The Impact of Metabolic Syndrome on the Incidence of Atrial Fibrillation: A Nationwide Longitudinal Cohort Study in South Korea

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
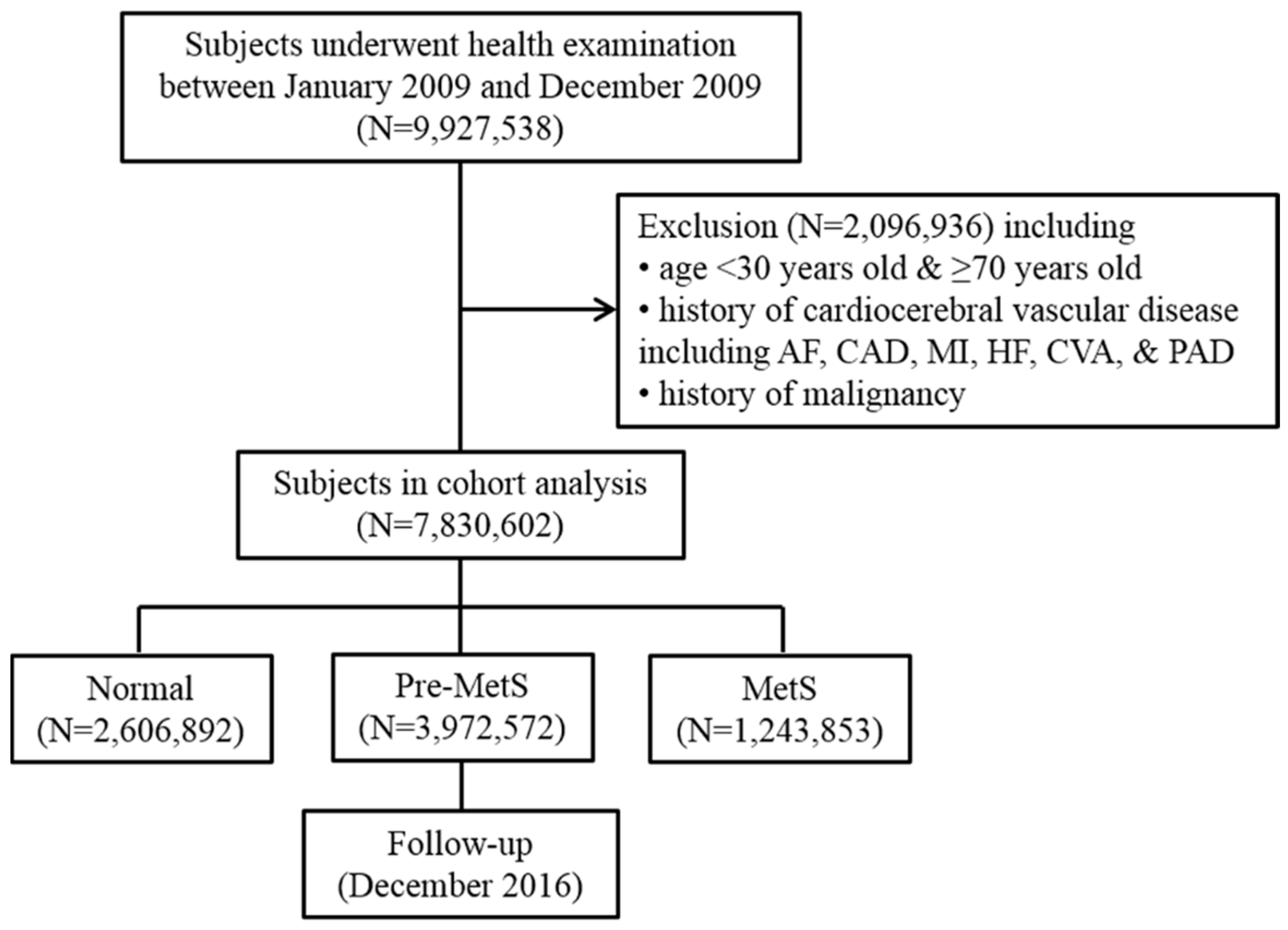
2.1. Study Population
2.2. Definition of Metabolic Syndrome
2.3. Definition of Primary Outcome
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Association between MetS Status and AF Risk
3.3. Impact of MetS Status and Components on the Risk of AF
4. Discussion
4.1. Comparison to Previous Studies
4.2. MetS and AF
4.3. Clinical Implications
4.4. Limitations
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Benjamin, E.J.; Wolf, P.A.; D’Agostino, R.B.; Silbershatz, H.; Kannel, W.B.; Levy, D. Impact of Atrial Fibrillation on the Risk of Death: The Framingham Heart Study. Circulation 1998, 98, 946–952. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.; Hart, C.L.; Hole, D.J.; McMurray, J.J. A Population-based Study of the Long-Term Risks Associated with Atrial Fibrillation: 20-Year Follow-up of the Renfrew/Paisley Study. Am. J. Med. 2002, 113, 359–364. [Google Scholar] [CrossRef]
- Krahn, A.D.; Manfreda, J.; Tate, R.B.; Mathewson, F.A.; Cuddy, T.E. The Natural History of Atrial Fibrillation: Incidence, Risk Factors, and Prognosis in the Manitoba Follow-up Study. Am. J. Med. 1995, 98, 476–484. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Levy, D.; Vaziri, S.M.; D’Agostino, R.B.; Belanger, A.J.; Wolf, P.A. Independent Risk Factors for Atrial Fibrillation in a Population-Based Cohort. The Framingham Heart Study. JAMA 1994, 271, 840–844. [Google Scholar] [CrossRef] [PubMed]
- Frost, L.; Hune, L.J.; Vestergaard, P. Overweight and obesity as risk factors for atrial fibrillation or Flutter: The danish diet, cancer, and health study. Am. J. Med. 2005, 118, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Gami, A.S.; Hodge, D.O.; Herges, R.M.; Olson, E.J.; Nykodym, J.; Kara, T.; Somers, V.K. Obstructive Sleep Apnea, Obesity, and the Risk of Incident Atrial Fibrillation. J. Am. Coll. Cardiol. 2007, 49, 565–571. [Google Scholar] [CrossRef] [Green Version]
- Kodama, S.; Saito, K.; Tanaka, S.; Horikawa, C.; Saito, A.; Heianza, Y.; Anasako, Y.; Nishigaki, Y.; Yachi, Y.; Iida, K.T.; et al. Alcohol Consumption and Risk of Atrial Fibrillation: A Meta-Analysis. J. Am. Coll. Cardiol. 2011, 57, 427–436. [Google Scholar] [CrossRef] [Green Version]
