Global Evolution of Research in Artificial Intelligence in Health and Medicine: A Bibliometric Study

 ,
,  , ,
, ,  ,
,  , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
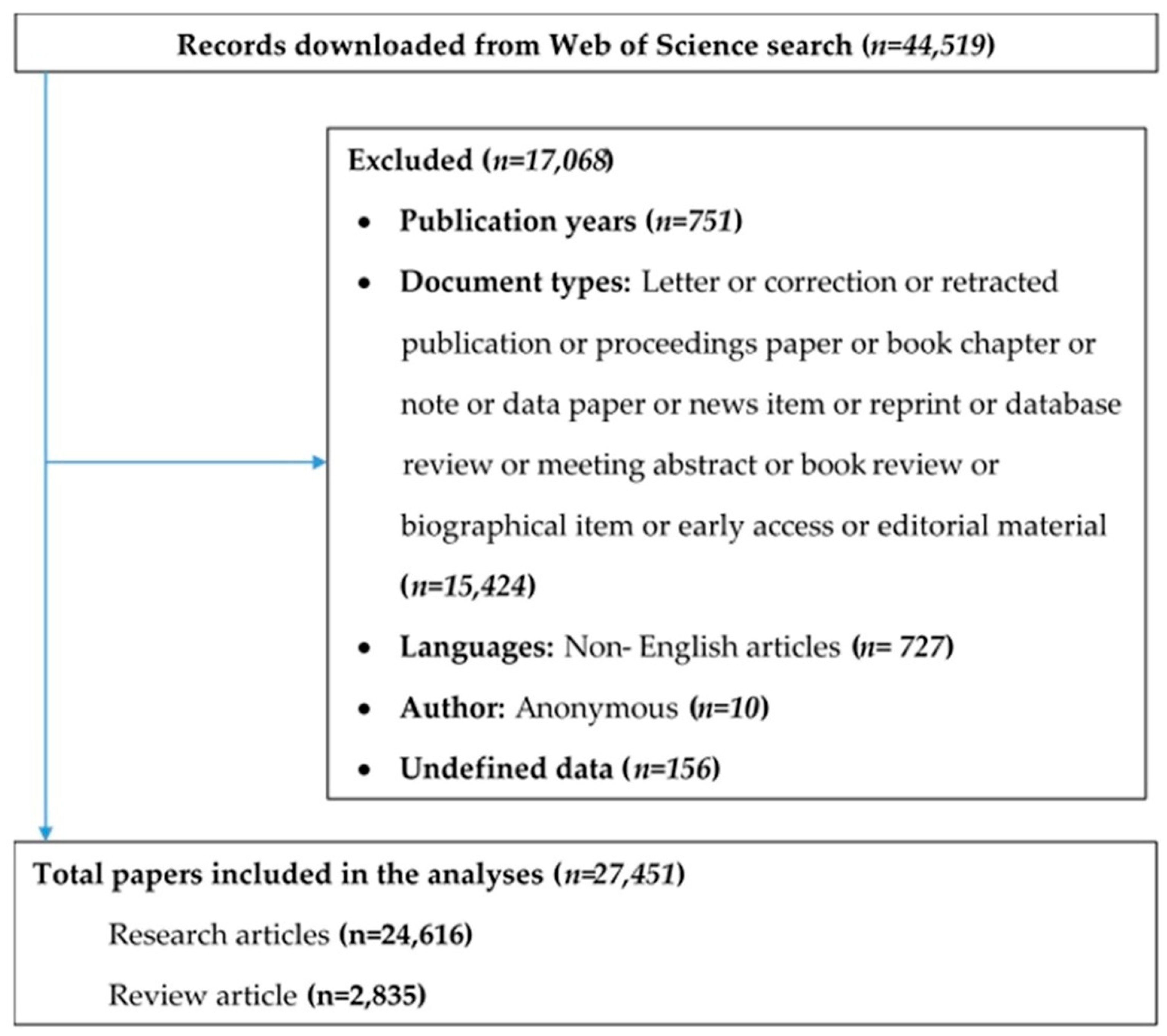
2.1. Search Strategy
2.1.1. Inclusion Step
- (1)
- “Artificial intelligence” OR “Machine intelligence” OR “artificial neutral network*” OR “Machine learning” OR “Deep learn*” OR “Natural language process*” OR “Robotic*” OR “thinking computer system” OR “fuzzy expert system*” OR “evolutionary computation” OR “hybrid intelligent system*”
- (2)
- disease* OR illness OR health-related OR medic* OR “medical diagnosis” OR treatment OR health* OR wellness OR well-being
2.1.2. Exclusion Step
2.2. Data Extraction
2.3. Data Analysis
3. Results
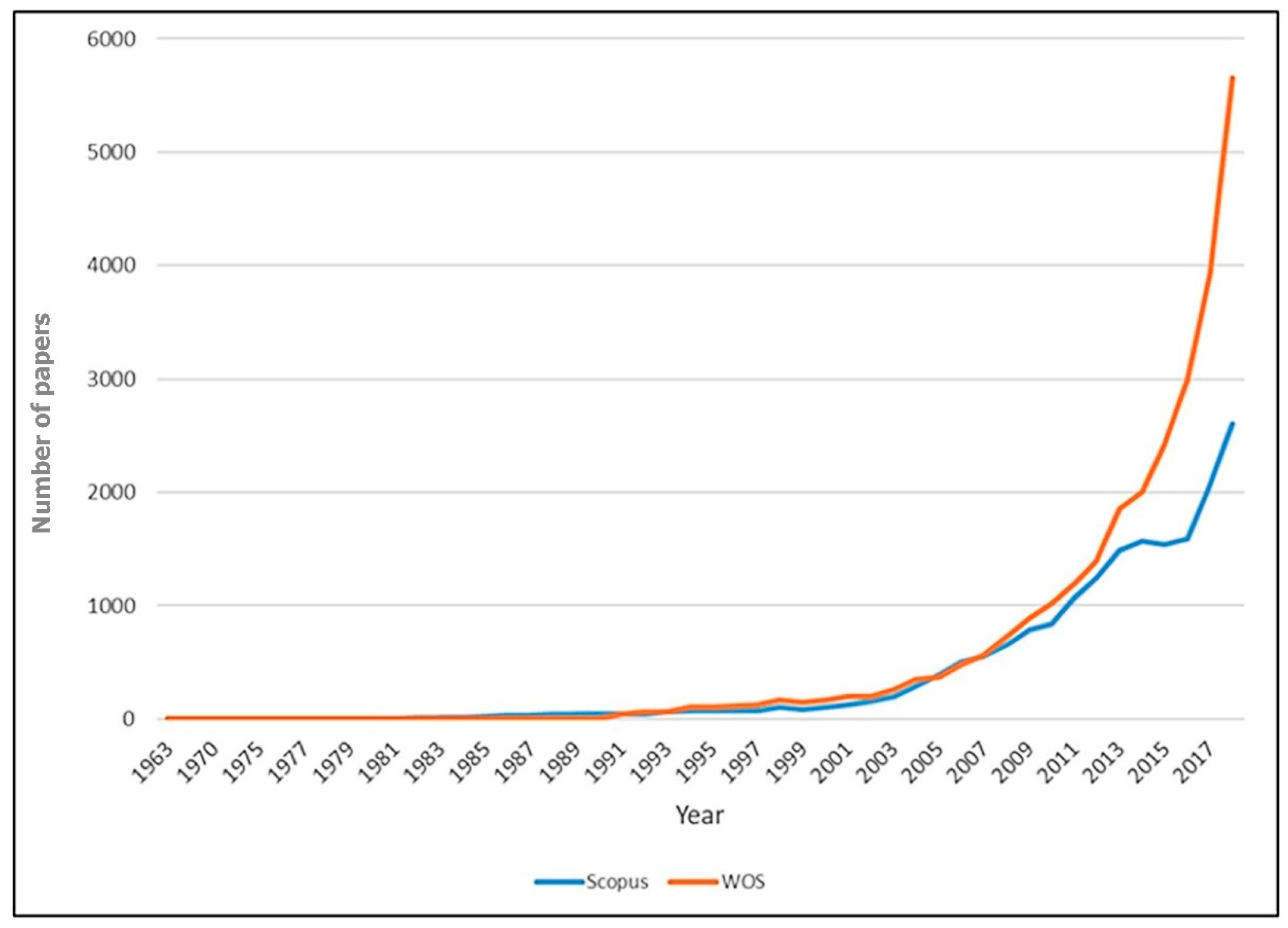
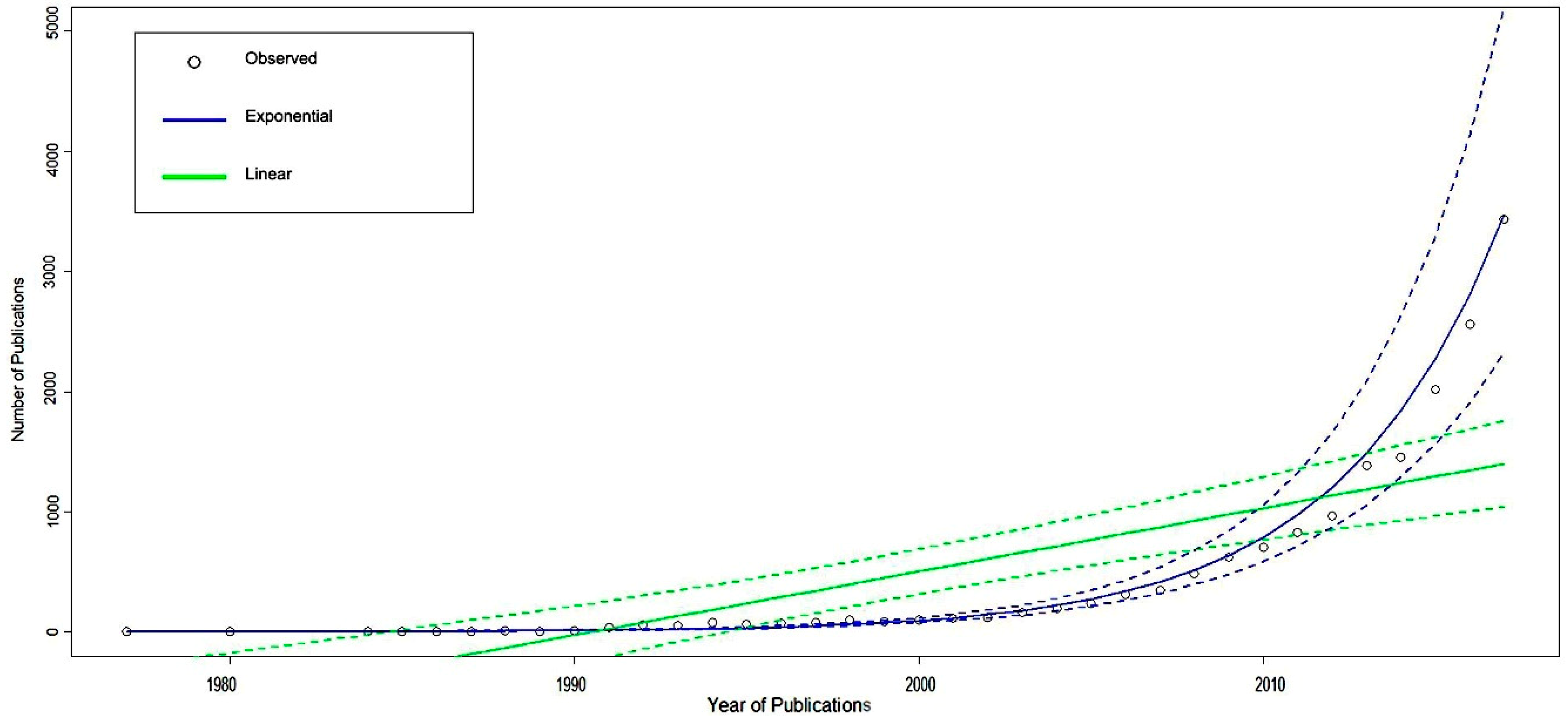
3.1. The Publication Trend
- Most of the papers (80.0%) were assorted into one (n = 14,756; 53.6%) or two (n = 7225; 26.4%) subject categories.
- The number of publications dated between 2008 and 2017 (16,913 articles) accounts for 61.6% of the total number of publications being analyzed. This figure was double compared with the previous time range and seven times as much as that in the previous ten-year period.
- The number of countries means the paper was written by one country only or in collaboration with others. Based on that information, we found that AI-related medical research was mainly performed by one to three countries (85.9%). The global collaboration among nation-states was not so high (14.0%).
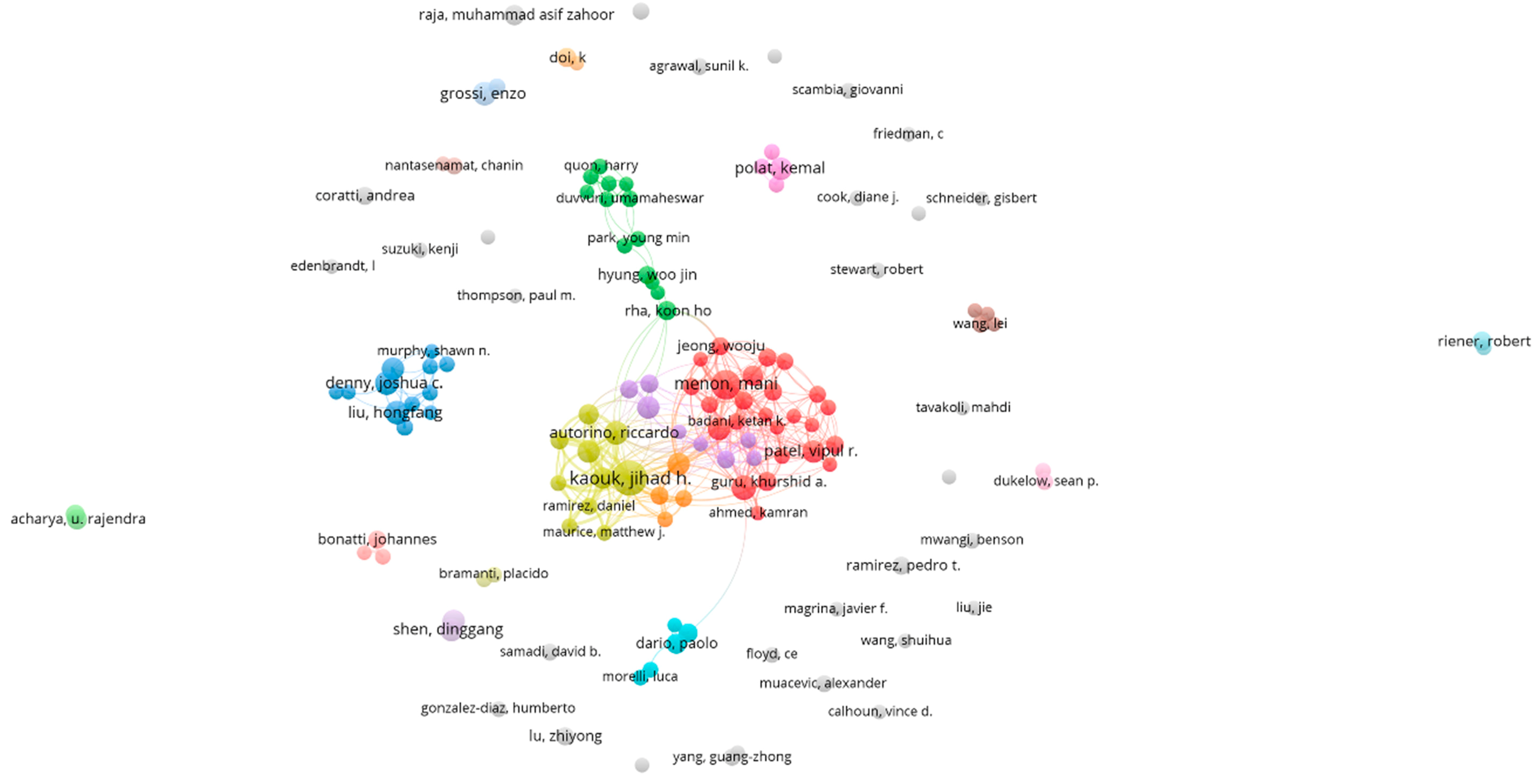
3.2. Contribution by Author
3.3. Global Collaboration
3.4. Keyword and Text Analysis
- Types of AI: among all the keywords applied for searching, three kinds of AI being outstanding compared with others were “machine learning”, “robotics”, and “deep learning”
- AI applications in health and medicine: For example, “machine learning”, “artificial intelligence”, “support vector machines” were used to support the diagnose and/or treatment of “Parkinson’s disease”, “Alzheimer’s disease” or used in “neuroimaging”. “Robotics” was utilized mainly for assisting laparoscopy of “oropharyngeal cancer” or “cervical cancer” or “surgery”. “Natural language processing” was applied for collecting “health records” information contributing to “big data” system.
