Effect of Prophylactic Amiodarone Infusion on the Recurrence of Ventricular Arrhythmias in Out-of-Hospital Cardiac Arrest Survivors: A Propensity-Matched Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Methods
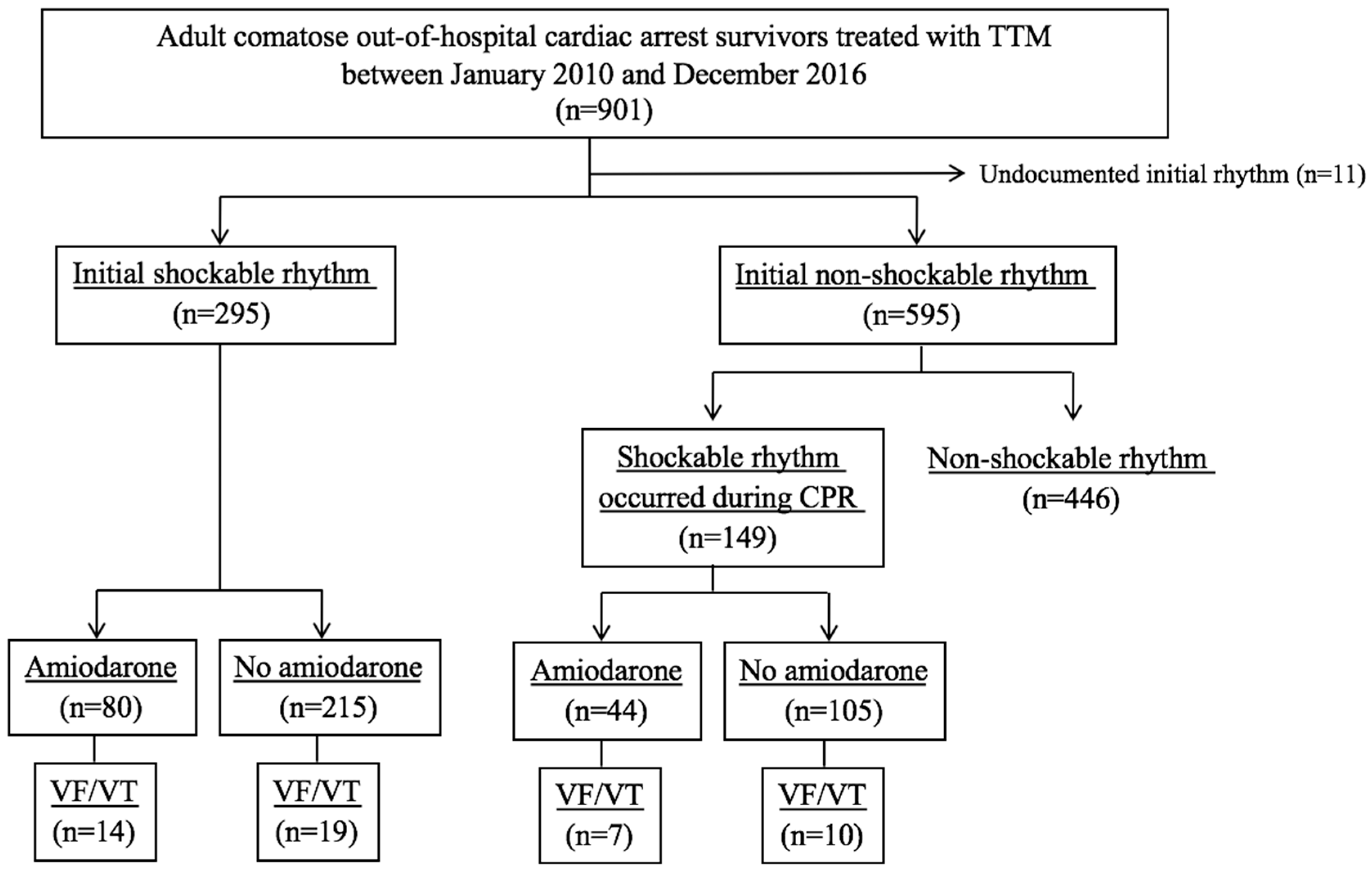
2.1. Setting and Study Population
2.2. TTM Protocol
2.3. Data Collection and Outcome
2.4. Statistical Analysis
3. Results
3.1. Comparison between the Prophylactic and Non-Prophylactic Groups
3.2. Recurrence of Ventricular Tachyarrhythmia
3.3. Analysis of Propensity-Score-Matched Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Despres, J.P.; Fullerton, H.J.; et al. Executive summary: Heart disease and stroke statistics--2016 update: A report from the American Heart Association. Circulation 2016, 133, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N. Engl. J. Med. 2002, 346, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, N.; Wetterslev, J.; Cronberg, T.; Erlinge, D.; Gasche, Y.; Hassager, C.; Horn, J.; Hovdenes, J.; Kjaergaard, J.; Kuiper, M.; et al. Targeted temperature management at 33 degrees C versus 36 degrees C after cardiac arrest. N. Engl. J. Med. 2013, 369, 2197–2206. [Google Scholar] [CrossRef] [PubMed]
- Kirkegaard, H.; Soreide, E.; de Haas, I.; Pettila, V.; Taccone, F.S.; Arus, U.; Storm, C.; Hassager, C.; Nielsen, J.F.; Sorensen, C.A.; et al. Targeted temperature management for 48 vs. 24 hours and neurologic outcome after out-of-hospital cardiac arrest: A randomized clinical trial. JAMA 2017, 318, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Callaway, C.W.; Donnino, M.W.; Fink, E.L.; Geocadin, R.G.; Golan, E.; Kern, K.B.; Leary, M.; Meurer, W.J.; Peberdy, M.A.; Thompson, T.M.; et al. Part 8: Post-cardiac arrest care: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2015, 132, S465–S482. [Google Scholar] [CrossRef] [PubMed]
- Tiainen, M.; Parikka, H.J.; Makijarvi, M.A.; Takkunen, O.S.; Sarna, S.J.; Roine, R.O. Arrhythmias and heart rate variability during and after therapeutic hypothermia for cardiac arrest. Crit. Care Med. 2009, 37, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Rolfast, C.L.; Lust, E.J.; de Cock, C.C. Electrocardiographic changes in therapeutic hypothermia. Crit. Care 2012, 16, R100. [Google Scholar] [CrossRef]
- Lebiedz, P.; Meiners, J.; Samol, A.; Wasmer, K.; Reinecke, H.; Waltenberger, J.; Eckardt, L. Electrocardiographic changes during therapeutic hypothermia. Resuscitation 2012, 83, 602–606. [Google Scholar] [CrossRef]
- Lee, W.S.; Nam, G.B.; Kim, S.H.; Choi, J.H.; Jo, U.; Kim, W.Y.; Oh, Y.S.; Park, K.N.; Seo, G.W.; Kim, K.H.; et al. ECG features and proarrhythmic potentials of therapeutic hypothermia. Heart 2016, 102, 1558–1565. [Google Scholar] [CrossRef]
