A Meta-Epidemiological Appraisal of the Effects of Interdisciplinary Multimodal Pain Therapy Dosing for Chronic Low Back Pain


Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Study Selection
2.2. Data Extraction
2.3. Assessment of Bias
2.4. Data Synthesis and Analysis
3. Results
3.1. Characteristics of Included Studies
3.2. Risk of Bias in Included Studies
3.3. Publication Bias
3.4. Analyses for Outcomes of Interdisciplinary Multimodal Pain Therapy (IMPT) by Length, Contact, and Intensity
3.5. Meta-Regression
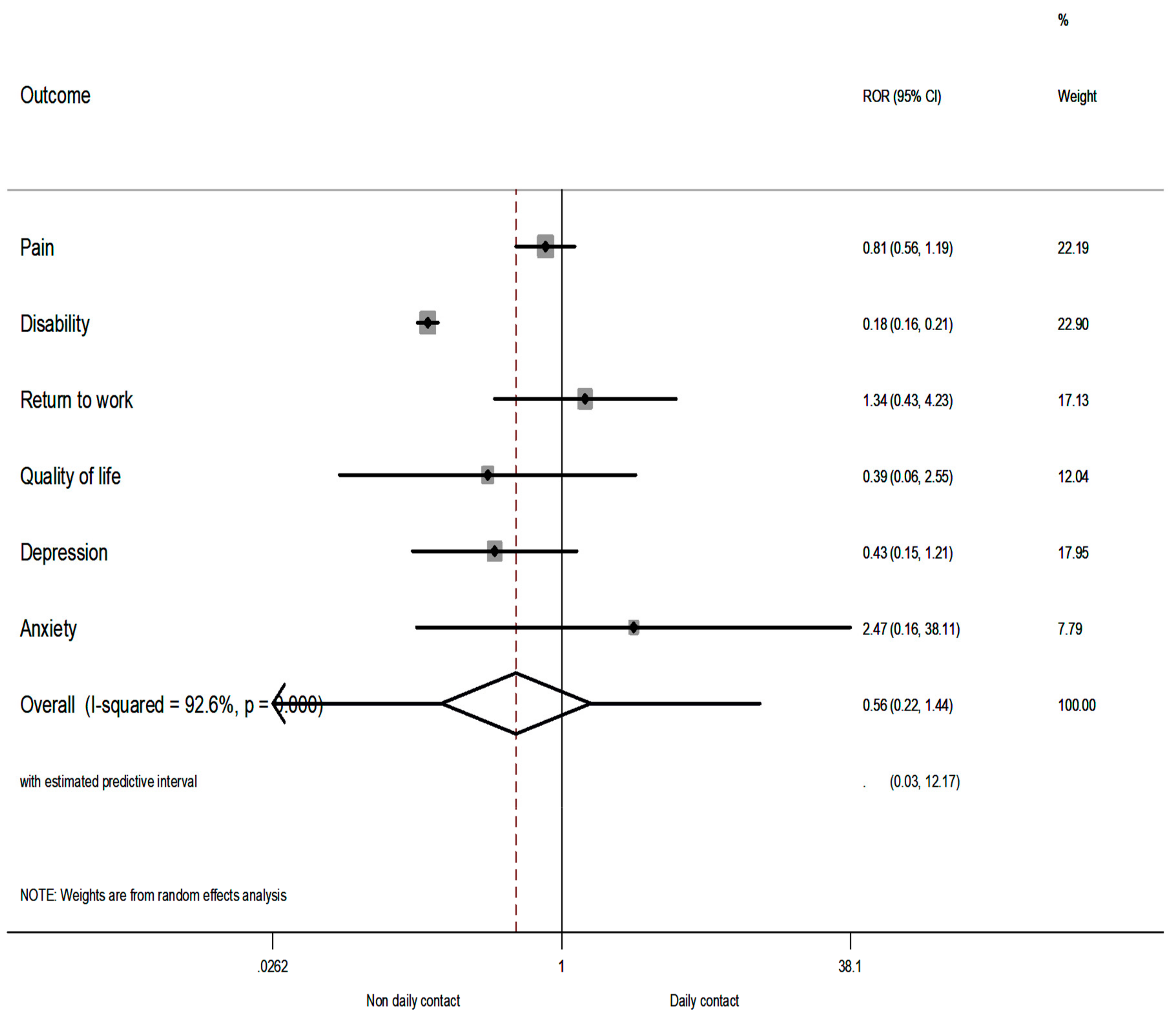
3.6. Comparison of Relative Odds Ratios
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Saragiotto, B.T.; de Almeida, M.O.; Yamato, T.P.; Maher, C.G. Multidisciplinary biopsychosocial rehabilitation for nonspecific chronic low back pain. Phys. Ther. 2016, 96, 759–763. [Google Scholar] [CrossRef] [PubMed]
- Kamper, S.J.; Apeldoorn, A.T.; Chiarotto, A.; Smeets, R.J.; Ostelo, R.W.; Guzman, J.; van Tulder, M.W. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain. Cochrane Database Syst. Rev. 2014, 9, CD000963. [Google Scholar] [CrossRef] [PubMed]
- Kamper, S.J.; Apeldoorn, A.T.; Chiarotto, A.; Smeets, R.J.; Ostelo, R.W.; Guzman, J.; van Tulder, M.W. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis. BMJ 2015, 350, h444. [Google Scholar] [CrossRef] [PubMed]
- Guzman, J.; Esmail, R.; Karjalainen, K.; Malmivaara, A.; Irvin, E.; Bombardier, C. Multidisciplinary bio-psycho-social rehabilitation for chronic low back pain. Cochrane Database Syst. Rev. 2002, 1, CD000963. [Google Scholar]
- Dragioti, E.; Evangelou, E.; Larsson, B.; Gerdle, B. Effectiveness of multidisciplinary programmes for clinical pain conditions: An umbrella review. J. Rehabil. Med. 2018, 50, 779–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scascighini, L.; Toma, V.; Dober-Spielmann, S.; Sprott, H. Multidisciplinary treatment for chronic pain: A systematic review of interventions and outcomes. Rheumatology (Oxford) 2008, 47, 670–678. [Google Scholar] [CrossRef]
- Lambeek, L.C.; van Tulder, M.W.; Swinkels, I.C.; Koppes, L.L.; Anema, J.R.; van Mechelen, W. The trend in total cost of back pain in The Netherlands in the period 2002 to 2007. Spine (Phila. Pa. 1976) 2011, 36, 1050–1058. [Google Scholar] [CrossRef] [PubMed]
- Reneman, M.F.; Waterschoot, F.P.C.; Bennen, E.; Schiphorst Preuper, H.R.; Dijkstra, P.U.; Geertzen, J.H.B. Dosage of pain rehabilitation programs: A qualitative study from patient and professionals’ perspectives. BMC Musculoskelet. Disord. 2018, 19, 206. [Google Scholar] [CrossRef]
