Longtime Neurologic Outcome of Extracorporeal Membrane Oxygenation and Non Extracorporeal Membrane Oxygenation Acute Respiratory Distress Syndrome Survivors

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
- -
- a thorough medical history of the time from hospital discharge up to the day of the visit
- -
- assessment of orientation
- -
- clinical assessment of cranial nerve function
- -
- muscle strength
- -
- sensation
- -
- motor activities
- -
- coordination (finger-to-nose-test, rapid alternating movements), testing for postural instability (Rhomberg test, pronator-drift), and walking the patient in different modalities (normal, tiptoe, tightrope).
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA J. Am. Med. Assoc. 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Bein, T.; Grasso, S.; Moerer, O.; Quintel, M.; Guerin, C.; Deja, M.; Brondani, A.; Mehta, S. The standard of care of patients with ards: Ventilatory settings and rescue therapies for refractory hypoxemia. Intensive Care Med. 2016, 42, 699–711. [Google Scholar] [CrossRef] [PubMed]
- Terragni, P.P.; Rosboch, G.; Tealdi, A.; Corno, E.; Menaldo, E.; Davini, O.; Gandini, G.; Herrmann, P.; Mascia, L.; Quintel, M.; et al. Tidal hyperinflation during low tidal volume ventilation in acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2007, 175, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Vaquer, S.; De Haro, C.; Peruga, P.; Oliva, J.C.; Artigas, A. Systematic review and meta-analysis of complications and mortality of veno-venous extracorporeal membrane oxygenation for refractory acute respiratory distress syndrome. Ann. Intensive Care 2017, 7, 51. [Google Scholar] [CrossRef] [PubMed]
- Fichtner, F.; Moerer, O.; Laudi, S.; Weber-Carstens, S.; Nothacker, M.; Kaisers, U.; The Guideline Group on Mechanical Ventilation. Extracorporeal Membrane Oxygenation in Acute Respiratory Insufficiency. Mechanical ventilation and extracorporeal membrane oxygenation in acute respiratory insufficiency. Deutsch. Arzteblatt Int. 2018, 115, 840–847. [Google Scholar]
- Sauer, C.M.; Yuh, D.D.; Bonde, P. Extracorporeal membrane oxygenation use has increased by 433% in adults in the united states from 2006 to 2011. ASAIO J. Am. Soc. Artif. Internal Org. 2015, 61, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, R.; Barili, F.; Mauro, M.D.; Gelsomino, S.; Parise, O.; Rycus, P.T.; Maessen, J.; Mueller, T.; Muellenbach, R.; Belohlavek, J.; et al. In-hospital neurologic complications in adult patients undergoing venoarterial extracorporeal membrane oxygenation: Results from the extracorporeal life support organization registry. Crit. Care Med. 2016, 44, e964–e972. [Google Scholar] [CrossRef]
