Outcomes of Older Patients (≥60 years) with New-Onset Idiopathic Nephrotic Syndrome Receiving Immunosuppressive Regimen: A Multicentre Study of 116 Patients

 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Data Collection and Definitions
2.3. Statistical Analysis
3. Results
3.1. Renal Presentation
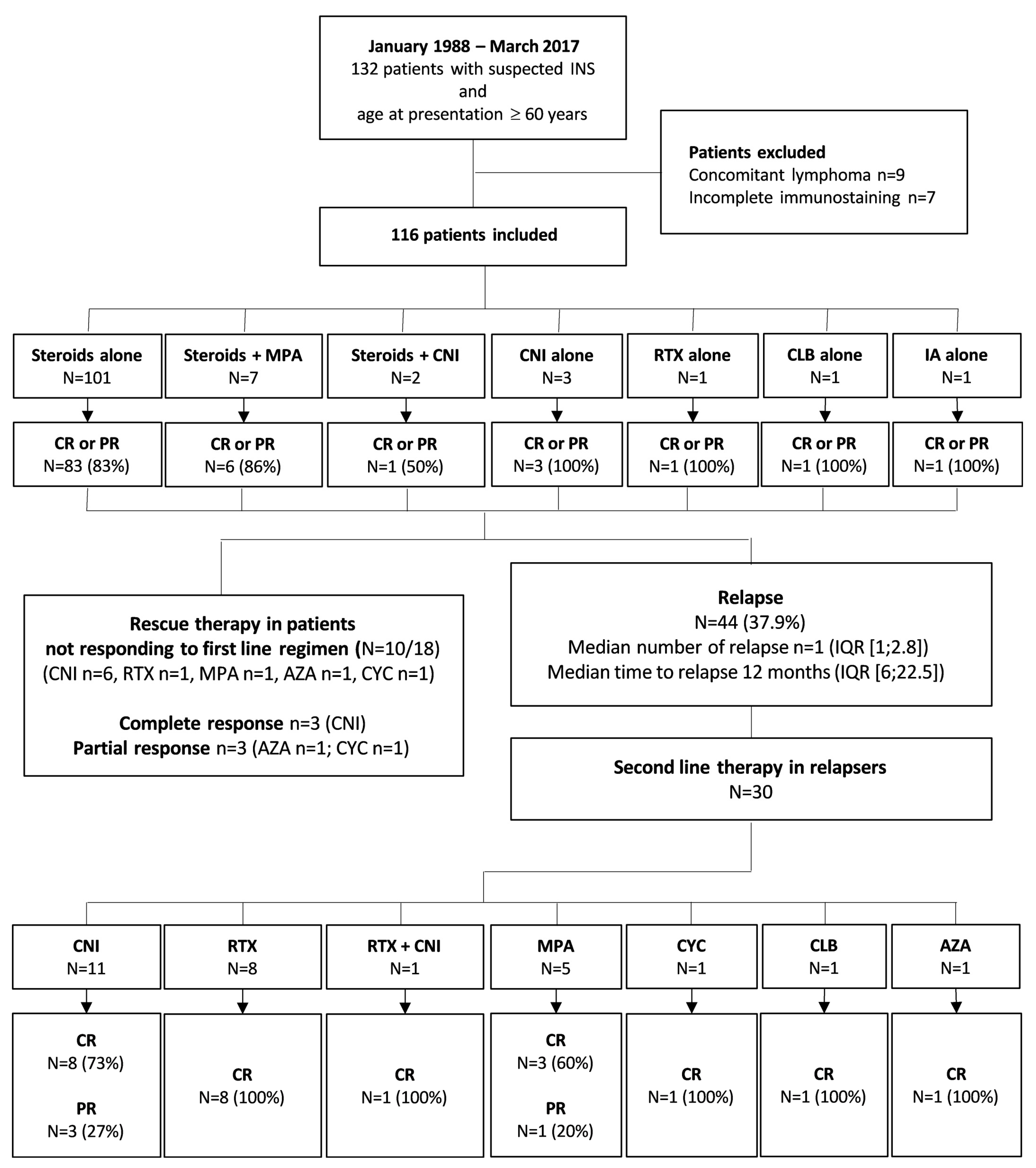
3.2. Treatments of First Flare and Renal Outcomes
3.3. Management of Relapses and Incomplete Renal Response
3.4. Adverse Events and Long-Term Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Vivarelli, M.; Massella, L.; Ruggiero, B.; Emma, F. Minimal Change Disease. Clin. J. Am. Soc. Nephrol. 2017, 12, 332–345. [Google Scholar] [CrossRef] [PubMed]
- Maas, R.J.; Deegens, J.K.; Wetzels, J.F. Permeability factors in idiopathic nephrotic syndrome: Historical perspectives and lessons for the future. Nephrol. Dial. Transplant. 2014, 29, 2207–2216. [Google Scholar] [CrossRef] [PubMed]
- Sahali, D.; Sendeyo, K.; Mangier, M.; Audard, V.; Zhang, S.Y.; Lang, P.; Ollero, M.; Pawlak, A. Immunopathogenesis of idiopathic nephrotic syndrome with relapse. Semin. Immunopathol. 2014. [Google Scholar] [CrossRef] [PubMed]
- Maas, R.J.; Deegens, J.K.; Smeets, B.; Moeller, M.J.; Wetzels, J.F. Minimal change disease and idiopathic FSGS: Manifestations of the same disease. Nat. Rev. Nephrol. 2016, 12, 768–776. [Google Scholar] [CrossRef] [PubMed]
- Mathieson, P.W. Immune dysregulation in minimal change nephropathy. Nephrol. Dial. Transplant. 2003, 18 (Suppl. 6), vi26–vi29. [Google Scholar] [CrossRef]
- Jamin, A.; Berthelot, L.; Couderc, A.; Chemouny, J.M.; Boedec, E.; Dehoux, L.; Abbad, L.; Dossier, C.; Daugas, E.; Monteiro, R.C.; et al. Autoantibodies against podocytic UCHL1 are associated with idiopathic nephrotic syndrome relapses and induce proteinuria in mice. J. Autoimmun. 2018, 89, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Lombel, R.M.; Gipson, D.S.; Hodson, E.M. Kidney Disease: Improving Global Outcomes Treatment of steroid-sensitive nephrotic syndrome: New guidelines from KDIGO. Pediatr. Nephrol. 2013, 28, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Pasini, A.; Benetti, E.; Conti, G.; Ghio, L.; Lepore, M.; Massella, L.; Molino, D.; Peruzzi, L.; Emma, F.; Fede, C.; et al. The Italian Society for Pediatric Nephrology (SINePe) consensus document on the management of nephrotic syndrome in children: Part I—Diagnosis and treatment of the first episode and the first relapse. Ital. J. Pediatr. 2017, 43, 41. [Google Scholar] [CrossRef] [PubMed]
