Detection and Characterization of a Biochemical Signature Associated with Diabetic Nephropathy Using Near-infrared Spectroscopy on Tissue Sections

 , ,
, , 
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Population
2.2. Determination of Routine Laboratory Parameters
2.3. Preparation of Tissue Sections
2.4. Carbamoylation and (de)Glycation of Tissue Sections
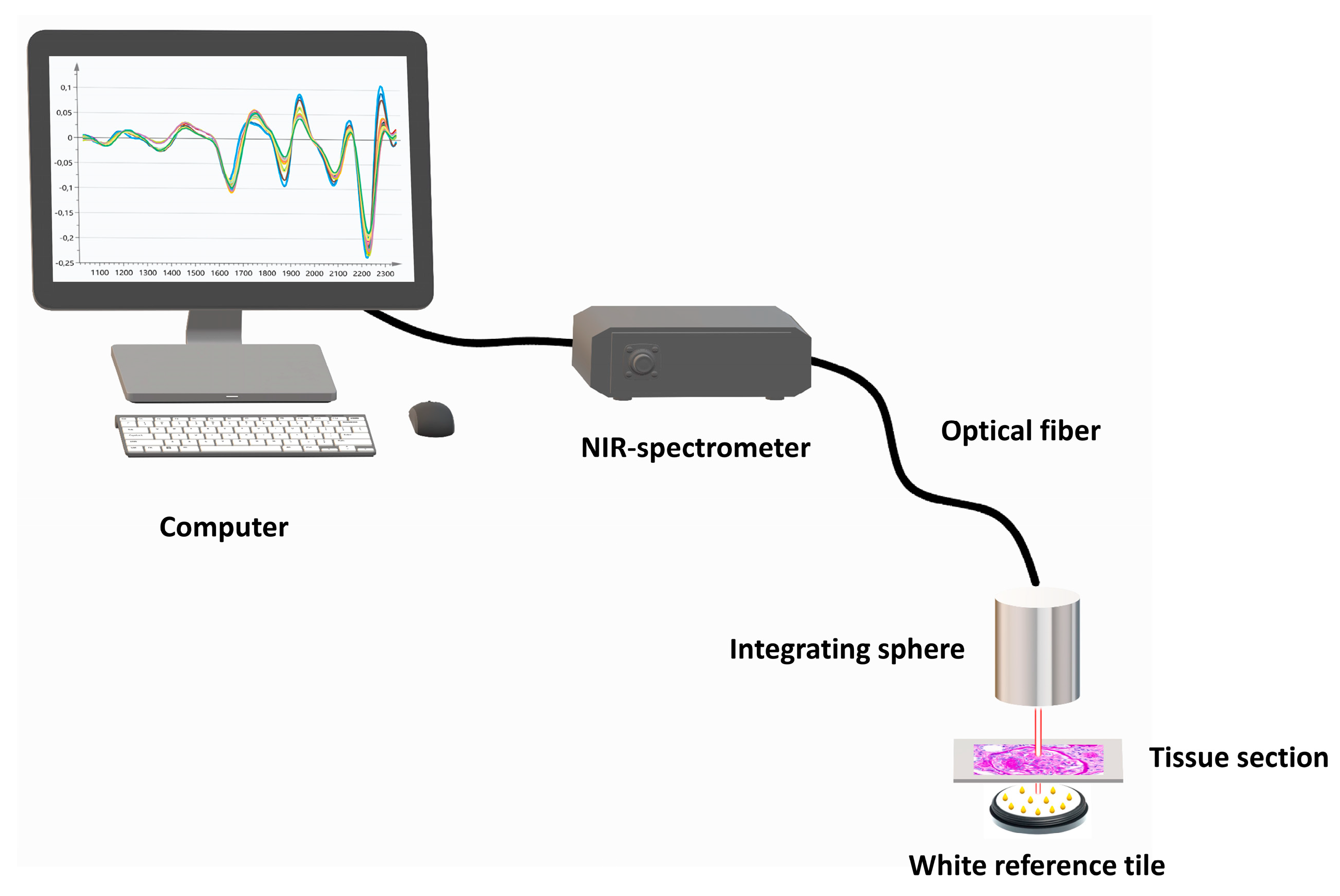
2.5. Near-Infrared Spectroscopic Analysis
2.6. Multivariate Data Analysis
2.7. Statistical Analysis
3. Results
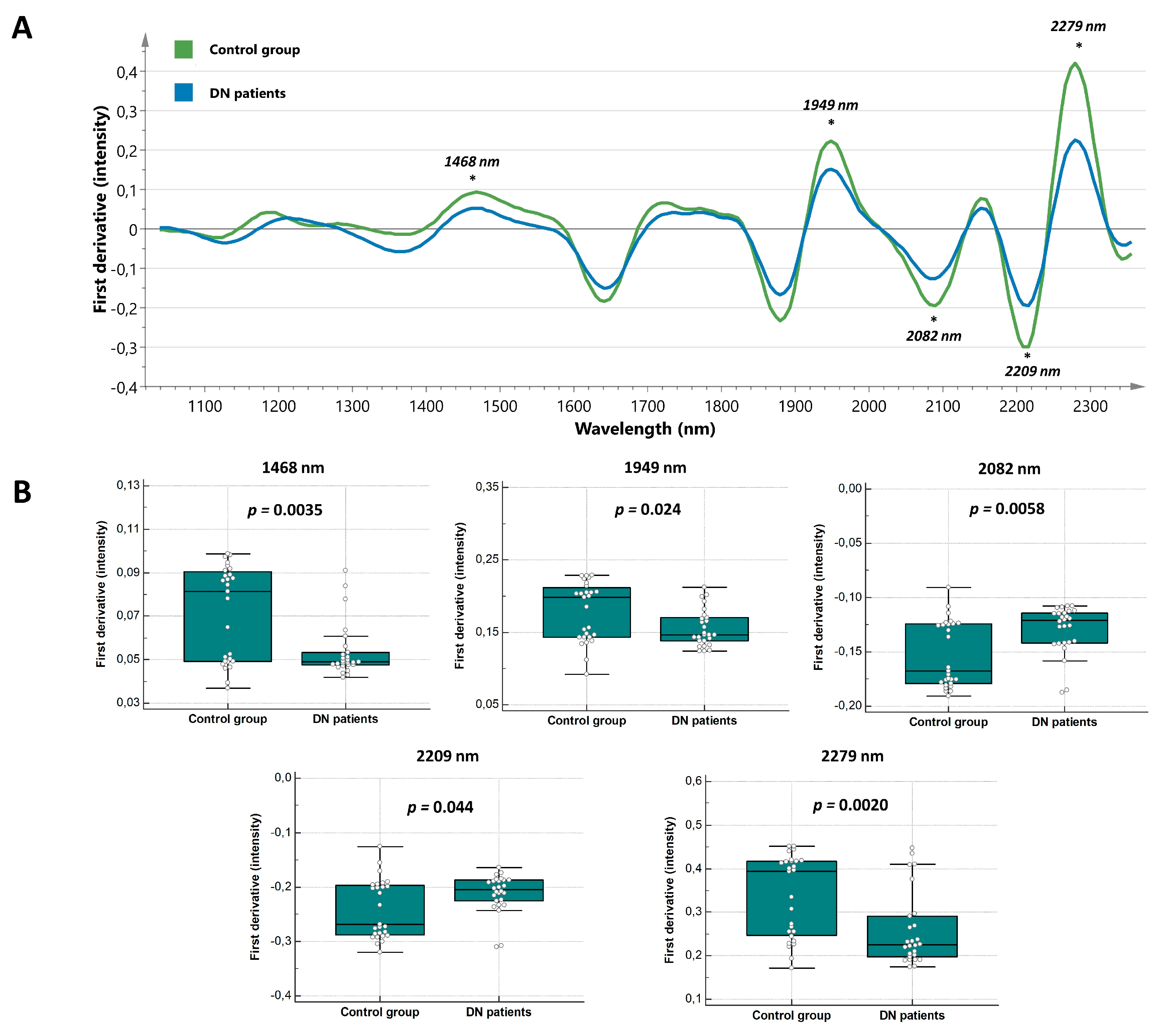
3.1. Exploration of Discriminative Spectral Features in Diabetic Nephropathy Patients
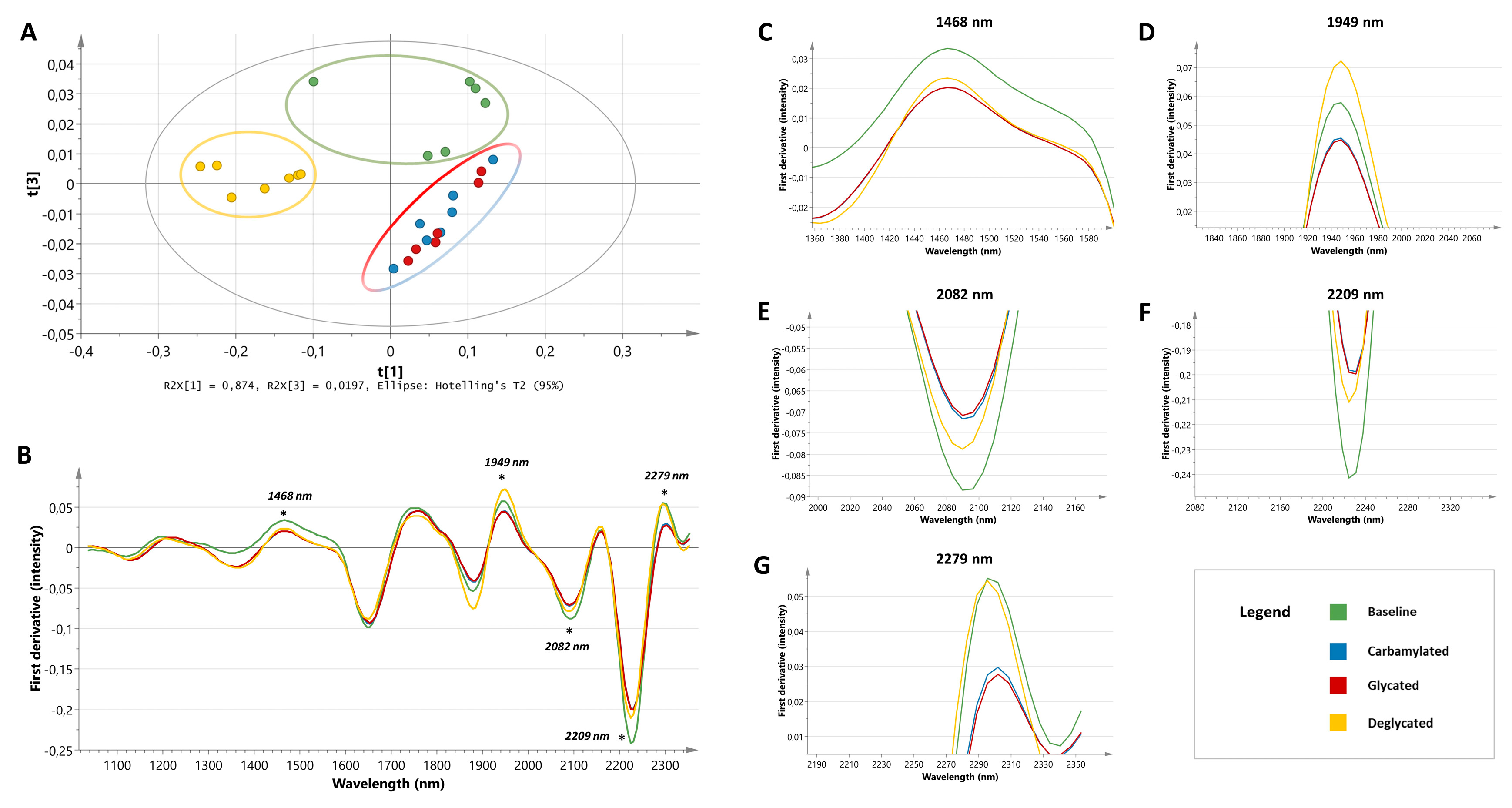
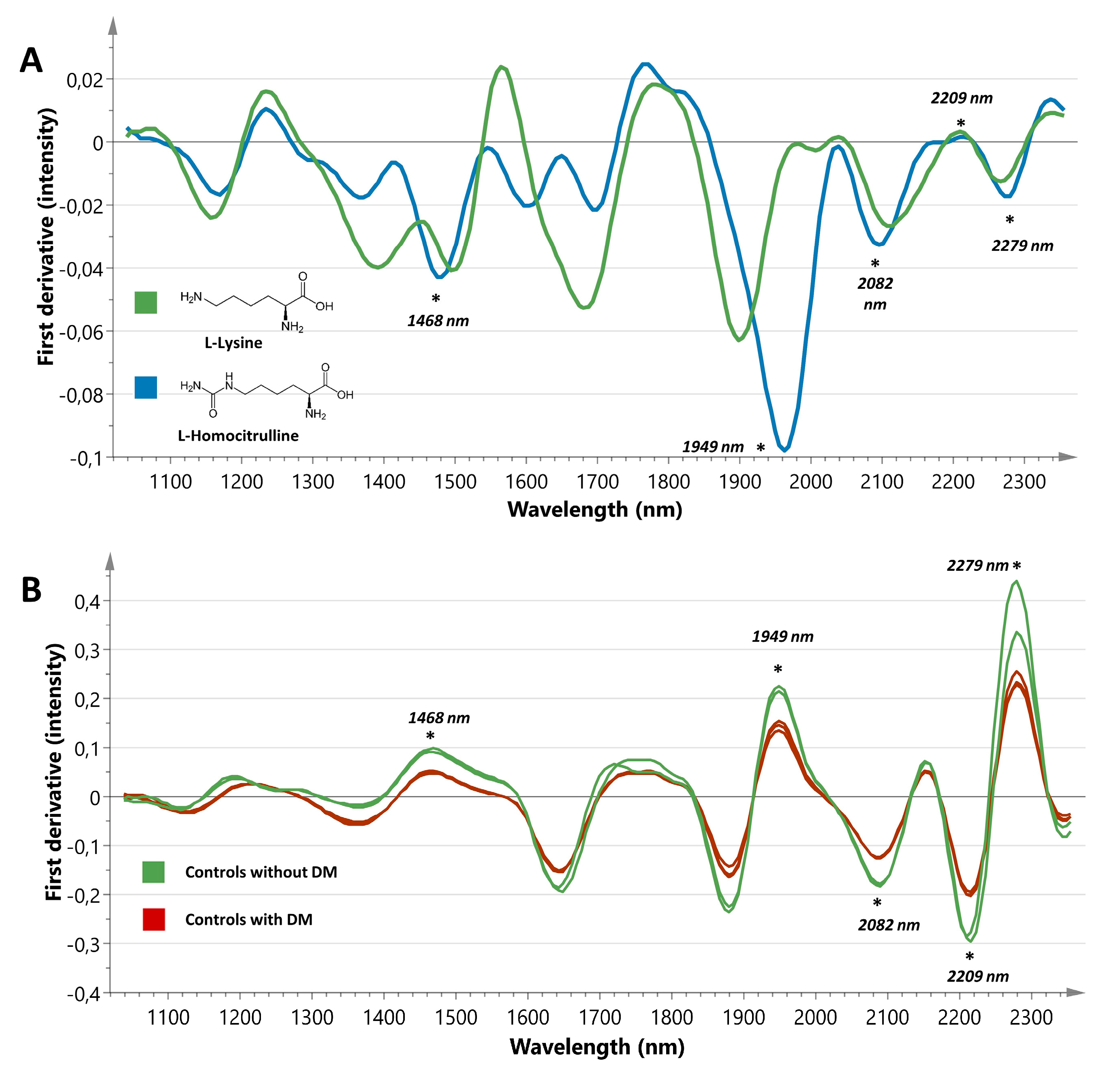
3.2. Unravelling The Biochemical Nature of Discriminative Spectral Features
3.3. Discriminative Power of The Biochemical Signature
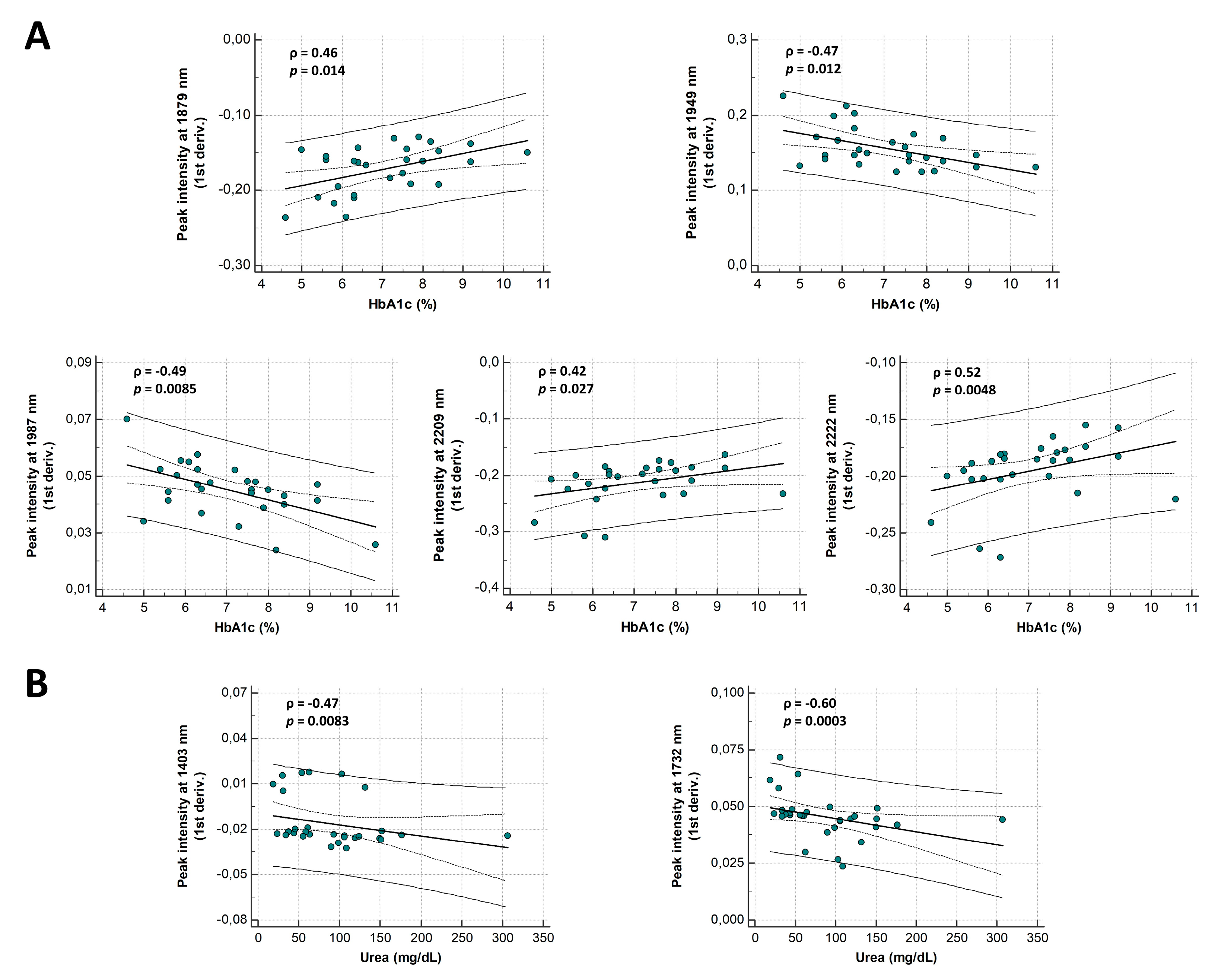
3.4. Correlation of Spectral Markers with Routine Laboratory Parameters and Age