- Sawin, C.T.; Geller, A.; Wolf, P.A.; Belanger, A.J.; Baker, E.; Bacharach, P.; Wilson, P.W.; Benjamin, E.J.; D’Agostino, R.B. Low Serum Thyrotropin Concentrations as a Risk Factor for Atrial Fibrillation in Older Persons. N. Engl. J. Med. 1994, 331, 1249–1252. [Google Scholar] [CrossRef]
- Severino, P.; Mariani, M.V.; Maraone, A.; Piro, A.; Ceccacci, A.; Tarsitani, L.; Maestrini, V.; Mancone, M.; Lavalle, C.; Pasquini, M.; et al. Triggers for Atrial Fibrillation: The Role of Anxiety. Cardiol. Res. Pract. 2019, 2019, 1208505. [Google Scholar] [CrossRef]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and Management of the Metabolic Syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Zimmet, P.; Shaw, J.; IDF Epidemiology Task Force Consensus Group. The Metabolic Syndrome—A New Worldwide Definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Watanabe, H.; Tanabe, N.; Watanabe, T.; Darbar, D.; Roden, D.M.; Sasaki, S.; Aizawa, Y. Metabolic Syndrome and Risk of development of Atrial Fibrillation: The Niigata Preventive Medicine Study. Circulation 2008, 117, 1255–1260. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, A.M.; Agarwal, S.K.; Ambrose, M.; Folsom, A.R.; Soliman, E.Z.; Alonso, A. Metabolic Syndrome and Incidence of Atrial Fibrillation among Blacks and Whites in the Atherosclerosis Risk in Communities (ARIC) Study. Am. Heart J. 2010, 159, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Nystrom, P.K.; Carlsson, A.C.; Leander, K.; de Faire, U.; Hellenius, M.L.; Gigante, B. Obesity, Metabolic Syndrome and Risk of Atrial Fibrillation: A Swedish, Prospective Cohort Study. PLoS ONE 2015, 10, e0127111. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.G.; Choi, K.J.; Han, S.; Hwang, K.W.; Kwon, C.H.; Park, G.M.; Won, K.B.; Ann, S.H.; Kim, J.; Kim, S.J.; et al. Metabolic Syndrome and the Risk of New-Onset Atrial Fibrillation in Middle-Aged East Asian Men. Circ. J. 2018, 82, 1763–1769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheol Seong, S.; Kim, Y.Y.; Khang, Y.H.; Heon Park, J.; Kang, H.J.; Lee, H.; Do, C.H.; Song, J.S.; Hyon Bang, J.; Ha, S.; et al. Data Resource Profile: The National Health Information Database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2017, 46, 799–800. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Shin, H.; Song, J.H.; Kwak, S.H.; Kang, S.M.; Won Yoon, J.; Choi, S.H.; Cho, S.I.; Park, K.S.; Lee, H.K.; et al. Increasing Prevalence of Metabolic Syndrome in Korea: The Korean National Health and Nutrition Examination Survey for 1998–2007. Diabetes Care 2011, 34, 1323–1328. [Google Scholar] [CrossRef]