- Samuel, S.; Bitzan, M.; Zappitelli, M.; Dart, A.; Mammen, C.; Pinsk, M.; Cybulsky, A.V.; Walsh, M.; Knoll, G.; Hladunewich, M.; et al. Canadian Society of Nephrology Commentary on the 2012 KDIGO Clinical Practice Guideline for Glomerulonephritis: Management of Nephrotic Syndrome in Children. Am. J. Kidney Dis. 2014, 63, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Pravitsitthikul, N.; Willis, N.S.; Hodson, E.M.; Craig, J.C. Non-corticosteroid immunosuppressive medications for steroid-sensitive nephrotic syndrome in children. Cochrane database Syst. Rev. 2013, CD002290. [Google Scholar] [CrossRef] [PubMed]
- Cattran, D.C.; Alexopoulos, E.; Heering, P.; Hoyer, P.F.; Johnston, A.; Meyrier, A.; Ponticelli, C.; Saito, T.; Choukroun, G.; Nachman, P.; et al. Cyclosporin in idiopathic glomerular disease associated with the nephrotic syndrome: Workshop recommendations. Kidney Int. 2007, 72, 1429–1447. [Google Scholar] [CrossRef] [PubMed]
- Gruppen, M.P.; Bouts, A.H.; Jansen-van der Weide, M.C.; Merkus, M.P.; Zurowska, A.; Maternik, M.; Massella, L.; Emma, F.; Niaudet, P.; Cornelissen, E.A.M.; et al. A randomized clinical trial indicates that levamisole increases the time to relapse in children with steroid-sensitive idiopathic nephrotic syndrome. Kidney Int. 2018, 93, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Takei, T.; Itabashi, M.; Moriyama, T.; Kojima, C.; Shiohira, S.; Shimizu, A.; Tsuruta, Y.; Ochi, A.; Amemiya, N.; Mochizuki, T.; et al. Effect of single-dose rituximab on steroid-dependent minimal-change nephrotic syndrome in adults. Nephrol. Dial. Transplant. 2013, 28, 1225–1232. [Google Scholar] [CrossRef] [PubMed]
- Guitard, J.; Hebral, A.-L.; Fakhouri, F.; Joly, D.; Daugas, E.; Rivalan, J.; Guigonis, V.; Ducret, F.; Presne, C.; Pirson, Y.; et al. Rituximab for minimal-change nephrotic syndrome in adulthood: Predictive factors for response, long-term outcomes and tolerance. Nephrol. Dial. Transplant. 2014, 29, 2084–2091. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, R.D.; Hulse, E.; Rigden, S. Rituximab therapy for steroid-dependent minimal change nephrotic syndrome. Pediatr. Nephrol. 2006, 21, 1698–1700. [Google Scholar] [CrossRef] [PubMed]
- Munyentwali, H.; Bouachi, K.; Audard, V.; Remy, P.; Lang, P.; Mojaat, R.; Deschenes, G.; Ronco, P.M.; Plaisier, E.M.; Dahan, K.Y. Rituximab is an efficient and safe treatment in adults with steroid-dependent minimal change disease. Kidney Int. 2013, 83, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.H.J.; Chung, J.-J.; Akilesh, S.; Koziell, A.; Jain, S.; Hodgin, J.B.; Miller, M.J.; Stappenbeck, T.S.; Miner, J.H.; Shaw, A.S. B cell–derived IL-4 acts on podocytes to induce proteinuria and foot process effacement. JCI Insight 2017, 2, e81836. [Google Scholar] [CrossRef] [PubMed]
