Application of Diagnostic Interview for Internet Addiction (DIA) in Clinical Practice for Korean Adolescents

 and
and
Abstract
:1. Introduction
2. Materials and Methods
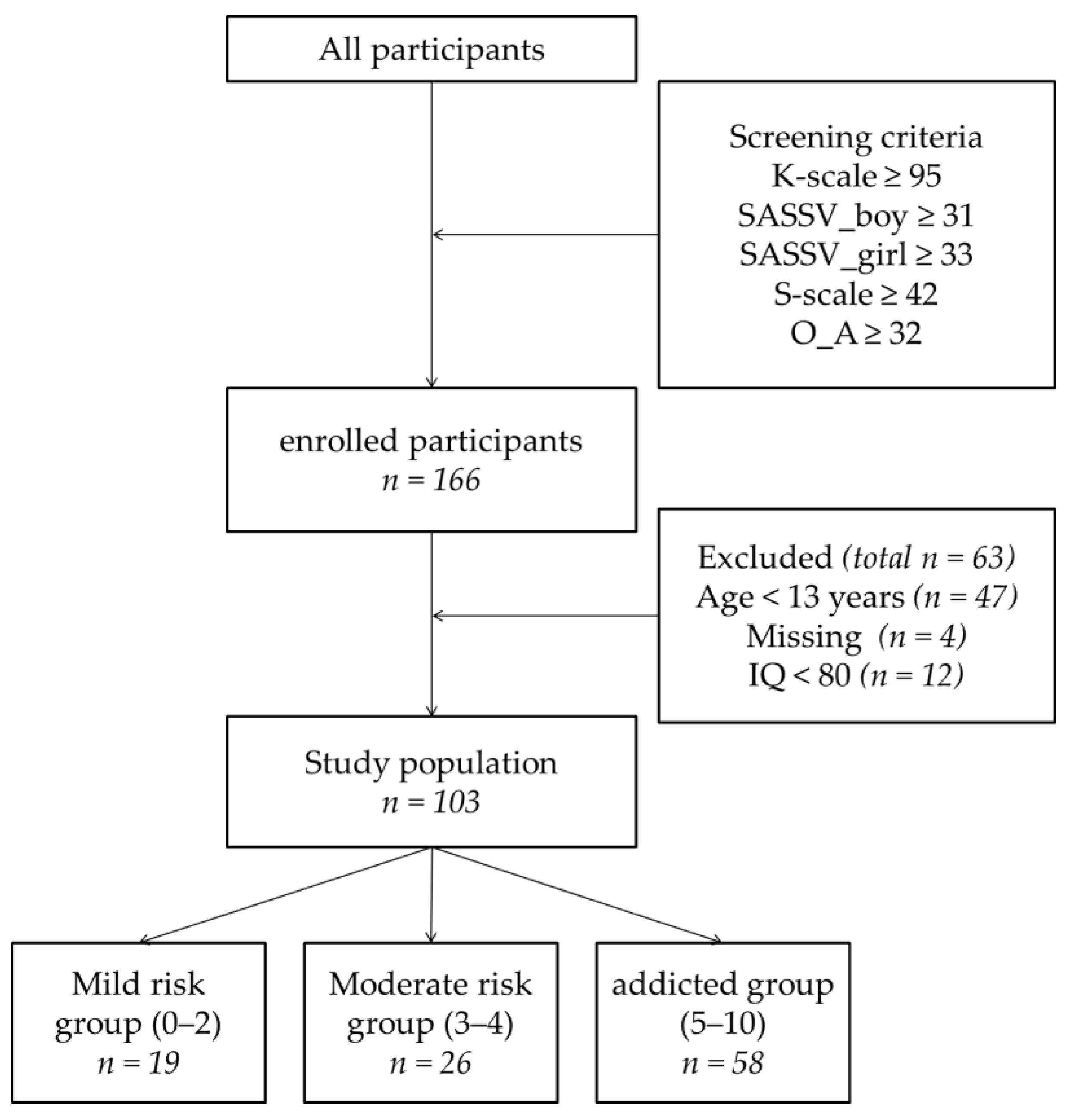
2.1. Participants and Procedure
2.2. Measurements
2.2.1. Diagnostic interview for Internet Addiction (DIA)
2.2.2. Internet and Smartphone Addiction Scales
2.2.3. Clinical Measurements
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
3.1. Demographic Characteristics
3.2. Psychometric Properties of the Diagnostic Interview for Internet Addiction
3.3. Comparison of Clinical Variables among the Diagnostic Interview for Internet Addiction Subgroups
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Korean National Information Society Agency. A Survey on Internet Addiction; Korean National Information Society Agency Report: Seoul, Korea, 2015. [Google Scholar]
- Yu, H.; Cho, J. Prevalence of internet gaming disorder among Korean adolescents and associations with non-psychotic psychological symptoms, and physical aggression. Am. J. Health Behav. 2016, 40, 705–716. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The ICD-11 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub.: Arlington, VA, USA, 2013. [Google Scholar]
- Griffiths, M.; King, D.; Demetrovics, Z. DSM-5 internet gaming disorder needs a unified approach to assessment. Neuropsychiatry 2014, 4, 1–4. [Google Scholar] [CrossRef]
- King, D.L.; Haagsma, M.C.; Delfabbro, P.H.; Gradisar, M.; Griffiths, M.D. Toward a consensus definition of pathological video-gaming: A systematic review of psychometric assessment tools. Clin. Psychol. Rev. 2013, 33, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Petry, N.M.; O’brien, C.P. Internet gaming disorder and the DSM-5. Addict 2013, 108, 1186–1187. [Google Scholar] [CrossRef] [PubMed]
- Petry, N.M.; Rehbein, F.; Gentile, D.A.; Lemmens, J.S.; Rumpf, H.J.; Mößle, T.; Bischof, G.; Tao, R.; Fung, D.S.; Borges, G. An international consensus for assessing internet gaming disorder using the new DSM-5 approach. Addiction 2014, 109, 1399–1406. [Google Scholar] [CrossRef] [PubMed]
- Pontes, H.M.; Kiraly, O.; Demetrovics, Z.; Griffiths, M.D. The conceptualisation and measurement of DSM-5 Internet Gaming Disorder: The development of the IGD-20 Test. PLoS ONE 2014, 9, e110137. [Google Scholar] [CrossRef] [PubMed]
- Pontes, H.M.; Griffiths, M.D. Measuring DSM-5 Internet gaming disorder: Development and validation of a short psychometric scale. Comput. Human Behav. 2015, 45, 137–143. [Google Scholar] [CrossRef]
- Jeong, H.; Yim, H.W.; Lee, S.-Y.; Lee, H.K.; Potenza, M.N.; Kwon, J.-H.; Koo, H.J.; Kweon, Y.-S.; Bhang, S.-Y.; Choi, J.-S. Discordance between self-report and clinical diagnosis of Internet gaming disorder in adolescents. Sci. Rep. 2018, 8, 10084. [Google Scholar] [CrossRef]
