Remifentanil Alleviates Propofol-Induced Burst Suppression without Affecting Bispectral Index in Female Patients: A Randomized Controlled Trial

Abstract
:1. Introduction
2. Method
2.1. Study Design and Data Collection
2.2. Statistical Analysis
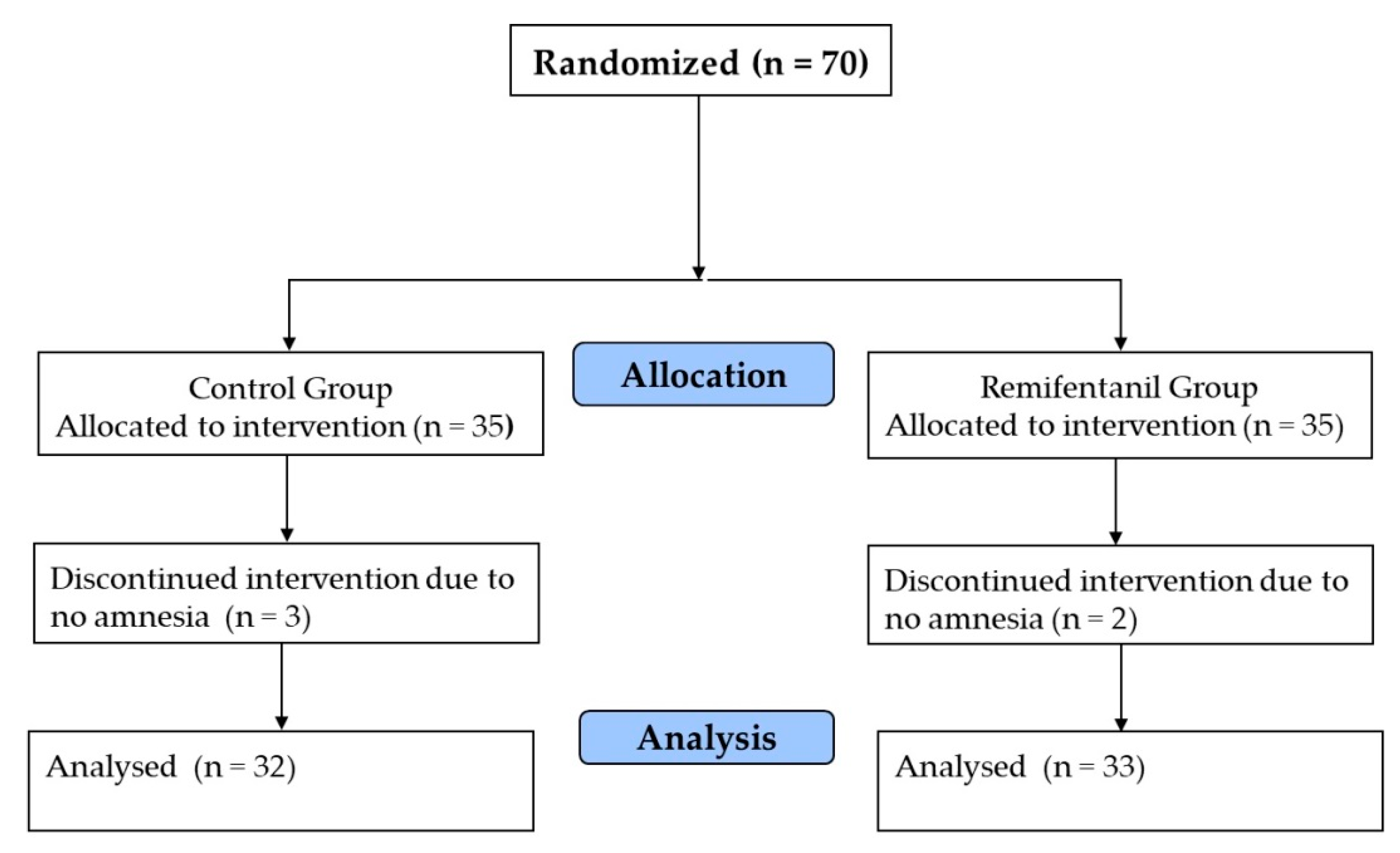
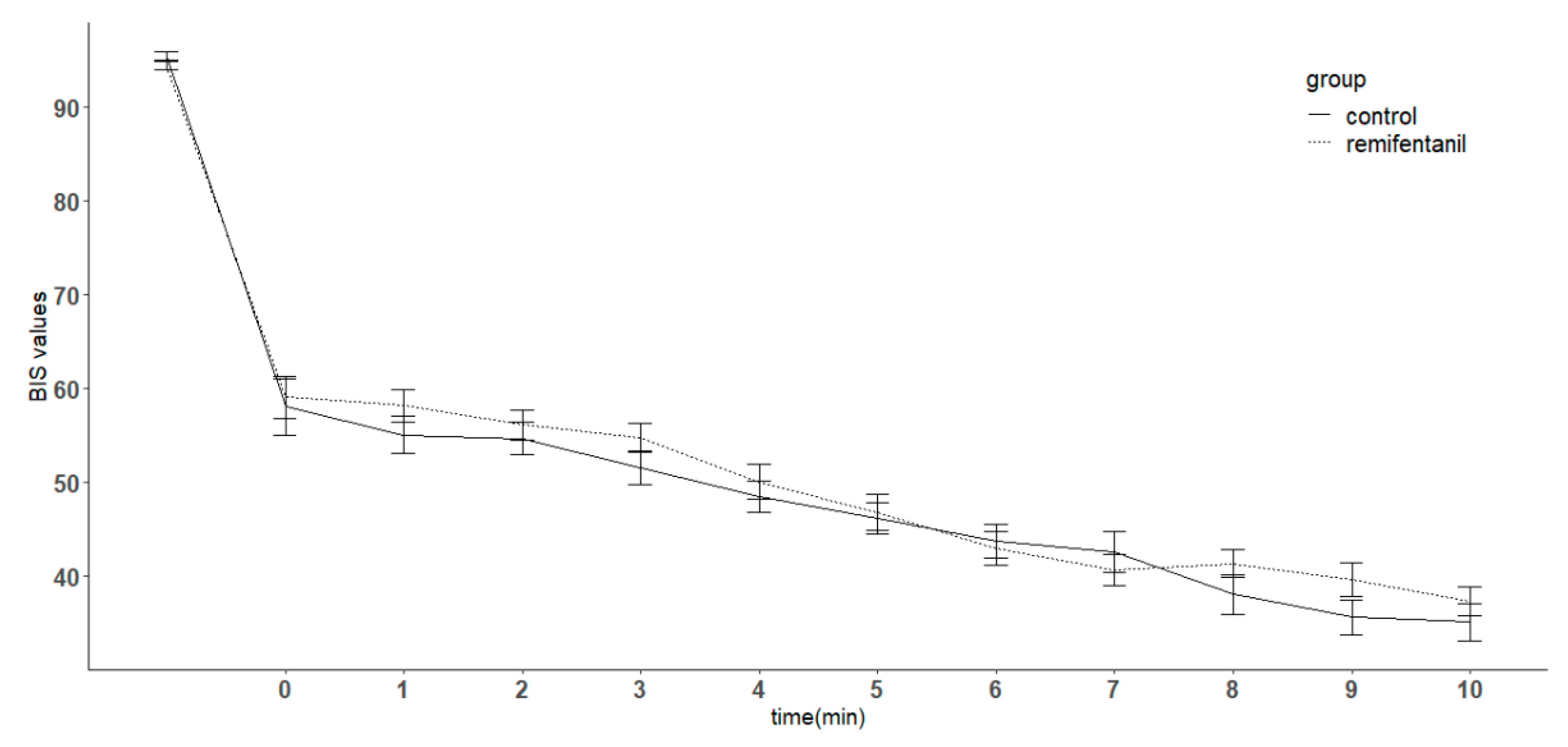
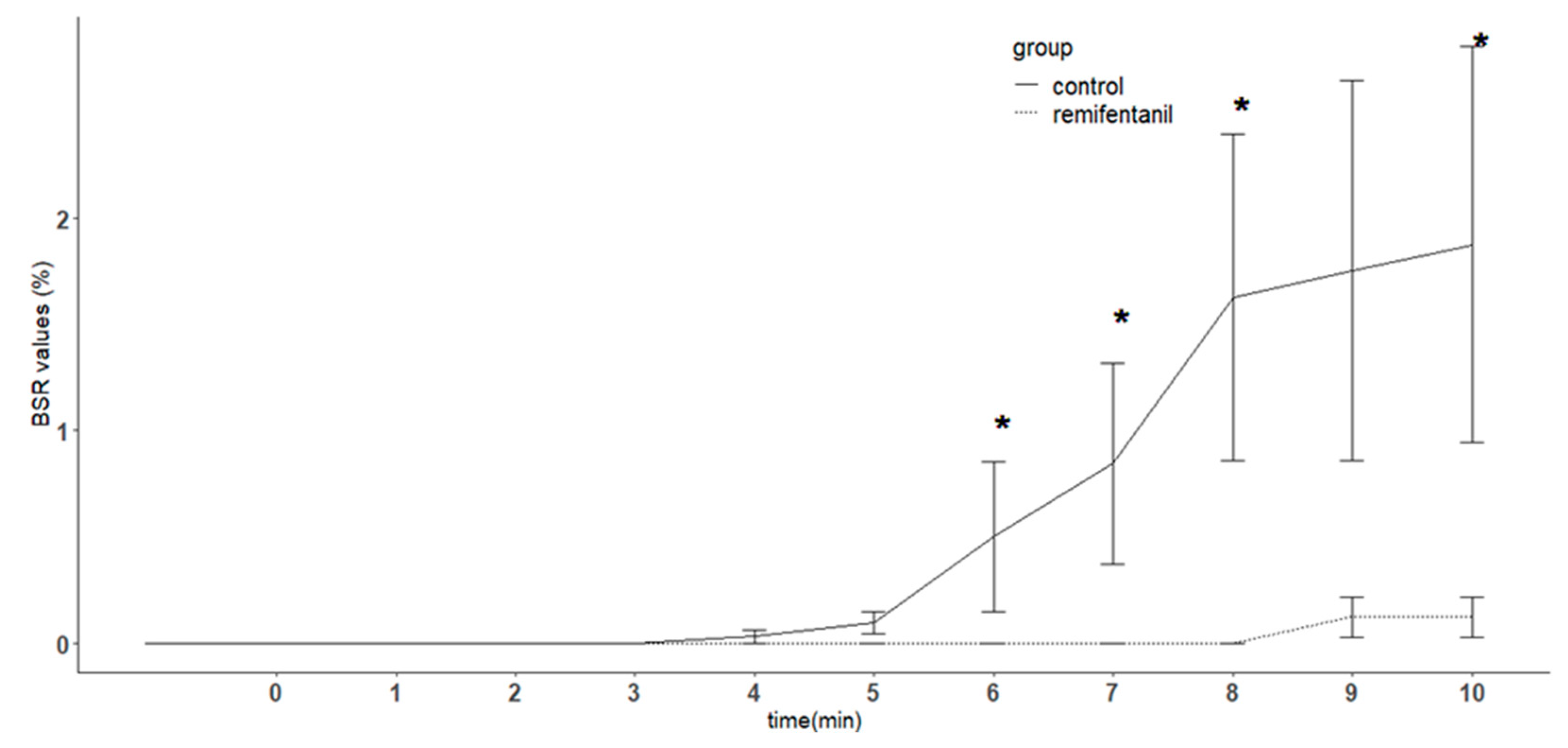
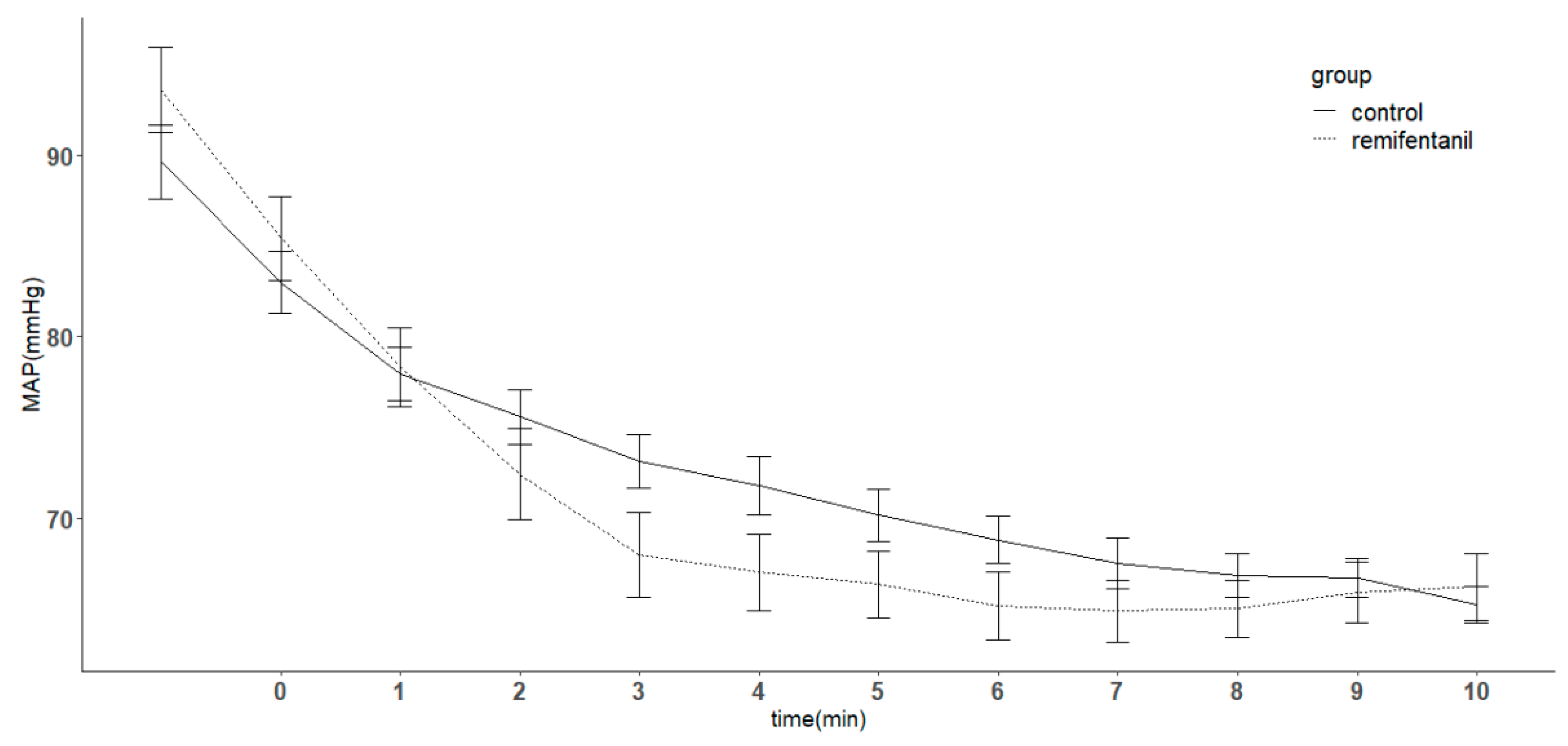
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Glass, P.S.; Bloom, M.; Kearse, L.; Rosow, C.; Sebel, P.; Manberg, P. Bispectral analysis measures sedation and memory effects of propofol, midazolam, isoflurane, and alfentanil in healthy volunteers. Anesthesiology 1997, 86, 836–847. [Google Scholar] [CrossRef] [PubMed]
- Guignard, B.; Menigaux, C.; Dupont, X.; Fletcher, D.; Chauvin, M. The effect of remifentanil on the bispectral index change and hemodynamic responses after orotracheal intubation. Anesth. Analg. 2000, 90, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Andrzejowski, J.; Sleigh, J.W.; Johnson, I.A.; Sikiotis, L. The effect of intravenous epinephrine on the bispectral index and sedation. Anaesthesia 2000, 55, 761–763. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, T.W.; Bruhn, J.; Radulescu, L.; Andresen, C.; Shafer, T.J.; Cohane, C.; Shafer, S.L. Pharmacodynamic interaction between propofol and remifentanil regarding hypnosis, tolerance of laryngoscopy, bispectral index, and electroencephalographic approximate entropy. Anesthesiology 2004, 100, 1353–1372. [Google Scholar] [CrossRef] [PubMed]
