Galectin 3 and Galectin 3 Binding Protein Improve the Risk Stratification after Myocardial Infarction

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Definitions, Endpoints, and Follow-Up
2.3. Measurements of Biomarkers
2.4. Statistical Analysis
3. Results
3.1. Study Population
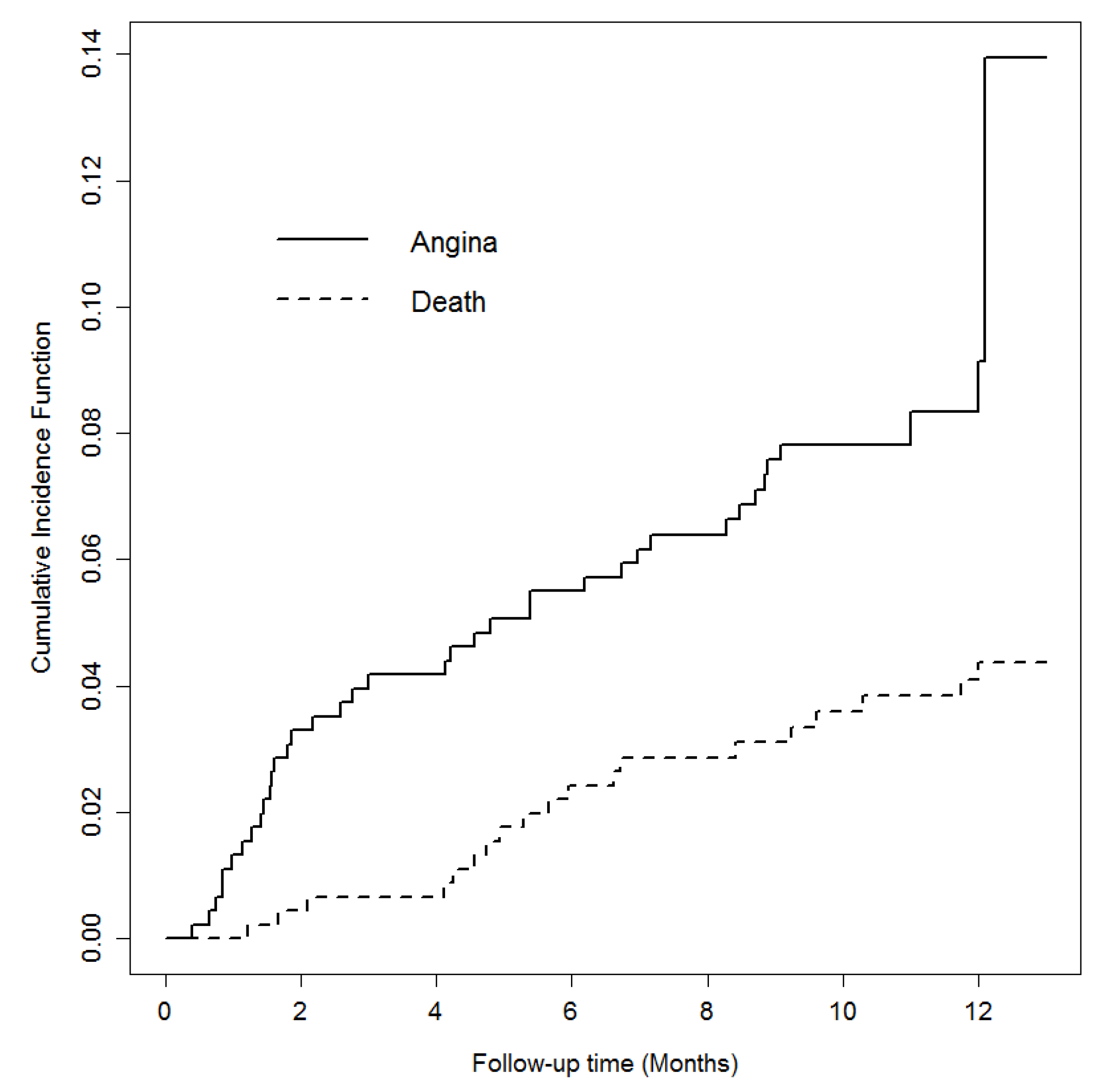
3.2. Outcome During the Follow-Up
3.2.1. Angina and Reinfarction during Follow-Up
3.2.2. Mortality during Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- The Top 10 Causes of Death. Available online: http://www.who.int/en/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 26 July 2018).