- Wölfling, K.; Beutel, M.; Müller, K. Construction of a standardized clinical interview to assess internet addiction: First findings regarding the usefulness of AICA-C. J. Addict. Res. Ther. 2012, 6, 1–7. [Google Scholar] [CrossRef]
- Koo, H.J.; Han, D.H.; Park, S.-Y.; Kwon, J.-H. The structured clinical interview for DSM-5 Internet gaming disorder: Development and validation for diagnosing IGD in adolescents. Psychiatry Investig. 2017, 14, 21–29. [Google Scholar] [CrossRef]
- Lee, S.-Y.; Lee, H.K.; Jeong, H.; Yim, H.W.; Bhang, S.-Y.; Jo, S.-J.; Baek, K.-Y.; Kim, E.; Kim, M.S.; Choi, J.-S. The hierarchical implications of Internet gaming disorder criteria: Which indicate more severe pathology? Psychiatry Investig. 2017, 14, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Young, K.S.; Rogers, R.C. The relationship between depression and Internet addiction. Cyberpsychol. Behav. 1998, 1, 25–28. [Google Scholar] [CrossRef]
- Mehroof, M.; Griffiths, M.D. Online gaming addiction: The role of sensation seeking, self-control, neuroticism, aggression, state anxiety, and trait anxiety. Cyberpsychol. Behav. Soc. Netw. 2010, 13, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Müller, K.; Janikian, M.; Dreier, M.; Wölfling, K.; Beutel, M.; Tzavara, C.; Richardson, C.; Tsitsika, A. Regular gaming behavior and internet gaming disorder in European adolescents: Results from a cross-national representative survey of prevalence, predictors, and psychopathological correlates. Eur. Child Adolesc. Psychiatry 2015, 24, 565–574. [Google Scholar] [CrossRef] [PubMed]
- King, D.L.; Delfabbro, P.H. The cognitive psychopathology of internet gaming disorder in adolescence. J. Abnorm. Child Psychol. 2016, 44, 1635–1645. [Google Scholar] [CrossRef]
- Whang, L.S.-M.; Lee, S.; Chang, G. Internet over-users’ psychological profiles: A behavior sampling analysis on internet addiction. Cyberpsychol. Behav. 2003, 6, 143–150. [Google Scholar] [CrossRef]
- Strittmatter, E.; Kaess, M.; Parzer, P.; Fischer, G.; Carli, V.; Hoven, C.W.; Wasserman, C.; Sarchiapone, M.; Durkee, T.; Apter, A. Pathological Internet use among adolescents: Comparing gamers and non-gamers. Psychiatry Res. 2015, 228, 128–135. [Google Scholar] [CrossRef]
- Wartberg, L.; Kriston, L.; Kramer, M.; Schwedler, A.; Lincoln, T.; Kammerl, R. Internet gaming disorder in early adolescence: Associations with parental and adolescent mental health. Eur. Psychiatry 2017, 43, 14–18. [Google Scholar] [CrossRef]
- Gentile, D.A.; Choo, H.; Liau, A.; Sim, T.; Li, D.; Fung, D.; Khoo, A. Pathological video game use among youths: A two-year longitudinal study. Pediatrics 2011, 127. [Google Scholar] [CrossRef]
- Lam, L.T.; Peng, Z.-W.; Mai, J.-C.; Jing, J. Factors associated with Internet addiction among adolescents. Cyberpsychol. Behav. 2009, 12, 551–555. [Google Scholar] [CrossRef]