- Schuller, P.J.; Newell, S.; Strickland, P.A.; Barry, J.J. Response of bispectral index to neuromuscular block in awake volunteers. Br. J. Anaesth. 2015, 115 (Suppl. 1), i95–i103. [Google Scholar] [CrossRef]
- Dahaba, A.A.; Mattweber, M.; Fuchs, A.; Zenz, W.; Rehak, P.H.; List, W.F.; Metzler, H. The effect of different stages of neuromuscular block on the bispectral index and the bispectral index-XP under remifentanil/propofol anesthesia. Anesth. Analg. 2004, 99, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Nunes, R.R.; Bersot, C.D.A.; Garritano, J.G. Intraoperative neurophysiological monitoring in neuroanesthesia. Curr. Opin. Anaesthesiol. 2018, 31, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, D.A.; Nunes, C.S.; Antunes, L.M.; Santos, I.A.; Lobo, F.; Casal, M.; Ferreira, L.; Amorim, P. The effect of a remifentanil bolus on the bispectral index of the EEG (BIS) in anaesthetized patients independently from intubation and surgical stimuli. Eur. J. Anaesthesiol. 2006, 23, 305–310. [Google Scholar] [CrossRef]
- Albertin, A.; Casati, A.; Federica, L.; Roberto, V.; Travaglini, V.; Bergonzi, P.; Torri, G. The effect-site concentration of remifentanil blunting cardiovascular responses to tracheal intubation and skin incision during bispectral index-guided propofol anesthesia. Anesth. Analg. 2005, 101, 125–130. [Google Scholar] [CrossRef]
- Yufune, S.; Takamatsu, I.; Masui, K.; Kazama, T. Effect of remifentanil on plasma propofol concentration and bispectral index during propofol anaesthesia. Br. J. Anaesth. 2011, 106, 208–214. [Google Scholar] [CrossRef]