- Lorusso, R.; Gelsomino, S.; Parise, O.; Di Mauro, M.; Barili, F.; Geskes, G.; Vizzardi, E.; Rycus, P.T.; Muellenbach, R.; Mueller, T.; et al. Neurologic injury in adults supported with veno-venous extracorporeal membrane oxygenation for respiratory failure: Findings from the extracorporeal life support organization database. Crit. Care Med. 2017, 45, 1389–1397. [Google Scholar] [CrossRef]
- Sutter, R.; Tisljar, K.; Marsch, S. Acute neurologic complications during extracorporeal membrane oxygenation—A systematic review. Crit. Care Med. 2018, 46, 1506–1513. [Google Scholar] [CrossRef]
- Pinto, V.L.; Pruthi, S.; Westrick, A.C.; Shannon, C.N.; Bridges, B.C.; Le, T.M. Brain magnetic resonance imaging findings in pediatric patients post extracorporeal membrane oxygenation. ASAIO J. Am. Soc. Artif. Internal Org. 2017, 63, 810–814. [Google Scholar] [CrossRef]
- Mehrholz, J.; Muckel, S.; Oehmichen, F.; Pohl, M. First results about recovery of walking function in patients with intensive Care unit-acquired muscle weakness from the general weakness syndrome therapy (gymnast) cohort study. BMJ Open 2015, 5, e008828. [Google Scholar] [CrossRef] [PubMed]
- Kazmi, S.O.; Sivakumar, S.; Karakitsos, D.; Alharthy, A.; Lazaridis, C. Cerebral pathophysiology in extracorporeal membrane oxygenation: Pitfalls in daily clinical management. Crit. Care Res. Pract. 2018, 2018, 3237810. [Google Scholar] [CrossRef] [PubMed]
- Nasr, D.M.; Rabinstein, A.A. Neurologic complications of extracorporeal membrane oxygenation. J. Clin. Neurol. 2015, 11, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Pappalardo, F.; Montisci, A. Neurologic complications during v-v extracorporeal membrane oxygenation: Still counting. J. Thorac. Dis. 2017, 9, 2774–2776. [Google Scholar] [CrossRef] [PubMed]
- Xie, A.; Lo, P.; Yan, T.D.; Forrest, P. Neurologic complications of extracorporeal membrane oxygenation: A review. J. Cardiothorac. Vasc. Anesth. 2017, 31, 1836–1846. [Google Scholar] [CrossRef]
- Chiumello, D.; Coppola, S.; Froio, S.; Gotti, M. What’s next after ards: Long-term outcomes. Respir. Care 2016, 61, 689–699. [Google Scholar] [CrossRef]