- Rémy, P.; Audard, V.; Natella, P.A.; Pelle, G.; Dussol, B.; Leray-Moragues, H.; Vigneau, C.; Bouachi, K.; Dantal, J.; Vrigneaud, L.; et al. An open-label randomized controlled trial of low-dose corticosteroid plus enteric-coated mycophenolate sodium versus standard corticosteroid treatment for minimal change nephrotic syndrome in adults (MSN Study). Kidney Int. 2018, 94, 1217–1226. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Liu, Z.; Wang, L.; Wang, R.; Ding, G.; Shi, W.; Fu, P.; He, Y.; Cheng, G.; Wu, S.; et al. Tacrolimus Monotherapy after Intravenous Methylprednisolone in Adults with Minimal Change Nephrotic Syndrome. J. Am. Soc. Nephrol. 2017, 28, 1286–1295. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, A. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef] [PubMed]
- Waldman, M.; Crew, R.J.; Valeri, A.; Busch, J.; Stokes, B.; Markowitz, G.; D’Agati, V.; Appel, G. Adult minimal-change disease: Clinical characteristics, treatment and outcomes. Clin. J. Am. Soc. Nephrol. 2007, 2, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Tse, K.-C.; Lam, M.-F.; Yip, P.-S.; Li, F.-K.; Choy, B.-Y.; Lai, K.-N.; Chan, T.-M. Idiopathic minimal change nephrotic syndrome in older adults: Steroid responsiveness and pattern of relapses. Nephrol. Dial. Transplant. 2003, 18, 1316–1320. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, M.; Katafuchi, R.; Yanase, T.; Ikeda, K.; Tanaka, H.; Fujimi, S. Steroid responsiveness and frequency of relapse in adult-onset minimal change nephrotic syndrome. Am. J. Kidney Dis. 2002, 39, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.-J.; Hsu, S.-C.; Chen, F.-F.; Sung, J.-M.; Tseng, C.-C.; Wang, M.-C. Adult-Onset Minimal Change Disease among Taiwanese. Am. J. Nephrol. 2001, 21, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Maas, R.J.; Deegens, J.K.; Beukhof, J.R.; Reichert, L.J.; Ten Dam, M.A.; Beutler, J.J.; van den Wall Bake, A.W.L.; Rensma, P.L.; Konings, C.J.; Geerse, D.A.; et al. The Clinical Course of Minimal Change Nephrotic Syndrome With Onset in Adulthood or Late Adolescence: A Case Series. Am. J. Kidney Dis. 2017, 69, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Meyrier, A.; Niaudet, P. Acute kidney injury complicating nephrotic syndrome of minimal change disease. Kidney Int. 2018, 94, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Tu, Y.-M.; Zhou, C.; Zhang, L.-H.; Liu, Z. Risk factors of venous thromboembolism in focal segmental glomerulosclerosis with nephrotic syndrome. Clin. Exp. Nephrol. 2016, 20, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-S.; Liverman, R.S.; Garro, R.; George, R.P.; Glumova, A.; Karp, A.; Jernigan, S.; Warshaw, B. Ofatumumab for the treatment of childhood nephrotic syndrome. Pediatr. Nephrol. 2017, 32, 835–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, B. Ofatumumab for rituximab-resistant nephrotic syndrome. N. Engl. J. Med. 2014, 370, 1268–1270. [Google Scholar] [CrossRef] [PubMed]
