The Effect of Positive End-Expiratory Pressure on Lung Micromechanics Assessed by Synchrotron Radiation Computed Tomography in an Animal Model of ARDS

 , , ,
, , ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Experimental Setup
2.2. Synchrotron Radiation Computed Tomography
2.3. Study Protocol
2.4. Image Recording and Analysis
2.5. Data Analysis
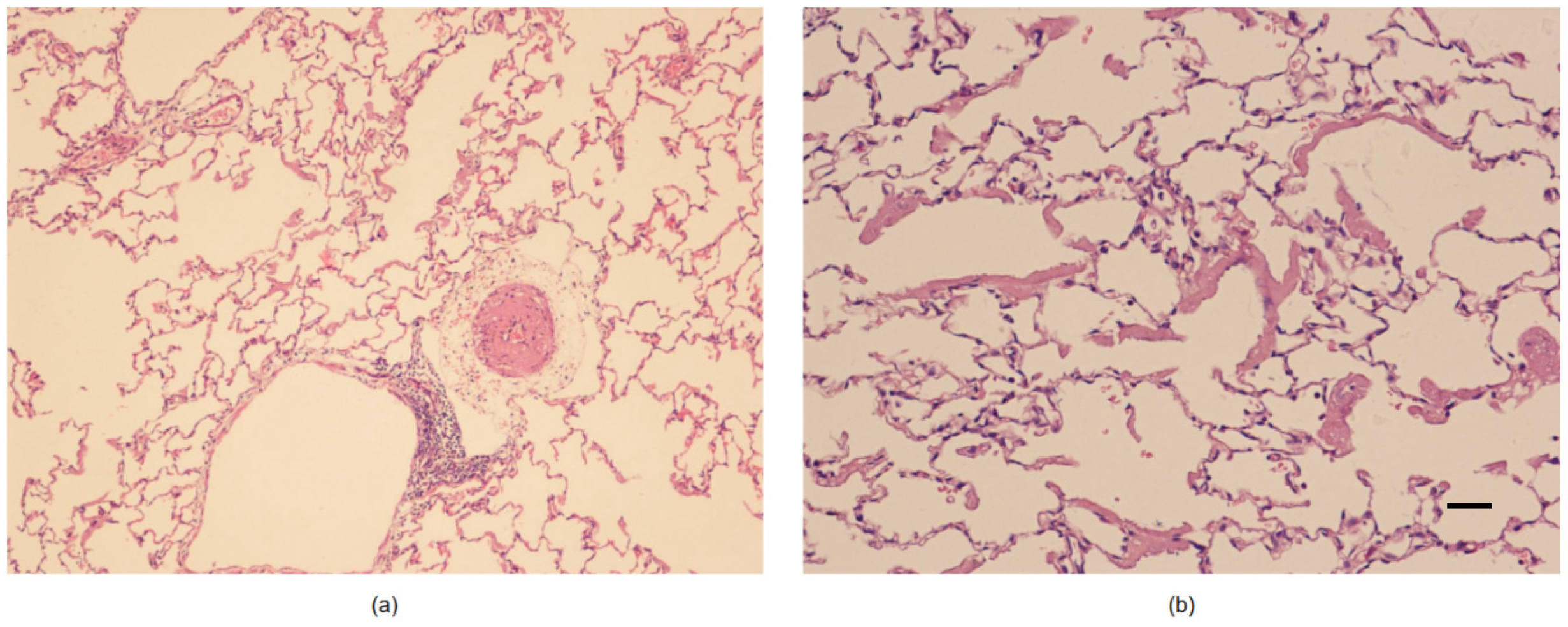
2.6. Histological Study
2.7. Statistical Analysis
3. Results
3.1. Airspaces Number and Dimension in the Whole Lung Slice
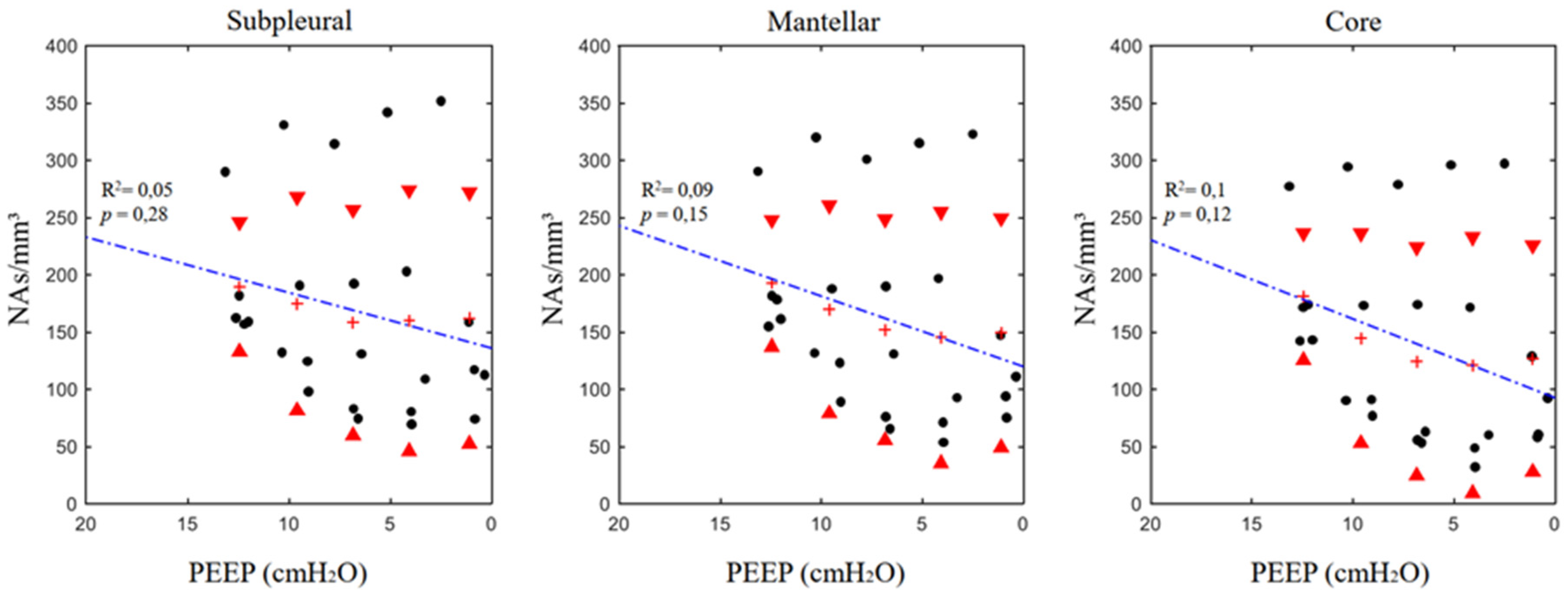
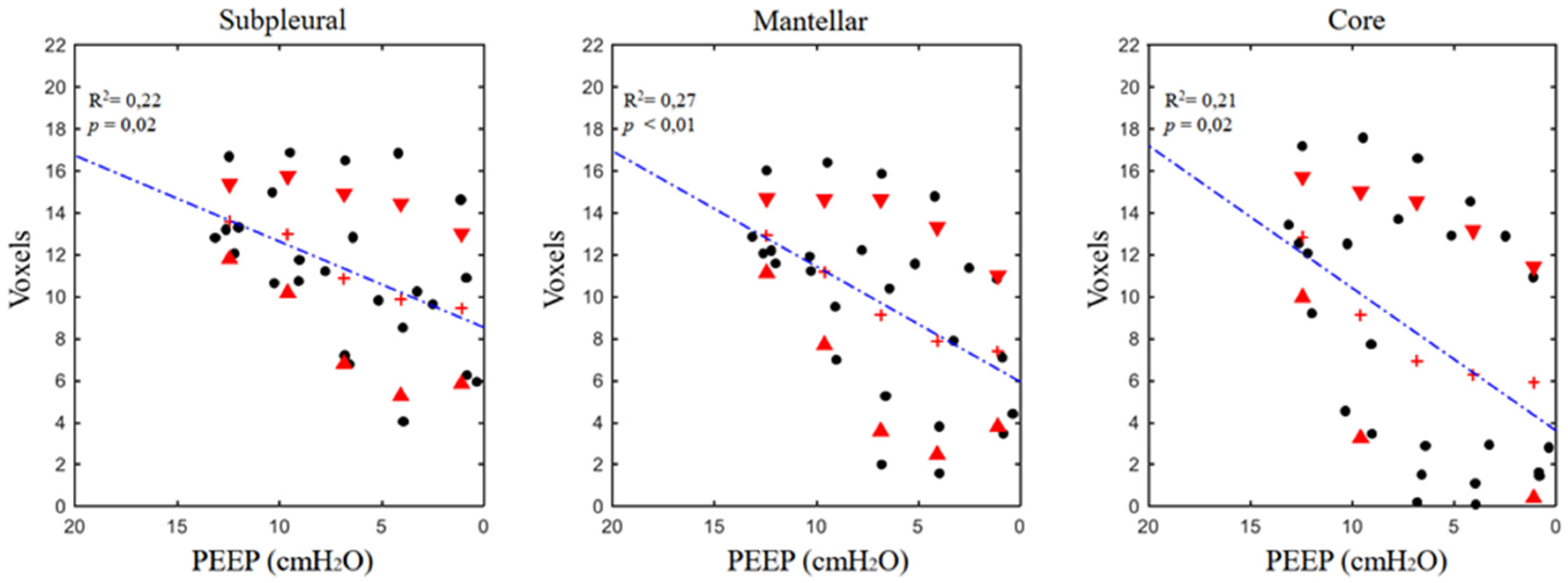
3.2. Airspaces Number and Dimension in the Three ROIs
4. Discussion
4.1. Number and Dimensional Variation in Experimental ARDS
4.2. Technical Aspects and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Slutsky, A.S.; Ranieri, V.M. Ventilator-induced lung injury. N. Engl. J. Med. 2013, 369, 2126–2136. [Google Scholar] [CrossRef] [PubMed]
- Ashbaugh, D.G.; Bigelow, D.B.; Petty, T.L.; Levine, B.E. Acute respiratory distress in adults. Lancet Lond. Engl. 1967, 2, 319–323. [Google Scholar] [CrossRef]
- Amato, M.B.; Barbas, C.S.; Medeiros, D.M.; Schettino Gde, P.; Lorenzi Filho, G.; Kairalla, R.A.; Deheinzelin, D.; Morais, C.; Fernandes Ede, O.; Takagaki, T.Y. Beneficial effects of the “open lung approach” with low distending pressures in acute respiratory distress syndrome. A prospective randomized study on mechanical ventilation. Am. J. Respir. Crit. Care Med. 1995, 152, 1835–1846. [Google Scholar] [CrossRef] [PubMed]
- Roupie, E.; Dambrosio, M.; Servillo, G.; Mentec, H.; el Atrous, S.; Beydon, L.; Brun-Buisson, C.; Lemaire, F.; Brochard, L. Titration of tidal volume and induced hypercapnia in acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 1995, 152, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Greaves, I.A.; Hildebrandt, J.; Hoppin, F.G. Micromechanics of the Lung. In Comprehensive Physiology; American Cancer Society: New York, NY, USA, 2011; pp. 217–231. ISBN 978-0-470-65071-4. [Google Scholar]