- Rosamond, W.D.; Chambless, L.E.; Folsom, A.R.; Cooper, L.S.; Conwill, D.E.; Clegg, L.; Wang, C.H.; Heiss, G. Trends in the Incidence of Myocardial Infarction and in mortality due to coronary heart disease, 1987 to 1994. N. Engl. J. Med. 1998, 33, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Altay, S.; Çakmak, H.A.; Kemaloğlu Öz, T.; Özpamuk Karadeniz, F.; Türer, A.; Erer, H.B.; Kılıç, G.F.; Keleş, İ.; Can, G.; Eren, M. Long-term prognostic significance of pentraxin-3 in patients with acute myocardial infarction: 5-year prospective cohort study. Anatol. J. Cardiol. 2017, 17, 202–209. [Google Scholar] [CrossRef]
- O’Donoghue, M.L.; Morrow, D.A.; Cannon, C.P.; Jarolim, P.; Desai, N.R.; Sherwood, M.W.; Murphy, S.A.; Gerszten, R.E.; Sabatine, M.S. Multimarker Risk Stratification in Patients with Acute Myocardial Infarction. J. Am. Heart. Assoc. 2016, 5. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Morrow, D.A.; De Lemos, J.A.; Gibson, C.M.; Murphy, S.A.; Rifai, N.; McCabe, C.; Antman, E.M.; Cannon, C.P.; Braunwald, E. Multimarker approach to risk stratification in non-ST elevation acute coronary syndromes: Simultaneous assessment of troponin I, C-reactive protein, and B-type natriuretic peptide. Circulation 2002, 105, 1760–1763. [Google Scholar] [CrossRef]
- Oemrawsingh, R.M.; Lenderink, T.; Akkerhuis, K.M.; Heeschen, C.; Baldus, S.; Fichtlscherer, S.; Hamm, C.W.; Simoons, M.L.; Boersma, E. Multimarker risk model containing troponin-T, interleukin 10, myeloperoxidase and placental growth factor predicts long-term cardiovascular risk after non-ST-segment elevation acute coronary syndrome. Heart 2011, 97, 1061–1066. [Google Scholar] [CrossRef] [Green Version]
- Agnello, L.; Bivona, G.; Sasso B, L.o.; Scazzone, C.; Bazan, V.; Bellia, C.; Ciaccio, M. Galectin-3 in acute coronary syndrome. Clin. Biochem. 2017, 50, 797–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugiura, T.; Dohi, Y.; Takase, H.; Yamashita, S.; Murai, S.; Tsuzuki, Y.; Ogawa, S.; Tanaka, Y.; Ohte, N. Serum levels of Mac-2 binding protein increase with cardiovascular risk and reflect silent atherosclerosis. Atherosclerosis 2016, 251, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, W.S.; Roger, V.L.; Jaffe, A.S.; Weston, S.A.; Abouezzeddine, O.F.; Jiang, R.; Manemann, S.M.; Enriquez-Sarano, M. Prognostic Value of Soluble ST2 After Myocardial Infarction: A Community Perspective. Am. J. Med. 2017, 130, 1112.e9–1112.e15. [Google Scholar] [CrossRef]
- Hashmi, S.; Al-Salam, S. Galectin-3 is expressed in the myocardium very early post-myocardial infarction. Cardiovasc. Pathol. 2015, 24, 213–223. [Google Scholar] [CrossRef] [PubMed]
- Mayr, A.; Klug, G.; Mair, J.; Streil, K.; Harrasser, B.; Feistritzer, H.J.; Jaschke, W.; Schocke, M.; Pachinger, O.; Metzler, B. Galectin-3: Relation to infarct scar and left ventricular function after myocardial infarction. Int. J. Cardiol. 2013, 163, 335–337. [Google Scholar] [CrossRef]