- Reneman, M.F.; Waterschoot, F.P.C.; Burgerhof, J.G.M.; Geertzen, J.H.B.; Schiphorst Preuper, H.R.; Dijkstra, P.U. Dosage of pain rehabilitation programmes for patients with chronic musculoskeletal pain: A non-inferiority randomised controlled trial. Disabil. Rehabil. 2018, 18, 1–8. [Google Scholar] [CrossRef]
- Waterschoot, F.P.; Dijkstra, P.U.; Geertzen, J.H.; Reneman, M.F. Dose or content? Effectiveness of pain rehabilitation programs for patients with chronic low back pain: A systematic review. Aurthor reply. Pain 2014, 155, 1902–1903. [Google Scholar] [CrossRef]
- Chen, J.J. Outpatient pain rehabilitation programs. Iowa Orthop. J. 2006, 26, 102–106. [Google Scholar] [PubMed]
- Kaiser, U.; Treede, R.D.; Sabatowski, R. Multimodal pain therapy in chronic noncancer pain-gold standard or need for further clarification? Pain 2017, 158, 1853–1859. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Furlan, A.D.; Pennick, V.; Bombardier, C.; van Tulder, M.; Editorial Board, Cochrane Back Review Group. 2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine (Phila. Pa. 1976) 2009, 15, 1929–1941. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Thompson, S.G.; Higgins, J.P. How should meta-regression analyses be undertaken and interpreted? Stat. Med. 2002, 21, 1559–1573. [Google Scholar] [CrossRef]
- Sterne, J.A.; Juni, P.; Schulz, K.F.; Altman, D.G.; Bartlett, C.; Egger, M. Statistical methods for assessing the influence of study characteristics on treatment effects in ‘meta-epidemiological’ research. Stat. Med. 2002, 21, 1513–1524. [Google Scholar] [CrossRef]
- Dragioti, E.; Dimoliatis, I.; Fountoulakis, K.N.; Evangelou, E. A systematic appraisal of allegiance effect in randomized controlled trials of psychotherapy. Ann. Gen. Psychiatry 2015, 14, 25. [Google Scholar] [CrossRef] [Green Version]
- Evangelou, E.; Tsianos, G.; Ioannidis, J.P. Doctors’ versus patients’ global assessments of treatment effectiveness: Empirical survey of diverse treatments in clinical trials. BMJ 2008, 336, 1287–1290. [Google Scholar] [CrossRef] [PubMed]
- Chinn, S. A simple method for converting an odds ratio to effect size for use in meta-analysis. Stat. Med. 2000, 19, 3127–3131. [Google Scholar] [CrossRef]
- Altman, D.G.; Egger, M.; Smith, G.D. Systematic Reviews in Health Care: Meta-Analysis in Context, 2nd ed.; BMJ Publishing Group: London, UK, 2001. [Google Scholar]