4. Discussion
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Nuffield Council on Bioethics. Bioethics Briefing Notes: Artificial Intelligence (AI) in Healthcare and Research. Available online: http://nuffieldbioethics.org/wp-content/uploads/Artificial-Intelligence-AI-in-healthcare-and-research.pdf (accessed on 21 December 2018).
- Elsevier. Artificial Intelligence: How Knowledge Is Created, Transferred, and Used; Elsevier Artificial Intelligence Program: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Frankish, K.; Ramsey, W.M. (Eds.) Introduction. In The Cambridge Handbook of Artificial Intelligence; Cambridge University Press: Cambridge, UK, 2014; pp. 1–14. [Google Scholar]
- Yu, K.-H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef]
- Hamet, P.; Tremblay, J. Artificial intelligence in medicine. Metabolism 2017, 69, S36–S40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trivikram, C.; Samarpitha, S.; Madhavi, K.; Moses, D. Evaluation of hybrid face and voice recognition systems for biometric identification in areas requiring high security. I-Manag. J. Pattern Recognit. 2017, 4, 9–16. [Google Scholar]
- Gunn, A. The diagnosis of acute abdominal pain with computer analysis. J. R. Coll. Surg. Edinb. 1976, 21, 170–172. [Google Scholar] [PubMed]
- Ramesh, A.N.; Kambhampati, C.; Monson, J.R.T.; Drew, P.J. Artificial intelligence in medicine. Ann. R. Coll. Surg. Engl. 2004, 86, 334–338. [Google Scholar] [CrossRef] [Green Version]
- Niu, J.; Tang, W.; Xu, F.; Zhou, X.; Song, Y. Global research on artificial intelligence from 1990–2014: Spatially-explicit bibliometric analysis. ISPRS Int. J. Geo-Inf. 2016, 5, 66. [Google Scholar] [CrossRef]
- Begovic, M.; Oprunenco, A.; Sadiku, L. Let’s Talk about Artificial Intelligence; UNDP: New York, NY, USA, 2018; Volume 2019. [Google Scholar]
- Jiang, F.; Jiang, Y.; Zhi, H.; Dong, Y.; Li, H.; Ma, S.; Wang, Y.; Dong, Q.; Shen, H.; Wang, Y. Artificial intelligence in healthcare: Past, present and future. Stroke Vasc. Neurol. 2017, 2, 230–243. [Google Scholar] [CrossRef] [PubMed]
- Shaban-Nejad, A.; Michalowski, M.; Buckeridge, D.L. Health intelligence: How artificial intelligence transforms population and personalized health. NPJ Digit. Med. 2018, 1, 53. [Google Scholar] [CrossRef]