- Tanner, R.M.; Baber, U.; Carson, A.P.; Voeks, J.; Brown, T.M.; Soliman, E.Z.; Howard, V.J.; Muntner, P. Association of the Metabolic Syndrome with Atrial Fibrillation among United States Adults (from the REasons for Geographic and Racial Differences in Stroke [REGARDS] Study). Am. J. Cardiol. 2011, 108, 227–232. [Google Scholar] [CrossRef]
- Lee, S.S.; Ae Kong, K.; Kim, D.; Lim, Y.M.; Yang, P.S.; Yi, J.E.; Kim, M.; Kwon, K.; Bum Pyun, W.; Joung, B.; et al. Clinical Implication of an Impaired Fasting Glucose and Prehypertension Related to New Onset Atrial Fibrillation in a Healthy Asian Population without Underlying Disease: A Nationwide Cohort Study in Korea. Eur. Heart. J. 2017, 38, 2599–2607. [Google Scholar] [CrossRef] [PubMed]
- Baek, Y.S.; Yang, P.S.; Kim, T.H.; Uhm, J.S.; Park, J.; Pak, H.N.; Lee, M.H.; Joung, B. Associations of Abdominal Obesity and New-Onset Atrial Fibrillation in the General Population. J. Am. Heart Assoc. 2017, 6, e004705. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Parise, H.; Levy, D.; D’Agostino, R.B., Sr.; Wolf, P.A.; Vasan, R.S.; Benjamin, E.J. Obesity and the Risk of New-Onset Atrial Fibrillation. JAMA 2004, 292, 2471–2477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayer, J.G.; Almafragy, H.S.; Patel, A.A.; Hellyer, R.L.; Celermajer, D.S. Body Mass Index Is an Independent Determinant of Left Atrial Size. Heart Lung Circ. 2008, 17, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Zhang, F.; Xhen, J.; Chen, X.; Fu, F.; Tang, M.; Chen, L. P-Wave Dispersion and Maximum Duration Are Independently Associated with Insulin Resistance in Metabolic Syndrome. Ann. Endocrinol. (Paris) 2014, 75, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Abed, H.S.; Samuel, C.S.; Lau, D.H.; Kelly, D.J.; Royce, S.G.; Alasady, M.; Mahajan, R.; Kuklik, P.; Zhang, Y.; Brooks, A.G.; et al. Obesity Results in Progressive Atrial Structural and Electrical Remodeling: Implications for Atrial Fibrillation. Heart Rhythm 2013, 10, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Munger, T.M.; Dong, Y.X.; Masaki, M.; Oh, J.K.; Mankad, S.V.; Borlaug, B.A.; Asirvatham, S.J.; Shen, W.K.; Lee, H.C.; Bielinski, S.J.; et al. Electrophysiological and Hemodynamic Characteristics Associated with Obesity in Patients with Atrial Fibrillation. J. Am. Coll. Cardiol. 2012, 60, 851–860. [Google Scholar] [CrossRef]
- Yasar, A.S.; Bilen, E.; Bilge, M.; Ipek, G.; Ipek, E.; Kirbas, O. P-Wave Duration and Dispersion in Patients with Metabolic Syndrome. Pacing Clin. Electrophysiol. 2009, 32, 1168–1172. [Google Scholar] [CrossRef]