- Henschke, N.; Maher, C.G.; Refshauge, K.M.; Herbert, R.D.; Cumming, R.G.; Bleasel, J.; York, J.; Das, A.; McAuley, J.H. Prognosis in patients with recent onset low back pain in Australian primary care: Inception cohort study. BMJ 2008, 337, a171. [Google Scholar] [CrossRef] [PubMed]
- Maetzel, A.; Li, L. The economic burden of low back pain: A review of studies published between 1996 and 2001. Best Pract. Res. Clin. Rheumatol. 2002, 16, 23–30. [Google Scholar] [CrossRef]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Oliveira, C.B.; Maher, C.G.; Pinto, R.Z.; Traeger, A.C.; Lin, C.C.; Chenot, J.F.; van Tulder, M.; Koes, B.W. Clinical practice guidelines for the management of non-specific low back pain in primary care: An updated overview. Eur. Spine J. 2018, 27, 2791–2803. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year * | Country | Sample Size | Female % | Mean Age (or Age Range) | Treatment | Control | Definition of Chronic LBP | Total Duration (Weeks) | Contact | Contact Duration (h/Week) | RoB Assessment |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Abbassi, 2012 | Iran | 33 | 88 | 45 | IMPT | TAU | LBP >6 months | 7 | Non-daily contact | 4 | Low risk |
| Alaranta, 1994 | Finland | 293 | 56 | 41 | IMPT | Physical | LBP >6 months | 6 | Daily contact | 100 | High risk |
| Altmaier, 1992 | USA | 45 | 73 | 40 | IMPT | Physical | LBP >3 months | 3 | Daily contact | 20 | High risk |
| Basler 1997 | Germany | 76 | 76 | 49 | IMPT | TAU | LBP >6 months | 12 | Non-daily contact | 2.5 | High risk |
| Bendix, 1996/1998 | Denmark | 106 | 70 | 40 | IMPT | TAU | LBP >6 months | 3 | Daily contact | 49 | High risk |
| Bendix, 1995/1998 | Denmark | 106 | 75 | 42 | IMPT | Physical | LBP >6 months | 4 | Daily contact | 45 | High risk |
| Bendix, 2000 | Denmark | 138 | 65 | 41 | IMPT | Physical | LBP >6 months | 4 | Daily contact | 45 | High risk |
| Coole, 2013 | UK | 51 | 53 | 44 | IMPT | Physical | LBP >3 months | 16 | Non-daily contact | 3 | High risk |
| Corey, 1996 | Canada | 138 | NR | NR | IMPT | TAU | LBP >3 months | 5 | Daily contact | 32.5 | High risk |
| Fairbank, 2005 | UK | 349 | 51 | 18–55 | IMPT | Surgery | LBP >1 year | 3 | Daily contact | 75 | Low risk |
| Harkapaa, 1989 | Finland | 309 | 37 | 45 | IMPT | Physical | LBP for >2 years | 3 | Daily contact | 100 | High risk |
| Hellum, 2011 | Norway | 173 | 51 | 41 | IMPT | Surgery | LBP >1 year | 5 | Non-daily contact | 12 | High risk |
| Henchoz, 2010 | Switzerland | 109 | 32 | 40 | IMPT | Physical | LBP >3 months | 3 | Non-daily contact | 30 | High risk |