- Gulati, A.; Sinha, A.; Jordan, S.C.; Hari, P.; Dinda, A.K.; Sharma, S.; Srivastava, R.N.; Moudgil, A.; Bagga, A. Efficacy and safety of treatment with rituximab for difficult steroid-resistant and -dependent nephrotic syndrome: Multicentric report. Clin. J. Am. Soc. Nephrol. 2010, 5, 2207–2212. [Google Scholar] [CrossRef] [PubMed]
- Magnasco, A.; Ravani, P.; Edefonti, A.; Murer, L.; Ghio, L.; Belingheri, M.; Benetti, E.; Murtas, C.; Messina, G.; Massella, L.; et al. Rituximab in children with resistant idiopathic nephrotic syndrome. J. Am. Soc. Nephrol. 2012, 23, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Dahan, K.; Debiec, H.; Plaisier, E.; Cachanado, M.; Rousseau, A.; Wakselman, L.; Michel, P.A.; Mihout, F.; Dussol, B.; Matignon, M.; et al. Rituximab for Severe Membranous Nephropathy: A 6-Month Trial with Extended Follow-Up. J. Am. Soc. Nephrol. 2017, 28, 348–358. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Patients N = 116 |
|---|---|
| Patients | |
| Age at presentation (years; median (IQR)) | 68 (64–77) |
| Male gender (n, %) | 72 (62) |
| BMI (kg/m²) | 25.6 (23.4–28.3) |
| Diabetes mellitus (n, %) | 19 (16.3) |
| Insulin (n, %) | 11 (61.1) |
| Autoimmune disease (n, %) | 14 (12) |
| Previous or concomitant cancer * (n, %) | 17 (14.7) |
| Time between cancer and INS (months; median (IQR)) | 60 (19–99) |
| Renal Presentation | |
| UPCr (g/g; median (IQR)) | 7 (5–10.8) |
| Serum albumin (g/L; median (IQR)) | 18 (12–24.5) |
| Serum creatinine (µmol/L; median (IQR)) | 121 (89–200) |
| eGFR (ml/min/1.73 m2; median (IQR)) | 50 (26; 67) |
| Acute kidney injury (n, %) | 61 (52.6) |
| Stage 1 (n, %) | 29 (25) |
| Stage 2 (n, %) | 14 (12.1) |
| Stage 3 (n, %) | 18 (15.5) |
| Haematuria (n, %) | 51 (44) |
| Hypertension (n, %) | 82 (71) |
| Renal Biopsy | |
| MCD (n, %) | 80 (69) |
| FSGS (n, %) | 36 (31) |
| IgM deposits (n, %) | 23 (19.8) |
| C3 deposits (n, %) | 32 (27.6) |
| Acute tubular necrosis (n, %) | 42 (36.2) |
| Percentage of glomerular sclerosis (median (IQR)) | 5 (0–20) |
| Percentage of interstitial fibrosis (median (IQR)) | 5 (0–15) |
| Characteristics | N = 116 |
|---|---|
| First-Line Treatment | |
| Immunosuppressive regimen | |
| Steroids (n, %) | 101 (87) |
| Pulses | 5 (4.3) |
| MPA and steroids (n, %) | 7 (6) |
| CNI (n, %) | 3 (2.6) |
| CNI and steroids (n, %) | 2 (1.7) |
| Rituximab (n, %) | 1 (0.9) |
| Other treatments (n, %) | 2 (1.7) |
| RAAS blocking agents (n, %) | 78 (67.2) |
| Response to Treatment | |
| Complete response (n, %) | 76 (65.5) |
| Partial response (n, %) | 20 (17.2) |
| No response (n, %) | 18 (15.5) |
| Time from the onset to the best renal response (days) | 61 (30–123) |
| Withdrawal of steroids (n, %) | 61 (52.6) |
| Relapse (n, %) | 44 (37.9) |
| Time from the best renal response (months; median (IQR)) | 12 (6–22.5) |
| On-going immunosuppressive treatment at the relapse | 23 (52.7) |