- Dandona, P.; Aljada, A.; Chaudhuri, A.; Mohanty, P.; Garg, R. Metabolic Syndrome: A Comprehensive Perspective Based on Interactions between Obesity, Diabetes, and Inflammation. Circulation 2005, 111, 1448–1454. [Google Scholar] [CrossRef]
- Visser, M.; Bouter, L.M.; McQuillan, G.M.; Wener, M.H.; Harris, T.B. Elevated C-Reactive Protein Levels in Overweight and Obese Adults. JAMA 1999, 282, 2131–2135. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Lip, G.Y.; Apostolakis, S. Inflammation in Atrial Fibrillation. J. Am. Coll. Cardiol. 2012, 60, 2263–2270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarzani, R.; Salvi, F.; Dessi-Fulgheri, P.; Rappelli, A. Renin-Angiotensin System, Natriuretic Peptides, Obesity, Metabolic Syndrome, and Hypertension: An Integrated View in Humans. J. Hypertens. 2008, 26, 831–843. [Google Scholar] [CrossRef] [PubMed]
- Dinh, W.; Lankisch, M.; Nickl, W.; Scheyer, D.; Scheffold, T.; Kramer, F.; Krahn, T.; Klein, R.M.; Barroso, M.C.; Futh, R. Insulin Resistance and Glycemic Abnormalities are Associated with Deterioration of Left Ventricular Diastolic Function: A Cross-Sectional Study. Cardiovasc. Diabetol. 2010, 9, 63. [Google Scholar] [CrossRef] [PubMed]
- Kravariti, M.; Naka, K.K.; Kalantaridou, S.N.; Kazakos, N.; Katsouras, C.S.; Makrigiannakis, A.; Paraskevaidis, E.A.; Chrousos, G.P.; Tsatsoulis, A.; Michalis, L.K. Predictors of Endothelial Dysfunction in Young Women with Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2005, 90, 5088–5095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aljada, A.; Ghanim, H.; Mohanty, P.; Kapur, N.; Dandona, P. Insulin Inhibits the Pro-Inflammatory Transcription Factor Early Growth Response Gene-1 (Egr)-1 Expression in Mononuclear Cells (MNC) and Reduces Plasma Tissue Factor (TF) and Plasminogen Activator Inhibitor-1 (PAI-1) Concentrations. J. Clin. Endocrinol. Metab. 2002, 87, 1419–1422. [Google Scholar] [CrossRef] [PubMed]
- Dandona, P.; Aljada, A.; Mohanty, P.; Ghanim, H.; Hamouda, W.; Assian, E.; Ahmad, S. Insulin Inhibits Intranuclear Nuclear Factor KappaB and Stimulates IkappaB in Mononuclear Cells in Obese Subjects: Evidence for an Anti-Inflammatory Effect? J. Clin. Endocrinol. Metab. 2001, 86, 3257–3265. [Google Scholar] [CrossRef]
- Grassi, G.; Dell’Oro, R.; Quarti-Trevano, F.; Scopelliti, F.; Seravalle, G.; Paleari, F.; Gamba, P.L.; Mancia, G. Neuroadrenergic and Reflex Abnormalities in Patients with Metabolic Syndrome. Diabetologia 2005, 48, 1359–1365. [Google Scholar] [CrossRef]
