Effects of Bilateral Infraorbital and Infratrochlear Nerve Block on Emergence Agitation after Septorhinoplasty: A Randomized Controlled Trial

 ,
,
Abstract
:1. Introduction
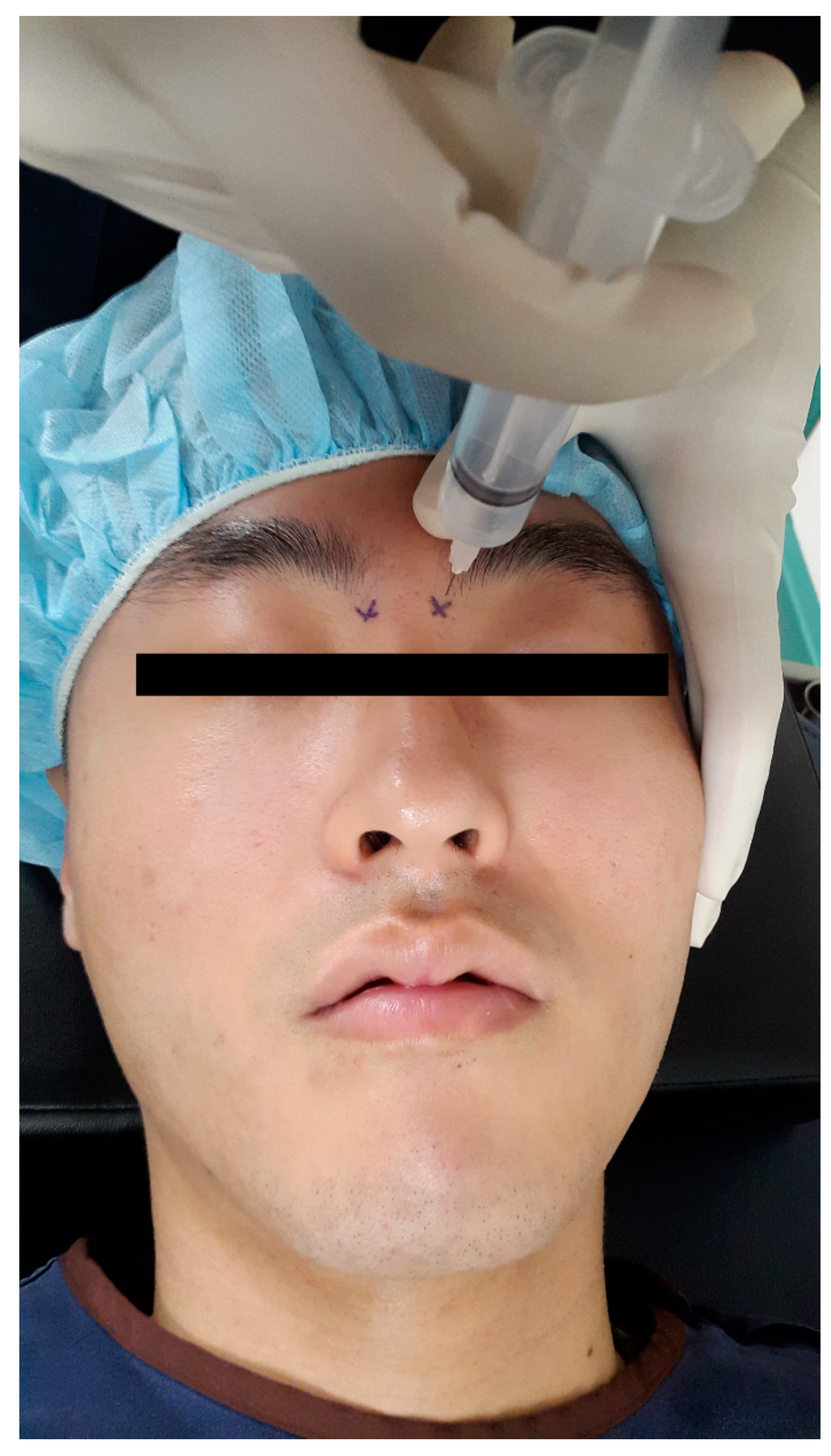
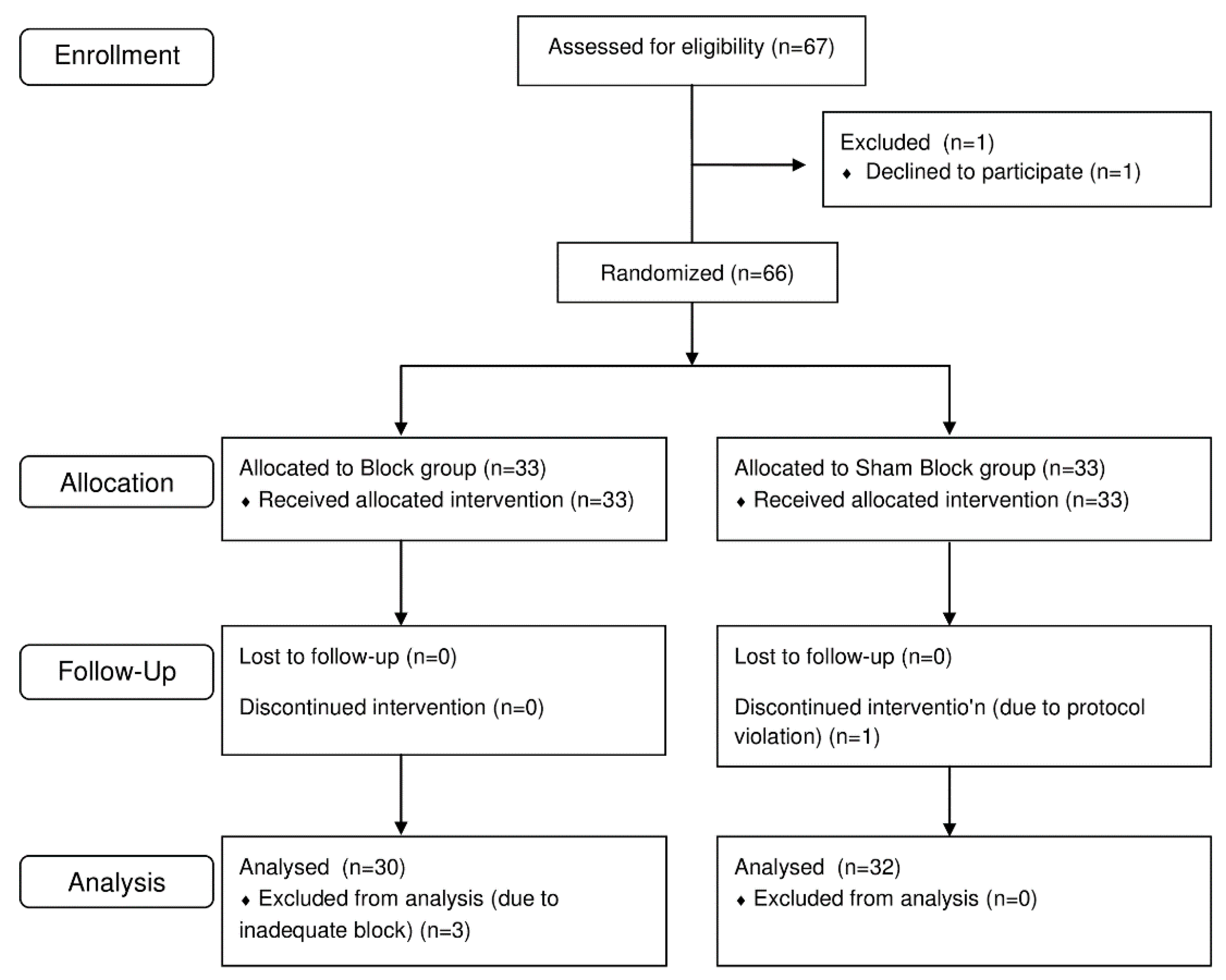
2. Materials and Methods
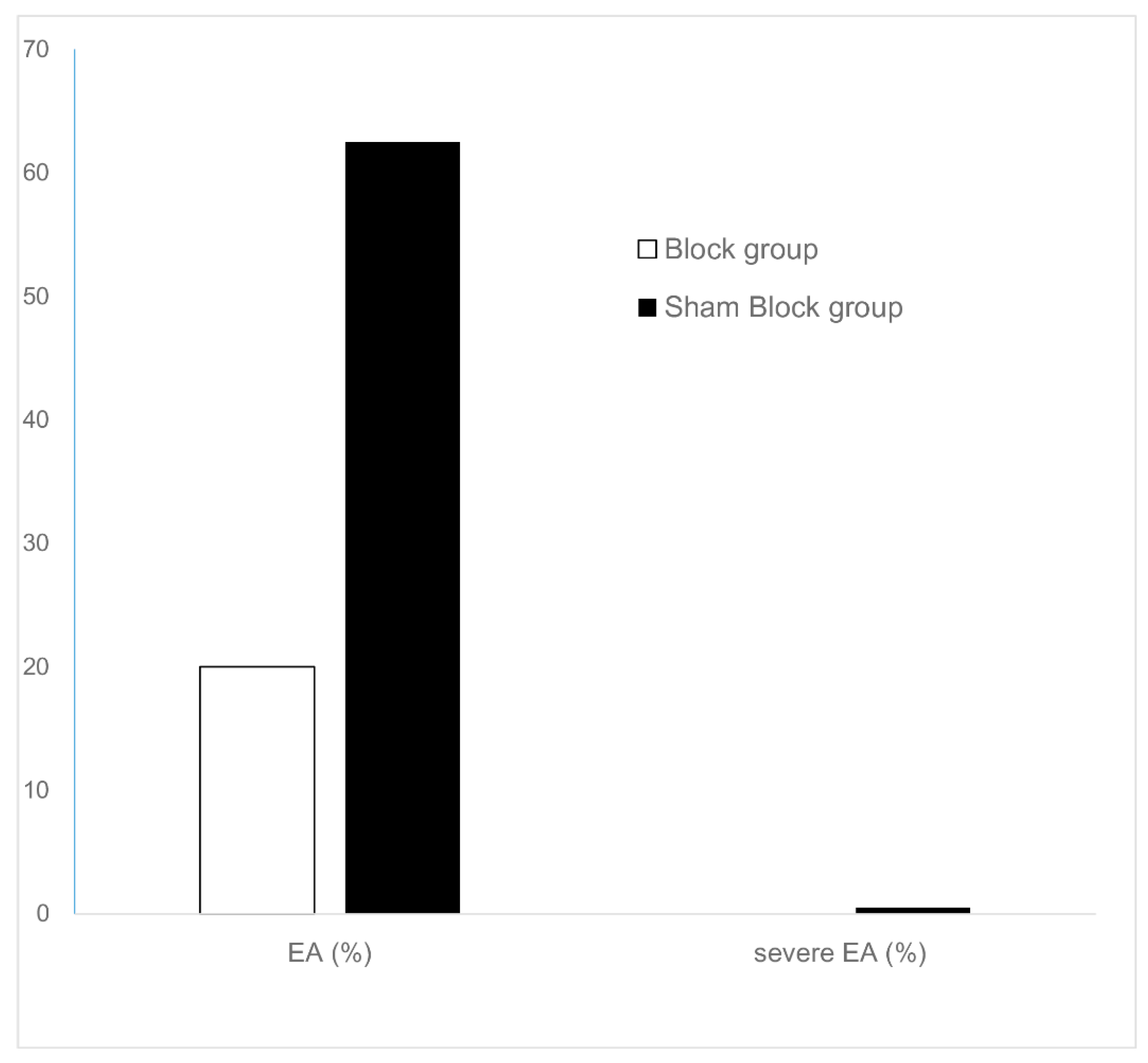
3. Results
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Lepouse, C.; Lautner, C.A.; Liu, L.; Gomis, P.; Leon, A. Emergence delirium in adults in the post-anaesthesia care unit. Br. J. Anaesth. 2006, 96, 747–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vlajkovic, G.P.; Sindjelic, R.P. Emergence delirium in children: Many questions, few answers. Anesth. Analg. 2007, 104, 84–91. [Google Scholar] [CrossRef]
- Hudek, K. Emergence delirium: A nursing perspective. AORN J. 2009, 89, 509–516. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, D.K.; Kim, H.Y.; Kim, J.K.; Choi, S.W. Risk factors of emergence agitation in adults undergoing general anesthesia for nasal surgery. Clin. Exp. Otorhinolaryngol. 2015, 8, 46–51. [Google Scholar] [CrossRef]
- Yu, D.; Chai, W.; Sun, X.; Yao, L. Emergence agitation in adults: Risk factors in 2000 patients. Can. J. Anaesth. 2010, 57, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Gerbershagen, H.J.; Aduckathil, S.; van Wijck, A.J.; Peelen, L.M.; Kalkman, C.J.; Meissner, W. Pain intensity on the first day after surgery: A prospective cohort study comparing 179 surgical procedures. Anesthesiology 2013, 118, 934–944. [Google Scholar] [CrossRef]
- Wittekindt, D.; Wittekindt, C.; Schneider, G.; Meissner, W.; Guntinas-Lichius, O. Postoperative pain assessment after septorhinoplasty. Eur. Arch. Otorhinolaryngol. 2012, 269, 1613–1621. [Google Scholar] [CrossRef] [PubMed]
- Jeffrey, L.A.; Michael, A.A.; Richard, T.C.; Tong, J.G.; David, G.N. Practice guidelines for acute pain management in the perioperative setting: An updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology 2012, 116, 248–273. [Google Scholar] [CrossRef]