- Scaramuzzo, G.; Broche, L.; Pellegrini, M.; Porra, L.; Derosa, S.; Tannoia, A.P.; Marzullo, A.; Borges, J.B.; Bayat, S.; Bravin, A.; et al. Regional behavior of airspaces during positive pressure reduction assessed by synchrotron radiation computed tomography. Front. Physiol. 2019, 10, 719. [Google Scholar] [CrossRef] [PubMed]
- Perchiazzi, G.; Rylander, C.; Vena, A.; Derosa, S.; Polieri, D.; Fiore, T.; Giuliani, R.; Hedenstierna, G. Lung regional stress and strain as a function of posture and ventilatory mode. J. Appl. Physiol. 2011, 110, 1374–1383. [Google Scholar] [CrossRef] [Green Version]
- Perchiazzi, G.; Rylander, C.; Derosa, S.; Pellegrini, M.; Pitagora, L.; Polieri, D.; Vena, A.; Tannoia, A.; Fiore, T.; Hedenstierna, G. Regional distribution of lung compliance by image analysis of computed tomograms. Respir. Physiol. Neurobiol. 2014, 201, 60–70. [Google Scholar] [CrossRef]
- Kaczka, D.W.; Cao, K.; Christensen, G.E.; Bates, J.H.T.; Simon, B.A. Analysis of regional mechanics in canine lung injury using forced oscillations and 3D image registration. Ann. Biomed. Eng. 2011, 39, 1112–1124. [Google Scholar] [CrossRef]
- Schiller, H.J.; Steinberg, J.; Halter, J.; McCann, U.; DaSilva, M.; Gatto, L.A.; Carney, D.; Nieman, G. Alveolar inflation during generation of a quasi-static pressure/volume curve in the acutely injured lung. Crit. Care Med. 2003, 31, 1126–1133. [Google Scholar] [CrossRef]
- Gattinoni, L.; Quintel, M. How ARDS should be treated. Crit. Care Lond. Engl. 2016, 20, 86. [Google Scholar] [CrossRef]
- Otis, A.B.; Mckerrow, C.B.; Bartlett, R.A.; Mead, J.; Mcilroy, M.B.; Selver-Stone, N.J.; Radford, E.P. Mechanical factors in distribution of pulmonary ventilation. J. Appl. Physiol. 1956, 8, 427–443. [Google Scholar] [CrossRef]
- Al-Rawas, N.; Banner, M.J.; Euliano, N.R.; Tams, C.G.; Brown, J.; Martin, A.D.; Gabrielli, A. Expiratory time constant for determinations of plateau pressure, respiratory system compliance, and total resistance. Crit. Care Lond. Engl. 2013, 17, R23. [Google Scholar] [CrossRef]
- Guttmann, J.; Eberhard, L.; Fabry, B.; Bertschmann, W.; Zeravik, J.; Adolph, M.; Eckart, J.; Wolff, G. Time constant/volume relationship of passive expiration in mechanically ventilated ARDS patients. Eur. Respir. J. 1995, 8, 114–120. [Google Scholar] [CrossRef]
