Aortic Valve Sclerosis Adds to Prediction of Short-Term Mortality in Patients with Documented Coronary Atherosclerosis

 , , ,
, , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Methods
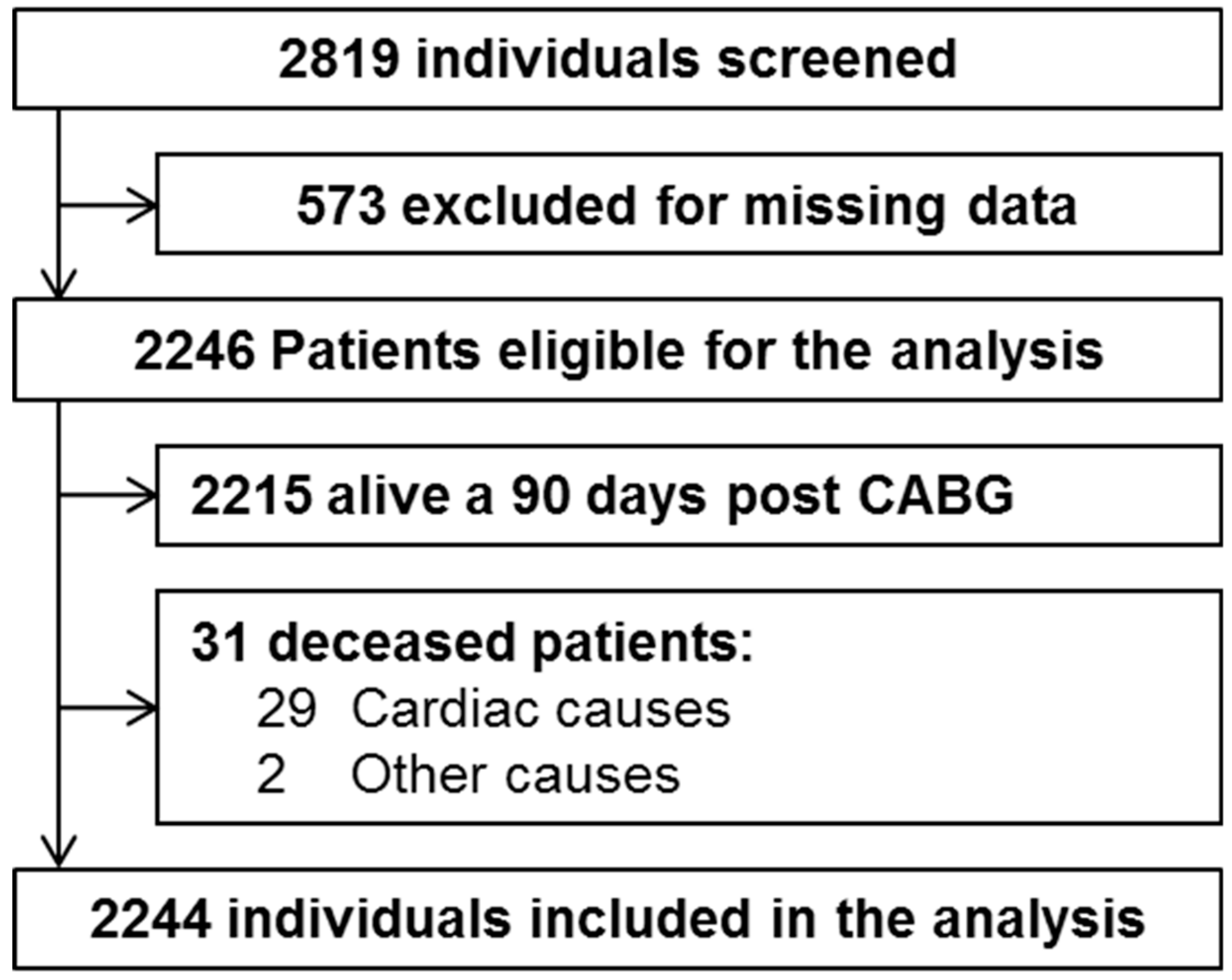
2.1. Patients
2.2. Echocardiographic Evaluation
2.3. Statistical Analysis
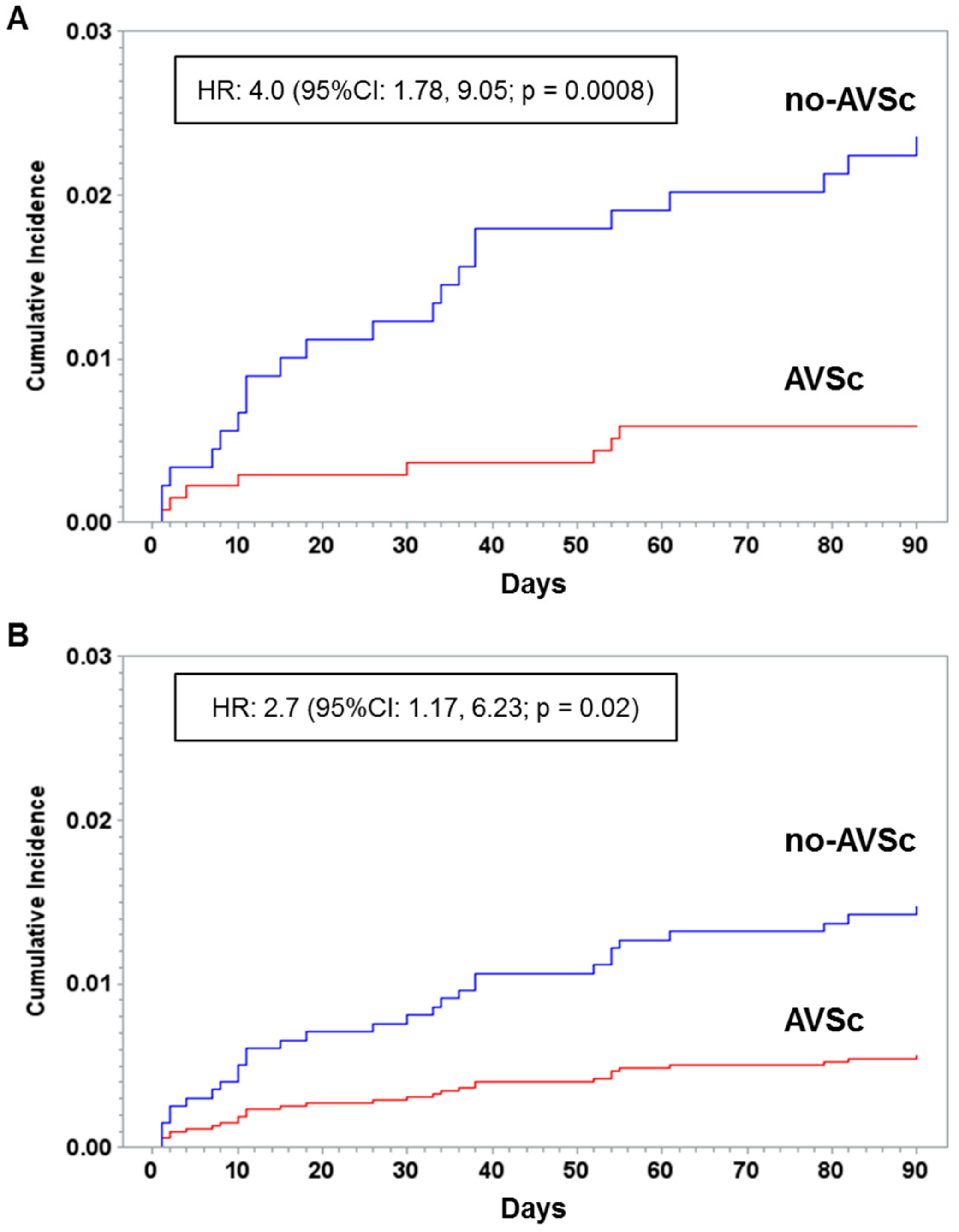
3. Results
4. Discussion
4.1. Clinical Relevance
4.2. Strengths and Limitations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gharacholou, S.M.; Karon, B.L.; Shub, C.; Pellikka, P.A. Aortic valve sclerosis and clinical outcomes: Moving toward a definition. Am. J. Med. 2011, 124, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Fleisher, L.A.; Jneid, H.; Mack, M.J.; McLeod, C.J.; O’Gara, P.T.; et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: A Report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation 2017. [Google Scholar] [CrossRef] [PubMed]
- Poggio, P.; Branchetti, E.; Grau, J.B.; Lai, E.K.; Gorman, R.C.; Gorman, J.H., 3rd; Sacks, M.S.; Bavaria, J.E.; Ferrari, G. Osteopontin-CD44v6 interaction mediates calcium deposition via phospho-Akt in valve interstitial cells from patients with noncalcified aortic valve sclerosis. Arterioscler Thromb. Vasc. Biol. 2014, 34, 2086–2094. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Kuusisto, J.; Reichenbach, D.D.; Gown, A.M.; O’Brien, K.D. Characterization of the early lesion of ‘degenerative’ valvular aortic stenosis. Histological and immunohistochemical studies. Circulation 1994, 90, 844–853. [Google Scholar] [CrossRef] [PubMed]
- Chandra, H.R.; Goldstein, J.A.; Choudhary, N.; O’Neill, C.S.; George, P.B.; Gangasani, S.R.; Cronin, L.; Marcovitz, P.A.; Hauser, A.M.; O’Neill, W.W. Adverse outcome in aortic sclerosis is associated with coronary artery disease and inflammation. J. Am. Coll. Cardiol. 2004, 43, 169–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otto, C.M.; Lind, B.K.; Kitzman, D.W.; Gersh, B.J.; Siscovick, D.S. Association of aortic-valve sclerosis with cardiovascular mortality and morbidity in the elderly. N. Engl. J. Med. 1999, 341, 142–147. [Google Scholar] [CrossRef]