- Kudenchuk, P.J.; Daya, M.; Dorian, P.; Resuscitation Outcomes Consortium Investigators. Amiodarone, lidocaine, or placebo in out-of-hospital cardiac arrest. N. Engl. J. Med. 2016, 375, 802–803. [Google Scholar] [CrossRef]
- Kim, Y.J.; Min, S.Y.; Lee, D.H.; Lee, B.K.; Jeung, K.W.; Lee, H.J.; Shin, J.; Ko, B.S.; Ahn, S.; Nam, G.B.; et al. The role of post-resuscitation electrocardiogram in patients with st-segment changes in the immediate post-cardiac arrest period. JACC Cardiovasc. Interv. 2017, 10, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P.R. Observational Studies; Springer: New York, NY, USA; Berlin, Germany, 1995. [Google Scholar]
- Kudenchuk, P.J.; Brown, S.P.; Daya, M.; Rea, T.; Nichol, G.; Morrison, L.J.; Leroux, B.; Vaillancourt, C.; Wittwer, L.; Callaway, C.W.; et al. Amiodarone, lidocaine, or placebo in out-of-hospital cardiac arrest. N. Engl. J. Med. 2016, 374, 1711–1722. [Google Scholar] [CrossRef] [PubMed]
- Julian, D.G.; Camm, A.J.; Frangin, G.; Janse, M.J.; Munoz, A.; Schwartz, P.J.; Simon, P. Randomised trial of effect of amiodarone on mortality in patients with left-ventricular dysfunction after recent myocardial infarction: EMIAT. European Myocardial Infarct Amiodarone Trial Investigators. Lancet 1997, 349, 667–674. [Google Scholar] [CrossRef]
- Cairns, J.A.; Connolly, S.J.; Roberts, R.; Gent, M. Randomised trial of outcome after myocardial infarction in patients with frequent or repetitive ventricular premature depolarisations: CAMIAT. Canadian amiodarone myocardial infarction arrhythmia trial investigators. Lancet 1997, 349, 675–682. [Google Scholar] [CrossRef]
- You, B.; Pu, J.; Liu, N.; Yu, R.; Ruan, Y.; Li, Y.; Wang, L. Effect of lidocaine and amiodarone on transmural heterogeneity of ventricular repolarization in isolated rabbit hearts model of sustained global ischemia. J. Huazhong Univ. Sci. Technolog. Med. Sci. 2005, 25, 400–403. [Google Scholar] [PubMed]
- Varbiro, G.; Toth, A.; Tapodi, A.; Bognar, Z.; Veres, B.; Sumegi, B.; Gallyas, F., Jr. Protective effect of amiodarone but not N-desethylamiodarone on postischemic hearts through the inhibition of mitochondrial permeability transition. J. Pharmacol. Exp. Ther. 2003, 307, 615–625. [Google Scholar] [CrossRef]
- Ide, T.; Tsutsui, H.; Kinugawa, S.; Utsumi, H.; Takeshita, A. Amiodarone protects cardiac myocytes against oxidative injury by its free radical scavenging action. Circulation 1999, 100, 690–692. [Google Scholar] [CrossRef]
- Khan, J.N.; Prasad, N.; Glancy, J.M. QTc prolongation during therapeutic hypothermia: Are we giving it the attention it deserves? Europace 2010, 12, 266–270. [Google Scholar] [CrossRef]