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Persson, F.; Rossing, P. Diagnosis of diabetic kidney disease: State of the art and future perspective. Kidney Int. Suppl. 2018, 8, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou-Marketou, N.; Chrousos, G.P.; Kanaka-Gantenbein, C. Diabetic nephropathy in type 1 diabetes: A review of early natural history, pathogenesis, and diagnosis. Diabetes Metab. Res. Rev. 2017, 33, e2841. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, K.R.; Bakris, G.L.; Bilous, R.W.; Chiang, J.L.; De Boer, I.H.; Goldstein-Fuchs, J.; Hirsch, I.B.; Kalantar-Zadeh, K.; Narva, A.S.; Navaneethan, S.D.; et al. Diabetic kidney disease: A report from an ADA consensus conference. Diabetes Care 2014, 37, 2864–2883. [Google Scholar] [CrossRef] [PubMed]
- Varma, V.K.; Kajdacsy-Balla, A.; Akkina, S.K.; Setty, S.; Walsh, M.J. A label-free approach by infrared spectroscopic imaging for interrogating the biochemistry of diabetic nephropathy progression. Kidney Int. 2016, 89, 1153–1159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Josephson, M.A. Monitoring and managing graft health in the kidney transplant recipient. Clin. J. Am. Soc. Nephrol. 2011, 6, 1774–1780. [Google Scholar] [CrossRef] [PubMed]