- Mudaly, T.; Moodley, D.; Pillay, A.; Seebregts, C.J. Architectural frameworks for developing national health information systems in low and middle income countries. In Proceedings of the First International Conference on Enterprise Systems: ES 2013, Cape Town, South Africa, 7–8 November 2013; pp. 1–9. [Google Scholar]
- Pearson, T. How to Replicate Watson Hardware and Systems Design for Your Own Use in Your Basement; IBM: Watson, MN, USA, 2011. [Google Scholar]
- Neill, D.B. Using artificial intelligence to improve hospital inpatient care. IEEE Intell. Syst. 2013, 28, 92–95. [Google Scholar] [CrossRef]
- Sharifi, V.; Rahimi Movaghar, A.; Mohammadi, M.; Goodarzi, R.; Izadian, E.; Farhoudian, A.; Mansouri, N.; Nejatisafa, A.A. Analysis of mental health research in the Islamic republic of Iran over 3 decades: A scientometric study. East. Mediterr. Health J. 2008, 14, 1060–1069. [Google Scholar]
- Eghbal, M.J.; Ardakani, N.D.; Asgary, S. A scientometric study of pubmed-indexed endodontic articles: A comparison between Iran and other regional countries. Iran. Endod. J. 2012, 7, 56–59. [Google Scholar]
- Vuong, Q.-H.; La, V.-P.; Vuong, T.-T.; Ho, M.-T.; Nguyen, H.-K.T.; Nguyen, V.-H.; Pham, H.-H.; Ho, M.-T. An open database of productivity in Vietnam’s social sciences and humanities for public use. Sci. Data 2018, 5, 180188. [Google Scholar] [CrossRef]
- Yao, Q.; Chen, K.; Yao, L.; Lyu, P.-H.; Yang, T.-A.; Luo, F.; Chen, S.-Q.; He, L.-Y.; Liu, Z.-Y. Scientometric trends and knowledge maps of global health systems research. Health Res. Policy Syst. 2014, 12, 26. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Yeh, H.-Y.; Wu, J.-C.; Haschler, I.; Chen, T.-J.; Wetter, T. Taiwan’s national health insurance research database: Administrative health care database as study object in bibliometrics. Scientometrics 2011, 86, 365–380. [Google Scholar] [CrossRef]
- Peykari, N.; Djalalinia, S.; Kasaeian, A.; Naderimagham, S.; Hasannia, T.; Larijani, B.; Farzadfar, F. Diabetes research in Middle East countries: A scientometrics study from 1990 to 2012. J. Res. Med Sci. 2015, 20, 253–262. [Google Scholar]
- Clavirate Analytics. Web of Science; Clavirate Analytics: Philadelphia, PA, USA, 2018. [Google Scholar]