- Wira, C.R.; Becker, J.U.; Martin, G.; Donnino, M.W. Anti-arrhythmic and vasopressor medications for the treatment of ventricular fibrillation in severe hypothermia: A systematic review of the literature. Resuscitation 2008, 78, 21–29. [Google Scholar] [CrossRef]
- Hohnloser, S.H.; Klingenheben, T.; Singh, B.N. Amiodarone-associated proarrhythmic effects. A review with special reference to torsade de pointes tachycardia. Ann. Intern. Med. 1994, 121, 529–535. [Google Scholar] [CrossRef]
- Kudenchuk, P.J.; Cobb, L.A.; Copass, M.K.; Cummins, R.O.; Doherty, A.M.; Fahrenbruch, C.E.; Hallstrom, A.P.; Murray, W.A.; Olsufka, M.; Walsh, T. Amiodarone for resuscitation after out-of-hospital cardiac arrest due to ventricular fibrillation. N. Engl. J. Med. 1999, 341, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Kudenchuk, P.J.; Newell, C.; White, L.; Fahrenbruch, C.; Rea, T.; Eisenberg, M. Prophylactic lidocaine for post resuscitation care of patients with out-of-hospital ventricular fibrillation cardiac arrest. Resuscitation 2013, 84, 1512–1518. [Google Scholar] [CrossRef] [PubMed]
- Kudenchuk, P.J.; Leroux, B.G.; Daya, M.; Rea, T.; Vaillancourt, C.; Morrison, L.J.; Callaway, C.W.; Christenson, J.; Ornato, J.P.; Dunford, J.V.; et al. Antiarrhythmic drugs for nonshockable-turned-shockable out-of-hospital cardiac arrest: The ALPS study (Amiodarone, Lidocaine, or Placebo). Circulation 2017, 136, 2119–2131. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Total (N = 444) | No Prophylactic Amiodarone (n = 320) | Prophylactic Amiodarone (n = 124) | p Value |
|---|---|---|---|---|
| Age, years | 55.0 [45.0–65.0] | 56.0 [46.0–65.0] | 53.5 [42.3–64.0] | 0.20 |
| Male | 333 (75.0) | 242 (75.6) | 91 (73.4) | 0.63 |
| Past medical history | ||||
| History of cardiac arrest | 7 (1.6) | 6 (1.9) | 1 (0.8) | 0.68 |
| Acute coronary syndrome | 79 (17.8) | 59 (18.4) | 20 (16.1) | 0.57 |
| Arrhythmia | 27 (6.1) | 16 (5.0) | 11 (8.9) | 0.13 |
| Hypertension | 160 (36.0) | 128 (40.0) | 32 (25.8) | 0.005 |
| Diabetes | 88 (19.8) | 64 (20.0) | 24 (19.4) | 0.88 |
| Chronic pulmonary disease | 10 (2.3) | 5 (4.0) | 5 (1.6) | 0.15 |
| Chronic renal disease | 18 (4.1) | 17 (5.3) | 1 (0.8) | 0.03 |
| Liver cirrhosis | 3 (0.7) | 3 (0.9) | 0 (0.0) | 0.56 |
| Malignancy | 14 (3.2) | 14 (4.4) | 0 (0.0) | 0.009 |
| Vital signs | ||||
| Systolic pressure, mmHg | 119.5 [93.8-–141.0] | 116.0 [90.0–142.0] | 120.0 [100.0–140.0] | 0.79 |
| Diastolic pressure, mmHg | 70.5 [60.0–90.0] | 71.0 [60.0–90.0] | 70.0 [60.0–90.0] | 0.58 |
| Pulse rate, beats/min | 101.3 ± 27.7 | 101.4 ± 27.3 | 101.0 ± 29.9 | 0.89 |
| Body temperature, °C | 36.1 [35.5–36.4] | 36.1 [35.5–36.4] | 36.0 [35.3–36.4] | 0.26 |