- Herridge, M.S.; Moss, M.; Hough, C.L.; Hopkins, R.O.; Rice, T.W.; Bienvenu, O.J.; Azoulay, E. Recovery and outcomes after the acute respiratory distress syndrome (ards) in patients and their family Caregivers. Intensive Care Med. 2016, 42, 725–738. [Google Scholar] [CrossRef]
- Wang, Z.Y.; Li, T.; Wang, C.T.; Xu, L.; Gao, X.J. Assessment of 1-year outcomes in survivors of severe acute respiratory distress syndrome receiving extracorporeal membrane oxygenation or mechanical ventilation: A prospective observational study. Chin. Med. J. Engl. 2017, 130, 1161–1168. [Google Scholar] [CrossRef]
- Nordon-Craft, A.; Moss, M.; Quan, D.; Schenkman, M. Intensive care unit–acquired weakness: Implications for physical therapist management. Phys. Ther. 2012, 92, 1494–1506. [Google Scholar] [CrossRef]
- Bercker, S.; Weber-Carstens, S.; Deja, M.; Grimm, C.; Wolf, S.; Behse, F.; Busch, T.; Falke, K.J.; Kaisers, U. Critical illness polyneuropathy and myopathy in patients with acute respiratory distress syndrome. Crit. Care Med. 2005, 33, 711–715. [Google Scholar] [CrossRef]
- Fletcher, S.N.; Kennedy, D.D.; Ghosh, I.R.; Misra, V.P.; Kiff, K.; Coakley, J.H.; Hinds, C.J. Persistent neuromuscular and neurophysiologic abnormalities in long-term survivors of prolonged critical illness. Crit. Care Med. 2003, 31, 1012–1016. [Google Scholar] [CrossRef] [PubMed]
- Stoll, C.; Haller, M.; Briegel, J.; Meier, M.; Manert, W.; Hummel, T.; Heyduck, M.; Lenhart, A.; Polasek, J.; Bullinger, M.; et al. health-related quality of life. Long-term survival in patients with ards following extracorporeal membrane oxygenation (ecmo). Der Anaesthesist 1998, 47, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Angus, D.C.; Musthafa, A.A.; Clermont, G.; Griffin, M.F.; Linde-Zwirble, W.T.; Dremsizov, T.T.; Pinsky, M.R. Quality-adjusted survival in the first year after the acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2001, 163, 1389–1394. [Google Scholar] [CrossRef] [PubMed]
- Madonick, M.J. Ophthalmoplegia internuclearis anterior without a lesion of the posterior longitudinal bundle. Arch. Neurol. Psychiatry 1951, 66, 338–345. [Google Scholar] [CrossRef]
- Henkin, R.I.; Larson, A.L.; Powell, R.D. Hypogeusia, dysgeusia, hyposmia, and dysosmia following influenza-like infection. Ann. Otol. Rhinol. Laryngol. 1975, 84, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Hohman, M.H.; Hadlock, T.A. Etiology, diagnosis, and management of facial palsy: 2000 patients at a facial nerve center. Laryngoscope 2014, 124, E283–E293. [Google Scholar] [CrossRef] [PubMed]