- Yamagishi, S.I.; Matsui, T.; Nakamura, K. Possible Molecular Mechanisms by Which Angiotensin II Type 1 Receptor Blockers (ARBs) Prevent the Development of Atrial Fibrillation in Insulin Resistant Patients. Horm. Metab. Res. 2008, 40, 640–644. [Google Scholar] [CrossRef]
- Vaziri, S.M.; Larson, M.G.; Lauer, M.S.; Benjamin, E.J.; Levy, D. Influence of Blood Pressure on Left Atrial Size. The Framingham Heart Study. Hypertension 1995, 25, 1155–1160. [Google Scholar] [CrossRef]
- Aronis, K.N.; Wang, N.; Phillips, C.L.; Benjamin, E.J.; Marcus, G.M.; Newman, A.B.; Rodondi, N.; Satterfield, S.; Harris, T.B.; Magnani, J.W.; et al. Associations of Obesity and Body Fat Distribution with Incident Atrial Fibrillation in the Biracial Health Aging and Body Composition Cohort of Older Adults. Am. Heart J. 2015, 170, 498–505. [Google Scholar] [CrossRef]
- Pathak, R.K.; Middeldorp, M.E.; Lau, D.H.; Mehta, A.B.; Mahajan, R.; Twomey, D.; Alasady, M.; Hanley, L.; Antic, N.A.; McEvoy, R.D.; et al. Aggressive Risk Factor Reduction Study for Atrial Fibrillation and Implications for the Outcome of Ablation: The ARREST-AF Cohort Study. J. Am. Coll. Cardiol. 2014, 64, 2222–2231. [Google Scholar] [CrossRef] [PubMed]
- Pathak, R.K.; Middeldorp, M.E.; Meredith, M.; Mehta, A.B.; Mahajan, R.; Wong, C.X.; Twomey, D.; Elliott, A.D.; Kalman, J.M.; Abhayaratna, W.P.; et al. Long-Term Effect of Goal-Directed Weight Management in an Atrial Fibrillation Cohort: A Long-Term Follow-Up Study (LEGACY). J. Am. Coll. Cardiol. 2015, 65, 2159–2169. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Normal N = 2,606,892 (33.3%) | Pre-MetS N = 3,972,572 (50.7%) | MetS N = 1,251,138 (15.9%) | p-Value |
|---|---|---|---|---|
| Age (years) at baseline | <0.001 | |||
| 30–39 | 796,857 (52.7) | 624,638 (41.3) | 91,002 (6.0) | |
| 40–49 | 769,361 (35.5) | 1,090,078 (50.4) | 304,487 (14.1) | |
| 50–59 | 705,192 (29.3) | 1,285,531 (53.4) | 418,382 (17.4) | |
| 60–69 | 335,482 (19.3) | 970,325 (55.7) | 437,267 (25.2) | |
| Sex | <0.001 | |||
| Male | 1,139,011 (25.6) | 2,415,161 (54.3) | 892,010 (20.1) | |
| Female | 1,467,881 (43.4) | 1,557,411 (46.0) | 359,128 (10.6) | |
| Smoking status | <0.001 | |||
| Non-smoker | 1,727,253 (39.1) | 2,134,365 (48.3) | 553,548 (12.5) | |
| Ex-smoker | 264,442 (24.7) | 581,953 (54.2) | 226,601 (21.1.) | |
| Current smoker | 597,385 (26.0) | 1,233,704 (53.8) | 463,565 (20.2.) | |
