Acetazolamide Therapy in Patients with Heart Failure: A Meta-Analysis

 , , , and
, , , and 
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Literature Review
2.2. Selection Criteria
2.3. Data Abstraction
2.4. Statistical Analysis
3. Results
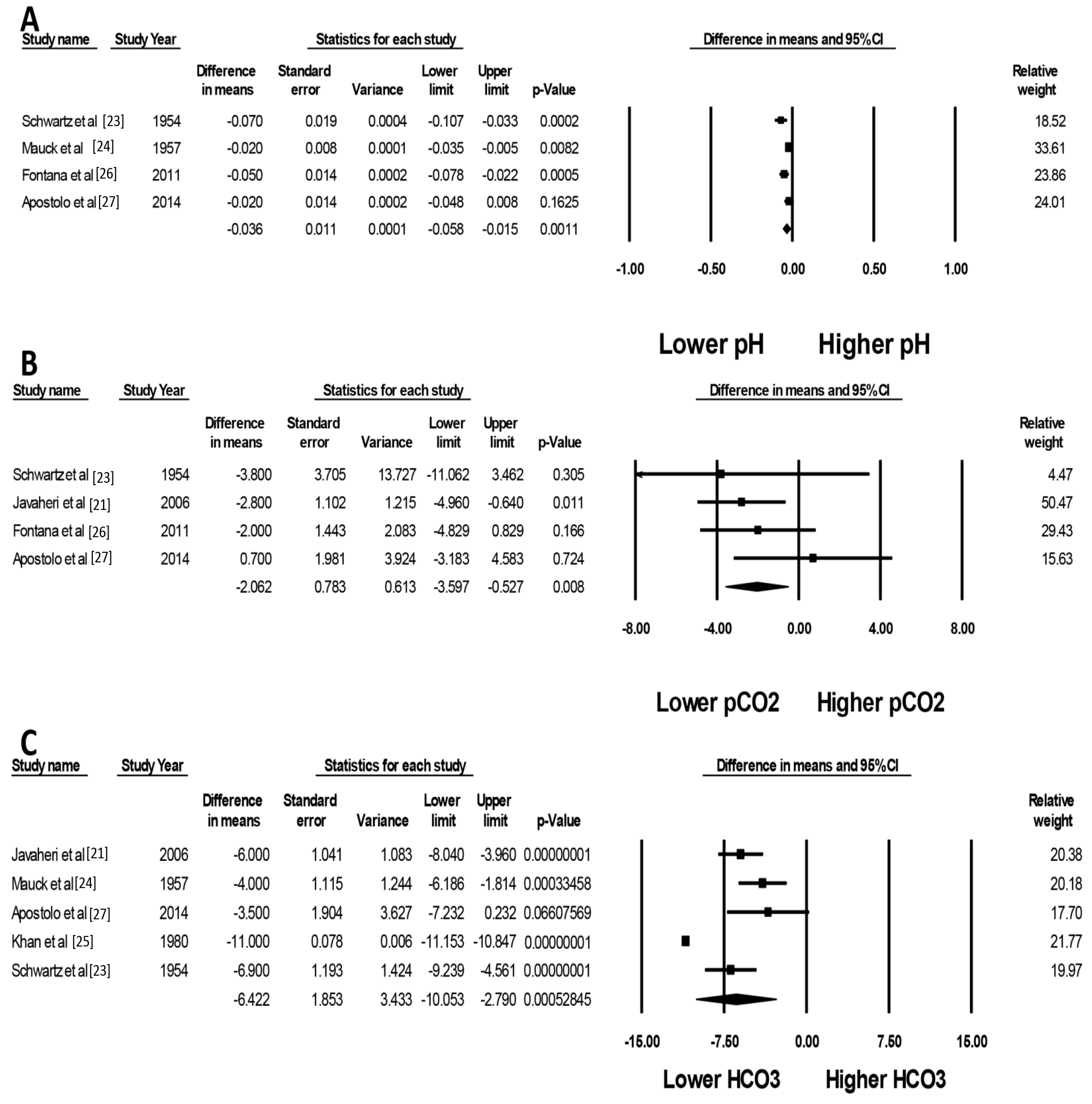
3.1. Effects of Acetazolamide on Acid/Base Balance in HF Patients
3.2. Effects of Acetazolamide on Apnea Indexes
3.3. Sensitivity Analysis
3.4. Evaluation for Publication Bias
4. Discussion
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Cook, C.; Cole, G.; Asaria, P.; Jabbour, R.; Francis, D.P. The annual global economic burden of heart failure. Int. J. Cardiol. 2014, 171, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Bowman, B.N.; Nawarskas, J.J.; Anderson, J.R. Treating Diuretic Resistance: An Overview. Cardiol. Rev. 2016, 24, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Friedberg, C.K.; Taymor, R.; Minor, J.B.; Halpern, M. The use of diamox, a carbonic anhydrase inhibitor, as an oral diuretic in patients with congestive heart failure. N. Engl. J. Med. 1953, 248, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, G.R.; Baxter, M.R.; Hejtmancik, M.R.; Moran, A.R. Diamox: New oral nonmercurial, nontoxic diuretic for the treatment of congestive heart failure. Tex. State J. Med. 1954, 50, 209–213. [Google Scholar] [PubMed]
- Belsky, H. Use of a new oral diuretic, diamox, in congestive heart failure. N. Engl. J. Med. 1953, 249, 140–143. [Google Scholar] [CrossRef] [PubMed]
- Suarez, R.M., Sr.; Suarez, R.M., Jr.; Buso, R.; Sabater, J. Diamox; a new non-mercurial diuretic for oral administration; clinical observations on the treatment of edema due to cardiac failure. Bol. Asoc. Med. P. R. 1953, 45, 381–386. [Google Scholar]
- Ellison, D.H. The physiologic basis of diuretic synergism: Its role in treating diuretic resistance. Ann. Intern. Med. 1991, 114, 886–894. [Google Scholar] [CrossRef]
- Fallahzadeh, M.A.; Dormanesh, B.; Fallahzadeh, M.K.; Roozbeh, J.; Fallahzadeh, M.H.; Sagheb, M.M. Acetazolamide and Hydrochlorothiazide Followed by Furosemide Versus Furosemide and Hydrochlorothiazide Followed by Furosemide for the Treatment of Adults With Nephrotic Edema: A Randomized Trial. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2017, 69, 420–427. [Google Scholar] [CrossRef]
- Zahedi, K.; Barone, S.; Xu, J.; Soleimani, M. Potentiation of the effect of thiazide derivatives by carbonic anhydrase inhibitors: Molecular mechanisms and potential clinical implications. PLoS ONE 2013, 8, e79327. [Google Scholar] [CrossRef]
- Imiela, T.; Budaj, A. Acetazolamide as Add-on Diuretic Therapy in Exacerbations of Chronic Heart Failure: A Pilot Study. Clin. Drug Investig. 2017, 37, 1175–1181. [Google Scholar] [CrossRef]
- Ritchie, N.D.; Baggott, A.V.; Andrew Todd, W.T. Acetazolamide for the prevention of acute mountain sickness—A systematic review and meta-analysis. J. Travel Med. 2012, 19, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Sii, F.; Horsburgh, J.; Shah, P. Anuric acute kidney injury due to low dose oral acetazolamide with hypercrystalluria. Clin. Exp. Ophthalmol. 2017, 45, 927–929. [Google Scholar] [CrossRef]