- Nieuwenhuijs, D.J.; Olofsen, E.; Romberg, R.R.; Sarton, E.; Ward, D.; Engbers, F.; Vuyk, J.; Mooren, R.; Teppema, L.J.; Dahan, A. Response surface modeling of remifentanil-propofol interaction on cardiorespiratory control and bispectral index. Anesthesiology 2003, 98, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Strachan, A.N.; Edwards, N.D. Randomized placebo-controlled trial to assess the effect of remifentanil and propofol on bispectral index and sedation. Br. J. Anaesth. 2000, 84, 489–490. [Google Scholar] [CrossRef] [PubMed]
- Amzica, F. What does burst suppression really mean? Epilepsy Behav. 2015, 49, 234–237. [Google Scholar] [CrossRef]
- Yoshitani, K.; Kawaguchi, M.; Takahashi, M.; Kitaguchi, K.; Furuya, H. Plasma propofol concentration and EEG burst suppression ratio during normothermic cardiopulmonary bypass. Br. J. Anaesth. 2003, 90, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Declerck, A.; Liu, N.; Chazot, T.; Fischler, M. BIS values during resuscitation: the role of the suppression ratio (case report). J. Clin. Monit. Comput. 2009, 23, 307–309. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Chazot, T.; Mutter, C.; Fischler, M. Elevated burst suppression ratio: the possible role of hypoxemia. Anesth. Analg. 2006, 103, 1609–1610. [Google Scholar] [CrossRef]
- Seder, D.B.; Fraser, G.L.; Robbins, T.; Libby, L.; Riker, R.R. The bispectral index and suppression ratio are very early predictors of neurological outcome during therapeutic hypothermia after cardiac arrest. Intensive Care Med. 2010, 36, 281–288. [Google Scholar] [CrossRef]
