Body Weight Fluctuation as a Risk Factor for Type 2 Diabetes: Results from a Nationwide Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Source of Data and Study Population
2.2. Body Weight Variability and Weight Change Status
2.3. Definition of Incident Type 2 Diabetes
2.4. Covariate Measurements
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Risk of New-Onset Diabetes According to Body Weight Fluctuation
3.3. Subgroup Analysis of the Risk of New-Onset Diabetes for Large Body-Weight Fluctuations
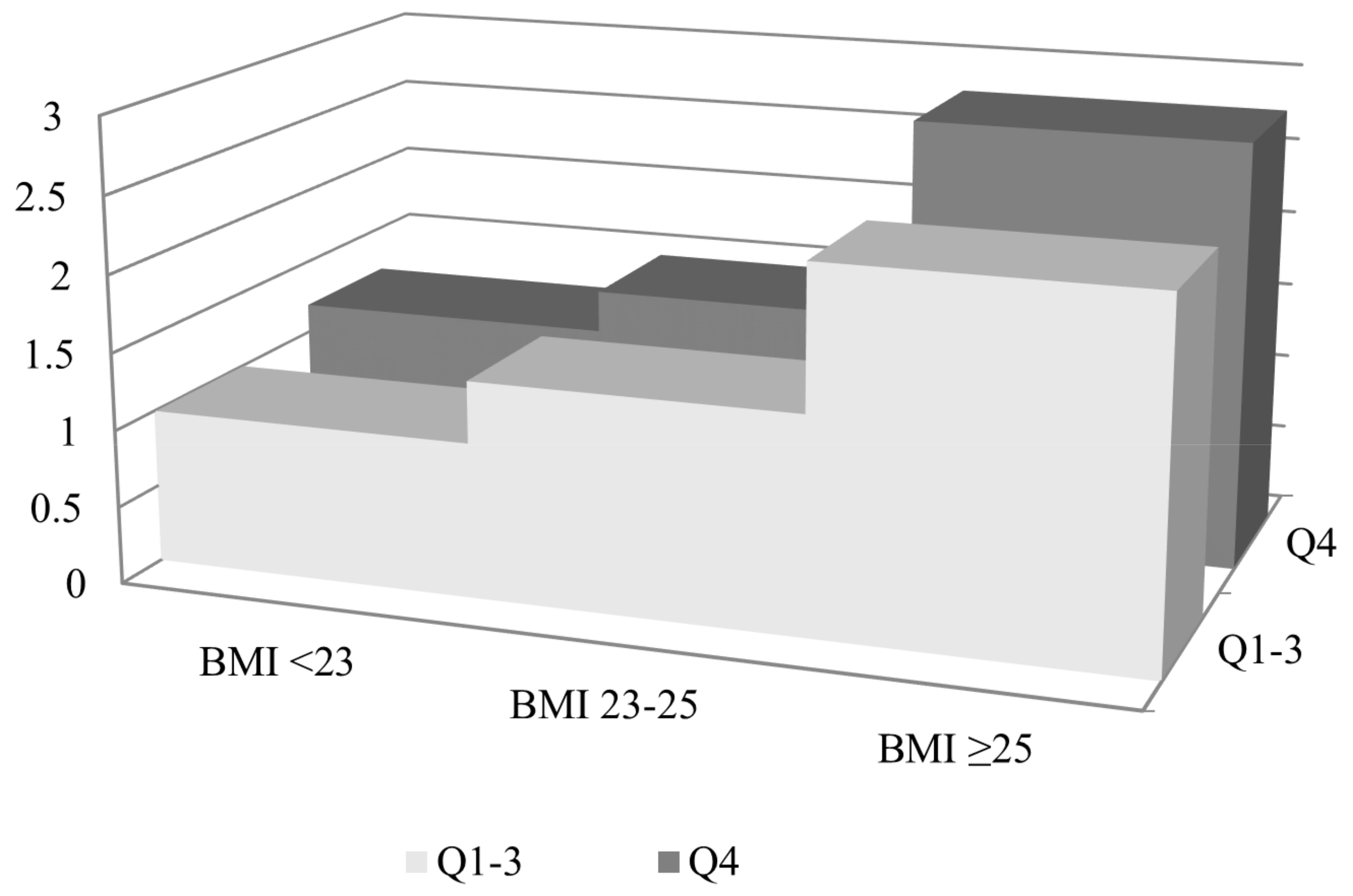
3.4. Risk of New-Onset Diabetes According to Baseline Obesity Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Morris, R.D.; Rimm, A.A. Long-term weight fluctuation and non-insulin-dependent diabetes mellitus in white women. Ann. Epidemiol. 1992, 2, 657–664. [Google Scholar] [CrossRef]
- Schotte, D.E.; Cohen, E.; Singh, S.P. Effects of weight cycling on metabolic control in male outpatients with non-insulin-dependent diabetes mellitus. Health Psychol. 1990, 9, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Lissner, L.; Odell, P.M.; D’Agostino, R.B.; Stokes, J., III; Kreger, B.E.; Belanger, A.J.; Brownell, K.D. Variability of body weight and health out- comes in the Framingham population. N. Engl. J. Med. 1991, 324, 1839–1844. [Google Scholar] [CrossRef] [PubMed]
- Mehta, T.; Smith, D.L.; Muhammad, J.; Casazza, K. Impact of weight cycling on risk of morbidity and mortality. Obes. Rev. 2014, 15, 870–881. [Google Scholar] [CrossRef] [PubMed]
- Delahanty, L.M.; Pan, Q.; Jablonski, K.A.; Aroda, V.R.; Watson, K.E.; Bray, G.A.; Kahn, S.E.; Florez, J.C.; Perreault, L.; Franks, P.W. Effects of weight loss, weight cycling, and weight loss maintenance on diabetes incidence and change in cardiometabolic traits in the diabetes prevention program. Diabetes Care 2014, 37, 2738–2745. [Google Scholar] [CrossRef] [PubMed]
- Montani, J.P.; Schutz, Y.; Dulloo, A.G. Dieting and weight cycling as risk factors for cardiometabolic diseases: Who is really at risk? Obes. Rev. 2015, 16, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Bangalore, S.; Fayyad, R.; Laskey, R.; DeMicco, D.A.; Messerli, F.H.; Waters, D.D. Body-Weight Fluctuations and Outcomes in Coronary Disease. N. Engl. J. Med. 2017, 376, 1332–1340. [Google Scholar] [CrossRef]
- Madigan, C.D.; Pavey, T.; Daley, A.J.; Jolly, K.; Brown, W.J. Is weight cycling associated with adverse health outcomes? A cohort study. Prev. Med. (Baltim). 2018, 108, 47–52. [Google Scholar] [CrossRef]
- Nam, G.E.; Cho, K.H.; Han, K.; Han, B.; Cho, S.J.; Roh, Y.K.; Kim, S.M.; Choi, Y.S.; Kim, D.H.; Kim, Y.H.; et al. Impact of body mass index and body weight variabilities on mortality: A nationwide cohort study. Int. J. Obes. 2019, 43, 412–423. [Google Scholar] [CrossRef]