- Henderson, W.R.; Molgat-Seon, Y.; Dominelli, P.B.; Brasher, P.M.A.; Griesdale, D.E.G.; Foster, G.E.; Yacyshyn, A.; Ayas, N.T.; Sheel, A.W. Gas density alters expiratory time constants before and after experimental lung injury. Exp. Physiol. 2015, 100, 1217–1228. [Google Scholar] [CrossRef] [Green Version]
- Chiumello, D.; Carlesso, E.; Cadringher, P.; Caironi, P.; Valenza, F.; Polli, F.; Tallarini, F.; Cozzi, P.; Cressoni, M.; Colombo, A.; et al. Lung stress and strain during mechanical ventilation for acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2008, 178, 346–355. [Google Scholar] [CrossRef]
- Cressoni, M.; Cadringher, P.; Chiurazzi, C.; Amini, M.; Gallazzi, E.; Marino, A.; Brioni, M.; Carlesso, E.; Chiumello, D.; Quintel, M.; et al. Lung inhomogeneity in patients with acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2014, 189, 149–158. [Google Scholar] [CrossRef]
- Gattinoni, L.; Carlesso, E.; Caironi, P. Stress and strain within the lung. Curr. Opin. Crit. Care 2012, 18, 42–47. [Google Scholar] [CrossRef]
- Mead, J.; Takishima, T.; Leith, D. Stress distribution in lungs: A model of pulmonary elasticity. J. Appl. Physiol. 1970, 28, 596–608. [Google Scholar] [CrossRef]
- Pellegrini, M.; Derosa, S.; Tannoia, A.; Rylander, C.; Fiore, T.; Larsson, A.; Hedenstierna, G.; Perchiazzi, G. Effects of superimposed tissue weight on regional compliance of injured lungs. Respir. Physiol. Neurobiol. 2016, 228, 16–24. [Google Scholar] [CrossRef]
- Fredberg, J.J.; Kamm, R.D. Stress transmission in the lung: Pathways from organ to molecule. Annu. Rev. Physiol. 2006, 68, 507–541. [Google Scholar] [CrossRef]
- Gattinoni, L.; Caironi, P.; Pelosi, P.; Goodman, L.R. What has computed tomography taught us about the acute respiratory distress syndrome? Am. J. Respir. Crit. Care Med. 2001, 164, 1701–1711. [Google Scholar] [CrossRef]
- Hajari, A.J.; Yablonskiy, D.A.; Sukstanskii, A.L.; Quirk, J.D.; Conradi, M.S.; Woods, J.C. Morphometric changes in the human pulmonary acinus during inflation. J. Appl. Physiol. 2012, 112, 937–943. [Google Scholar] [CrossRef]