- González, G.E.; Cassaglia, P.; Noli Truant, S.; Fernández, M.M.; Wilensky, L.; Volberg, V.; Malchiodi, E.L.; Morales, C.; Gelpi, R.J. Galectin-3 is essential for early wound healing and ventricular remodeling after myocardial infarction in mice. Int. J. Cardiol. 2014, 176, 1423–1425. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.; Zhang, Z.; Chen, L.; Zhang, P.; Cui, Y.; Liu, H.; Ma, H.; Jiang, Y.; Wang, Y.; Yang, L.; Wu, H.; Cui, L. Elevated plasma levels of Mac-2 binding protein predict poor cardiovascular outcomes in patients with acute coronary syndrome. Coron. Artery Dis. 2017, 28, 683–689. [Google Scholar] [CrossRef]
- Gleissner, C.A.; Erbel, C.; Linden, F.; Domschke, G.; Akhavanpoor, M.; Helmes, C.M.; Doesch, A.O.; Kleber, M.E.; Katus, H.A.; Maerz, W. Galectin-3 binding protein, coronary artery disease and cardiovascular mortality: Insights from the LURIC study. Atherosclerosis 2017, 260, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Roffi, M.; Patrono, C.; Collet, J.P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar]
- Thygesen, K.; Alpert, J.S.; White, H.D.; Jaffe, A.S.; Katus, H.A.; Apple, F.S.; Lindahl, B.; Morrow, D.A.; Chaitman, B.A.; Clemmensen, P.M.; et al. Third universal definition of myocardial infarction. Eur. Heart J. 2012, 33, 2551–2567. [Google Scholar] [CrossRef] [Green Version]
- Gray, R.J. A class of k-sample tests for comparing the cumulative incidence of a competing risk. Ann. Stat. 1988, 16, 1141–1154. [Google Scholar] [CrossRef]
- Lemon, S.C.; Roy, J.; Clark, M.A.; Friedmann, P.D.; Rakowski, W. Classification and regression tree analysis in public health: Methodological review and comparison with logistic regression. Ann. Behav. Med. 2003, 26, 172–181. [Google Scholar] [CrossRef]
- Breiman, L.F.; Olshen, R.A.; Stone, C.J. Classification and Regression Trees, 2nd ed.; Wadsworth: Pacific Grove, CA, USA, 1984. [Google Scholar]
- Erdman, L.K.; D’Acremont, V.; Hayford, K.; Rajwans, N.; Kilowoko, M.; Kyungu, E.; Hongoa, P.; Alamo, L.; Streiner, D.L.; Genton, B.; Kain, K.C. Biomarkers of Host Response Predict Primary End-Point Radiological Pneumonia in Tanzanian Children with Clinical Pneumonia: A Prospective Cohort Study. PLoS ONE 2015, 10, e0137592. [Google Scholar] [CrossRef] [PubMed]
- Arnold, S.V.; Smolderen, K.G.; Kennedy, K.F.; Li, Y.; Shore, S.; Stolker, J.M.; Wang, T.Y.; Jones, P.G.; Zhao, Z.; Spertus, J.A. Risk factors for rehospitalization for acute coronary syndromes and unplanned revascularization following acute myocardial infarction. J. Am. Heart Assoc. 2015, 4. [Google Scholar] [CrossRef]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Anand, S.S.; Islam, S.; Rosengren, A.; Franzosi, M.G.; Steyn, K.; Yusufali, A.H.; Keltai, M.; Diaz, R.; Rangarajan, S.; Yusuf, S.; et al. Risk factors for myocardial infarction in women and men: Insights from the INTERHEART study. Eur. Heart J. 2008, 29, 932–940. [Google Scholar] [CrossRef] [PubMed]