- Bandaru, S.P.; Liu, S.; Waxman, S.G.; Tan, A.M. Dendritic spine dysgenesis contributes to hyperreflexia after spinal cord injury. J. Neurophysiol. 2015, 113, 1598–1615. [Google Scholar] [CrossRef] [Green Version]
- Yates, C.; Charlesworth, A.; Allen, S.R.; Reese, N.B.; Skinner, R.D.; Garcia-Rill, E. The onset of hyperreflexia in the rat following complete spinal cord transection. Spinal Cord 2008, 46, 798–803. [Google Scholar] [CrossRef] [Green Version]
- Yates, C.C.; Charlesworth, A.; Reese, N.B.; Skinner, R.D.; Garcia-Rill, E. The effects of passive exercise therapy initiated prior to or after the development of hyperreflexia following spinal transection. Exp. Neurol. 2008, 213, 405–409. [Google Scholar] [CrossRef] [Green Version]
- Yates, C.C.; Charlesworth, A.; Reese, N.B.; Ishida, K.; Skinner, R.D.; Garcia-Rill, E. Modafinil normalized hyperreflexia after spinal transection in adult rats. Spinal Cord 2009, 47, 481–485. [Google Scholar] [CrossRef]
- Suddon, H. A classification of nerve injuries. Br. Med. J. 1942, 4, 237–239. [Google Scholar] [CrossRef] [PubMed]
- Campbell, W.W. Evaluation and management of peripheral nerve injury. Clin. Neurophysiol. 2008, 119, 1951–1965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rydevik, B.; Lundborg, G. Permeability of intraneural microvessels and perineurium following acute, graded experimental nerve compression. Scand. J. Plast. Reconstr. Surg. 1977, 11, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Olivecrona, C.; Blomfeldt, R.; Ponzer, S.; Stanford, B.R.; Nilsson, B.Y. Tourniquet cuff pressure and nerve injury in knee arthroplasty in a bloodless field: A neurophysiological study. Acta Orthop. 2013, 84, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Dumitru, D.; Diaz, C.A.; King, J.C. Prevalence of denervation in paraspinal and foot intrinsic musculature. Am. J. Phys. Med. Rehabil. 2001, 80, 482–490. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| ECMO | nonECMO | p-Value | |
|---|---|---|---|
| Age | 53.87 ± 10.66 | 61.92 ± 10.81 | 0.059 |
| Sex (f:m) | 6:11 | 5:8 | 0.526 |
| SAPS II admission | 33.80 ± 9.34 | 37.69 ± 10.74 | 0.320 |
| ECMO duration (days) | 11.26 ± 8.22 | - | - |
| Mechanical ventilation (days) | 17.86 ± 12.69 | 9.95 ± 5.18 | 0.046 * |