- Shah, S.J.; Ristow, B.; Ali, S.; Na, B.Y.; Schiller, N.B.; Whooley, M.A. Acute myocardial infarction in patients with versus without aortic valve sclerosis and effect of statin therapy (from the Heart and Soul Study). Am. J. Cardiol. 2007, 99, 1128–1133. [Google Scholar] [CrossRef] [PubMed]
- Rabbani, M.S.; Qadir, I.; Ahmed, Y.; Gul, M.; Sharif, H. Heart valve surgery: EuroSCORE vs. EuroSCORE II vs. Society of Thoracic Surgeons score. Heart Int. 2014, 9, 53–58. [Google Scholar] [CrossRef]
- Kolh, P.; Windecker, S.; Alfonso, F.; Collet, J.P.; Cremer, J.; Falk, V.; Filippatos, G.; Hamm, C.; Head, S.J.; Jüni, P.; et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur. Heart J. 2014, 35, 2541–2619. [Google Scholar]
- Flachskampf, F.A.; Wouters, P.F.; Edvardsen, T.; Evangelista, A.; Habib, G.; Hoffman, P.; Hoffmann, R.; Lancellotti, P.; Pepi, M. Recommendations for transoesophageal echocardiography: EACVI update 2014. Eur. Heart J. Cardiovasc. Imaging. 2014, 15, 353–365. [Google Scholar] [CrossRef]
- Hahn, R.T.; Abraham, T.; Adams, M.S.; Bruce, C.J.; Glas, K.E.; Lang, R.M.; Reeves, S.T.; Shanewise, J.S.; Siu, S.C.; Stewart, W.; et al. Guidelines for performing a comprehensive transesophageal echocardiographic examination: Recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J. Am. Soc. Echocardiogr. 2013, 26, 921–964. [Google Scholar] [CrossRef] [PubMed]
- Cai, Q.; Serrano, R.; Kalyanasundaram, A.; Shirani, J. A preoperative echocardiographic predictive model for assessment of cardiovascular outcome after renal transplantation. J. Am. Soc. Echocardiogr. 2010, 23, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Valentijn, T.M.; Hoeks, S.E.; Bakker, E.J.; Voute, M.T.; Chonchol, M.; van de Luijtgaarden, K.M.; Verhagen, H.J.; Stolker, R.J. Influence of aortic valve calcium on outcome in patients undergoing peripheral vascular surgery. Am. J. Cardiol. 2012, 110, 1195–1199. [Google Scholar] [CrossRef] [PubMed]
- Volzke, H.; Haring, R.; Lorbeer, R.; Wallaschofski, H.; Reffelmann, T.; Empen, K.; Rettig, R.; John, U.; Felix, S.B.; Dorr, M. Heart valve sclerosis predicts all-cause and cardiovascular mortality. Atherosclerosis 2010, 209, 606–610. [Google Scholar] [CrossRef] [PubMed]