- Elsevier. Scopus; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Brynjolfsson, E.; McAfee, A. The Second Machine Age: Work, Progress, and Prosperity in a Time of Brilliant Technologies; WW Norton & Company: New York, NY, USA, 2014. [Google Scholar]
- Viktor, M.-S.; Kenneth, C. Big Data: A Revolution That Will Transform How We Live, Work, and Think; John Murray: London, UK, 2013. [Google Scholar]
- Flemming, N. How artificial intelligence is changing drug discovery. Nature 2018, 557, S55–S57. [Google Scholar] [CrossRef] [Green Version]
- Ho, T.; Nguyen, H.; Vuong, T.; Dam, Q.; Pham, H.; Vuong, Q. Exploring Vietnamese co-authorship patterns in social sciences with basic network measures of 2008–2017 Scopus data. F1000Research 2017, 6, 1559. [Google Scholar] [CrossRef]
- European Commission. USA-China-EU Plans for AI: Where do We Stand? European Commission: Brussels, Belgium, 2018. [Google Scholar]
- Pesapane, F.; Volonté, C.; Codari, M.; Sardanelli, F. Artificial intelligence as a medical device in radiology: Ethical and regulatory issues in Europe and the United States. Insights Imaging 2018, 9, 745–753. [Google Scholar] [CrossRef]
- Kyu, H.H.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the global burden of disease study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef]
- Libbrecht, M.W.; Noble, W.S. Machine learning applications in genetics and genomics. Nat. Rev. Genet. 2015, 16, 321–332. [Google Scholar] [CrossRef]
- Komorowski, M.; Celi, L.A.; Badawi, O.; Gordon, A.C.; Faisal, A.A. The artificial intelligence clinician learns optimal treatment strategies for sepsis in intensive care. Nat. Med. 2018, 24, 1716–1720. [Google Scholar] [CrossRef]
- Cao, X. A call for global research on non-communicable diseases. Lancet 2015, 385, e5–e6. [Google Scholar] [CrossRef]
- Jeelani, S.; Dany, A.; Anand, B.; Vandana, S.; Maheswaran, T.; Rajkumar, E. Robotics and medicine: A scientific rainbow in hospital. J. Pharm. Bioallied Sci. 2015, 7, S381–S383. [Google Scholar] [CrossRef]
- Liu, D.; Ray, B.; Neavin, D.R.; Zhang, J.; Athreya, A.P.; Biernacka, J.M.; Bobo, W.V.; Hall-Flavin, D.K.; Skime, M.K.; Zhu, H.; et al. Beta-defensin 1, aryl hydrocarbon receptor and plasma kynurenine in major depressive disorder: Metabolomics-informed genomics. Transl. Psychiatry 2018, 8, 10. [Google Scholar] [CrossRef]