- Taylor, C.B.; Jatulis, D.E.; Fortmann, S.P.; Kraemer, H.C. Weight variability effects: A prospective analysis from the Stanford Five-City Project. Am. J. Epidemiol. 1995, 141, 461–465. [Google Scholar] [CrossRef]
- Lissner, L.; Andres, R.; Muller, D.C.; Shimokata, H. Body weight variability in men: Metabolic rate, health and longevity. Int. J. Obes. 1990, 14, 373–383. [Google Scholar] [PubMed]
- Rhee, E.J.; Cho, J.H.; Kwon, H.; Park, S.E.; Park, C.Y.; Oh, K.W.; Park, S.W.; Lee, W.Y. Increased risk of diabetes development in individuals with weight cycling over 4 years: The Kangbuk Samsung Health study. Diabetes Res. Clin. Pract. 2018, 139, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Kodama, S.; Fujihara, K.; Ishiguro, H.; Horikawa, C.; Ohara, N.; Yachi, Y.; Tanaka, S.; Shimano, H.; Kato, K.; Hanyu, O.; et al. Unstable bodyweight and incident type 2 diabetes mellitus: A meta-analysis. J. Diabetes Investig. 2017, 8, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yatsuya, H.; Li, Y.; Chiang, C.; Hirakawa, Y.; Kawazoe, N.; Tamakoshi, K.; Toyoshima, H.; Aoyama, A. Long-term weight-change slope, weight fluctuation and risk of type 2 diabetes mellitus in middle-aged Japanese men and women: Findings of Aichi Workers’ Cohort Study. Nutr. Diabetes 2017, 7, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Mackie, G.M.; Samocha-Bonet, D.; Tam, C.S. Does weight cycling promote obesity and metabolic risk factors? Obes. Res. Clin. Pract. 2017, 11, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Yokomichi, H.; Ohde, S.; Takahashi, O.; Mochizuki, M.; Takahashi, A.; Yoda, Y.; Tsuji, M.; Akiyama, Y.; Yamagata, Z. Weight cycling and the subsequent onset of type 2 diabetes mellitus: 10-year cohort studies in urban and rural Japan. BMJ Open 2017, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Neamat-Allah, J.; Barrdahl, M.; Hüsing, A.; Katzke, V.A.; Bachlechner, U.; Steffen, A.; Kaaks, R.; Schulze, M.B.; Boeing, H.; Kühn, T. Weight cycling and the risk of type 2 diabetes in the EPIC-Germany cohort. Diabetologia 2015, 58, 2718–2725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waring, M.E.; Eaton, C.B.; Lasater, T.M.; Lapane, K.L. Incident diabetes in relation to weight patterns during middle age. Am. J. Epidemiol. 2010, 171, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Kataja-Tuomola, M.; Sundell, J.; Männistö, S.; Virtanen, M.J.; Kontto, J.; Albanes, D.; Virtamo, J. Short-term weight change and fluctuation as risk factors for type 2 diabetes in Finnish male smokers. Eur. J. Epidemiol. 2010, 25, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Field, A.E.; Manson, J.E.; Laird, N.; Williamson, D.F.; Willett, W.C.; Colditz, G.A. Weight cycling and the risk of developing type 2 diabetes among adult women in the United States. Obes. Res. 2004, 12, 267–274. [Google Scholar] [CrossRef]