- Barasch, E.; Gottdiener, J.S.; Marino Larsen, E.K.; Chaves, P.H.; Newman, A.B. Cardiovascular morbidity and mortality in community-dwelling elderly individuals with calcification of the fibrous skeleton of the base of the heart and aortosclerosis (The Cardiovascular Health Study). Am. J. Cardiol. 2006, 97, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Targher, G.; Zoppini, G.; Cicoira, M.; Bonapace, S.; Negri, C.; Stoico, V.; Faggiano, P.; Vassanelli, C.; Bonora, E. Aortic and mitral annular calcifications are predictive of all-cause and cardiovascular mortality in patients with type 2 diabetes. Diabetes Care 2012, 35, 1781–1786. [Google Scholar] [CrossRef] [PubMed]
- Taylor, H.A., Jr.; Clark, B.L.; Garrison, R.J.; Andrew, M.E.; Han, H.; Fox, E.R.; Arnett, D.K.; Samdarshi, T.; Jones, D.W. Relation of aortic valve sclerosis to risk of coronary heart disease in African-Americans. Am. J. Cardiol. 2005, 95, 401–404. [Google Scholar] [CrossRef]
- Coffey, S.; Cox, B.; Williams, M.J. The prevalence, incidence, progression, and risks of aortic valve sclerosis: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2014, 63, 2852–2861. [Google Scholar] [CrossRef]
- Di Minno, M.N.D.; Di Minno, A.; Ambrosino, P.; Songia, P.; Pepi, M.; Tremoli, E.; Poggio, P. Cardiovascular morbidity and mortality in patients with aortic valve sclerosis: A systematic review and meta-analysis. Int. J. Cardiol. 2018, 260, 138–144. [Google Scholar] [CrossRef]
- Da Rosa, E.M.; Sant’anna, J.R.; Oppermann, L.P.; Castro, I. Prognosis of aortic valve sclerosis in cardiovascular mortality of patients seen at the cardiology institute of Rio Grande do Sul. Arq. Bras. Cardiol. 2007, 88, 234–239. [Google Scholar] [CrossRef]