- Lai, C.Y.Y.; Ho, C.S.H.; Lim, C.R.; Ho, R.C.M. Functional near-infrared spectroscopy in psychiatry. BJPsych Adv. 2018, 23, 324–330. [Google Scholar] [CrossRef]
- Ho, C.S.; Zhang, M.W.; Ho, R.C. Optical topography in psychiatry: A chip off the old block or a new look beyond the mind-brain frontiers? Front. Psychiatry 2016, 7, 74. [Google Scholar] [CrossRef]
- Athreya, A.; Iyer, R.; Neavin, D.; Wang, L.; Weinshilboum, R.; Kaddurah-Daouk, R.; Rush, J.; Frye, M.; Bobo, W. Augmentation of physician assessments with multi-omics enhances predictability of drug response: A case study of major depressive disorder. IEEE Comput. Intell. Mag. 2018, 13, 20–31. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Do, T.; Hoang, T.; Pomponiu, V.; Zhou, Y.; Chen, Z.; Cheung, N.; Koh, D.; Tan, A.; Tan, S. Accessible melanoma detection using smartphones and mobile image analysis. IEEE Trans. Multimed. 2018, 20, 2849–2864. [Google Scholar] [CrossRef]
- Nejati, H.; Alizadeh Ghazijahani, H.; Abdollahzadeh, M.; Malekzadeh, T.; Cheung, N.-M.; Lee, K.H.; Low, L. Fine-grained wound tissue analysis using deep neural network. In Proceedings of the 2018 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Calgary, AB, Canada, 15–20 April 2018; pp. 1010–1014. [Google Scholar]
- Dixit, M.N.; Kwitt, R.N.; Niethammer, M.N.; Vasconcelos, N.N. Aga: Attribute guided augmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017. [Google Scholar]
- Liu, B.; Dixit, M.; Kwitt, R.; Vasconcelos, N. Feature space transfer for data augmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Salt Lake City, UT, USA, 18–22 June 2018. [Google Scholar]
- Goodfellow, I.J.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative adversarial nets. In Proceedings of the 27th International Conference on Neural Information Processing Systems—Volume 2; MIT Press: Montreal, QC, Canada, 2014; pp. 2672–2680. [Google Scholar]
- Tran, N.-T.; Bui, A.; Cheung, N.-M. Improving GAN with neighbors embedding and gradient matching. In Proceedings of the Thirty-Third AAAI Conference on Artificial Intelligence (AAAI-19), Honolulu, HI, USA, 27 January–1 February 2019. [Google Scholar]
- Lim, S.K.; Loo, Y.; Tran, N.-T.; Cheung, N.-M.; Roig, G.; Elovici, Y. DOPING: Generative data augmentation for unsupervised anomaly detection with GAN. In Proceedings of the IEEE International Conference on Data Mining 2018, Singapore, 17–20 November 2018. [Google Scholar]