- Du, X.; Qi, X.; Yang, Y.; Du, G.; Gao, P.; Zhang, Y.; Qin, W.; Li, X.; Zhang, Q. Altered structural correlates of impulsivity in adolescents with internet gaming disorder. Front. Hum. Neurosci. 2016, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- Ko, C.-H.; Yen, J.-Y.; Yen, C.-F.; Lin, H.-C.; Yang, M.-J. Factors predictive for incidence and remission of internet addiction in young adolescents: A prospective study. Cyberpsychol. Behav. 2007, 10, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Cao, F.; Su, L. Internet addiction among Chinese adolescents: Prevalence and psychological features. Child Care Health Dev. 2007, 33, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Dalbudak, E.; Evren, C.; Aldemir, S.; Coskun, K.S.; Ugurlu, H.; Yildirim, F.G. Relationship of internet addiction severity with depression, anxiety, and alexithymia, temperament and character in university students. Cyberpsychol. Behav. Soc. Netw. 2013, 16, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Van der Aa, N.; Overbeek, G.; Engels, R.C.; Scholte, R.H.; Meerkerk, G.-J.; Van den Eijnden, R.J. Daily and compulsive internet use and well-being in adolescence: A diathesis-stress model based on big five personality traits. J. Youth Adolesc. 2009, 38, 765. [Google Scholar] [CrossRef] [PubMed]
- Müller, K.W.; Koch, A.; Dickenhorst, U.; Beutel, M.E.; Duven, E.; Wölfling, K. Addressing the question of disorder-specific risk factors of internet addiction: A comparison of personality traits in patients with addictive behaviors and comorbid internet addiction. BioMed. Res. Int. 2013. [Google Scholar] [CrossRef] [PubMed]
- Korean National Information Society Agency. A Validation Study of K-Scale as a Diagnostic Tool; Korean National Information Society Agency Report: Seoul, Korea, 2013. [Google Scholar]
- Kwon, M.; Kim, D.-J.; Cho, H.; Yang, S. The smartphone addiction scale: Development and validation of a short version for adolescents. PLoS ONE 2013, 8, e83558. [Google Scholar] [CrossRef] [PubMed]
- Korean National Information Society Agency. Third Standardization of Korean Internet Addiction Proneness Scale; NIA IV-RER-11050; Korean National Information Society Agency Report: Seoul, Korea, 2011. [Google Scholar]
- Young, K.S. Internet addiction: The emergence of a new clinical disorder. Cyberpsychol. Behav. 1998, 1, 237–244. [Google Scholar] [CrossRef]
- Kim, E.; Lee, S.; Oh, S. The validation of Korean adolescent internet addiction scale (K-AIAS). Korean J. Clin. Psychol. 2003, 22, 125–139. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Beck Depression Inventory-II (BDI-II); Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Lee, E.-H.; Lee, S.-J.; Hwang, S.-T.; Hong, S.-H.; Kim, J.-H. Reliability and validity of the Beck Depression Inventory-II among Korean adolescents. Psychiatry Investig. 2017, 14, 30–36. [Google Scholar] [CrossRef]