| Jackel, 1990 | Germany | 71 | 62 | 49 | IMPT | WL | LBP >3 months | 6 | Daily contact | 36 | High risk |
| Jousset, 2004 | France | 84 | 33 | 40 | IMPT | Physical | LBP >3 months | 5 | Daily contact | 30 | High risk |
| Kaapa, 2006 | Finland | 120 | 100 | 46 | IMPT | Physical | LBP >1 year | 7 | Daily contact | 100 | Low risk |
| Kole-Snijders, 1999 | Netherlands | 148 | 64 | 40 | IMPT | WL | LBP >6 months | 8 | Daily contact | 13 | High risk |
| Kool, 2007 | Switzerland | 174 | 21 | 42 | IMPT | Physical | LBP >3 months | 3 | Non-daily contact | 24 | Low risk |
| Lambeek, 2010 | Netherlands | 134 | 42 | 18–65 | IMPT | TAU | LBP >3 months | 12 | Non-daily contact | 3 | Low risk |
| Leeuw, 2008 | Netherlands | 85 | 48 | 45 | IMPT | IMPT | LBP >3 months | 16 | Non-daily contact | 2 | Low risk |
| Linton, 2005 | Sweden | 185 | 83 | 49 | IMPT | TAU | NR | 6 | Non-daily contact | 2 | High risk |
| Lukinmaa, 1989 | Finland | 158 | 53 | 44 | IMPT | TAU | NR | 1 | Non-daily contact | 2.5 | High risk |
| Mangels, 2009 | Germany | 363 | 78 | 49 | IMPT | Physical | ICD 10 | 4 | Daily contact | 100 | Low risk |
| Meng, 2011 | Germany | 360 | 64 | 49 | IMPT | TAU/IMPT | ICD 10 | 7 | Non-daily contact | 1 | High risk |
| Mitchell, 1994 | Canada | 542 | 29 | nr | IMPT | TAU | NR | 8 | Daily contact | 35 | High risk |
| Moix, 2003 | Spain | 30 | 53 | 54 | IMPT | TAU | NR | 11 | Non-daily contact | 1 | High risk |
| Monticone, 2013 | Italy | 90 | 58 | 50 | IMPT | TAU | LBP >3 months | 5 | Non-daily contact | 3 | Low risk |
| Monticone, 2014 | Italy | 20 | NR | NR | IMPT | Physical | LBP >3 months | 8 | Non-daily contact | 3 | Low risk |
| Morone, 2011 | Italy | 73 | 64 | 60 | IMPT | TAU | LBP >3 months | 4 | Non-daily contact | 4 | High risk |
| Morone, 2012 | Italy | 75 | 72 | 55 | IMPT | TAU/ Physical | LBP >3 months | 4 | Non-daily contact | 4 | High risk |
| Nicholas, 1991 | Australia | 58 | 52 | 41 | IMPT | Physical | LBP >6 months | 5 | Non-daily contact | 3.5 | High risk |
| Nicholas, 1992 | Australia | 20 | 45 | 44 | IMPT | Physical | LBP >6 months | 5 | Non-daily contact | 3.5 | High risk |
| Roche, 2007/2011 | France | 132 | 35 | 40 | IMPT | Physical | LBP >3 months | 5 | Daily contact | 30 | Low risk |
| Smeets, 2006/2008 | Netherlands | 212 | 42 | 47 | IMPT | WL | LBP >3 months | 10 | Non-daily contact | 7.1 | Low risk |
| Skouen, 2002 | Norway | 195 | 44 | 43 | IMPT | TAU/IMPT | NR | 4 | Daily contact | 30 | High risk |