- Frid-Adar, M.; Diamant, I.; Klang, E.; Amitai, M.; Goldberger, J.; Greenspan, H. GAN-based synthetic medical image augmentation for increased CNN performance in liver lesion classification. Neurocomputing 2018, 321, 321–331. [Google Scholar] [CrossRef]
- Dai, Z.; Yang, Z.; Yang, F.; Cohen, W.; Salakhutdinov, R. Good semi-supervised learning that requires a bad GAN. In Proceedings of the Advances in Neural Information Processing Systems, Long Beach, CA, USA, 4–9 December 2017. [Google Scholar]
- Pathak, D.; Krahenbuhl, P.; Donahue, J.; Darrell, T.A.; Efros, A. Context encoders: Feature learning by inpainting. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 26 June–1 July 2016. [Google Scholar]
- Gidaris, S.; Singh, P.; Komodakis, N. Unsupervised representation learning by predicting image rotations. arXiv, 2018; arXiv:1803.07728. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Category | Number | Percent |
|---|---|---|---|
| Total number of papers | 27,451 | 100 | |
| Year of publication | 2018–2014 | 16,913 | 61.62 |
| 2013–2009 | 6303 | 22.97 | |
| 2008–2004 | 2471 | 9.00 | |
| 2003–1999 | 968 | 3.53 | |
| 1998–1994 | 599 | 2.18 | |
| 1993–1989 | 174 | 0.64 | |
| <1989 | 23 | 0.06 | |
| Number of authors | 1 | 1413 | 5.15 |
| 2–3 | 8085 | 29.45 | |
| 4–6 | 10,992 | 40.05 | |
| 7–10 | 5237 | 19.07 | |
| >10 | 1724 | 6.28 | |
| Number of subject categories | 1 | 14,756 | 53.75 |
| 2 | 7225 | 26.32 | |
| 3 | 3597 | 13.10 | |
| 4 | 1244 | 4.53 | |
| >5 | 629 | 2.30 | |
| Number of countries in authorship | 1 | 18,532 | 67.51 |
| 2 | 4954 | 18.05 | |
| 3 | 1126 | 4.1 | |
| 4 | 295 | 1.07 | |
| 5 | 109 | 0.4 | |
| 6 | 42 | 0.15 | |
| 7 | 32 | 0.12 | |
| 8 | 20 | 0.07 | |
| 9 | 6 | 0.02 | |
| >10 | 18 | 0.06 |
| No. | Country | Total Papers | % Papers | Total Citations | Cite Rate | Total Downloads | Total Co-Authors | Total Institutes | Total Country | % Papers with International Collaboration |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | United States | 10,623 | 30.8 | 232,669 | 3.4 | 25,384 | 5.8 | 6.8 | 1.5 | 33.6% |
| 2 | China | 2617 | 7.6 | 27,997 | 2.9 | 15,995 | 5.9 | 7.3 | 1.7 | 44.8% |
| 3 | Italy | 1834 | 5.3 | 29,485 | 2.8 | 3343 | 7.4 | 8.4 | 2.1 | 55.2% |
| 4 | Germany | 1553 | 4.5 | 31,219 | 3.3 | 3415 | 7.4 | 8.9 | 2.1 | 53.1% |