| Alcohol consumption | <0.001 | |||
| No drink | 1,260,556 (36.0) | 1,745,471 (49.8) | 497,220 (14.2.) | |
| 2–3 per month | 1,080,613 (33.9) | 1,611,254 (50.5) | 497,186 (15.6.) | |
| 1–4 per week | 538,841 (34.1) | 795,190 (50.2) | 248,610 (15.7) | |
| ≥5 per week | 45,971 (18.7) | 135,990 (55.4) | 63,366 (25.8) | |
| Exercise | ||||
| No exercise | 1,216,659 (33.9) | 1,803,595 (50.2) | 569,220 (15.9) | |
| 1–4 per week | 538,841 (34.1) | 795,190 (50.2) | 248,610 (15.7) | |
| ≥5 per week | 828,890 (31.9) | 1,342,260 (51.7) | 423,684 (16.3) | |
| Family history of HTN | <0.001 | |||
| Yes | 231,065 (28.0) | 42,583 (51.5) | 169,292 (20.5) | |
| No | 1,533,367 (34.1) | 2,271,217 (50.5) | 691,741 (15.4) | |
| Family history of DM | <0.001 | |||
| Yes | 206,381 (29.1) | 358,590 (50.5) | 144,595 (20.4) | |
| No | 1,566,796 (33.8) | 2,353,078 (50.7) | 720,945 (15.5) | |
| Family history of stroke | <0.001 | |||
| Yes | 115,766 (27.4) | 224,443 (53.1) | 82,800 (19.6) | |
| No | 1,656,733 (33.6) | 2,486,810 (50.5) | 792,319 (15.9) | |
| Family history of coronary heart disease | <0.001 | |||
| Yes | 80,356 (31.4) | 131,259 (51.3) | 44,348 (17.3) | |
| No | 1,691,243 (33.2) | 2,577,805 (50.7) | 819,893 (16.1) |
| Sex | MetS Status | Age Groups (Years) | |||
|---|---|---|---|---|---|
| 30–39 | 40–49 | 50–59 | 60–69 | ||
| Male | Normal | 5.03 | 12.32 | 34.40 | 85.99 |
| Pre-MetS | 6.20 | 17.31 | 51.48 | 122.95 | |
| MetS | 10.83 | 25.56 | 71.09 | 169.9 | |
| p-value * | <0.001 | <0.001 | <0.001 | <0.001 | |
| Female | No MetS | 1.21 | 4.04 | 11.65 | 34.07 |
| Pre-MetS | 2.18 | 7.19 | 18.24 | 54.22 | |
| MetS | 3.25 | 8.69 | 32.05 | 84.08 | |
| p-value * | >0.05 | <0.01 | <0.001 | <0.001 | |
| Non-Adjusted HR (95% CI) | Multivariable HR * (95% CI) | |||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | ||
| MetS status | ||||
| Normal | 1 | 1 | 1 | 1 |
| Pre-MetS | 2.43 (2.313–2.554) | 1.538 (1.463–1.617) | 1.532 (1.457–1.611) | 1.391 (1.322–1.464) |
| MetS | 4.616 (4.379–4.866) | 2.219 (2.103–2.343) | 2.205 (2.089–2.328) | 1.722 (1.621–1.829) |
| Sex | ||||
| Female | 1 | 1 | 1 | |
| Male | 2.332 (2.222–2.446) | 2.358 (2.247–2.475) | 1.969 (1.86–2.085) | |
| Age group | ||||
| 30–39 | 1 | 1 | 1 | |
| 40–49 | 2.62 (2.327–2.95) | 2.596 (2.305–2.923) | 2.613 (2.319–2.944) | |
| 50–59 | 7.36 (6.58–8.233) | 7.227 (6.461–8.085) | 7.553 (6.748–8.455) | |
| 60–69 | 18.571 (16.622–20.747) | 18.258 (16.341–20.4) | 19.523 (17.46–21.83) | |