| Status at Last Follow-Up | |
| Follow-up duration (months; median (IQR)) | 34 (11.8–56.5) |
| Alive (n, %) | 109 (94) |
| Sustained complete response (n, %) | 78 (67.2) |
| eGFR (mL/min/1.73 m2) | 64 (41–79) |
| ESRD (n, %) | 5 (4.3) |
| Time interval from the onset (months; median (IQR)) | 25 (0–46) |
| Characteristics | N = 23 | |
|---|---|---|
| Line of treatment (n, %) | ||
| First | 1 (4.3) | |
| Second | 10 (43.6) | |
| Third | 9 (39.1) | |
| Fourth | 3 (13) | |
| Delayed Neutropenia | None | |
| INS Response according to the Line of Treatment | Median Time to Response | |
| First-Line, CR/PR/NR | 1/0/0 | 284 days |
| Second-Line, CR/PR/NR | 9/0/1 | 42 days |
| Third-Line, CR/PR/NR | 3/3/0 | 25 days |
| Fourth-Line, CR/PR/NR | 1/0/0 | 30 days |
| Relapse after Rituximab (n, %) * | Median Time to Response | |
| First-Line | 1 (100) | 15 months |
| Second-Line | 2 (20) | 33 months |
| Third-Line | 3 (33) | 10 months |
| Fourth-Line | 1 (100) | 11 months |
| Adverse Events | N (%) |
|---|---|
| Pulmonary Embolism | 1 (0.8) |
| Deep Vein Thrombosis | 3 (2.9) |
| Acute Kidney Injury | 11 (9.5) |
| Diabetes Mellitus | |
| De novo | 16 (13.8) |
| Worsening | 11 (9.5) |
| De novo Hypertension | 28 (24.1) |
| Infection Requiring Hospitalization | 25 (21.6) |
| Cancer | 15 (12.9) |
| Time from the Onset of INS (months; median (IQR)) | 23 (13–44) |
| Osteoporosis | 14 (12.1) |
| Dyslipidaemia | 50 (43.1) |
| Psychiatric Disorder | 19 (16.4) |
| Adrenal Failure | 7 (6.3) |
| Significant Tremor | 3 (2.6) |
| Hirsutism | 4 (3.4) |
| Gingival Hypertrophy | 5 (4.3) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colliou, E.; Karras, A.; Boffa, J.-J.; Ribes, D.; Garrouste, C.; Quintrec, M.L.; Daugas, E.; Huart, A.; Ducloux, D.; Hummel, A.; et al. Outcomes of Older Patients (≥60 years) with New-Onset Idiopathic Nephrotic Syndrome Receiving Immunosuppressive Regimen: A Multicentre Study of 116 Patients. J. Clin. Med. 2019, 8, 298. https://doi.org/10.3390/jcm8030298
Colliou E, Karras A, Boffa J-J, Ribes D, Garrouste C, Quintrec ML, Daugas E, Huart A, Ducloux D, Hummel A, et al. Outcomes of Older Patients (≥60 years) with New-Onset Idiopathic Nephrotic Syndrome Receiving Immunosuppressive Regimen: A Multicentre Study of 116 Patients. Journal of Clinical Medicine. 2019; 8(3):298. https://doi.org/10.3390/jcm8030298
Chicago/Turabian StyleColliou, Eloïse, Alexandre Karras, Jean-Jacques Boffa, David Ribes, Cyril Garrouste, Moglie Le Quintrec, Eric Daugas, Antoine Huart, Didier Ducloux, Aurélie Hummel, and et al. 2019. "Outcomes of Older Patients (≥60 years) with New-Onset Idiopathic Nephrotic Syndrome Receiving Immunosuppressive Regimen: A Multicentre Study of 116 Patients" Journal of Clinical Medicine 8, no. 3: 298. https://doi.org/10.3390/jcm8030298