| 5 | Canada | 1312 | 3.8 | 22,608 | 2.9 | 3343 | 6.2 | 8.0 | 1.8 | 48.5% |
| 6 | France | 1308 | 3.8 | 22,687 | 3.1 | 2623 | 7.4 | 9.0 | 2.2 | 63.7% |
| 7 | India | 1264 | 3.7 | 12,871 | 2.1 | 3350 | 4.5 | 4.9 | 1.6 | 31.6% |
| 8 | Spain | 1029 | 3.0 | 14,653 | 2.6 | 2852 | 6.5 | 7.7 | 2.0 | 49.3% |
| 9 | Australia | 910 | 2.6 | 17,413 | 3.5 | 3337 | 5.8 | 7.5 | 2.0 | 50.5% |
| 10 | Japan | 841 | 2.4 | 11,054 | 2.2 | 2107 | 6.7 | 7.5 | 1.7 | 35.7% |
| 11 | Turkey | 787 | 2.3 | 9058 | 1.8 | 1121 | 4.1 | 4.4 | 1.4 | 20.3% |
| 12 | Iran | 713 | 2.1 | 7438 | 2.2 | 1599 | 4.1 | 4.6 | 1.4 | 30.2% |
| 13 | Netherlands | 640 | 1.9 | 14,811 | 4.4 | 1948 | 8.0 | 10.1 | 2.4 | 59.2% |
| 14 | Switzerland | 554 | 1.6 | 10,197 | 3.6 | 1804 | 7.6 | 9.7 | 2.3 | 63.5% |
| 15 | Taiwan | 543 | 1.6 | 6213 | 1.8 | 1084 | 5.1 | 6.6 | 1.5 | 28.5% |
| 16 | Brazil | 489 | 1.4 | 6097 | 2.6 | 1380 | 6.6 | 8.1 | 1.9 | 44.6% |
| 17 | Israel | 384 | 1.1 | 6393 | 3.4 | 950 | 7.8 | 9.8 | 2.4 | 69.8% |
| 18 | Sweden | 382 | 1.1 | 6220 | 3.0 | 700 | 7.7 | 9.7 | 2.4 | 61.3% |
| 19 | Belgium | 365 | 1.1 | 7269 | 3.5 | 696 | 8.8 | 10.7 | 2.8 | 66.6% |
| 20 | Singapore | 349 | 1.0 | 5378 | 3.2 | 1904 | 6.0 | 7.1 | 2.2 | 66.2% |
| Title | Robotic | Machine Learning | Artificial Neural Network | Artificial Intelligence | Natural Language Process | Deep Learning | Fuzzy Expert System | Evolutionary Computation | Clinical Application | Treatment | Prediction | Diagnosis | Total | Rank Burden of Diseases (DALY) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cancer | 1774 | 767 | 366 | 144 | 103 | 0 | 5 | 6 | 28 | 209 | 1008 | 82 | 4492 | 12 |
| Heart Diseases | 263 | 357 | 166 | 75 | 33 | 59 | 11 | 3 | 11 | 19 | 331 | 33 | 1361 | 1 |
| Vision | 543 | 264 | 81 | 101 | 57 | 1 | 4 | 5 | 19 | 27 | 189 | 21 | 1312 | 22 |
| Stroke | 543 | 99 | 45 | 16 | 9 | 0 | 0 | 2 | 13 | 32 | 119 | 5 | 883 | 3 |
| Alzheimer | 17 | 314 | 70 | 18 | 8 | 0 | 0 | 1 | 5 | 2 | 210 | 48 | 693 | 24 |
| Depression | 71 | 232 | 29 | 33 | 24 | 0 | 1 | 0 | 7 | 39 | 178 | 6 | 620 | 20 |
| Kidney | 293 | 64 | 38 | 14 | 9 | 0 | 2 | 0 | 1 | 17 | 125 | 9 | 572 | 19 |
| Diabetes | 38 | 159 | 86 | 34 | 20 | 0 | 4 | 3 | 1 | 6 | 176 | 21 | 548 | 8 |
| Respiratory | 119 | 104 | 64 | 20 | 16 | 2 | 0 | 0 | 1 | 9 | 136 | 6 | 477 | 4 |