| Laboratory findings, initial | ||||
| White blood cell, × 103/μL | 13.4 [10.6–18.1] | 13.3 [10.7–18.0] | 13.7 [10.5–18.6] | 0.68 |
| Hemoglobin, g/dL | 14.2 [12.4–15.4] | 13.9 [12.1–15.3] | 14.6 [12.8–15.7] | 0.03 |
| Sodium, mmol/L | 141.0 [138.0–143.0] | 141.0 [138.0–143.0] | 141.0 [138.0–143.0] | 0.62 |
| Potassium, mmol/L | 3.8 [3.4–4.4] | 3.9 [3.4–4.4] | 3.6 [3.3–4.3] | 0.02 |
| Calcium, mg/dL | 8.0 [7.4–8.7] | 8.0 [7.3–8.7] | 8.1 [7.3–8.8] | 0.11 |
| Magnesium, mg/dL | 2.2 [2.0–2.6] | 2.2 [1.9–2.5] | 2.4 [2.1–2.7] | 0.004 |
| Troponin-I, ng/mL | 0.605 [0.116–4.800] | 0.650 [0.124–4.870] | 0.529 [0.101–3.460] | 0.49 |
| CK-MB, ng/mL | 7.9 [2.8–30.4] | 7.8 [2.9–25.1] | 8.8 [2.3–43.8] | 0.58 |
| BNP, pg/mL | 129.6 [41.0–691.0] | 117.0 [40.0–448.2] | 183.0 [42.0–1357.5] | 0.17 |
| Outcome | Total Data (N = 444) | Matched Data (n = 186) | ||||
|---|---|---|---|---|---|---|
| No Prophylactic Amiodarone (n = 320) | Prophylactic Amiodarone (n = 124) | p-Value | No Prophylactic Amiodarone (n = 93) | Prophylactic Amiodarone (n = 93) | p-Value | |
| Recurrent shockable arrest | 29 (9.1) | 21 (16.9) | 0.02 | 11 (11.8) | 14 (15.1) | 0.51 |
| Survival discharge | 236 (73.8) | 98 (79.0) | 0.25 | 72 (77.4) | 73 (78.5) | 0.87 |
| Good neurologic outcome | 155 (48.4) | 71 (57.3) | 0.10 | 48 (51.6) | 55 (59.1) | 0.26 |
| Model | N | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|---|
| Crude | 444 | 2.046 | 1.117–3.746 | 0.02 |
| Multivariate adjusted | 441 | 1.946 | 1.038–3.647 | 0.04 |
| Propensity score matching | 186 | 1.321 | 0.574–3.043 | 0.51 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, B.K.; Youn, C.S.; Kim, Y.-J.; Ryoo, S.M.; Lim, K.S.; Nam, G.-B.; Kim, S.J.; Kim, W.Y. Effect of Prophylactic Amiodarone Infusion on the Recurrence of Ventricular Arrhythmias in Out-of-Hospital Cardiac Arrest Survivors: A Propensity-Matched Analysis. J. Clin. Med. 2019, 8, 244. https://doi.org/10.3390/jcm8020244
Lee BK, Youn CS, Kim Y-J, Ryoo SM, Lim KS, Nam G-B, Kim SJ, Kim WY. Effect of Prophylactic Amiodarone Infusion on the Recurrence of Ventricular Arrhythmias in Out-of-Hospital Cardiac Arrest Survivors: A Propensity-Matched Analysis. Journal of Clinical Medicine. 2019; 8(2):244. https://doi.org/10.3390/jcm8020244
Chicago/Turabian StyleLee, Byung Kook, Chun Song Youn, Youn-Jung Kim, Seung Mok Ryoo, Kyung Soo Lim, Gi-Byoung Nam, Su Jin Kim, and Won Young Kim. 2019. "Effect of Prophylactic Amiodarone Infusion on the Recurrence of Ventricular Arrhythmias in Out-of-Hospital Cardiac Arrest Survivors: A Propensity-Matched Analysis" Journal of Clinical Medicine 8, no. 2: 244. https://doi.org/10.3390/jcm8020244