- French, S.A.; Folsom, A.R.; Jeffery, R.W.; Zheng, W.; Mink, P.J.; Baxter, J.E. Weight variability and incident disease in older women: The Iowa women’s health study. Int. J. Obes. 1997, 21, 217–223. [Google Scholar] [CrossRef]
- Korea National Health Insurance Service. National Health Insurance System of Korea. Available online: http://www.kobia.kr/skin/bbs/downloads_e2/download.php?tbl=policy_report&no=401 (accessed on 25 February 2019).
- Cheol Seong, S.; Kim, Y.-Y.; Khang, Y.-H.; Heon Park, J.; Kang, H.-J.; Lee, H.; Do, C.-H.; Song, J.-S.; Hyon Bang, J.; Ha, S.; et al. Data Resource Profile: The National Health Information Database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2017, 46, 799–800. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.-C.; Lee, S.-Y. National health screening program of Korea. J. Korean Med. Assoc. 2010, 53, 363–370. [Google Scholar] [CrossRef]
- Weisell, R.C. Body mass index as an indicator of obesity. Asia Pac. J. Clin. Nutr. 2002, 11, S681–S684. [Google Scholar] [CrossRef] [Green Version]
- Cereda, E.; Malavazos, A.E.; Caccialanza, R.; Rondanelli, M.; Fatati, G.; Barichella, M. Weight cycling is associated with body weight excess and abdominal fat accumulation: A cross-sectional study. Clin. Nutr. 2011, 30, 718–723. [Google Scholar] [CrossRef] [PubMed]
- Will, J.C.; Williamson, D.F.; Ford, E.S.; Calle, E.E.; Thun, M.J. Intentional weight loss and 13-year diabetes incidence in overweight adults. Am. J. Public Health 2002, 92, 1245–1248. [Google Scholar] [CrossRef]
- Hamman, R.F.; Wing, R.R.; Edelstein, S.L.; Lachin, J.M.; Bray, G.A.; Delahanty, L.; Hoskin, M.; Kriska, A.M.; Mayer-Davis, E.J.; Pi-Sunyer, X. Effect of weight loss with lifestyle intervention on risk of diabetes. Diabetes Care 2006, 29, 2102–2107. [Google Scholar] [CrossRef] [PubMed]
- Colditz, G.A.; Willett, W.C.; Rotnitzky, A.; Manson, J.E. Weight gain as a risk factor for clinical diabetes mellitus in women. Ann. Intern. Med. 1995, 122, 481–486. [Google Scholar] [CrossRef]
- Tuomilehto, J.; Lindström, J.; Eriksson, J.G.; Valle, T.T.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef]
- Chan, J.M.; Rimm, E.B.; Colditz, G.A.; Stampfer, M.J.; Willett, W.C. Obesity, fat distribution, and weight gain as risk factors for clinical diabetes in men. Diabetes Care 1994, 17, 961–969. [Google Scholar] [CrossRef]
- Rodin, J.; Radke-Sharpe, N.; Rebuffé-Scrive, M.; Greenwood, M.R. Weight cycling and fat distribution. Int. J. Obes. 1990, 14, 303–310. [Google Scholar] [PubMed]