- Owens, D.S.; Budoff, M.J.; Katz, R.; Takasu, J.; Shavelle, D.M.; Carr, J.J.; Heckbert, S.R.; Otto, C.M.; Probstfield, J.L.; Kronmal, R.A.; et al. Aortic valve calcium independently predicts coronary and cardiovascular events in a primary prevention population. JACC Cardiovasc. Imaging 2012, 5, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Corciu, A.I.; Siciliano, V.; Poggianti, E.; Petersen, C.; Venneri, L.; Picano, E. Cardiac calcification by transthoracic echocardiography in patients with known or suspected coronary artery disease. Int. J. Cardiol. 2010, 142, 288–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pradelli, D.; Faden, G.; Mureddu, G.; Rossi, A.; Cioffi, G.; Gaibazzi, N.; Soranna, D.; Corrao, G.; Faggiano, P. Impact of aortic or mitral valve sclerosis and calcification on cardiovascular events and mortality: A meta-analysis. Int. J. Cardiol. 2013, 170, e51–e55. [Google Scholar] [CrossRef] [PubMed]
- Barili, F.; Pacini, D.; D’Ovidio, M.; Dang, N.C.; Alamanni, F.; Di Bartolomeo, R.; Grossi, C.; Davoli, M.; Fusco, D.; Parolari, A. The impact of EuroSCORE II risk factors on prediction of long-term mortality. Ann. Thorac. Surg. 2016, 102, 1296–1303. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.W.; Hickey, G.L.; Dimarakis, I.; Trivedi, U.; Bryan, A.; Treasure, T.; Cooper, G.; Pagano, D.; Buchan, I.; Bridgewater, B. How does EuroSCORE II perform in UK cardiac surgery; an analysis of 23740 patients from the Society for Cardiothoracic Surgery in Great Britain and Ireland National Database. Heart 2012, 98, 1568–1572. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G. Practical Statistics for Medical Research; Chapman and Hall: London, UK, 1991; pp. 404–408. [Google Scholar]



{kind=link}
{kind=link}
| Variables | AVSc (n = 892) | No-AVSc (n = 1352) | p-Value |
|---|---|---|---|
| Age, years | 69.4 ± 7.8 | 64.7 ± 9.1 | <0.0001 |
| Male n, (%) | 708 (79.4) | 1174 (86.8) | <0.0001 |
| Body mass index, kg/m2 | 26.6 ± 3.5 | 26.8 ± 3.7 | 0.25 |
| Diabetes mellitus n, (%) | 298 (33.4) | 367 (27.1) | 0.0001 |
| Hypertension n, (%) | 668 (74.9) | 989 (73.2) | 0.36 |
| Dyslipidemia n, (%) | 628 (70.4) | 1002 (74.1) | 0.053 |
| Current smoking n, (%) | 147 (27.3) | 246 (28.6) | 0.84 |
| NYHA heart failure class n, (%) | 0.002 | ||
| I | 133 (15.7) | 257 (19.9) | |
| II | 523 (61.8) | 811 (62.9) | |
| III | 162 (19.2) | 175 (13.6) | |
| IV | 28 (3.3) | 46 (3.6) | |