- Bekfani, T.; Abraham, W.T. Current and future developments in the field of central sleep apnoea. Europace 2016, 18, 1123–1134. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Easterbrook, P.J.; Berlin, J.A.; Gopalan, R.; Matthews, D.R. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- Javaheri, S. Acetazolamide improves central sleep apnea in heart failure: A double-blind, prospective study. Am. J. Respir. Crit. Care Med. 2006, 173, 234–237. [Google Scholar] [CrossRef] [PubMed]
- Javaheri, S.; Sands, S.A.; Edwards, B.A. Acetazolamide attenuates Hunter-Cheyne-Stokes breathing but augments the hypercapnic ventilatory response in patients with heart failure. Ann. Am. Thorac. Soc. 2014, 11, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, W.B.; Relman, A.S.; Leaf, A. Oral administration of a potent carbonic anhydrase inhibitor (diamox). III. Its use as a diuretic in patients with severe congestive heart failure due to cor pulmonale. Ann. Intern. Med. 1955, 42, 79–89. [Google Scholar] [PubMed]
- Langford, H.G.; Mauck, H.P. Effect of acetazoleamide (diamox) on the electrolyte patterns of ambulatory patients with mild congestive failure. Am. J. Med. Sci. 1957, 233, 176–181. [Google Scholar] [PubMed]
- Khan, M.I. Treatment of refractory congestive heart failure and normokalemic hypochloremic alkalosis with acetazolamide and spironolactone. Can. Med. Assoc. J. 1980, 123, 883–887. [Google Scholar] [PubMed]
- Fontana, M.; Emdin, M.; Giannoni, A.; Iudice, G.; Baruah, R.; Passino, C. Effect of acetazolamide on chemosensitivity, Cheyne-Stokes respiration, and response to effort in patients with heart failure. Am. J. Cardiol. 2011, 107, 1675–1680. [Google Scholar] [CrossRef] [PubMed]
- Apostolo, A.; Agostoni, P.; Contini, M.; Antonioli, L.; Swenson, E.R. Acetazolamide and inhaled carbon dioxide reduce periodic breathing during exercise in patients with chronic heart failure. J. Card. Fail. 2014, 20, 278–288. [Google Scholar] [CrossRef]
- Verbrugge, F.H.; Dupont, M.; Bertrand, P.B.; Nijst, P.; Penders, J.; Dens, J.; Verhaert, D.; Vandervoort, P.; Tang, W.H.W.; Mullens, W. Determinants and impact of the natriuretic response to diuretic therapy in heart failure with reduced ejection fraction and volume overload. Acta Cardiol. 2015, 70, 265–273. [Google Scholar] [CrossRef] [Green Version]
- Moyer, J.H.; Ford, R.V. Laboratory and clinical observations on ethoxzolamide (cardrase) as a diuretic agent. Am. J. Cardiol. 1958, 1, 497–504. [Google Scholar] [CrossRef]
- Dharia, S.M.; Brown, L.K. Epidemiology of Sleep-Disordered Breathing and Heart Failure: What Drives What. Curr. Heart Fail. Rep. 2017, 14, 351–364. [Google Scholar] [CrossRef]
- Aurora, R.N.; Chowdhuri, S.; Ramar, K.; Bista, S.R.; Casey, K.R.; Lamm, C.I.; Kristo, D.A.; Mallea, J.M.; Rowley, J.A.; Zak, R.S.; et al. The treatment of central sleep apnea syndromes in adults: Practice parameters with an evidence-based literature review and meta-analyses. Sleep 2012, 35, 17–40. [Google Scholar] [CrossRef]
- Verbraecken, J.; Willemen, M.; De Cock, W.; Coen, E.; Van de Heyning, P.; De Backer, W. Central sleep apnea after interrupting longterm acetazolamide therapy. Respir. Physiol. 1998, 112, 59–70. [Google Scholar] [CrossRef]
- Massumi, R.A.; Evans, J.M. Studies on the continuous use of a carbonic anhydrase inhibitor (diamox) in ambulatory patients. Am. Heart J. 1955, 49, 626–632. [Google Scholar] [CrossRef]