| ICU stay (days) | 20.93 ± 11.34 | 19.69 ± 11.18 | 0.773 |
| Hospital stay (days) | 40.93 ± 16.57 | 39.38 ± 24.61 | 0.849 |
| Discharge – Follow-up (months) | 21.85 ± 12.13 | 23.82 ± 11.47 | 0.628 |
| ECMO | nonECMO | p-Value | |
|---|---|---|---|
| Orientation (no. of findings) | 0 | 1 | 0.464 |
| Cranial nerves (no. of findings) | 5 | 4 | 1.0 |
| Rhomberg test (no. of findings) | 4 | 2 | 0.655 |
| Arm elevation (no. of findings) | 3 | 0 | 0.226 |
| Walking (no. of findings) | 7 | 6 | 1.0 |
| Diadochokinesis (no. of findings) | 0 | 0 | - |
| Finger-nose-test (no. of findings) | 0 | 0 | - |
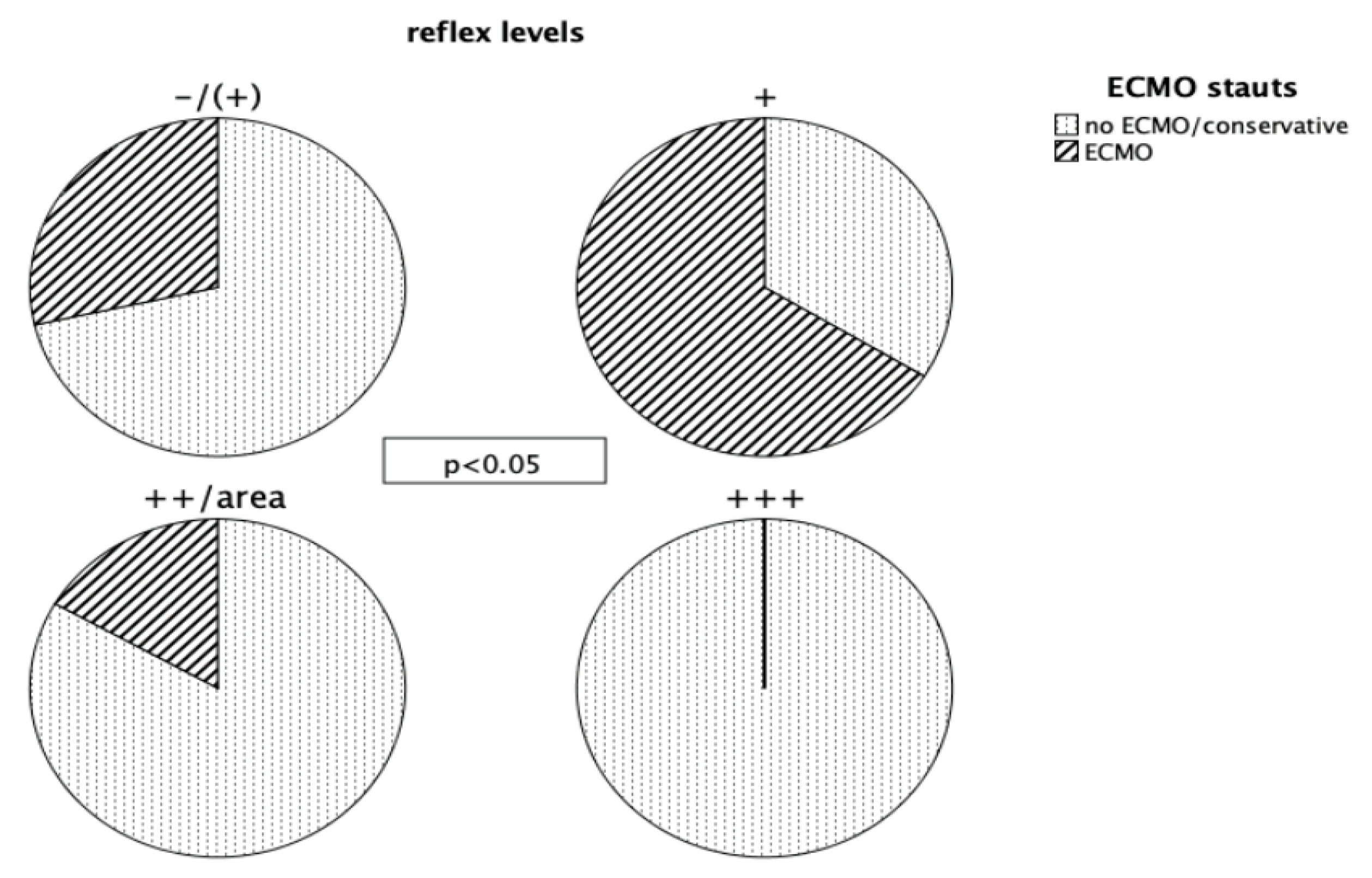
| BTR right (no. of findings) | 1 | 5 | 0.013 * |
| BTR left (no. of findings) | 0 | 5 | 0.013 * |
| TTR right (no. of findings) | 1 | 5 | 0.022 * |
| TTR left (no. of findings) | 0 | 5 | 0.013 * |
| BRTR right (no. of findings) | 0 | 4 | 0.035 * |
| BRTR left (no. of findings) | 0 | 4 | 0.035 * |
| PTR right (no. of findings) | 3 | 9 | 0.027 * |
| PTR left (no. of findings) | 4 | 8 | 0.125 |
| GTR right (no. of findings) | 2 | 8 | 0.041 * |
| GTR left (no. of findings) | 2 | 7 | 0.149 |
| Babinski (no. of findings) | 0 | 0 | - |
| Paresis (no. of findings) | 5 | 0 | 0.044 * |
| Paresthesia (no. of findings) | 10 | 4 | 0.128 |
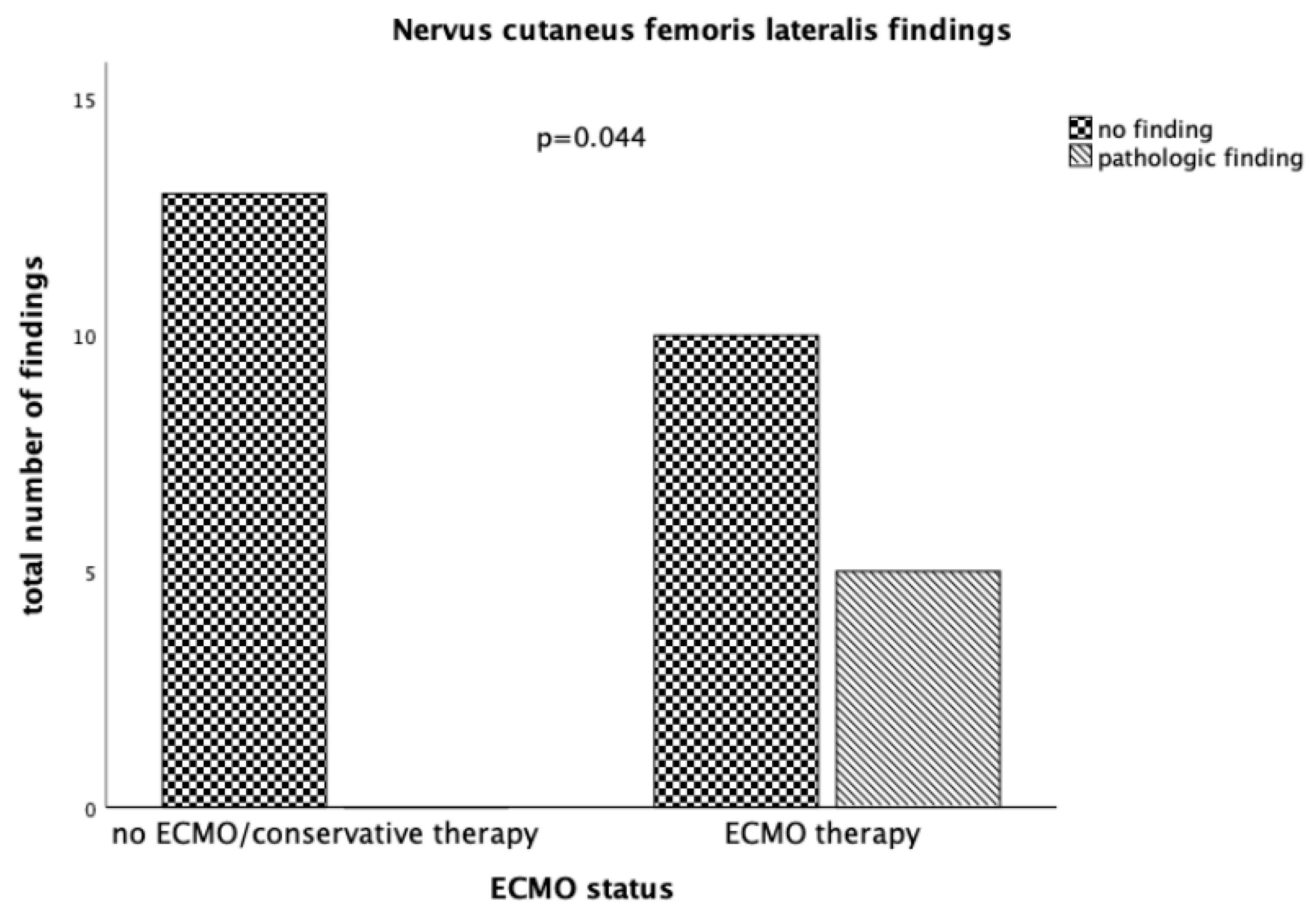
| Lesion of N. cutaneus femoris lateralis (no. of findings) | 5 | 0 | 0.044 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harnisch, L.-O.; Riech, S.; Mueller, M.; Gramueller, V.; Quintel, M.; Moerer, O. Longtime Neurologic Outcome of Extracorporeal Membrane Oxygenation and Non Extracorporeal Membrane Oxygenation Acute Respiratory Distress Syndrome Survivors. J. Clin. Med. 2019, 8, 1020. https://doi.org/10.3390/jcm8071020
Harnisch L-O, Riech S, Mueller M, Gramueller V, Quintel M, Moerer O. Longtime Neurologic Outcome of Extracorporeal Membrane Oxygenation and Non Extracorporeal Membrane Oxygenation Acute Respiratory Distress Syndrome Survivors. Journal of Clinical Medicine. 2019; 8(7):1020. https://doi.org/10.3390/jcm8071020
Chicago/Turabian StyleHarnisch, Lars-Olav, Sebastian Riech, Marion Mueller, Vanessa Gramueller, Michael Quintel, and Onnen Moerer. 2019. "Longtime Neurologic Outcome of Extracorporeal Membrane Oxygenation and Non Extracorporeal Membrane Oxygenation Acute Respiratory Distress Syndrome Survivors" Journal of Clinical Medicine 8, no. 7: 1020. https://doi.org/10.3390/jcm8071020