- Besch, G.; Liu, N.; Samain, E.; Pericard, C.; Boichut, N.; Mercier, M.; Chazot, T.; Pili-Floury, S. Occurrence of and risk factors for electroencephalogram burst suppression during propofol-remifentanil anaesthesia. Br. J. Anaesth. 2011, 107, 749–756. [Google Scholar] [CrossRef]
- Fritz, B.A.; Kalarickal, P.L.; Maybrier, H.R.; Muench, M.R.; Dearth, D.; Chen, Y.; Escallier, K.E.; Ben Abdallah, A.; Lin, N.; Avidan, M.S. Intraoperative Electroencephalogram Suppression Predicts Postoperative Delirium. Anesth. Analg. 2016, 122, 234–242. [Google Scholar] [CrossRef] [Green Version]
- Soehle, M.; Dittmann, A.; Ellerkmann, R.K.; Baumgarten, G.; Putensen, C.; Guenther, U. Intraoperative burst suppression is associated with postoperative delirium following cardiac surgery: a prospective, observational study. BMC Anesthesiol. 2015, 15, 61. [Google Scholar] [CrossRef]
- Joe, H.B.; Kim, J.Y.; Kwak, H.J.; Oh, S.E.; Lee, S.Y.; Park, S.Y. Effect of sex differences in remifentanil requirements for the insertion of a laryngeal mask airway during propofol anesthesia: A prospective randomized trial. Medicine (Baltimore) 2016, 95, e5032. [Google Scholar] [CrossRef] [PubMed]
- Pleym, H.; Spigset, O.; Kharasch, E.D.; Dale, O. Gender differences in drug effects: implications for anesthesiologists. Acta Anaesthesiol. Scand. 2003, 47, 241–259. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.H.; Lim, S.J.; Kim, M.J.; Jeon, J.P.; Moon, Y.E.; Kim, J.E.; Lee, Y.K. The effect of music on the effect-site concentration of propofol for loss of consciousness. Korean J. Anesthesiol. 2008, 55, 156–160. [Google Scholar] [CrossRef]