- Xin, Y.; Cereda, M.; Kadlecek, S.; Emami, K.; Hamedani, H.; Duncan, I.; Rajaei, J.; Hughes, L.; Meeder, N.; Naji, J.; et al. Hyperpolarized gas diffusion MRI of biphasic lung inflation in short- and long-term emphysema models. Am. J. Physiol. Lung Cell. Mol. Physiol. 2017, 313, L305–L312. [Google Scholar] [CrossRef]
- Salito, C.; Aliverti, A.; Rivolta, I.; Mazzuca, E.; Miserocchi, G. Alveolar mechanics studied by in vivo microscopy imaging through intact pleural space. Respir. Physiol. Neurobiol. 2014, 202, 44–49. [Google Scholar] [CrossRef]
- Carney, D.E.; Bredenberg, C.E.; Schiller, H.J.; Picone, A.L.; McCann, U.G.; Gatto, L.A.; Bailey, G.; Fillinger, M.; Nieman, G.F. The mechanism of lung volume change during mechanical ventilation. Am. J. Respir. Crit. Care Med. 1999, 160, 1697–1702. [Google Scholar] [CrossRef]
- Bravin, A.; Coan, P.; Suortti, P. X-ray phase-contrast imaging: From pre-clinical applications towards clinics. Phys. Med. Biol. 2013, 58, R1–R35. [Google Scholar] [CrossRef]
- Directive 2010/63/EU of the European Parliament and of the Council of 22 September 2010 on the Protection of Animals Used for Scientific Purposes. Text with EEA relevance. Off. J. Eur. Union 2010, 276, 33–79.
- Suortti, P.; Fiedler, S.; Bravin, A.; Brochard, T.; Mattenet, M.; Renier, M.; Spanne, P.; Thomlinson, W.; Charvet, A.M.; Elleaume, H.; et al. Fixed-exit monochromator for computed tomography with synchrotron radiation at energies 18–90 keV. J. Synchrotron Radiat. 2000, 7, 340–347. [Google Scholar] [CrossRef]
- Coan, P.; Peterzol, A.; Fiedler, S.; Ponchut, C.; Labiche, J.C.; Bravin, A. Evaluation of imaging performance of a taper optics CCD; FReLoN’ camera designed for medical imaging. J. Synchrotron Radiat. 2006, 13, 260–270. [Google Scholar] [CrossRef]
- Dougherty, E.R.; Lotufo, R.A. Gray scale morphology. In Hands-on Morphological Image Processing; SPIE Optical Engineering Press: Bellingham, WA, USA, 2003; ISBN 9780819447203. [Google Scholar]
- Bonferroni, C.E. Teoria Statistica Delle Classi e Calcolo Delle Probabilità; Libreria Internazionale Seeber: Firenze, Italia, 1936. [Google Scholar]