- Wallner, S.J.; Luschnigg, N.; Schnedl, W.J.; Lahousen, T.; Sudi, K.; Crailsheim, K.; Möller, R.; Tafeit, E.; Horejsi, R. Body fat distribution of overweight females with a history of weight cycling. Int. J. Obes. 2004, 28, 1143–1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kershaw, E.E.; Flier, J.S. Adipose tissue as an endocrine organ. J. Clin. Endocrinol. Metab. 2004, 89, 2548–2556. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.K.; Gutierrez, D.A.; Kennedy, A.; Hasty, A.H. Weight cycling increases T-cell accumulation in adipose tissue and impairs systemic glucose tolerance. Diabetes 2013, 62, 3180–3188. [Google Scholar] [CrossRef] [PubMed]
- Dankner, R.; Chetrit, A.; Shanik, M.H.; Raz, I.; Roth, J. Basal-state hyperinsulinemia in healthy normoglycemic adults is predictive of type 2 diabetes over a 24-year follow-up: A preliminary report. Diabetes Care 2009, 32, 1464–1466. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, T.L.; Barrett-Connor, E.; Wingard, D.L. The association of lifetime weight and weight control patterns with diabetes among men and women in an adult community. Int. J. Obes. 1989, 13, 723–729. [Google Scholar] [PubMed]
- Martinez-Millana, A.; Argente-Pla, M.; Valdivieso Martinez, B.; Traver Salcedo, V.; Merino-Torres, J. Driving Type 2 Diabetes Risk Scores into Clinical Practice: Performance Analysis in Hospital Settings. J. Clin. Med. 2019, 8, 107. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Body Weight Variability (ASV) a | pb | ||||
|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | ||
| n | 1,125,230 | 909,697 | 838,844 | 982,113 | |
| Age (years) | 45.62 ± 11.25 | 44.69 ± 11.02 | 43.99 ± 11.62 | 41.32 ± 11.51 | <0.001 |
| Sex (male, %) | 686,313 (60.99) | 617,197 (67.85) | 577,603 (68.86) | 704,187 (71.7) | <0.001 |
| Height (cm) c | 165.41 ± 8.6 | 166.73 ± 8.54 | 167.3 ± 8.64 | 168.79 ± 8.57 | <0.001 |
| Body weight (kg) c | 63.15 ± 10.99 | 65.36 ± 11.23 | 66.79 ± 11.57 | 70.46 ± 12.71 | <0.001 |
| Waist circumference (cm) c | 78.21 ± 8.66 | 79.52 ± 8.57 | 80.43 ± 8.65 | 82.44 ± 9.1 | <0.001 |
| BMI (kg/m2) c | 23.02 ± 2.93 | 23.45 ± 2.97 | 23.81 ± 3.06 | 24.67 ± 3.4 | <0.001 |
| Smoking status | <0.001 | ||||
| Non-smoker | 494,831 (44.05) | 366,189 (40.32) | 335,965 (40.11) | 378,029 (38.55) | |
| Ex-smoker | 549,898 (48.95) | 470,391 (51.8) | 432,733 (51.67) | 514,782 (52.49) | |
| Current smoker | 78,579 (7) | 71,596 (7.88) | 68,870 (8.22) | 87,830 (8.96) | |
| Alcohol consumption | <0.001 | ||||
| None | 630,177 (56.05) | 459,670 (50.56) | 413,663 (49.35) | 453,304 (46.18) | |
| ≤Twice/week | 198,285 (17.64) | 177,984 (19.58) | 162,727 (19.41) | 192,835 (19.65) | |
| ≥Three times/week | 295,842 (26.31) | 271,424 (29.86) | 261,909 (31.24) | 335,421 (34.17) | |
| Physical activity (regular) | 234,258 (20.83) | 193,048 (21.23) | 176,553 (21.06) | 212,629 (21.66) | <0.001 |
| Household income (lower 20%) | 191,579 (17.03) | 144,372 (15.87) | 138,953 (16.56) | 153,461 (15.63) | <0.001 |