- Di Chiara, A.; Chiarella, F.; Savonitto, S.; Lucci, D.; Bolognese, L.; De Servi, S.; Greco, C.; Boccanelli, A.; Zonzin, P.; Coccolini, S.; et al. Epidemiology of acute myocardial infarction in the Italian CCU network: The BLITZ study. Eur. Heart J. 2003, 24, 1616–1629. [Google Scholar] [CrossRef]
- Lindahl, B.; Toss, H.; Siegbahn, A.; Venge, P.; Wallentin, L. Markers of myocardial damage and inflammation in relation to long-term mortality in unstable coronary artery disease. FRISC Study Group. Fragmin during Instability in Coronary Artery Disease. N. Engl. J. Med. 2000, 343, 1139–1147. [Google Scholar] [CrossRef]
- Lee, Y.J.; Kang, S.W.; Song, J.K.; Park, J.J.; Bae, Y.D.; Lee, E.Y.; Lee, E.B.; Song, Y.W. Serum galectin-3 and galectin-3 binding protein levels in Behçet’s disease and their association with disease activity. Clin. Exp. Rheumatol. 2007, 25, S41–S45. [Google Scholar] [PubMed]
- Falk, E.; Nakano, M.; Bentzon, J.F.; Finn, A.V.; Virmani, R. Update on acute coronary syndromes: The pathologists’ view. Eur. Heart J. 2013, 34, 719–728. [Google Scholar]
- Ridker, P.M.; Hennekens, C.H.; Buring, J.E.; Rifai, N. C-reactive protein and other markers of inflammation in the prediction of cardiovascular disease in women. N. Engl. J. Med. 2000, 342, 836–843. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef]
- Dumic, J.; Dabelic, S.; Flögel, M. Galectin-3: An open-ended story. Biochim. Biophys. Acta. 2006, 1760, 616–635. [Google Scholar] [CrossRef]
- Tsai, T.H.; Sung, P.H.; Chang, L.T.; Sun, C.K.; Yeh, K.H.; Chung, S.Y.; Chua, S.; Chen, Y.L.; Wu, C.J.; Chang, H.W.; et al. Value and level of galectin-3 in acute myocardial infarction patients undergoing primary percutaneous coronary intervention. J. Atheroscler. Thromb. 2012, 19, 1073–1082. [Google Scholar] [CrossRef]
- Pfeffer, M.A.; Braunwald, E. Ventricular remodeling after myocardial infarction. Experimental observations and clinical implications. Circulation 1990, 81, 1161–1172. [Google Scholar] [CrossRef]
- Di Tano, G.; Caretta, G.; De Maria, R.; Parolini, M.; Bassi, L.; Testa, S.; Pirelli, S. Galectin-3 predicts left ventricular remodelling after anterior-wall myocardial infarction treated by primary percutaneous coronary intervention. Heart 2017, 103, 71–77. [Google Scholar] [CrossRef]
- Fox, K.A.; Dabbous, O.H.; Goldberg, R.J.; Pieper, K.S.; Eagle, K.A.; Van de Werf, F.; Avezum, A.; Goodman, S.G.; Flather, M.D.; Anderson, F.A., Jr.; et al. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: Prospective multinational observational study (GRACE). BMJ 2006, 333, 1091. [Google Scholar] [CrossRef]
- Lax, A.; Sanchez-Mas, J.; Asensio-Lopez, M.C.; Fernandez-Del Palacio, M.J.; Caballero, L.; Garrido, I.P.; Pastor-Perez, F.J.; Januzzi, J.L.; Pascual-Figal, D.A. Mineralocorticoid receptor antagonists modulate galectin-3 and interleukin-33/ST2 signaling in left ventricular systolic dysfunction after acute myocardial infarction. JACC Heart Fail. 2015, 3, 50–58. [Google Scholar] [CrossRef]