| CAD severity | 0.23 | ||
| 1-Vessel coronary disease n, (%) | 102 (11.4) | 166 (12.3) | |
| 2-Vessel coronary disease n, (%) | 157 (17.6) | 272 (20.1) | |
| 3-Vessel coronary disease n, (%) | 633 (71.0) | 914 (67.6) | |
| Arteries with a stenosis ≥50% | |||
| Long common trunk n, (%) | 249 (27.9) | 351 (26) | 0.31 |
| Anterior interventricular artery n, (%) | 821 (92) | 1234 (91.3) | 0.52 |
| Circumflex artery n, (%) | 760 (85.2) | 1104 (81.7) | 0.03 |
| Right coronary artery n, (%) | 667 (74.8) | 1006 (74.4) | 0.84 |
| Left ventricular ejection fraction, % | 56.3 ± 10.6 | 57.9 ± 10.0 | 0.0008 |
| Previous myocardial infarction n, (%) | 364 (40.8) | 506 (37.4) | 0.11 |
| CPB n, (%) | 787 (88.2) | 1219 (90.2) | 0.15 |
| CPB time, minutes | 85.2 ± 41.4 | 90.8 ± 40.7 | 0.002 |
| Clamping time, min | 66.3 ± 22.6 | 70.3 ± 23.1 | 0.0002 |
| Number of transfused units per patients, (interquartile range) | 2 (0; 2) | 0 (0; 2) | <0.0001 |
| EuroSCORE II, (interquartile range) | 1.6 (0.9; 3) | 2.4 (1.3; 4.3) | <0.0001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poggio, P.; Cavallotti, L.; Myasoedova, V.A.; Bonomi, A.; Songia, P.; Gripari, P.; Valerio, V.; Amato, M.; Barbieri, S.; Faggiano, P.; et al. Aortic Valve Sclerosis Adds to Prediction of Short-Term Mortality in Patients with Documented Coronary Atherosclerosis. J. Clin. Med. 2019, 8, 1172. https://doi.org/10.3390/jcm8081172
Poggio P, Cavallotti L, Myasoedova VA, Bonomi A, Songia P, Gripari P, Valerio V, Amato M, Barbieri S, Faggiano P, et al. Aortic Valve Sclerosis Adds to Prediction of Short-Term Mortality in Patients with Documented Coronary Atherosclerosis. Journal of Clinical Medicine. 2019; 8(8):1172. https://doi.org/10.3390/jcm8081172
Chicago/Turabian StylePoggio, Paolo, Laura Cavallotti, Veronika A. Myasoedova, Alice Bonomi, Paola Songia, Paola Gripari, Vincenza Valerio, Mauro Amato, Simone Barbieri, Pompilio Faggiano, and et al. 2019. "Aortic Valve Sclerosis Adds to Prediction of Short-Term Mortality in Patients with Documented Coronary Atherosclerosis" Journal of Clinical Medicine 8, no. 8: 1172. https://doi.org/10.3390/jcm8081172