- Kataoka, H. Treatment of hypochloremia with acetazolamide in an advanced heart failure patient and importance of monitoring urinary electrolytes. J. Cardiol. Cases 2018, 17, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Leon Jimenez, D.; Gomez Huelgas, R.; Fernandez Romero, A.J.; Lopez Chozas, J.M.; Perez de Isla, L.; Miramontes Gonzalez, J.P. Diuretic treatment of the patient with diabetes and heart failure. Role of SGLT2 inhibitors and similarities with carbonic anhydrase inhibitors. Rev. Clin. Esp. 2018. [Google Scholar] [CrossRef]
- Mullens, W.; Verbrugge, F.H.; Nijst, P.; Martens, P.; Tartaglia, K.; Theunissen, E.; Bruckers, L.; Droogne, W.; Troisfontaines, P.; Damman, K.; et al. Rationale and design of the ADVOR (Acetazolamide in Decompensated Heart Failure with Volume Overload) trial. Eur. J. Heart Fail. 2018, 20, 1591–1600. [Google Scholar] [CrossRef] [PubMed]
- Nunez, J.; Heredia, R.; Paya, A.; Sanchis, I.; Del Prado, S.; Minana, G.; Santas, E.; de la Espriella, R.; Núñez, E.; Sanchis, J.; et al. Use of acetazolamide in the treatment of patients with refractory congestive heart failure. Cardiovasc. Ther. 2018, 36, e12465. [Google Scholar] [CrossRef] [PubMed]
- Terziyski, K.; Draganova, A. Central Sleep Apnea with Cheyne-Stokes Breathing in Heart Failure—From Research to Clinical Practice and Beyond. Adv. Exp. Med. Biol. 2018, 1067, 327–351. [Google Scholar] [PubMed]
- Verbrugge, F.H. Editor’s Choice-Diuretic resistance in acute heart failure. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 379–389. [Google Scholar] [CrossRef] [PubMed]
- Verbrugge, F.H.; Martens, P.; Ameloot, K.; Haemels, V.; Penders, J.; Dupont, M.; Tang, W.H.W.; Droogné, W.; Mullens, W. Spironolactone to increase natriuresis in congestive heart failure with cardiorenal syndrome. Acta Cardiol. 2018, 1–8. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Author, Year) | Javaheri, 2006 [21] | Javaheri, 2014 [22] | Imiela, 2017 [10] | |
|---|---|---|---|---|
| Method | Study design | RCT, double-blind cross-over placebo and acetazolamide | RCT, double-blind cross-over placebo and acetazolamide | RCT, single-center, unblinded |
| Total number | 12 | 6 | 20 | |
| Patient sample | Stable systolic heart failure | Stable systolic heart failure | Patient hospitalized with chronic heart failure exacerbation | |
| CHF definition | Systolic HF (EF < 35%) with Cheyne-Stokes breathing and AHI > 15/h | Systolic heart failure and CSA (AHI > 15/h) | EF < 50%, signs of volume overload | |
| Acetazolamide dosing | Acetazolamide 3.5–4 mg/kg + KCL 60 meq | Acetazolamide 3.5–4 mg/kg + KCL 60 meq | Once daily (dose-adjusted to body weight, range from 250 mg to 500 mg) as add-on diuretics to furosemide | |
| Description | RCT about acetazolmide but designed for sleep disorder | RCT about acetazolmide but designed for sleep disorder | RCT dedicated to acetazolamide | |
| Cochrane risk of bias | Selection | Low | Low | Low |
| Performance | Low | Low | High | |
| Detection | Low | Low | High | |
| Attrition | Low | Low | Low | |
| Reporting | Low | Low | Low | |
| Other | Low | Low | Low |
| Study (Author, Year) | Schwartz, 1955 [23] | Mauck, 1957 [24] | Khan, 1980 [25] | Fontana, 2011 [26] | Apostolo, 2014 [27] | Verbrugge, 2015 [28] | |
|---|---|---|---|---|---|---|---|