- Hickling, K.G. Best compliance during a decremental, but not incremental, positive end-expiratory pressure trial is related to open-lung positive end-expiratory pressure: A mathematical model of acute respiratory distress syndrome lungs. Am. J. Respir. Crit. Care Med. 2001, 163, 69–78. [Google Scholar] [CrossRef]
- Suki, B.; Barabási, A.L.; Hantos, Z.; Peták, F.; Stanley, H.E. Avalanches and power-law behaviour in lung inflation. Nature 1994, 368, 615–618. [Google Scholar] [CrossRef]
- Bachofen, H.; Hildebrandt, J.; Bachofen, M. Pressure-volume curves of air- and liquid-filled excised lungs-surface tension in situ. J. Appl. Physiol. 1970, 29, 422–431. [Google Scholar] [CrossRef]
- Albaiceta, G.M.; Taboada, F.; Parra, D.; Luyando, L.H.; Calvo, J.; Menendez, R.; Otero, J. Tomographic study of the inflection points of the pressure-volume curve in acute lung injury. Am. J. Respir. Crit. Care Med. 2004, 170, 1066–1072. [Google Scholar] [CrossRef]
- Scaramuzzo, G.; Spadaro, S.; Waldmann, A.D.; Böhm, S.H.; Ragazzi, R.; Marangoni, E.; Alvisi, V.; Spinelli, E.; Mauri, T.; Volta, C.A. Heterogeneity of regional inflection points from pressure-volume curves assessed by electrical impedance tomography. Crit. Care 2019, 23, 119. [Google Scholar] [CrossRef]
- Albert, S.P.; DiRocco, J.; Allen, G.B.; Bates, J.H.T.; Lafollette, R.; Kubiak, B.D.; Fischer, J.; Maroney, S.; Nieman, G.F. The role of time and pressure on alveolar recruitment. J. Appl. Physiol. 2009, 106, 757–765. [Google Scholar] [CrossRef] [Green Version]
- Otis, D.R.; Johnson, M.; Pedley, T.J.; Kamm, R.D. Role of pulmonary surfactant in airway closure: A computational study. J. Appl. Physiol. 1993, 75, 1323–1333. [Google Scholar] [CrossRef]
- Bates, J.H.T. A recruitment model of quasi-linear power-law stress adaptation in lung tissue. Ann. Biomed. Eng. 2007, 35, 1165–1174. [Google Scholar] [CrossRef]
- Gaver, D.P.; Samsel, R.W.; Solway, J. Effects of surface tension and viscosity on airway reopening. J. Appl. Physiol. 1990, 69, 74–85. [Google Scholar] [CrossRef]