| Hypertension d | 206,915 (18.39) | 168,887 (18.57) | 159,818 (19.05) | 180,666 (18.4) | <0.001 |
| Dyslipidemia d | 175,343 (15.58) | 141,105 (15.51) | 133,160 (15.87) | 152,793 (15.56) | <0.001 |
| History of heart disease | 9807 (1.16) | 7550 (1.08) | 7750 (1.22) | 8176 (1.09) | <0.001 |
| History of stroke | 3007 (0.36) | 2344 (0.34) | 2688 (0.42) | 3079 (0.41) | <0.001 |
| Systolic blood pressure (mmHg) | 120.25 ± 13.69 | 120.91 ± 13.55 | 121.34 ± 13.58 | 121.9 ± 13.48 | <0.001 |
| Diastolic blood pressure (mmHg) | 75.62 ± 9.54 | 76.13 ± 9.48 | 76.31 ± 9.5 | 76.7 ± 9.49 | <0.001 |
| Fasting plasma glucose (mg/dL) | 92.42 ± 10.73 | 92.61 ± 10.73 | 92.64 ± 10.75 | 92.48 ± 10.84 | <0.001 |
| Total cholesterol (mg/dL) | 194.26 ± 34.61 | 194.87 ± 34.57 | 195.03 ± 34.91 | 195.28 ± 35.56 | <0.001 |
| Group | n | Incident Diabetes | Duration | Incidence a | Model 1 b | Model 2 c | Model 3 d | |
|---|---|---|---|---|---|---|---|---|
| Body weight variability (ASV) e | Q1 | 1,125,230 | 20,793 | 4,906,440.78 | 4.24 | 1.00 | 1.00 | 1.00 |
| Q2 | 909,697 | 16,652 | 3,966,357.77 | 4.20 | 1.04 (1.02, 1.06) | 1.02 (1.001, 1.04) | 0.99 (0.97, 1.01) | |
| Q3 | 838,844 | 16,384 | 3,647,718.23 | 4.49 | 1.13 (1.10, 1.15) | 1.09 (1.06, 1.11) | 1.01 (0.99, 1.03) | |
| Q4 | 982,113 | 20,546 | 4,262,509.48 | 4.82 | 1.39 (1.36, 1.41) | 1.29 (1.27, 1.32) | 1.10 (1.07, 1.12) |
| Highest Quartile of BWV | ||
|---|---|---|
| HR (95% CI) a | p for Interaction | |
| Weight change status (%) | 0.43 | |
| Loss (≥5) | 1.11 (1.06, 1.16) | |
| Stable (±<5) | 1.07 (1.05, 1.10) | |
| Gain (≥5) | 1.12 (1.08, 1.16) | |
| Fasting plasma glucose (mg/dL) | <0.001 | |
| <100 | 1.24 (1.21, 1.27) | |
| ≥100, <126 | 1.00 (0.98, 1.02) | |
| Age (years) | 0.19 | |
| <65 | 1.10 (1.08, 1.12) | |
| ≥65 | 1.09 (1.04, 1.14) | |
| Sex | 0.001 | |
| Male | 1.08 (1.06,1.10) | |
| Female | 1.14 (1.10,1.17) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, K.-Y.; Hwang, H.-S.; Cho, K.-H.; Han, K.; Nam, G.E.; Kim, Y.H.; Kwon, Y.; Park, Y.-G. Body Weight Fluctuation as a Risk Factor for Type 2 Diabetes: Results from a Nationwide Cohort Study. J. Clin. Med. 2019, 8, 950. https://doi.org/10.3390/jcm8070950
Park K-Y, Hwang H-S, Cho K-H, Han K, Nam GE, Kim YH, Kwon Y, Park Y-G. Body Weight Fluctuation as a Risk Factor for Type 2 Diabetes: Results from a Nationwide Cohort Study. Journal of Clinical Medicine. 2019; 8(7):950. https://doi.org/10.3390/jcm8070950
Chicago/Turabian StylePark, Kye-Yeung, Hwan-Sik Hwang, Kyung-Hwan Cho, Kyungdo Han, Ga Eun Nam, Yang Hyun Kim, Yeongkeun Kwon, and Yong-Gyu Park. 2019. "Body Weight Fluctuation as a Risk Factor for Type 2 Diabetes: Results from a Nationwide Cohort Study" Journal of Clinical Medicine 8, no. 7: 950. https://doi.org/10.3390/jcm8070950