- Joshi, G.P. Putting it all together: Recommendations for improving pain management in plastic surgical procedures. Plast. Reconstr. Surg. 2014, 134, 94s–100s. [Google Scholar] [CrossRef] [PubMed]
- Kanakaraj, M.; Shanmugasundaram, N.; Chandramohan, M.; Kannan, R.; Perumal, S.M.; Nagendran, J. Regional anesthesia in faciomaxillary and oral surgery. J. Pharm. Bioallied Sci. 2012, 4, S264–S269. [Google Scholar] [CrossRef]
- Moskovitz, J.B.; Sabatino, F. Regional nerve blocks of the face. Emerg. Med. Clin. N. Am. 2013, 31, 517–527. [Google Scholar] [CrossRef]
- Boselli, E.; Bouvet, L.; Augris-Mathieu, C.; Begou, G.; Diot-Junique, N.; Rahali, N.; Vertu-Ciolino, D.; Gerard, C.; Pivot, C.; Disant, F.; et al. Infraorbital and infratrochlear nerve blocks combined with general anaesthesia for outpatient rhinoseptoplasty: A prospective randomised, double-blind, placebo-controlled study. Anaesth. Crit. Care Pain Med. 2015. [Google Scholar] [CrossRef]
- Cekic, B.; Geze, S.; Erturk, E.; Akdogan, A.; Eroglu, A. A comparison of levobupivacaine and levobupivacaine-tramadol combination in bilateral infraorbital nerve block for postoperative analgesia after nasal surgery. Ann. Plast. Surg. 2013, 70, 131–134. [Google Scholar] [CrossRef]
- Higashizawa, T.; Koga, Y. Effect of infraorbital nerve block under general anesthesia on consumption of isoflurane and postoperative pain in endoscopic endonasal maxillary sinus surgery. J. Anesth. 2001, 15, 136–138. [Google Scholar] [CrossRef]
- Mariano, E.R.; Watson, D.; Loland, V.J.; Chu, L.F.; Cheng, G.S.; Mehta, S.H.; Maldonado, R.C.; Ilfeld, B.M. Bilateral infraorbital nerve blocks decrease postoperative pain but do not reduce time to discharge following outpatient nasal surgery. Can. J. Anaesth. 2009, 56, 584–589. [Google Scholar] [CrossRef] [Green Version]