- Broche, L.; Perchiazzi, G.; Porra, L.; Tannoia, A.; Pellegrini, M.; Derosa, S.; Sindaco, A.; Batista Borges, J.; Degrugilliers, L.; Larsson, A.; et al. Dynamic Mechanical Interactions Between Neighboring Airspaces Determine Cyclic Opening and Closure in Injured Lung. Crit. Care Med. 2017, 45, 687–694. [Google Scholar] [CrossRef] [Green Version]
- Gil, J.; Bachofen, H.; Gehr, P.; Weibel, E.R. Alveolar volume-surface area relation in air- and saline-filled lungs fixed by vascular perfusion. J. Appl. Physiol. 1979, 47, 990–1001. [Google Scholar] [CrossRef]
- Roan, E.; Waters, C.M. What do we know about mechanical strain in lung alveoli? Am. J. Physiol. Lung Cell. Mol. Physiol. 2011, 301, L625–L635. [Google Scholar] [CrossRef] [Green Version]
- Tsunoda, S.; Fukaya, H.; Sugihara, T.; Martin, C.J.; Hildebrandt, J. Lung volume, thickness of alveolar walls, and microscopic anisotropy of expansion. Respir. Physiol. 1974, 22, 285–296. [Google Scholar] [CrossRef]
- Matthay, M.A.; Ware, L.B.; Zimmerman, G.A. The acute respiratory distress syndrome. J. Clin. Investig. 2012, 122, 2731–2740. [Google Scholar] [CrossRef] [Green Version]
- Broche, L.; Pisa, P.; Porra, L.; Degrugilliers, L.; Bravin, A.; Pellegrini, M.; Borges, J.B.; Perchiazzi, G.; Larsson, A.; Hedenstierna, G.; et al. Individual airway closure characterized in vivo by phase-contrast CT imaging in injured rabbit lung. Crit. Care Med. 2019. Epub ahead of print. [Google Scholar] [CrossRef]
- D’Angelo, E. Local alveolar size and transpulmonary pressure in situ and in isolated lungs. Respir. Physiol. 1972, 14, 251–266. [Google Scholar] [CrossRef]
- Tenney, S.M.; Remmers, J.E. Comparative quantitative morphology of the mammalian lung: Diffusing area. Nature 1963, 197, 54–56. [Google Scholar] [CrossRef]
- Gattinoni, L.; Pelosi, P.; Vitale, G.; Pesenti, A.; D’Andrea, L.; Mascheroni, D. Body position changes redistribute lung computed-tomographic density in patients with acute respiratory failure. Anesthesiology 1991, 74, 15–23. [Google Scholar] [CrossRef]
- Pelosi, P.; D’Andrea, L.; Vitale, G.; Pesenti, A.; Gattinoni, L. Vertical gradient of regional lung inflation in adult respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 1994, 149, 8–13. [Google Scholar] [CrossRef]
