0.012 |
| Biological Therapy * | 199 (53.4) | 54 (32.9) | 145 (69.4) | p < 0.0001 |
| 25(OH)D3 (ng/mL); median (range) | 26 (3–100) | 28 (3–100) | 25.5 (3–76) | p = 0.049 |
| Vit D supplementation | 245 (53.6) | 108 (55.7) | 137 (52.1) | |
| Vit D measured in winter | 303 (64.5) | 139 (70.2) | 164 (60.3) | |
| fCal µg/g, mean (SD) | 315 (352) | 356 (367) | 289 (341) |
| 25(OH)D3 Serum Levels ng/mL | Number of Patients |
|---|---|
| Overall (n = 470) | (%) |
| 25(OH)D3 ≥ 30 ng/mL, n (%) | 188 (40) |
| 25(OH)D3 30–10 ng/mL, n (%) | 232 (49.4) |
| 25(OH)D3 < 10 ng/mL, n (%) | 49 (10.4) |
| Crohn’s disease (n = 272) | |
| 25(OH)D3 ≥ 30 ng/mL, n (%) | 99 (36.4) |
| 25(OH)D3 30–10 ng/mL, n (%) | 144 (52.9) |
| 25(OH)D3 < 10 ng/mL, n (%) | 28 (10.3) |
| Ulcerative colitis (n = 198) | |
| 25(OH)D3 ≥ 30 ng/mL, n (%) | 89 (44.9) |
| 25(OH)D3 30–10 ng/mL, n (%) | 88 (44.4) |
| 25(OH)D3 < 10 ng/mL, n (%) | 21 (10.6) |
| Medication | Entire Cohort | Ulcerative Colitis | Crohn’s Disease |
|---|---|---|---|
| Conventional Treatment | 169 (36) | 110 (55.6) | 64 (30.6) |
| 5-ASA total, n (%) | 86 (23) | 75 (37.8) | 17 (6.3) |
| 5-ASA, n (%) | 74 (19.8) | 57 (28.8) | 17 (6.3) |
| 5-ASA in combination, n (%) | 12 (3.2) | 18 (9) | N/A |
| Glucocorticoids, n (%) | 21 (5.6) | 9 (4.5) | 12 (4.4) |
| Azathioprine/6-MP total, n (%) | 52 (13.9) | 21 (10.6) | 31 (11.7) |
| Azathioprine/6-MP, n (%) | 38 (10.2) | 12 (6.1) | 26 (9.8) |
| Azathioprine/6-MP in combination, n (%) | 14 (3.7) | 9 (4.5) | 5 (1.9) |
| Other Therapies, n (%) | 10 (2.7) | 5 (2.5) | 4 (1.5) |
| Biological treatment | 198 (42.1) | 51 (25.7) | 140 (50) |
| TNFα Inhibitor total, n (%) | 105 (28.1) | 22 (11.1) | 78 (29.5) |
| TNFα Inhibitor, n (%) | 77 (20.6) | 10 (5) | 62 (23.4) |
| TNFα Inhibitor in combination, n (%) | 28 (7.5) | 12 (6.1) | 16 (6.1) |
| Integrin Inhibitor total, n (%) | 65 (17.4) | 29 (14.6) | 36 (13.6) |
| Integrin inhibitor, n (%) | 51 (13.7) | 20 (10) | 32 (12.1) |
| Integrin inhibitor in combination, n (%) | 14 (3.7) | 9 (4) | 4 (1.5) |
| Il12/23 blocker, n (%) | 26 (6.9) | N/A | 26 (9.6%) |
| No treatment | 90 (19.1) | 28 (14.4) | 62 (22.8) |
| Missing information | 13 (2.8) | 9 (4.5) | 6 (2.3) |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| p Value | OR (95% CI) | p Value | OR (95% CI) | |
| Entire cohort | ||||
| Age | 0.007 | 1.01 (1.00–1.03) | ||
| Male Gender | 0.05 | 1.44 (0.96–2.09) | 0.06 | 1.69 (0.96–2.97) |
| Remission (yes) | 0.0001 | 2.38 (1.56–3.64) | 0.02 | 2.01 (1.10–3.69) |
| Leukocytes | 0.049 | 0.93 (0.87–0.99) | ||
| fCal µg/g | 0.042 | 0.99 (0.99–1.00) | ||
| Vit. D supplementation (yes) | 0.0001 | 3.74 (2.50–5.61) | 0.0001 | 4.64 (2.56–8.39) |
| Biological therapy (yes) | 0.032 | 0.63 (0.42–0.96) | ||
| Crohn’s disease | ||||
| Remission (yes) | 0.001 | 2.51 (1.47–4.28) | 0.05 | 2.11 (0.97–4.56) |
| fCal µg/g | 0.03 | 0.99 (0.99–1.00) | 0.05 | 0.99 (0.99–1.00) |
| Vit. D supplementation (yes) | 0.0001 | 3.72 (2.16–6.39) | 0.0001 | 4.37 (1.91–10.00) |
| Biological therapy (yes) | 0.009 | 0.45 (0.24–0.82) | 0.01 | 0.35 (0.15–0.81) |
| Ulcerative colitis | ||||
| Age | 0.006 | 1.02 (1.00–1.05) | 0.04 | 1.02 (1.00–1.04) |
| Male Gender | 0.020 | 1.98 (1.20–3.50) | 0.003 | 2.70 (1.40–5.18) |
| Remission (yes) | 0.07 | 2.13 (0.92–4.91) | ||
| Vit. D supplementation (yes) | 0.0001 | 3.75 (2.04–6.90) | 0.0001 | 4.35 (2.23–8.47) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hausmann, J.; Kubesch, A.; Amiri, M.; Filmann, N.; Blumenstein, I. Vitamin D Deficiency is Associated with Increased Disease Activity in Patients with Inflammatory Bowel Disease. J. Clin. Med. 2019, 8, 1319. https://doi.org/10.3390/jcm8091319
Hausmann J, Kubesch A, Amiri M, Filmann N, Blumenstein I. Vitamin D Deficiency is Associated with Increased Disease Activity in Patients with Inflammatory Bowel Disease. Journal of Clinical Medicine. 2019; 8(9):1319. https://doi.org/10.3390/jcm8091319
Chicago/Turabian StyleHausmann, Johannes, Alica Kubesch, Mana Amiri, Natalie Filmann, and Irina Blumenstein. 2019. "Vitamin D Deficiency is Associated with Increased Disease Activity in Patients with Inflammatory Bowel Disease" Journal of Clinical Medicine 8, no. 9: 1319. https://doi.org/10.3390/jcm8091319
APA StyleHausmann, J., Kubesch, A., Amiri, M., Filmann, N., & Blumenstein, I. (2019). Vitamin D Deficiency is Associated with Increased Disease Activity in Patients with Inflammatory Bowel Disease. Journal of Clinical Medicine, 8(9), 1319. https://doi.org/10.3390/jcm8091319