- Molliex, S.; Navez, M.; Baylot, D.; Prades, J.M.; Elkhoury, Z.; Auboyer, C. Regional anaesthesia for outpatient nasal surgery. Br. J. Anaesth. 1996, 76, 151–153. [Google Scholar] [CrossRef]
- Kim, J.; Shin, W. How to do random allocation (randomization). Clin. Orthop. Surg. 2014, 6, 103–109. [Google Scholar] [CrossRef]
- Karkut, B.; Reader, A.; Drum, M.; Nusstein, J.; Beck, M. A comparison of the local anesthetic efficacy of the extraoral versus the intraoral infraorbital nerve block. J. Am. Dent. Assoc. (1939) 2010, 141, 185–192. [Google Scholar] [CrossRef]
- Saeedi, O.J.; Wang, H.; Blomquist, P.H. Penetrating globe injury during infraorbital nerve block. Arch. Otolaryngol. Head Neck Surg. 2011, 137, 396–397. [Google Scholar] [CrossRef]
- Beck, D.O.; Kenkel, J.M. Evidence-based medicine: Rhinoplasty. Plast. Reconstr. Surg. 2014, 134, 1356–1371. [Google Scholar] [CrossRef]
- Gun, R.; Yorgancilar, E.; Yildirim, M.; Bakir, S.; Topcu, I.; Akkus, Z. Effects of lidocaine and adrenaline combination on postoperative edema and ecchymosis in rhinoplasty. Int. J. Oral Maxillofac. Surg. 2011, 40, 722–729. [Google Scholar] [CrossRef]
- Riker, R.R.; Picard, J.T.; Fraser, G.L. Prospective evaluation of the Sedation-Agitation Scale for adult critically ill patients. Crit. Care Med. 1999, 27, 1325–1329. [Google Scholar] [CrossRef]
- Somaini, M.; Engelhardt, T.; Fumagalli, R.; Ingelmo, P.M. Emergence delirium or pain after anaesthesia–how to distinguish between the two in young children: A retrospective analysis of observational studies. Br. J. Anaesth. 2016, 116, 377–383. [Google Scholar] [CrossRef]
- Myles, P.S.; Myles, D.B.; Galagher, W.; Boyd, D.; Chew, C.; MacDonald, N.; Dennis, A. Measuring acute postoperative pain using the visual analog scale: The minimal clinically important difference and patient acceptable symptom state. Br. J. Anaesth. 2017, 118, 424–429. [Google Scholar] [CrossRef]