- Spielberg, C.; Gorsuch, R.; Lushene, R.; Vagg, P.; Jacobs, G. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Rosenberg, M. Conceiving the Self; Basic Books: New York, NY, USA, 1979. [Google Scholar]
- Barratt, E.S.; White, R. Impulsiveness and anxiety related to medical students’ performance and attitudes. J. Med. Educ. 1969, 44, 604–607. [Google Scholar] [PubMed]
- Lee, H. Impulsivity Test Scale; Guidance Korea: Seoul, Korea, 1992. [Google Scholar]
- Seo, S.; Kwon, S. Validation study of the Korean version of the aggression questionnaire. Korean J. Clin. Psychol. 2002, 21, 487–501. [Google Scholar]
- Buss, A.H.; Perry, M. The aggression questionnaire. J. Pers. Soc. Psychol. 1992, 63, 452. [Google Scholar] [CrossRef] [PubMed]
- Rowlison, R.T.; Felner, R.D. Major life events, hassles, and adaptation in adolescence: Confounding in the conceptualization and measurement of life stress and adjustment revisited. J. Pers. Soc. Psychol. 1988, 55, 432. [Google Scholar] [CrossRef] [PubMed]
- Han, M.H.; Yoo, A.J. Development of daily hassles scale for children in Korea. J. Korean Home Econ. Assoc. 1995, 33, 49–64. [Google Scholar]
- Cho, H.; Kwon, M.; Choi, J.-H.; Lee, S.-K.; Choi, J.S.; Choi, S.-W.; Kim, D.-J. Development of the Internet addiction scale based on the Internet Gaming Disorder criteria suggested in DSM-5. Addict. Behav. 2014, 39, 1361–1366. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.R.; Hwang, S.S.-H.; Choi, J.-S.; Kim, D.-J.; Demetrovics, Z.; Király, O.; Nagygyörgy, K.; Griffiths, M.; Hyun, S.Y.; Youn, H.C. Characteristics and psychiatric symptoms of internet gaming disorder among adults using self-reported DSM-5 criteria. Psychiatry Investig. 2016, 13, 58–66. [Google Scholar] [CrossRef] [PubMed]
- González-Bueso, V.; Santamaría, J.; Fernández, D.; Merino, L.; Montero, E.; Ribas, J. Association between internet gaming disorder or pathological video-game use and comorbid psychopathology: A comprehensive review. Int. J. Environ. Res. Public Health 2018, 15, 668. [Google Scholar] [CrossRef]
- Laconi, S.; Pires, S.; Chabrol, H. Internet gaming disorder, motives, game genres and psychopathology. Comput. Human Behav. 2017, 75, 652–659. [Google Scholar] [CrossRef]
- Wang, H.R.; Cho, H.; Kim, D.-J. Prevalence and correlates of comorbid depression in a nonclinical online sample with DSM-5 internet gaming disorder. J. Affect. Disord. 2018, 226, 1–5. [Google Scholar] [CrossRef]
- Hyun, G.J.; Han, D.H.; Lee, Y.S.; Kang, K.D.; Yoo, S.K.; Chung, U.-S.; Renshaw, P.F. Risk factors associated with online game addiction: A hierarchical model. Comput. Human Behav. 2015, 48, 706–713. [Google Scholar] [CrossRef]