- Adler, S. Diabetic nephropathy: Linking histology, cell biology, and genetics. Kidney Int. 2004, 66, 2095–2106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Currie, G.; McKay, G.; Delles, C. Biomarkers in diabetic nephropathy: Present and future. World J. Diabetes 2014, 5, 763–776. [Google Scholar] [CrossRef] [PubMed]
- De Bruyne, S.; Speeckaert, M.M.M.; Delanghe, J.R. Applications of mid-infrared spectroscopy in the clinical laboratory setting. Crit. Rev. Clin. Lab. Sci. 2018, 55, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Nicolas, C.; Jaisson, S.; Gorisse, L.; Tessier, F.J.; Niquet-Léridon, C.; Jacolot, P.; Pietrement, C.; Gillery, P. Carbamoylation is a competitor of glycation for protein modification in vivo. Diabetes Metab. 2018, 44, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Gorisse, L.; Pietrement, C.; Vuiblet, V.; Schmelzer, C.E.H.; Köhler, M.; Duca, L.; Debelle, L.; Fornès, P.; Jaisson, S.; Gillery, P. Protein carbamoylation is a hallmark of aging. Proc. Natl. Acad. Sci. USA 2016, 113, 1191–1196. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, L.; Matafome, P.; Crisóstomo, J.; Santos-Silva, D.; Sena, C.; Pereira, P.; Seiça, R. Advanced glycation end products and diabetic nephropathy: A comparative study using diabetic and normal rats with methylglyoxal-induced glycation. J. Physiol. Biochem. 2014, 70, 173–184. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2018. Diabetes Care 2018, 41, S13–S27. [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Iii, A.F.C.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2014, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Orsonneau, J.L.; Douet, P.; Massoubre, C.; Lustenberger, P.; Bernard, S. An improved pyrogallol red-molybdate method for determining total urinary protein. Clin. Chem. 1989, 35, 2233–2236. [Google Scholar] [PubMed]
- De Bruyne, S.; Speeckaert, R.; Boelens, J.; Hayette, M.P.; Speeckaert, M.; Delanghe, J. Infrared spectroscopy as a novel tool to diagnose onychomycosis. Br. J. Dermatol. 2018, 180, 637–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monteyne, T.; Coopman, R.; Kishabongo, A.S.; Himpe, J.; Lapauw, B.; Shadid, S.; Van Aken, E.H.; Berenson, D.; Speeckaert, M.M.; De Beer, T.; et al. Analysis of protein