- Bortone, L.; Bertolizio, G.; Engelhardt, T.; Frawley, G.; Somaini, M.; Ingelmo, P.M. The effect of fentanyl and clonidine on early postoperative negative behavior in children: A double-blind placebo controlled trial. Paediatr. Anaesth. 2014, 24, 614–619. [Google Scholar] [CrossRef]
- Abu-Shahwan, I.; Chowdary, K. Ketamine is effective in decreasing the incidence of emergence agitation in children undergoing dental repair under sevoflurane general anesthesia. Paediatr. Anaesth. 2007, 17, 846–850. [Google Scholar] [CrossRef]
- Chen, J.Y.; Jia, J.E.; Liu, T.J.; Qin, M.J.; Li, W.X. Comparison of the effects of dexmedetomidine, ketamine, and placebo on emergence agitation after strabismus surgery in children. Can. J. Anaesth. 2013, 60, 385–392. [Google Scholar] [CrossRef] [Green Version]
- Fang, X.Z.; Gao, J.; Ge, Y.L.; Zhou, L.J.; Zhang, Y. Network Meta-Analysis on the Efficacy of Dexmedetomidine, Midazolam, Ketamine, Propofol, and Fentanyl for the Prevention of Sevoflurane-Related Emergence Agitation in Children. Am. J. Ther. 2016, 23, e1032–1042. [Google Scholar] [CrossRef]
- Nakayama, S.; Furukawa, H.; Yanai, H. Propofol reduces the incidence of emergence agitation in preschool-aged children as well as in school-aged children: A comparison with sevoflurane. J. Anesth. 2007, 21, 19–23. [Google Scholar] [CrossRef]
- Badawy, A.A.; Kasem, S.A.; Rashwan, D.; Al Menesy, T.; Adel, G.; Mokhtar, A.M.; Badawy, Y.A. The role of Gabapentin oral solution in decreasing desflurane associated emergence agitation and delirium in children after stabismus surgery, a prospective randomized double-blind study. BMC Anesth. 2018, 18, 73. [Google Scholar] [CrossRef]
- Marouf, H.M. Effect of Pregabalin Premedication on Emergence Agitation in Children after Sevoflurane Anesthesia: A Randomized Controlled Study. Anesth. Essays Res. 2018, 12, 31–35. [Google Scholar] [CrossRef]
