The Correlation between Severity of Neurological Impairment and Left Ventricular Function in Patients after Acute Ischemic Stroke

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Definition of Stroke Severity
2.4. Patients’ Enrollment and Allocation
2.5. Laboratory Test for Circulatory Complete Blood Count/Differential Count
2.6. Primary and Secondary Endpoints
2.7. Study Protocol for Evaluation and Clinical Follow-Up
2.8. Medications for AIS
2.9. Echocardiographic Measurement for LV Systolic Function and Grade of Valvular Regurgitation
2.10. Statistical Analysis
3. Results
3.1. Patients’ Characteristics (Table 1)

{kind=link}
| Variables | Total (n = 99) | Group 1 (n = 50) | Group 2 (n = 49) | p-Value |
|---|---|---|---|---|
| Clinical | ||||
| Age/year | 64.16 ± 11.85 | 60.74 ± 11.83 | 68.06 ± 10.51 | 0.002 |
| Male sex/No. (%) | 59 (59.6%) | 30 (60.0%) | 29 (59.2%) | 0.934 |
| Smoker/No. (%) | 32 (32.3%) | 21 (42.0%) | 11 (22.4%) | 0.038 |
| Systolic BP/mmHg | 161.92 ± 29.16 | 165.10 ± 30.76 | 158.67 ± 27.37 | 0.275 |
| Diastolic BP/mmHg | 88.99 ± 17.26 | 91.70 ± 16.19 | 86.22 ± 18.03 | 0.115 |
| Hypertension/No. (%) | 79 (79.8%) | 38 (76.0%) | 41 (83.7%) | 0.324 |
| Diabetes/No. (%) | 34 (34.3%) | 19 (38.0%) | 15 (30.6%) | 0.439 |
| Dyslipidemia/No. (%) | 45 (45.5%) | 29 (58.0%) | 16 (32.7%) | 0.011 |
| Old MI/No. (%) | 3 (3.0%) | 1 (2.0%) | 2 (4.1%) | 0.492 |
| Old stroke/No. (%) | 19 (19.2%) | 8 (16.0%) | 11 (22.4%) | 0.415 |
| Atrial fibrillation/No. (%) | 11 (11.1%) | 1 (2.0%) | 10 (20.4%) | 0.004 |
| ACEI or ARB/No. (%) | 47 (47.5%) | 24 (48.0%) | 23 (46.9%) | 0.916 |
| Statin/No. (%) | 53 (53.5%) | 33 (66.0%) | 20 (40.8%) | 0.012 |
| Laboratory data | ||||
| Leukocyte count/1000/μL | 8.38 ± 2.71 | 8.26 ± 2.78 | 8.51 ± 2.67 | 0.654 |
| Neutrophil/1000/μL | 5.39 (3.70–7.16) | 4.97 (3.45–7.04) | 5.80 (4.10–7.25) | 0.136 |
| Lymphocyte/1000/μL | 1.93 (1.33–2.57) | 2.12 (1.58–2.91) | 1.45 (1.12–2.27) | 0.001 |
| Hemoglobin/g/dL | 14.20 ± 2.04 | 14.40 ± 1.86 | 14.00 ± 2.21 | 0.329 |
| Platelet count/1000/μL | 212.14 ± 68.62 | 218.40 ± 79.74 | 205.76 ± 55.15 | 0.362 |