glycation in human fingernail clippings with near-infrared (NIR) spectroscopy as an alternative technique for the diagnosis of diabetes mellitus. Clin. Chem. Lab. Med. 2018, 56, 1551–1558. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, L.; Johansson, E.; Kettaneh-Wold, N.; Trygg, J.; Wikström, C.; Wold, S. Pca. In Multi-and Megavariate Data Analysis Part 1, Basic Principles and Applications, 2nd ed.; Umetrics AB: Umea, Sweden, 2006; pp. 39–62. [Google Scholar]
- Workman, J.; Weyer, L. Practical Guide to Interpretive Near-Infrared Spectroscopy, 1st ed.; CRC Press: Boca Raton, FL, USA, 2007; pp. 240–262. [Google Scholar]
- Balion, C.M.; Draisey, T.F.; Thibert, R.J. Carbamoylated hemoglobin and carbamoylated plasma protein in hemodialyzed patients. Kidney Int. 1998, 53, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Fiorentino, M.; Bolignano, D.; Tesar, V.; Pisano, A.; Van Biesen, W. Renal biopsy in patients with diabetes: A pooled meta-analysis of 48 studies. Nephrol. Dial. Transplant. 2017, 32, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Delanghe, J.R.; Delanghe, S.E.; De Buyzere, M.L.; Speeckaert, M.M. Infrared spectroscopic imaging for interrogating the carbohydrate biochemistry of diabetic nephropathy progression. Kidney Int. 2016, 90, 225–226. [Google Scholar] [CrossRef] [PubMed]
- Brosius, F.C.; Pennathur, S. How to find a prognostic biomarker for progressive diabetic nephropathy. Kidney Int. 2013, 83, 996–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Ctr (n = 27) | DN (n = 26) | DM and RCC (n = 11) | Ctr vs. DN p-Value | Ctr vs. DM and RCC p-Value | DN vs. DM and RCC p-Value |
|---|---|---|---|---|---|---|
| Age (yr) | 55 (47–61) | 60 (50–66) | 70 (66–73) | N.S. | <0.0001 | 0.0061 |
| Women (%) | 70 | 77 | 91 | N.S. | N.S. | N.S. |
| DM (%) | 89 | 100 | 100 | N.S. | N.S. | N.S. |
| Creatinine (mg/dL) | 1.2 (1.0–1.9) | 1.9 (1.3–3.3) | 1.4 (1.3–1.5) | 0.0096 | N.S. | N.S. |
| eGFR (mL/min/1.73 m2) | 54 (38–79) | 36 (16–50) | 53 (40.0–54) | 0.0091 | N.S. | N.S. |
| Urea (mg/dL) | 44.0 (31.8–66.3) | 96.0 (54.0–124.0) | 38.0 (33.0–41.0) | 0.0011 | N.S. | 0.0011 |
| Proteinuria (g/g creat) | 0.2 (0.03–0.4) | 2.7 (2.3–6.9) | 0.0 (0.0–0.12) | <0.0001 | N.S. | <0.0001 |