- Egger, O.; Rauterberg, M. Internet Behavior and Addiction; Swiss Federal Institute of Technology: Zurich, Swizerland, 1996. [Google Scholar]
- Akin, A.; Iskender, M. Internet addiction and depression, anxiety and stress. Int. J. Educ. Sci. 2011, 3, 138–148. [Google Scholar]
- Ko, C.-H.; Hsieh, T.-J.; Wang, P.-W.; Lin, W.-C.; Yen, C.-F.; Chen, C.-S.; Yen, J.-Y. Altered gray matter density and disrupted functional connectivity of the amygdala in adults with Internet gaming disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2015, 57, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Yen, J.-Y.; Liu, T.-L.; Wang, P.-W.; Chen, C.-S.; Yen, C.-F.; Ko, C.-H. Association between Internet gaming disorder and adult attention deficit and hyperactivity disorder and their correlates: Impulsivity and hostility. Addict. Behav. 2017, 64, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Ryu, H.; Lee, J.-Y.; Choi, A.; Park, S.; Kim, D.-J.; Choi, J.-S. The relationship between impulsivity and internet gaming disorder in young adults: Mediating effects of interpersonal relationships and depression. Int. J. Environ. Res. Public Health 2018, 15, 458. [Google Scholar] [CrossRef] [PubMed]
- Montag, C.; Flierl, M.; Markett, S.; Walter, N.; Jurkiewicz, M.; Reuter, M. Internet addiction and personality in first-person-shooter video gamers. J. Media Psychol. 2011, 23, 163. [Google Scholar] [CrossRef]
- Jiménez-Murcia, S.; Fernández-Aranda, F.; Granero, R.; Chóliz, M.; La Verde, M.; Aguglia, E.; Signorelli, M.S.; Sá, G.M.; Aymamí, N.; Gómez-Peña, M. Video game addiction in gambling disorder: Clinical, psychopathological, and personality correlates. BioMed. Res. Int. 2014. [Google Scholar] [CrossRef] [PubMed]
- Whiteside, S.P.; Lynam, D.R. The five factor model and impulsivity: Using a structural model of personality to understand impulsivity. Pers. Individ. Dif. 2001, 30, 669–689. [Google Scholar] [CrossRef]
- Khazaal, Y.; Chatton, A.; Rothen, S.; Achab, S.; Thorens, G.; Zullino, D.; Gmel, G. Psychometric properties of the 7-item game addiction scale among French and German speaking adults. BMC Psychiatry 2016, 16, 132. [Google Scholar] [CrossRef]
- Müller, K.; Dreier, M.; Beutel, M.; Wölfling, K. Is Sensation Seeking a correlate of excessive behaviors and behavioral addictions? A detailed examination of patients with gambling disorder and internet addiction. Psychiatry Res. 2016, 242, 319–325. [Google Scholar] [CrossRef]
- Billieux, J.; Thorens, G.; Khazaal, Y.; Zullino, D.; Achab, S.; Van der Linden, M. Problematic involvement in online games: A cluster analytic approach. Comput. Human Behav. 2015, 43, 242–250. [Google Scholar] [CrossRef]