| NLR | 2.85 (1.67–4.66) | 2.20 (1.45–3.72) | 3.73 (2.27–5.72) | 0.001 |
| PLR | 113.0 (81.3–155.4) | 99.4 (77.4–125.6) | 133.0 (93.8–178.7) | 0.005 |
| Serum creatinine/mg/dL | 0.93 (0.75–1.22) | 0.93 (0.72–1.18) | 0.93 (0.78–1.47) | 0.448 |
| Total Cholesterol/mg/dL | 180.0 (153.3–210.5) | 179.5 (160.8–210.5) | 181.0 (147.3–210.3) | 0.779 |
| HDL/mg/dL | 43.71 ± 13.00 | 44.04 ± 15.32 | 43.38 ± 10.20 | 0.802 |
| LDL/mg/dL | 104.62 ± 46.64 | 101.42 ± 45.42 | 107.96 ± 48.13 | 0.491 |
| Triglyceride/mg/dL | 113.0 (78.5–166.5) | 135.5 (91.8–188.3) | 98.5 (65.8–139.8) | 0.004 |
| Stroke severity | ||||
| Average NIHSS | 8.59 ± 8.45 | 2.74 ± 1.40 | 14.55 ± 8.47 | <0.001 |
| Modified Rankin Scale | 2.87 ± 1.50 | 1.92 ± 1.05 | 3.84 ± 1.25 | <0.001 |
3.2. Echocardiographic Results and Clinical Outcomes (Table 2)
| Variables | Total (n = 99) | Group 1 (n = 50) | Group 2 (n = 49) | p-Value |
|---|---|---|---|---|
| Echocardiographic data | ||||
| IVS thickness/mm | 11.14 ± 4.55 | 11.47 ± 5.86 | 10.08 ± 2.75 | 0.815 |
| LVPW thickness/mm | 8.82 ± 1.76 | 8.82 ± 1.79 | 8.83 ± 1.75 | 0.758 |
| LVEDD/mm | 48.89 ± 8.08 | 47.30 ± 7.03 | 50.52 ± 8.82 | 0.054 |
| LVESD/mm | 31.71 ± 8.06 | 29.94 ± 7.27 | 33.71 ± 8.42 | 0.009 |
| LVEF/% | 64.96 ± 10.93 | 68.57 ± 7.84 | 61.27 ± 12.41 | 0.001 |
| Mild to severe MR/No. (%) | 26 (28.3%) | 8 (17.4%) | 18 (39.1%) | 0.021 |
| Mild to severe TR/No. (%) | 23 (25.0%) | 9 (19.6%) | 14 (30.4%) | 0.229 |
| Mitral stenosis/No. (%) | 0 (0%) | 0 (0%) | 0 (0%) | - |
| Aortic stenosis/No. (%) | 0 (0%) | 0 (0%) | 0 (0%) | - |
| Clinical outcomes | ||||
| In-hospital death/No. (%) | 2 (2.0%) | 0 (0.0%) | 2 (4.1%) | 0.242 |
| Pulmonary edema/No. (%) | 1 (1.0%) | 0 (0.0%) | 1 (2.0%) | 0.495 |
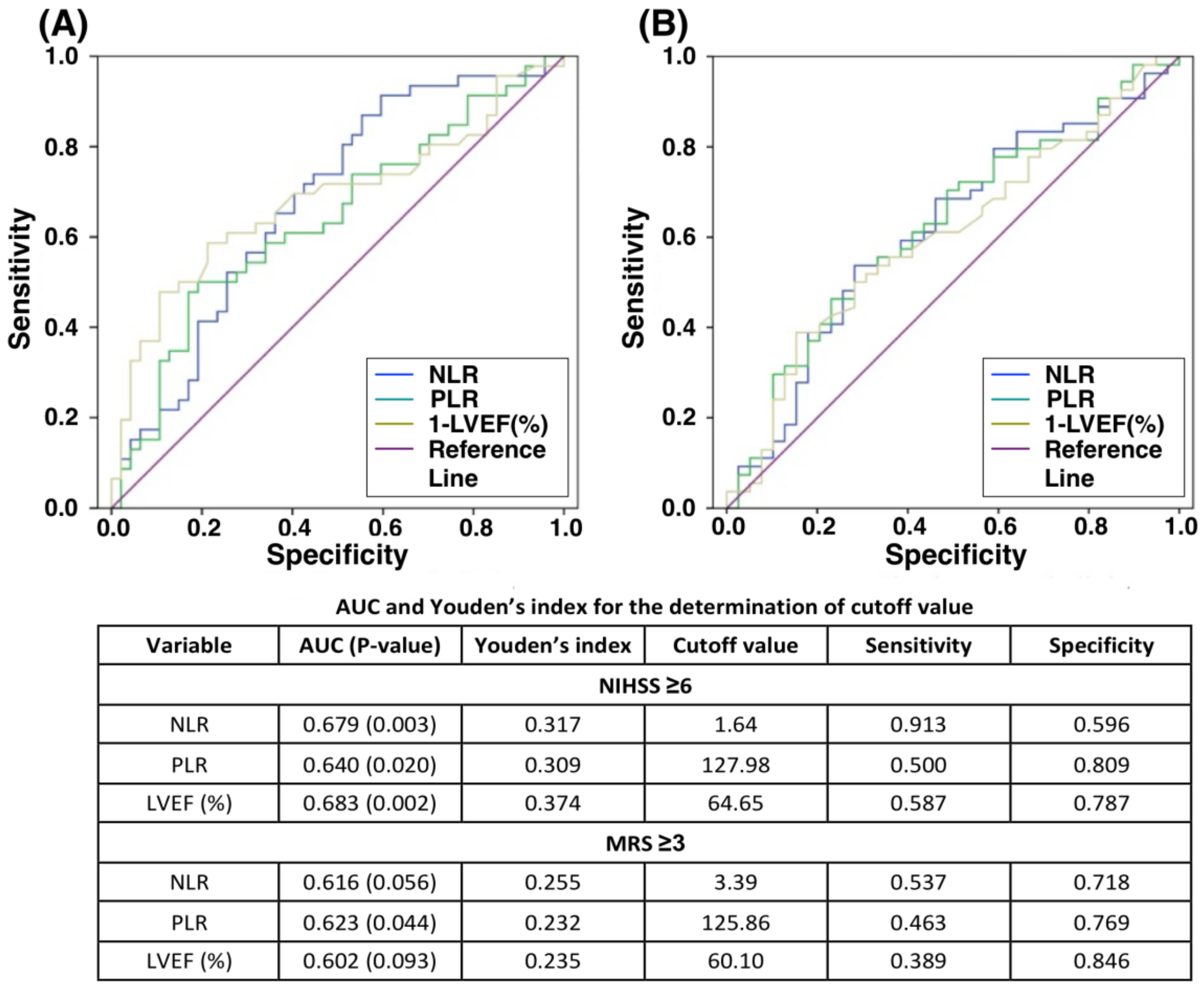
3.3. The Relationship of Stroke Severity (NIHSS or MRS) to Inflammatory Markers (NLR or PLR) and LV Systolic Function, followed by Identifying Cutoff Values of Moderate to Severe Stroke (Table 3 and Figure 1)
| Variables | Correlation Coefficient (R) | p-Value |
|---|---|---|
| NIHSS vs. MRS | 0.775 | <0.001 |
| NIHSS vs. NLR | 0.353 | <0.001 |