- Demir, C.Y.; Yuzkat, N. Prevention of Emergence Agitation with Ketamine in Rhinoplasty. Aesthet. Plast. Surg. 2018, 42, 847–853. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, J.M.; Lee, J.H.; Song, B.M.; Koo, B.N. Efficacy of intraoperative dexmedetomidine infusion on emergence agitation and quality of recovery after nasal surgery. Br. J. Anaesth. 2013, 111, 222–228. [Google Scholar] [CrossRef] [Green Version]
- Liang, C.; Ding, M.; Du, F.; Cang, J.; Xue, Z. Sevoflurane/propofol coadministration provides better recovery than sevoflurane in combined general/epidural anesthesia: A randomized clinical trial. J. Anesth. 2014, 28, 721–726. [Google Scholar] [CrossRef]
- Aouad, M.T.; Kanazi, G.E.; Siddik-Sayyid, S.M.; Gerges, F.J.; Rizk, L.B.; Baraka, A.S. Preoperative caudal block prevents emergence agitation in children following sevoflurane anesthesia. Acta Anaesthesiol. Scand. 2005, 49, 300–304. [Google Scholar] [CrossRef]
- Kim, H.S.; Kim, C.S.; Kim, S.D.; Lee, J.R. Fascia iliaca compartment block reduces emergence agitation by providing effective analgesic properties in children. J. Clin. Anesth. 2011, 23, 119–123. [Google Scholar] [CrossRef]
- Wang, H.; Liu, G.; Fu, W.; Li, S.T. The effect of infraorbital nerve block on emergence agitation in children undergoing cleft lip surgery under general anesthesia with sevoflurane. Paediatr. Anaesth. 2015, 25, 906–910. [Google Scholar] [CrossRef]
- Riker, R.R.; Fraser, G.L.; Simmons, L.E.; Wilkins, M.L. Validating the Sedation-Agitation Scale with the Bispectral Index and Visual Analog Scale in adult ICU patients after cardiac surgery. Intensiv. Care Med. 2001, 27, 853–858. [Google Scholar] [CrossRef]
- Sessler, C.N.; Gosnell, M.S.; Grap, M.J.; Brophy, G.M.; O’Neal, P.V.; Keane, K.A.; Tesoro, E.P.; Elswick, R.K. The Richmond Agitation-Sedation Scale: Validity and reliability in adult intensive care unit patients. Am. J. Respire. Crit. Care Med. 2002, 166, 1338–1344. [Google Scholar] [CrossRef]