| Schweikert, 2006 | Germany | 409 | 17 | 47 | IMPT | Physical | LBP >6 months | 3 | Daily contact | 17.5 | High risk |
| Strand, 2001 | Norway | 117 | 61 | 43 | IMPT | TAU | ICPC diagnosis | 5 | Daily contact | 30 | High risk |
| Streibelt, 2009 | Germany | 222 | 17 | 46 | IMPT | Physical | NR | 3 | Non-daily contact | 20 | High risk |
| Tavafian, 2008 | Iran | 102 | 100 | 43 | IMPT | TAU | LBP >3 months | 1 | Non-daily contact | 5 | High risk |
| Tavafian, 2011 | Iran | 197 | 22 | 45 | IMPT | TAU | LBP >3 months | 1 | Non-daily contact | 10 | Low risk |
| Tavafian, 2014 | Iran | 178 | 75 | 44 | IMPT | TAU | LBP >3 months | 1 | Daily contact | 5 | High risk |
| Tavafian 2017 | Iran | 146 | 78 | 46 | IMPT | TAU | LBP >3 months | 1 | Daily contact | 5 | Low risk |
| Tavafian, 2017 | Iran | 165 | 79 | 45 | IMPT | TAU | LBP >3 months | 1 | Daily contact | 5 | Low risk |
| Turner, 1990 | USA | 96 | 49 | 44 | IMPT | Physical/ WL | LBP >6 months | 8 | Non-daily contact | 2 | High risk |
| Van den Hout, 2003 | Netherlands | 84 | 34 | 40 | IMPT | IMPT | LBP >6 months | 8 | Non-daily contact | 20 | High risk |
| Vollenbroek-Hutten, 2004 | Netherlands | 163 | NR | 39 | IMPT | TAU | LBP >6 months | 7 | Non-daily contact | 9 | Low risk |
| Von Korff, 2005 | USA | 240 | 63 | 50 | IMPT | TAU | score >7/23 on RMDQ | 1 | Non-daily contact | 3 | High risk |
| Short-Term Outcomes | No. of RCTs | Average Total Duration (Median Weeks, IQR) | Average h/Week (Median, IQR) | Level of Daily/Non-Daily Contact (n) | Level of Active (i.e., Physical)/Non-Active Control (i.e., WL/TAU) (n) | Level of Low Risk/High Risk of Bias (n) | Overall ES (95% CI) Random-Effects Model | p-Value | I2 (%; 95% CI) p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Outcome 1: Pain | |||||||||
| Length | |||||||||
| Short length (<5 weeks) | 12 | 3 (1–4) | 7.5 (4–22) | 8/4 | 6/6 | 3/9 | SMD, −0.33 (−0.55 to −0.11) | 0.003 | 81 (67–88) 0.000 |
| Long length (≥5 weeks) | 16 | 8 (5.5–10) | 3.5 (2.7–10) | 4/12 | 8/8 | 8/8 | SMD, −0.45 (−0.73 to −0.17) | 0.001 | 79 (64–85) 0.000 |
| Contact | |||||||||
| Non-daily contact | 16 | 7.5 (4.5–10) | 3.3 (2.7–4) | 0/16 | 7/9 | 6/10 | SMD, −0.50 (−0.79 to −0.20) | 0.001 | 80 (67–86) 0.000 |
| Daily contact | 12 | 3 (2–5.5) | 22 (11.5–68) | 12/0 | 7/5 | 5/7 | SMD, -0.29 (−0.49 to −0.09) | 0.005 | 78 (59–86) 0.000 |
| Intensity | |||||||||
| <30 h per week | 23 | 5 (3–8) | 4 (3–7.1) | 7/16 | 10/13 | 8/15 | SMD, −0.42 (−0.62 to −0.20) | <0.000 | 81 (71–86) 0.000 |