| NIHSS vs. PLR | 0.269 | 0.007 |
| NIHSS vs. LVEF | −0.369 | <0.001 |
| MRS vs. NLR | 0.284 | 0.004 |
| MRS vs. PLR | 0.237 | 0.018 |
| MRS vs. LVEF | −0.250 | 0.016 |

3.4. Further Identification of Independent Risk Factors for Stroke Severity NIHSS ≥6 (Table 4)
| Stroke Severity | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| Variables | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
| Age per year | 1.061 | 1.020–1.102 | 0.003 | |||
| Age >65 years | 4.004 | 1.735–9.237 | 0.001 | 4.400 | 1.560–12.415 | 0.005 |
| Male sex | 0.967 | 0.433–2.158 | 0.934 | |||
| Smoker | 0.400 | 0.167–0.959 | 0.040 | |||
| Systolic BP | 0.992 | 0.919–1.006 | 0.273 | |||
| Diastolic BP | 0.981 | 0.958–1.005 | 0.118 | |||
| Hypertension | 1.618 | 0.597–4.389 | 0.344 | |||
| Diabetes | 0.720 | 0.313–1.657 | 0.440 | |||
| Dyslipidemia | 0.351 | 0.155–0.797 | 0.012 | 0.280 | 0.097–0.813 | 0.019 |
| Old MI | 2.085 | 0.183–23.769 | 0.554 | |||
| Old stroke | 1.520 | 0.553–4.176 | 0.417 | |||
| Atrial fibrillation | 12.564 | 1.541–102.417 | 0.018 | |||
| ACEI or ARB | 0.958 | 0.435–2.110 | 0.916 | |||
| Statin | 0.355 | 0.157–0.804 | 0.013 | |||
| Leukocyte count | 1.034 | 0.893–1.198 | 0.651 | |||
| Hemoglobin | 0.906 | 0.743–1.104 | 0.328 | |||
| Platelet count | 0.997 | 0.991–1.003 | 0.360 | |||
| NLR | 1.202 | 1.024–1.411 | 0.024 | |||
| NLR ≥1.64 | 7.500 | 2.331–24.113 | 0.001 | 6.953 | 1.710–28.264 | 0.007 |
| PLR | 1.003 | 0.999–1.008 | 0.118 | |||
| PLR ≥128 | 4.522 | 1.854–11.029 | 0.001 | |||
| NLR ≥1.64 and PLR >128 | 4.552 | 1.854–11.029 | 0.001 | |||
| Serum creatinine | 1.518 | 0.872–2.642 | 0.140 | |||
| Total Cholesterol | 0.998 | 0.990–1.006 | 0.634 | |||
| HDL | 0.996 | 0.966–1.027 | 0.799 | |||
| LDL | 1.003 | 0.994–1.012 | 0.487 | |||
| Triglyceride | 0.989 | 0.982–0.996 | 0.003 | |||
| IVS thickness | 0.966 | 0.878–1.064 | 0.485 | |||
| LVEF per % | 0.930 | 0.886–0.975 | 0.003 | |||
| LVEF ≥65% | 0.190 | 0.076–0.474 | <0.001 | 0.216 | 0.074–0.637 | 0.005 |
| Mild to severe MR | 3.054 | 1.163–8.018 | 0.023 | |||
3.5. Subgroup Analysis According to AIS Patients with or without AF (Ref. to Table S2)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