- Polat, R.; Peker, K.; Baran, I.; Bumin Aydin, G.; Topcu Guloksuz, C.; Donmez, A. Comparison between dexmedetomidine and remifentanil infusion in emergence agitation during recovery after nasal surgery: A randomized double-blind trial. Der Anaesth. 2015, 64, 740–746. [Google Scholar] [CrossRef]
- Michalek, P.; Donaldson, W.; McAleavey, F.; Johnston, P.; Kiska, R. Ultrasound imaging of the infraorbital foramen and simulation of the ultrasound-guided infraorbital nerve block using a skull model. Surg. Radiol. Anat. 2013, 35, 319–322. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Block Group (n = 30) | Sham Block Group (n = 32) | p Value | |
|---|---|---|---|
| Age (year) | 21.97 ± 1.474 | 22.38 ± 3.077 | 0.512 |
| Height (cm) | 174.5 ± 5.1 | 175.6 ± 5.6 | 0.411 |
| Weight (kg) | 69.8 ± 8.2 | 69.9 ± 8.3 | 0.935 |
| BMI (kg/m2) | 22.9 ± 2.3 | 22.6 ± 2.2 | 0.659 |
| History of smoking | 18 (60.0%) | 24 (75.0%) | 0.322 |
| ASA Class | 0.072 | ||
| I | 20 (66.7%) | 13 (40.6%) | |
| II | 10 (33.3%) | 19 (59.4%) | |
| Duration of surgery (min) | 95.5 ± 15.3 | 99.6 ± 14.5 | 0.288 |
| Duration of anesthesia (min) | 113.7 ± 15.5 | 120.3 ± 15.3 | 0.093 |
| Remifentanil consumption (μg/kg/min) | 0.074 ± 0.014 | 0.093 ± 0.019 | <0.0001 |
| Mean blood pressure (mmHg) | 0.258 | ||
| Baseline | 97.0 ± 6.7 | 93.4 ± 7.4 | 0.051 |
| Skin incision | 83.1 ± 7.2 | 84.6 ± 10.2 | 0.518 |
| During surgery | 74.1 ± 6.7 | 72.6 ± 6.2 | 0.370 |
| Skin closure | 76.9 ± 7.7 | 74.4 ± 8.1 | 0.227 |
| Heart rate (beats/min) | 0.670 | ||
| Baseline | 71.2 ± 9.4 | 70.1 ± 9.8 | 0.661 |
| Skin incision | 67.9 ± 9.2 | 70.7 ± 11.3 | 0.302 |
| During surgery | 63.4 ± 8.7 | 62.1 ± 6.5 | 0.484 |
| Skin closure | 66.6 ± 8.5 | 63.4 ± 7.0 | 0.109 |
| Block Group (n = 30) | Sham Block Group (n = 32) | p Value | |
|---|---|---|---|
| Tramadol use | 9 (30.0%) | 21 (65.6%) | 0.011 |
| Pethidine use | 0 (0.0%) | 2 (6.2%) | 0.501 |