- Stavropoulos, V.; Kuss, D.J.; Griffiths, M.D.; Wilson, P.; Motti-Stefanidi, F. MMORPG gaming and hostility predict Internet addiction symptoms in adolescents: An empirical multilevel longitudinal study. Addict. Behav. 2017, 64, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.-S.; Ko, Y.-H.; Song, H.-S.; Kwon, K.-H.; Lee, H.-S.; Nam, M.; Jung, I.-K. Characteristics of Internet use in relation to game genre in Korean adolescents. Cyberpsychol. Behav. 2006, 10, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Fernandez, O.; Honrubia-Serrano, M.L.; Baguley, T.; Griffiths, M.D. Pathological video game playing in Spanish and British adolescents: Towards the exploration of Internet Gaming Disorder symptomatology. Comput. Human Behav. 2014, 41, 304–312. [Google Scholar] [CrossRef]


{kind=link}
| Item | Standardized Representative Questions |
|---|---|
| 1. cognitive salience | “Even if you do not have Internet/Games/SNS, do you spend a lot of time thinking about Internet/Games/SNS or planning what to do next?” |
| 2. withdrawal | “Do you experience restlessness, irritability, depression, anxiety, sadness etc. when you reduce, stop, or not allowed Internet/Games/SNS?” |
| 3. tolerance | "Do you want to spend more Internet/Gaming/SNS time, find more interesting things, or use better equipment such as cell phones, computers to make you feel as fun as before?” |
| 4. difficulty in regulating use | “Do you feel you should reduce the Internet/Games/SNS, but you can’t reduce the time you spend doing Internet/Games/SNS?” |
| 5. loss of interest in other activities | “Because of the Internet/Games/SNS, would you be less interested in participating in other leisure activities such as hobbies or meet friends?” |
| 6. persistent use despite negative feelings | “Despite negative consequences, such as lack of sleep time, late school or work, spend too much money, debate with other people, or neglect important things, do you continue the Internet/Games/SNS?” |
| 7. deception regarding Internet/gaming/SNS use | “Do you lie or hide how much time you spend on the Internet/Games/SNS for your family or friends?” |
| 8. use of Internet/gaming/SNS to avoid negative feelings | “Do you use Internet games to avoid/relieve negative feelings?" “Do you use the game to forget unpleasant moods (e.g., helplessness, depression, guilty, anxiety, etc.)?” |
| 9. interference with role performance | “Have you ever been troubled or fallen out by the use of Internet /Games/SNS in your important interpersonal, career, and academic settings?” |
| 10. craving | “Do you have a strong desire to do activities such as internet/ Games/SNS?” “If you want to play internet/Games/SNS, is it hard to tolerate?” |
| DIA | K | SAS-SV | S | YIAT | O_A | |
|---|---|---|---|---|---|---|
| DIA | 1 | |||||
| K | 0.426 ** | 1 | ||||
| SAS-SV | 0.205 * | 0.638 ** | 1 | |||
| S | 0.234 * | 0.733 ** | 0.885 ** | 1 | ||