- Smaldone, G.C.; Mitzner, W.; Itoh, H. Role of alveolar recruitment in lung inflation: Influence on pressure-volume hysteresis. J. Appl. Physiol. 1983, 55, 1321–1332. [Google Scholar] [CrossRef]
- Mead, R. The Non-Orthogonal Design of Experiments. J. R. Stat. Soc. Ser. A Stat. Soc. 1990, 153, 151–201. [Google Scholar] [CrossRef]
- Borges, J.B.; Costa, E.L.V.; Suarez-Sipmann, F.; Widström, C.; Larsson, A.; Amato, M.; Hedenstierna, G. Early inflammation mainly affects normally and poorly aerated lung in experimental ventilator-induced lung injury. Crit. Care Med. 2014, 42, e279–e287. [Google Scholar] [CrossRef]
- Suki, B.; Hubmayr, R. Epithelial and endothelial damage induced by mechanical ventilation modes. Curr. Opin. Crit. Care 2014, 20, 17–24. [Google Scholar] [CrossRef]
- John, J.; Taskar, V.; Evander, E.; Wollmer, P.; Jonson, B. Additive nature of distension and surfactant perturbation on alveolocapillary permeability. Eur. Respir. J. 1997, 10, 192–199. [Google Scholar] [CrossRef]
- Brower, R.G.; Lanken, P.N.; MacIntyre, N.; Matthay, M.A.; Morris, A.; Ancukiewicz, M.; Schoenfeld, D.; Thompson, B.T. Higher versus Lower Positive End-Expiratory Pressures in Patients with the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2004, 351, 327–336. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variable | PEEP 12 | PEEP 9 | PEEP 6 | PEEP 3 | ZEEP |
|---|---|---|---|---|---|
| VT (mL) | 33.1 ± 17.6 | 28.6 ± 10.9 | 23.4 ± 13 | 17.3 ± 10.7 | 19.9 ± 9.0 |
| Measured PEEP (cmH2O) | 12.4 ± 0.4 | 9.6 ± 0.6 | 6.8 ± 0.5 | 4.1 ± 0.7 | 1.1 ± 0.8 |
| Ppeakrs (cmH2O) | 33.9 ± 5.7 | 32.7 ± 8.5 | 33.4 ± 11.1 | 34.1 ± 11.0 | 40.1 ± 7.7 |
| Pplatrs (cmH2O) | 31.5 ± 6 | 29.9 ± 8.4 | 29.8 ± 9.8 | 31.7 ± 11.0 | 36.3 ± 7.3 |
| Driving Pressure (cmH2O) | 21.4 ± 5.8 | 23.1 ± 8.6 | 26.6 ± 11.0 | 30.0 ± 10.9 | 39.0 ± 7.6 |
| Crs (mL/cmH2O) | 1.6 ± 0.8 | 1.4 ± 0.8 | 1.1 ± 0.7 | 0.7 ± 0.6 | 0.5 ± 0.3 |
| Parameters of Linear Regression | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ROI | PEEP 12 | PEEP 9 | PEEP 6 | PEEP 3 | PEEP 0 | m | k | R2 | p | ||