| >30 h per week | 5 | 5 (4–6) | 100 (36–100) | 5/0 | 4/1 | 3/2 | SMD, −0.32 (−0.63 to −0.05) | 0.022 | 79 (31–89) 0.001 |
| Outcome 2: Disability | |||||||||
| Length | |||||||||
| Short length (<5 weeks) | 10 | 3 (1–4) | 7.5 (4–30) | 5/5 | 5/5 | 2/8 | SMD, −0.27 (−0.48 to −0.07) | 0.007 | 75 (47–85) 0.000 |
| Long length (≥5 weeks) | 17 | 7 (6–10) | 3.5 (3–9) | 4/13 | 9/8 | 9/8 | SMD, −0.51 (−0.78 to −0.24) | <0.000 | 82 (73–88) 0.000 |
| Contact | |||||||||
| Non-daily contact | 18 | 7 (4–10) | 3.5 (3–4) | 0/18 | 8/10 | 7/11 | SMD, −0.58 (−0.86 to −0.31) | <0.000 | 81 (70–87) 0.000 |
| Daily contact | 9 | 4 (1–3) | 36 (18–100) | 9/0 | 6/3 | 4/5 | SMD, −0.16 (−0.33–0.01) | 0.055 | 67 (16–82) 0.002 |
| Intensity | |||||||||
| <30 h per week | 20 | 6 (4–9) | 3.8 (3–6) | 3/17 | 8/12 | 8/12 | SMD, −0.49 (−0.74 to −0.24) | <0.000 | 85 (78–89) 0.000 |
| >30 h per week | 7 | 5 (3–6) | 100 (30–100) | 6/1 | 6/1 | 3/4 | SMD, −0.26 (−0.43 to −0.09) | 0.003 | 54 (0–78) 0.043 |
| Outcome 3: Return to work | |||||||||
| Length | |||||||||
| Short length (<5 weeks) | 3 | 3 (1–4) | 24 (3–30) | 2/1 | 1/2 | 1/2 | OR, 1.46 (0.82–2.62) | 0.199 | 42 (0–83) 0.177 |
| Long length (≥5 weeks) | 2 | 5 (5–5) | 30 (30–30) | 2/0 | 2/0 | 1/1 | OR, 1.10 (0.55–2.20) | 0.786 | 0 (NA) # 0.938 |
| Contact | |||||||||
| Non-daily contact | 1 | 1 (1–1) | 3 (3–3) | 0/1 | 0/1 | 0/1 | OR, 0.91 (0.31–2.68) | 0.864 | NA |
| Daily contact | 4 | 4.5 (3.5–5) | 30 (27–30) | 4/0 | 1/3 | 2/2 | OR, 1.46 (0.96–2.21) | 0.075 | 12 (0–72) 0.332 |
| Intensity | |||||||||
| <30 h per week | 2 | 2 (1–3) | 13.5 (3–24) | 1/1 | 1/1 | 1/1 | OR, 1.63 (0.65–4.09) | 0.297 | 56 (NA) # 0.133 |
| >30 h per week | 3 | 5 (4–5) | 30 (30–30) | 3/0 | 2/1 | 1/2 | OR, 1.12 (0.69–1.82) | 0.645 | 0 (0–73) 0.994 |
| Outcome 4: Quality of life | |||||||||
| Length | |||||||||
| Short length (<5 weeks) | 8 | 1.5 (1–3.5) | 7.5 (4–13.7) | 5/3 | 3/5 | 2/6 | SMD, 0.49 (0.14–0.84) | 0.006 | 83 (65–90) 0.000 |
| Long length (≥5 weeks) | 1 | 10 (10–10) | 7.1 (7.1–7.1) | 0/1 | 1/0 | 1/0 | SMD, 0.14 (−0.24–0.52) | 0.470 | NA |
| Contact | |||||||||
| Non-daily contact | 4 | 4 (1–10) | 4 (3–7.1) | 0/4 | 2/2 | 2/2 | SMD, 0.53 (0.09–0.98) | 0.019 | 64 (0–86) 0.038 |
| Daily contact | 5 | 1.5 (1–3) | 10 (5–18) | 5/0 | 2/3 | 1/4 | SMD, 0.38 (−0.06–0.81) | 0.089 | 88 (70–93) 0.000 |
| Intensity | |||||||||
| <30 h per week | 8 | 2 (1–4)) | 6 (4–10) | 4/4 | 3/5 | 2/6 | SMD, 0.54 (0.25–0.83) | <0.000 | 75 (38–86) 0.000 |