| YIAT | 0.390 ** | 0.845 ** | 0.706 ** | 0.744 ** | 1 | |
| O_A | 0.343 ** | 0.084 | −0.223 * | −0.146 | 0.047 | 1 |
| DIA | BDI-II | STAI_X1 | RSES | BIS-II | AQ | DHQ | |
|---|---|---|---|---|---|---|---|
| DIA | 1 | ||||||
| BDI-II | 0.285 ** | 1 | |||||
| STAI_X1 | 0.294 ** | 0.758 ** | 1 | ||||
| RSES | −0.312 ** | −0.708 ** | −0.739 ** | 1 | |||
| BIS-II | 0.278 ** | 0.390 ** | 0.422 ** | −0.540 ** | 1 | ||
| AQ | 0.256 * | 0.429 ** | 0.387 ** | −0.369 ** | 0.380 ** | 1 | |
| DHQ | 0.283 ** | 0.538 ** | 0.595 ** | −0.465 ** | 0.287 ** | 0.506 ** | 1 |
| Mild Risk M (SD) | Moderate Risk M (SD) | Addicted M (SD) | Total M (SD) | F (Post Hoc) | |
|---|---|---|---|---|---|
| K | 58.15 (13.53) | 75.57 (18.73) | 78.74 (19.98) | 74.14 (20.03) | 8.807 ** (1<2.3) |
| S | 28.52 (7.45) | 35.11 (7.86) | 34.46 (9.50) | 33.53 (9.01) | 3.848 * (1<2.3) |
| YIAT | 32.76 (10.50) | 49.69 (14.13) | 50.71 (16.77) | 47.14 (16.52) | 9.383 ** (1<2.3) |
| O_A | 37.57 (8.00) | 40.36 (7.40) | 43.22 (6.31) | 41.47 (7.20) | 5.185 * (1<3) |
| BDI-II | 6.47 (5.79) | 15.69 (11.59) | 16.18 (12.90) | 14.21 (12.04) | 5.267 * (1<2.3) |
| STAI_X1 | 36.47 (9.60) | 44.32 (11.71) | 45.83 (12.19) | 43.63 (12.05) | 4.613 * (1<3) |
| RSES | 30.52 (4.38) | 26.88 (4.98) | 26.31 (6.33) | 27.27 (5.85) | 3.937 * (1>3) |
| BIS | 48.31 (6.61) | 57.52 (10.32) | 56.81 (9.49) | 55.34 (9.78) | 6.864 * (1<2.3) |
| AQ | 50.36 (12.51) | 62.56 (12.62) | 62.29 (17.83) | 60.05 (16.28) | 4.468 * (1<2.3) |
| DHQ | 55.84 (15.55) | 70.76 (15.70) | 70.77(17.43) | 67.87 (17.52) | 6.145 * (1<2.3) |
| JTCI_P | 54.55 (6.42) | 47.68 (7.58) | 45.22 (8.71) | 47.86 (8.66) | 8.743 ** (1>2.3) |
| JTCI_SD | 55.88 (10.80) | 48.68 (10.39) | 46.15 (10.81) | 48.89 (11.21) | 5.292 * (1>3) |
| JTCI_C | 56.88 (11.70) | 51.20 (8.84) | 48.81 (10.10) | 51.17 (10.47) | 4.065 * (1>3) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryu, H.; Lee, J.Y.; Choi, A.R.; Chung, S.J.; Park, M.; Bhang, S.-Y.; Kwon, J.-G.; Kweon, Y.-S.; Choi, J.-S. Application of Diagnostic Interview for Internet Addiction (DIA) in Clinical Practice for Korean Adolescents. J. Clin. Med. 2019, 8, 202. https://doi.org/10.3390/jcm8020202
Ryu H, Lee JY, Choi AR, Chung SJ, Park M, Bhang S-Y, Kwon J-G, Kweon Y-S, Choi J-S. Application of Diagnostic Interview for Internet Addiction (DIA) in Clinical Practice for Korean Adolescents. Journal of Clinical Medicine. 2019; 8(2):202. https://doi.org/10.3390/jcm8020202
Chicago/Turabian StyleRyu, Hyera, Ji Yoon Lee, A Ruem Choi, Sun Ju Chung, Minkyung Park, Soo-Young Bhang, Jun-Gun Kwon, Yong-Sil Kweon, and Jung-Seok Choi. 2019. "Application of Diagnostic Interview for Internet Addiction (DIA) in Clinical Practice for Korean Adolescents" Journal of Clinical Medicine 8, no. 2: 202. https://doi.org/10.3390/jcm8020202