- Xu, Z.; Liu, F.; Yue, Y.; Ye, T.; Zhang, B.; Zuo, M.; Xu, M.; Hao, R.; Xu, Y.; Yang, N.; et al. C50 for propofol-remifentanil target-controlled infusion and bispectral index at loss of consciousness and response to painful stimulus in Chinese patients: a multicenter clinical trial. Anesth. Analg. 2009, 108, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Chazot, T.; Huybrechts, I.; Law-Koune, J.D.; Barvais, L.; Fischler, M. The influence of a muscle relaxant bolus on bispectral and datex-ohmeda entropy values during propofol-remifentanil induced loss of consciousness. Anesth. Analg. 2005, 101, 1713–1718. [Google Scholar] [CrossRef] [PubMed]
- Bruhn, J.; Bouillon, T.W.; Shafer, S.L. Bispectral index (BIS) and burst suppression: revealing a part of the BIS algorithm. J. Clin. Monit. Comput. 2000, 16, 593–596. [Google Scholar] [CrossRef] [PubMed]
- Kreuer, S.; Bruhn, J.; Larsen, R.; Grundmann, U.; Shafer, S.L.; Wilhelm, W. Application of Bispectral Index and Narcotrend index to the measurement of the electroencephalographic effects of isoflurane with and without burst suppression. Anesthesiology 2004, 101, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Watson, P.L.; Shintani, A.K.; Tyson, R.; Pandharipande, P.P.; Pun, B.T.; Ely, E.W. Presence of electroencephalogram burst suppression in sedated, critically ill patients is associated with increased mortality. Crit. Care Med. 2008, 36, 3171–3177. [Google Scholar] [CrossRef] [Green Version]
- Kortelainen, J.; Koskinen, M.; Mustola, S.; Seppänen, T. Effects of remifentanil on the spectrum and quantitative parameters of electroencephalogram in propofol anesthesia. Anesthesiology 2009, 111, 574–583. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (n = 32) | Remifentanil (n = 33) | p-Value | |