| >30 h per week | 1 | 2 (2–2) | 100 (100–100) | 1/0 | 1/0 | 1/0 | SMD, −0.38 (−0.74 to −0.02) | 0.041 * | NA |
| Outcome 5: Depression | |||||||||
| Length | |||||||||
| Short length (<5 weeks) | 2 | 3.5 (3–4) | 58.8 (17.5–100) | 2/0 | 2/0 | 1/1 | SMD, 0.08 (−0.22–0.39) | 0.584 | 71 (NA)# 0.063 |
| Long length (≥5 weeks) | 8 | 7.5 (5.5–9) | 5.3 (2.8–21.5) | 2/6 | 5/3 | 3/5 | SMD, −0.09 (−0.29–0.11) | 0.358 | 20 (0–64) 0.273 |
| Contact | |||||||||
| Non-daily contact | 6 | 8 (5–10) | 3.5 (2–7.1) | 0/6 | 4/2 | 2/4 | SMD, 0.01 (−0.21–0.22) | 0.959 | 0 (0–61) 0.562 |
| Daily contact | 4 | 5 (3.5–6.5) | 68 (26.8–100) | 4/0 | 3/1 | 2/2 | SMD, −0.07 (−0.35–0.22) | 0.653 | 72 (0–88) 0.013 |
| Intensity | |||||||||
| <30 h per week | 7 | 8 (5–10) | 7.1 (2–17.5) | 2/5 | 4/3 | 2/5 | SMD, 0.12 (−0.03–0.27) | 0.119 | 1 (0–59) 0.414 |
| >30 h per week | 3 | 5 (4–7) | 100 (3.5–100) | 2/1 | 3/0 | 2/1 | SMD, −0.18 (−0.46–0.10) | 0.202 | 46 (0–84) 0.155 |
| Outcome 6: Anxiety | |||||||||
| Length | |||||||||
| Short length (<5 weeks) | 1 | 3 (3–3) | 17.5 (17.5–17.5) | 1/0 | 1/0 | 0/1 | SMD, 0.08 (−0.13–0.29) | 0.455 | NA |
| Long length (≥5 weeks) | 1 | 5 (5–5) | 3.5 (3.5–3.5) | 0/1 | 1/0 | 0/1 | SMD, −0.58 (−1.48–0.32) | 0.209 | NA |
| Contact | |||||||||
| Non-daily contact | 1 | 5 (5–5) | 3.5 (3.5–3.5) | 0/1 | 1/0 | 0/1 | SMD, −0.58 (−1.48–0.32) | 0.209 | NA |
| Daily contact | 1 | 3 (3–3) | 17.5 (17.5–17.5) | 1/0 | 1/0 | 0/1 | SMD, 0.08 (−0.13–0.29) | 0.455 | NA |
| Intensity | |||||||||
| <30 h per week | 2 | 4 (3–5) | 10.5 (3.5–17.5) | 1/1 | 2/0 | 0/2 | SMD, −0.10 (−0.67–0.48) | 0.740 | 48 (NA) # 0.164 |
| >30 h per week | 0 | 0 (0–0) | 0 (0–0) | 0/0 | 0/0 | 0/0 | NA | NA | NA |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dragioti, E.; Björk, M.; Larsson, B.; Gerdle, B. A Meta-Epidemiological Appraisal of the Effects of Interdisciplinary Multimodal Pain Therapy Dosing for Chronic Low Back Pain. J. Clin. Med. 2019, 8, 871. https://doi.org/10.3390/jcm8060871
Dragioti E, Björk M, Larsson B, Gerdle B. A Meta-Epidemiological Appraisal of the Effects of Interdisciplinary Multimodal Pain Therapy Dosing for Chronic Low Back Pain. Journal of Clinical Medicine. 2019; 8(6):871. https://doi.org/10.3390/jcm8060871
Chicago/Turabian StyleDragioti, Elena, Mathilda Björk, Britt Larsson, and Björn Gerdle. 2019. "A Meta-Epidemiological Appraisal of the Effects of Interdisciplinary Multimodal Pain Therapy Dosing for Chronic Low Back Pain" Journal of Clinical Medicine 8, no. 6: 871. https://doi.org/10.3390/jcm8060871