| HbA1c (%) | 6.6 (6.0–7.4) | 7.4 (6.2–8.1) | 6.6 (6.0–7.7) | N.S. | N.S. | N.S. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Bruyne, S.; Van Dorpe, J.; Himpe, J.; Van Biesen, W.; Delanghe, S.; Speeckaert, M.M.; Delanghe, J.R. Detection and Characterization of a Biochemical Signature Associated with Diabetic Nephropathy Using Near-infrared Spectroscopy on Tissue Sections. J. Clin. Med. 2019, 8, 1022. https://doi.org/10.3390/jcm8071022
De Bruyne S, Van Dorpe J, Himpe J, Van Biesen W, Delanghe S, Speeckaert MM, Delanghe JR. Detection and Characterization of a Biochemical Signature Associated with Diabetic Nephropathy Using Near-infrared Spectroscopy on Tissue Sections. Journal of Clinical Medicine. 2019; 8(7):1022. https://doi.org/10.3390/jcm8071022
Chicago/Turabian StyleDe Bruyne, Sander, Jo Van Dorpe, Jonas Himpe, Wim Van Biesen, Sigurd Delanghe, Marijn M. Speeckaert, and Joris R. Delanghe. 2019. "Detection and Characterization of a Biochemical Signature Associated with Diabetic Nephropathy Using Near-infrared Spectroscopy on Tissue Sections" Journal of Clinical Medicine 8, no. 7: 1022. https://doi.org/10.3390/jcm8071022