- Sanders-van Wijk, S.; Masson, S.; Milani, V.; Rickenbacher, P.; Gorini, M.; Tavazzi, L.T.; Tobler, D.; Rickli, H.; Latini, R.; Brunner-La Roccaenen, H.P.; et al. Interaction of Galectin-3 Concentrations with the Treatment Effects of β-Blockers and RAS Blockade in Patients with Systolic Heart Failure: A Derivation-Validation Study from TIME-CHF and GISSI-HF. Clin. Chem. 2016, 62, 605–616. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n = 469 | |
|---|---|
| Age | 67.63 (11.29) |
| Male sex (%) | 67.8 |
| BMI (kg/m2) | 26.82 (4.34) |
| SBP at admission (mmHg) | 136.02 (25.30) |
| DBP at admission (mmHg) | 79.40 (14.47) |
| Heart rate at admission (bpm) | 76.25 (16.82) |
| Cardiac arrest (%) | 3 |
| Left bundle branch block (%) | 5.5 |
| Diagnosis (%) - STEMI - NSTEMI | 60.1 39.9 |
| Killip > 1 (%) | 24.4 |
| Hypertension (%) | 72.1 |
| Diabetes mellitus (%) | 24.7 |
| Smoking (%) | 45.2 |
| Dyslipidemia (%) | 59.9 |
| Positive family history for IHD (%) | 23.9 |
| Known chronic kidney disease (%) | 9.2 |
| Peripheral artery disease (%) | 7.7 |
| Previous myocardial infarction (%) | 18.3 |
| Previous CABG (%) | 3.4 |
| Anemia at admission (%) | 26.7 |
| Total cholesterol (mg/dL) | 189.43 (44.92) |
| LDL cholesterol (mg/dL) | 118.02 (38.44) |
| HDL cholesterol (mg/dL) | 45.26 (12.27) |
| Triglycerides (mg/dL) | 113.5 (82–151) |
| TnI max (ng/mL) | 12.79 (2.86–52.45) |
| Hb1AC (%) | 6 (5.7–6.6) |
| Hs CRP (mg/dL) | 7 (2.8–21.87) |
| Galectin 3 (ng/mL) | 9.8 (7.77–12.77) |
| Galectin 3 binding protein (g/mL) | 9.08 (5.77–13.54) |
| IL-1 β (pg/mL) | 0.59 (0.42–0.97) |
| Na+ at discharge (mEq/L) | 138.94 (3.35) |
| Hemoglobin at discharge (g/dL) | 12.46 (1.67) |
| MDRD at discharge (mL/min) | 69.37 (27.08) |
| GRACE score at 6 months | 120.12 (31.05) |
| Left atrium area (cm2) | 21.46 (5.73) |
| EDD_I (cm) | 3 (4.79) |
| ESD_I (cm) | 1.83 (2.46) |
| Interventicular septum (cm) | 1.32 (1.07) |
| FS % | 34.57 (11.3) |
| EDV_I (cm2) | 47.04 (38.65–57.2) |
| ESV_I (cm2) | 21.41 (16.05–28.75) |
| E/A | 1.07 (0.77) |
| E/E’ | 11.87 (4.77) |
| WMSI | 1.31 (1.13–1.75) |
| Left ventricular mass (g) | 225.2 (68.26) |
| Left ventricular ejection fraction % | 52 (47–60) |
| Mitral insufficiency (%) - Mild - Moderate - Severe | 63.5 55.4 7.2 1.1 |
| Therapy - PCI (%) - CABG - Medical therapy | 70.6 11.1 18.2 |
| Symptom-onset-to-balloon time (h) | 2 (1 3.5) |
| GPIIbIIIa inhibitors (%) | 10.2 |
| Multivessel disease >70% (%) | 37.5 |
| Severe hemorrhagia (%) | 1.1 |
| Ventricular arrhythmias (%) | 16.2 |
| Supraventricular arrhythmias (%) | 12.6 |
| Brady arrhythmias (%) | 7.5 |
| Therapy at discharge (%) - ACE-I/ARB - Beta blockers - Digital - Amiodarone - Antialdosteronic agents - Loop diuretics - Aspirin - P2T12 inhibitors ⚬ Clopidogrel ⚬ Prasugrel ⚬ Ticagrelor - Statins - Oral antidiabetics - Insulin - Warfarin | 75.1 77.8 1.1 7.9 11.1 24.1 93.2 40.7 26.7 19.2 89.3 15.4 9.8 8.3 |
| NYHA class at discharge (%) - NYHA 1 - NYHA 2 - NYHA 3 | 88.5 8.2 3.2 |
| (a) | ||||
| Final Study Cohort n = 455 | Angina/Reinfarction n = 41 (9%) | No Angina/Reinfarction n = 408 (91%) | pValue | |