|---|---|---|---|
| Age (year) | 43.6 (7.7) | 41.5 (7.8) | 0.28 |
| Height (cm) | 160.1 (5.3) | 160.3(5.3) | 0.84 |
| Weight (kg) | 56.8 (6.6) | 57.9(8.5) | 0.54 |
| ASA physical status | |||
| I | 24 (75.0) | 24 (72.7) | 1 |
| II | 8 (25.0) | 9 (27.3) | - |
| BIS value | 95.4 (2.5) | 94.5 (2.8) | 0.13 |
| Mean blood pressure | 89.6 (11.4) | 93.6 (13.4) | 0.20 |
| Heart rate | 70.9 (11.9) | 73.6 (8.3) | 0.30 |
| 0~3 min | 4 min | 5 min | 6 min | 7 min | 8 min | 9 min | 10 min | |
|---|---|---|---|---|---|---|---|---|
| Control (n = 32) | 0 | 1 | 3 | 4 | 5 | 7 | 7 | 8 |
| Remifentanil (n = 33) | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 2 |
| p-value | 1 | 0.492 | 0.113 | 0.053 | <0.05 | <0.05 | 0.082 | <0.05 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, D.; Yang, S.; Lee, M.S.; Lee, Y. Remifentanil Alleviates Propofol-Induced Burst Suppression without Affecting Bispectral Index in Female Patients: A Randomized Controlled Trial. J. Clin. Med. 2019, 8, 1186. https://doi.org/10.3390/jcm8081186
Jung D, Yang S, Lee MS, Lee Y. Remifentanil Alleviates Propofol-Induced Burst Suppression without Affecting Bispectral Index in Female Patients: A Randomized Controlled Trial. Journal of Clinical Medicine. 2019; 8(8):1186. https://doi.org/10.3390/jcm8081186
Chicago/Turabian StyleJung, Dahye, Sungwon Yang, Min Soo Lee, and Yoonki Lee. 2019. "Remifentanil Alleviates Propofol-Induced Burst Suppression without Affecting Bispectral Index in Female Patients: A Randomized Controlled Trial" Journal of Clinical Medicine 8, no. 8: 1186. https://doi.org/10.3390/jcm8081186