| Substance use | 75 | 101 | 57 | 17 | 35 | 7 | 0 | 0 | 2 | 20 | 120 | 4 | 438 | 16 |
| HIV | 24 | 114 | 35 | 28 | 21 | 6 | 0 | 2 | 6 | 10 | 113 | 4 | 363 | 13 |
| Injuries | 162 | 32 | 9 | 9 | 5 | 0 | 1 | 0 | 5 | 7 | 30 | 1 | 261 | 5 |
| Asthma | 12 | 60 | 29 | 6 | 12 | 1 | 2 | 0 | 0 | 0 | 62 | 4 | 188 | 25 |
| Tuberculosis | 8 | 42 | 17 | 12 | 2 | 2 | 0 | 0 | 1 | 2 | 42 | 15 | 143 | 14 |
| Congenital | 64 | 24 | 14 | 5 | 1 | 3 | 0 | 0 | 3 | 6 | 19 | 3 | 142 | 9 |
| Cirrhosis | 11 | 23 | 24 | 6 | 2 | 0 | 0 | 0 | 2 | 4 | 38 | 2 | 112 | 11 |
| Malaria | 4 | 38 | 9 | 8 | 1 | 0 | 1 | 0 | 1 | 0 | 42 | 2 | 106 | 15 |
| Suicide | 0 | 43 | 1 | 3 | 10 | 0 | 0 | 0 | 1 | 1 | 34 | 1 | 94 | 16 |
| COPD | 5 | 32 | 7 | 3 | 3 | 0 | 1 | 0 | 0 | 0 | 29 | 1 | 81 | 6 |
| Neonatal | 7 | 22 | 8 | 5 | 4 | 3 | 1 | 0 | 0 | 0 | 22 | 1 | 73 | 2 |
| Hearing | 7 | 11 | 9 | 6 | 0 | 0 | 0 | 1 | 0 | 1 | 14 | 3 | 52 | 21 |
| Back pain | 18 | 5 | 9 | 2 | 1 | 0 | 0 | 0 | 2 | 2 | 11 | 0 | 50 | 10 |
| Headache disorders | 0 | 0 | 0 | 0 | 0 | 5 | 0 | 0 | 0 | 0 | 0 | 0 | 5 | 23 |
| Diarrhea | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 7 |
| Headache disorders | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 18 |
| Total | 4059 | 2907 | 1173 | 565 | 376 | 90 | 33 | 23 | 109 | 413 | 3048 | 272 | 13,068 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, B.X.; Vu, G.T.; Ha, G.H.; Vuong, Q.-H.; Ho, M.-T.; Vuong, T.-T.; La, V.-P.; Ho, M.-T.; Nghiem, K.-C.P.; Nguyen, H.L.T.; et al. Global Evolution of Research in Artificial Intelligence in Health and Medicine: A Bibliometric Study. J. Clin. Med. 2019, 8, 360. https://doi.org/10.3390/jcm8030360
Tran BX, Vu GT, Ha GH, Vuong Q-H, Ho M-T, Vuong T-T, La V-P, Ho M-T, Nghiem K-CP, Nguyen HLT, et al. Global Evolution of Research in Artificial Intelligence in Health and Medicine: A Bibliometric Study. Journal of Clinical Medicine. 2019; 8(3):360. https://doi.org/10.3390/jcm8030360
Chicago/Turabian StyleTran, Bach Xuan, Giang Thu Vu, Giang Hai Ha, Quan-Hoang Vuong, Manh-Tung Ho, Thu-Trang Vuong, Viet-Phuong La, Manh-Toan Ho, Kien-Cuong P. Nghiem, Huong Lan Thi Nguyen, and et al. 2019. "Global Evolution of Research in Artificial Intelligence in Health and Medicine: A Bibliometric Study" Journal of Clinical Medicine 8, no. 3: 360. https://doi.org/10.3390/jcm8030360