| Smoking status | ||||
| Non-smoker | 1 | 1 | 1 | |
| Ex-smoker | 1.051 (1.0–1.105) | 1.04 (0.99–1.094) | 1.047 (0.996–1.101) | |
| Current smoker | 1.017 (0.971–1.065) | 1.014 (0.969–1.062) | 1.034 (0.987–1.083) | |
| Exercise | ||||
| No exercise | 1 | 1 | 1 | |
| 1–4 per week | 0.949 (0.906–0.994) | 0.945 (0.902–0.99) | 0.943 (0.9–0.987) | |
| ≥5 per week | 1.009 (0.972–1.047) | 1.003 (0.996–1.041) | 0.99 (0.954–1.028) | |
| Family history of HTN | ||||
| No | 1 | 1 | ||
| Yes | 1.14 (1.09–1.193) | 1.129 (1.079–1.181) | ||
| Family history of stroke | ||||
| No | 1 | 1 | ||
| Yes | 1.139 (1.081–1.201) | 1.145 (1.086–1.208) | ||
| Family history of coronary heart disease | ||||
| No | 1 | 1 | ||
| Yes | 1.259 (1.173–1.352) | 1.262 (1.175–1.356) | ||
| Family history of DM | ||||
| No | 1 | 1 | ||
| Yes | 0.889 (0.844–0.937) | 0.887 (0.841–0.935) | ||
| Body mass index (kg/m2) | 1.069 (1.062–1.075) | |||
| Hemoglobin (g/dL) | 1.082 (1.066–1.099) | |||
| Creatinine (mg/dL) | 1.002 (0.992–1.012) | |||
| Total cholesterol (mg/dL) | 0.997 (0.997–0.998) | |||
| LDL cholesterol (mg/dL) | 1.0 (0.999–1.001) | |||
| ALT (IU/L) | 0.999 (0.998–1.0) | |||
| Multivariable HR * (95% CI) | p-Value | |
|---|---|---|
| Abdominal obesity | 1.316 (1.256–1.379) | <0.0001 |
| Elevated blood pressure | 1.451 (1.4–1.505) | <0.0001 |
| Elevated fasting glucose | 1.163 (1.123–1.205) | <0.0001 |
| High triglyceride | 0.944 (0.907–0.984) | 0.006 |
| Low HDL cholesterol | 1.048 (1.003–1.096) | 0.038 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, C.H.; Kim, H.; Kim, S.H.; Kim, B.S.; Kim, H.-J.; Sung, J.D.; Kim, D.-K.; Han, S.W.; Ryu, K.-H. The Impact of Metabolic Syndrome on the Incidence of Atrial Fibrillation: A Nationwide Longitudinal Cohort Study in South Korea. J. Clin. Med. 2019, 8, 1095. https://doi.org/10.3390/jcm8081095
Kwon CH, Kim H, Kim SH, Kim BS, Kim H-J, Sung JD, Kim D-K, Han SW, Ryu K-H. The Impact of Metabolic Syndrome on the Incidence of Atrial Fibrillation: A Nationwide Longitudinal Cohort Study in South Korea. Journal of Clinical Medicine. 2019; 8(8):1095. https://doi.org/10.3390/jcm8081095
Chicago/Turabian StyleKwon, Chang Hee, Hyeongsu Kim, Sung Hea Kim, Bum Sung Kim, Hyun-Joong Kim, Ji Dong Sung, Duk-Kyung Kim, Seong Woo Han, and Kyu-Hyung Ryu. 2019. "The Impact of Metabolic Syndrome on the Incidence of Atrial Fibrillation: A Nationwide Longitudinal Cohort Study in South Korea" Journal of Clinical Medicine 8, no. 8: 1095. https://doi.org/10.3390/jcm8081095