| Pain score (in NRS) | 0.003 | ||
| 0–2 h | 3.0 (2.0–4.0) | 4.0 (3.0–4.0) | <0.0001 |
| 2–8 h | 2.0 (2.0–2.0) | 2.0 (2.0–3.0) | 0.680 |
| 8–24 h | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 0.384 |
| 24–48 h | 0.0 (0.0–1.0) | 0.5 (0.0–1.0) | 0.256 |
| Adverse events | |||
| Neurologic deficit in PACU | 0 | 0 | |
| Neurologic deficit after 24 h | 0 | 0 | |
| Edema in PACU | 4 (13.3%) | 5 (15.6%) | 1.000 |
| Edema after 24 h | 3 (10.0%) | 4 (12.5%) | 1.000 |
| Hematoma in PACU | 3 (10.0%) | 3 (9.4%) | 1.000 |
| Hematoma after 24 h | 3 (10.0%) | 2 (6.3%) | 0.940 |
| PONV in PACU | 4 (13.3%) | 4 (12.5%) | 1.000 |
| PONV after 24 h | 1 (3.3%) | 0 (0.0%) | 0.974 |
| Patient satisfaction score | 3.5 (3.0–4.0) | 3.0 (3.0–4.0) | 0.034 |
| Odds Ratio | Confidence Interval | p Value | |
|---|---|---|---|
| NRS > 3 at 0–2 h | 16.50 | 4.47–60.87 | <0.0001 |
| Received sham block | 6.67 | 2.12–20.96 | 0.001 |
| History of smoking | 2.12 | 0.68–6.58 | 0.189 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, H.; Jung, S.H.; Hong, J.M.; Joo, Y.H.; Kim, Y.; Hong, S.H. Effects of Bilateral Infraorbital and Infratrochlear Nerve Block on Emergence Agitation after Septorhinoplasty: A Randomized Controlled Trial. J. Clin. Med. 2019, 8, 769. https://doi.org/10.3390/jcm8060769
Choi H, Jung SH, Hong JM, Joo YH, Kim Y, Hong SH. Effects of Bilateral Infraorbital and Infratrochlear Nerve Block on Emergence Agitation after Septorhinoplasty: A Randomized Controlled Trial. Journal of Clinical Medicine. 2019; 8(6):769. https://doi.org/10.3390/jcm8060769
Chicago/Turabian StyleChoi, Hoon, Seung Ho Jung, Jin Myung Hong, Young Ho Joo, Youme Kim, and Sang Hyun Hong. 2019. "Effects of Bilateral Infraorbital and Infratrochlear Nerve Block on Emergence Agitation after Septorhinoplasty: A Randomized Controlled Trial" Journal of Clinical Medicine 8, no. 6: 769. https://doi.org/10.3390/jcm8060769