| Diagnosis (%) - STEMI - NSTEMI | 60 40 | 36.6 63.4 | 62.3 37.7 | 0.002 |
| Treatment: - PCI - CABG - Medical treatment | 71.4 11.2 17.4 | 73.2 4.9 22 | 64.8 10.8 15.4 | 0.8 |
| LVEF (%) | 54 (47–60) | 57 (49–61) | 54 (47–60) | 0.14 |
| TnI max (ng/mL) | 12.5 (2.7–52) | 5.78 (1.6–17.2) | 13.9 (2.98–65) | 0.014 |
| Galectin 3 (ng/mL) | 9.8 (7.74–12.3) | 10 (8.07–11.5) | 9.8(7.73–12.34) | 0.8 |
| Galectin 3 binding protein (μg/mL) | 9.07 (5.78–13.44) | 9.1 (7.36–14.2) | 9.06 (5.75–13.4) | 0.55 |
| (b) | ||||
| Total Population n = 469 | Died n = 35 (7.5%) | Alive n = 434 (92.5%) | pValue | |
| Diagnosis (%) - STEMI - NSTEMI | 60.1 39.9 | 57.1 42.9 | 60.4 39.6 | 0.72 |
| Treatment (%) - PTCA - CABG - Medical treatment | 70.7 11.1 18.2 | 52.9 14.7 32.4 | 72.1 10.8 17.1 | 0.047 |
| LVEF (%) | 52 (47–60) | 43 (39–55) | 55 (48–60) | <0.001 |
| TnI max (ng/mL) | 12.8 (2.9–52.5) | 18.1 (3.6–68.4) | 12.3 (2.6–51) | 0.36 |
| Galectin 3 (ng/mL) | 9.8 (7.77–12.77) | 10.49 (10–15.84) | 9.74 (7.7–12.2) | <0.001 |
| Galectin 3 binding protein (μg/mL) | 9.08 (5.8–13.5) | 10.4 (6.3–16.2) | 9.03 (5.8–13.4) | 0.10 |
| (a) | ||
| Predictors (Ordered by p Value) | Recurrent Angina with Need of Rehospitalization/Revascularization or Myocardial Infarction | |
| HR (95% CI) | pvalue | |
| Male gender (vs. female) | 4.24 (2.21–8.14) | <0.001 |
| STEMI diagnosis (vs. NSTEMI) | 3.5 (1.7–7.04) | <0.001 |
| Diabetes mellitus (yes vs. no) | 2.63 (1.32–5.18) | 0.005 |
| Galectin 3 binding protein (for 1 unit increase) | 1.04 (1.01–1.08) | 0.01 |
| (b) | ||
| Predictors (Ordered by p Value) | All-Cause Mortality | |
| HR (95% CI) | pValue | |
| Age (for 1 y increase) | 1.08 (1.04–1.12) | <0.001 |
| EF % (for 10% increase) (for 5% increase) | 0.63 (0.45–0.84) 0.79 (0.68–0.92) | 0.001 |
| LnGalectin 3 (for 1 unit increase of original variable) | 3.5 (1.54–7.5) 1.12 | 0.002 |
| MDRD at discharge (for 10% increase) (for 5% increase) | 0.88 (0.75–1.03) 0.94 (0.86–1.01) | 0.09 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gagno, G.; Padoan, L.; Stenner, E.; Beleù, A.; Ziberna, F.; Hiche, C.; Paldino, A.; Barbati, G.; Biolo, G.; Fiotti, N.; et al. Galectin 3 and Galectin 3 Binding Protein Improve the Risk Stratification after Myocardial Infarction. J. Clin. Med. 2019, 8, 570. https://doi.org/10.3390/jcm8050570
Gagno G, Padoan L, Stenner E, Beleù A, Ziberna F, Hiche C, Paldino A, Barbati G, Biolo G, Fiotti N, et al. Galectin 3 and Galectin 3 Binding Protein Improve the Risk Stratification after Myocardial Infarction. Journal of Clinical Medicine. 2019; 8(5):570. https://doi.org/10.3390/jcm8050570
Chicago/Turabian StyleGagno, Giulia, Laura Padoan, Elisabetta Stenner, Alessandro Beleù, Fabiana Ziberna, Cristina Hiche, Alessia Paldino, Giulia Barbati, Gianni Biolo, Nicola Fiotti, and et al. 2019. "Galectin 3 and Galectin 3 Binding Protein Improve the Risk Stratification after Myocardial Infarction" Journal of Clinical Medicine 8, no. 5: 570. https://doi.org/10.3390/jcm8050570