| Method | Study design | Cohort, time series | Cohort, time series | Cohort, time series | Cohort | Cohort | Cohort |
| Total number | 17 | 14 | 74 | 12 | 20 | 54 | |
| Patient sample | Severe CHF with cor pulmonale | Stable CHF | Hospitalized decompensated CHF | CHF with periodic breathing | CHF with periodic breathing | Hospitalized decompensated CHF | |
| CHF definition | Clinical diagnosis with severe pulmonary disease, with ECG or Xray change of right heart enlargement or strain | Fully digitalized ambulatory CHF on 1 gm diet, mostly edema free. Wash out from other diuretics for two weeks | Patients diagnosed with CHF that failed treatment with furosemide, spironolactone and salt restriction | EF < 50%, with AHI > 15 | EF < 40%, with periodic breathing during exercise | At least three signs of volume overload, EF < 45% | |
| Acetazolamide dosing | 1–1.5 gm over 24 h | 250 mg qday | 250 mg qid (1 g per day), used as a replacement of furosemide | 250 mg po bid for 4 days | 500 mg IV and prolonged 2 gm over 24 h | 250 mg qday | |
| Description | Using acetazolamide to treat patient with cor pulmonale and respiratory acidosis | Studying effect of acetazolamide in ambulatory CHF, aiming at electrolyte values during therapy | Using acetazolamide instead of furosemide for diuresis | Measure breathing parameters with ABG analysis before and after acetazolamide treatment | Measured respiratory pattern before and after acetazolamide treatment | Cohort finding predictor of natriuresis | |
| Quality assessment (Newcastle-Ottawa scale) | Selection | 2 | 2 | 2 - Independent validation - Obvious series of cases | 3 - Using cohort of CHF - Non-exposed cohort is self prior to acetazolamide - Secure record | 3 - Using cohort of CHF - Non-exposed cohort is self prior to acetazolamide - secure record | 3 - True representation of CHF - Same community of control - Secure record |
| Comparability | 1 | 1 | 1 - Study controls by using prior-self prior to treatment with acetazolamide | 1 - Study controls by using prior-self prior to treatment with acetazolamide | 1 - Study controls by using prior-self prior to treatment with acetazolamide | 2 - Using multivariate analysis and still showed acetazolamide as important factor | |
| Outcome | 1 | 1 | 1 -Secure record (hospital) | NA | NA | NA | |
| Exposure | NA | NA | NA | 2 - Record linkage - Long follow up | 2 - Record linkage - Long follow up | 3 -Record linkage - Long follow up - Complete follow up of all subjects |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wongboonsin, J.; Thongprayoon, C.; Bathini, T.; Ungprasert, P.; Aeddula, N.R.; Mao, M.A.; Cheungpasitporn, W. Acetazolamide Therapy in Patients with Heart Failure: A Meta-Analysis. J. Clin. Med. 2019, 8, 349. https://doi.org/10.3390/jcm8030349
Wongboonsin J, Thongprayoon C, Bathini T, Ungprasert P, Aeddula NR, Mao MA, Cheungpasitporn W. Acetazolamide Therapy in Patients with Heart Failure: A Meta-Analysis. Journal of Clinical Medicine. 2019; 8(3):349. https://doi.org/10.3390/jcm8030349
Chicago/Turabian StyleWongboonsin, Janewit, Charat Thongprayoon, Tarun Bathini, Patompong Ungprasert, Narothama Reddy Aeddula, Michael A. Mao, and Wisit Cheungpasitporn. 2019. "Acetazolamide Therapy in Patients with Heart Failure: A Meta-Analysis" Journal of Clinical Medicine 8, no. 3: 349. https://doi.org/10.3390/jcm8030349