| Entire slice | ASdim (voxel) | ALL | 13.1 ± 2.2 | 11.1 ± 4.3 | 9 ± 5.7 | 8 ± 5.5 | 7.6 ± 4.3 | 0.55 | 6.03 | 0.21 | <0.01 (*) |
| ASnum (n/mm3) | ALL | 188 ± 52.0 | 163.2 ± 86.3 | 145.2 ± 92.3 | 142.4 ± 104.9 | 146.4 ± 96.7 | 5.96 | 116.41 | 0.08 | 0.02 (*) | |
| Regional analysis | ASdim (voxel) | SUB | 13.6 ± 1.8 | 13 ± 2.8 | 10.9 ± 4.1 | 9.9 ± 4.6 | 9.4 ± 3.6 | 0.41 | 8.54 | 0.22 | 0.02 (*) |
| MAN | 12.9 ± 1.8 | 11.2 ± 3.5 | 9.1 ± 5.5 | 7.9 ± 5.4 | 7.4 ± 3.6 | 0.55 | 5.95 | 0.27 | <0.01 (*) | ||
| COR | 12.9 ± 2.9 | 9.1 ± 5.9 | 6.9 ± 7.6 | 6.3 ± 6.9 | 5.9 ± 5.5 | 0.68 | 3.61 | 0.21 | 0.02 (*) | ||
| ASnum (n/mm3) | SUB | 189.7 ± 56.7 | 174.9 ± 93.3 | 158.7 ± 98.6 | 160.4 ± 114.1 | 162.5 ± 109.8 | 4.85 | 136.21 | 0.05 | 0.28 | |
| MAN | 193.0 ± 55.5 | 167.0 ± 90.9 | 152.3 ± 96.6 | 145.6 ± 109.7 | 149.7 ± 100.2 | 6.15 | 120.16 | 0.09 | 0.15 | ||
| COR | 181.2 ± 55.5 | 144.7 ± 91.7 | 124.6 ± 99.8 | 121.3 ± 111.7 | 127.1 ± 99.1 | 6.89 | 92.86 | 0.10 | 0.12 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scaramuzzo, G.; Broche, L.; Pellegrini, M.; Porra, L.; Derosa, S.; Tannoia, A.P.; Marzullo, A.; Borges, J.B.; Bayat, S.; Bravin, A.; et al. The Effect of Positive End-Expiratory Pressure on Lung Micromechanics Assessed by Synchrotron Radiation Computed Tomography in an Animal Model of ARDS. J. Clin. Med. 2019, 8, 1117. https://doi.org/10.3390/jcm8081117
Scaramuzzo G, Broche L, Pellegrini M, Porra L, Derosa S, Tannoia AP, Marzullo A, Borges JB, Bayat S, Bravin A, et al. The Effect of Positive End-Expiratory Pressure on Lung Micromechanics Assessed by Synchrotron Radiation Computed Tomography in an Animal Model of ARDS. Journal of Clinical Medicine. 2019; 8(8):1117. https://doi.org/10.3390/jcm8081117
Chicago/Turabian StyleScaramuzzo, Gaetano, Ludovic Broche, Mariangela Pellegrini, Liisa Porra, Savino Derosa, Angela Principia Tannoia, Andrea Marzullo, João Batista Borges, Sam Bayat, Alberto Bravin, and et al. 2019. "The Effect of Positive End-Expiratory Pressure on Lung Micromechanics Assessed by Synchrotron Radiation Computed Tomography in an Animal Model of ARDS" Journal of Clinical Medicine 8, no. 8: 1117. https://doi.org/10.3390/jcm8081117