| AIS | acute ischemic stroke |
| DAMP | damage-associated molecular patterns |
| NLR | neutrophil-to-lymphocyte ratio |
| PLR | platelet-to-lymphocyte ratio |
| BNP | brain natriuretic peptide |
| NT-proBNP | N-terminal pro-BNP |
| LV | left ventricular |
| LVEF | left ventricular ejection fraction |
| NE | neurological examination |
| NIHSS | National Institute of Health Stroke Scale |
| MRS | modified Rankin scale |
| NICU | neurology intensive care unit |
| AF | atrial fibrillation |
| MR | mitral regurgitation |
| TR | tricuspid regurgitation |
| AUC | area under the curve |
| ROC curve | receiver operating characteristic curve |
References
- Donnan, G.A.; Fisher, M.; Macleod, M.; Davis, S.M. Stroke. Lancet 2008, 371, 1612–1623. [Google Scholar] [CrossRef]
- Adams, H.P., Jr.; del Zoppo, G.; Alberts, M.J.; Bhatt, D.L.; Brass, L.; Furlan, A.; Grubb, R.L.; Higashida, R.T.; Jauch, E.C.; Kidwell, C.; et al. Guidelines for the early management of adults with ischemic stroke: A guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke 2007, 38, 1655–1711. [Google Scholar] [PubMed]
- D’Agostino, R.B.; Wolf, P.A.; Belanger, A.J.; Kannel, W.B. Stroke risk profile: Adjustment for antihypertensive medication. The Framingham Study. Stroke 1994, 25, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Ovbiagele, B.; Nguyen-Huynh, M.N. Stroke epidemiology: Advancing our understanding of disease mechanism and therapy. Neurotherapeutics 2011, 8, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.I.; Suarez, J.I.; Yahia, A.M.; Mohammad, Y.; Uzun, G.; Suri, M.F.; Zaidat, O.O.; Ayata, C.; Ali, Z.; Wityk, R.J. Timing of neurologic deterioration in massive middle cerebral artery infarction: A multicenter review. Crit. Care Med. 2003, 31, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Bill, O.; Zufferey, P.; Faouzi, M.; Michel, P. Severe stroke: Patient profile and predictors of favorable outcome. J. Thromb. Haemost. 2013, 11, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Hacke, W.; Schwab, S.; Horn, M.; Spranger, M.; De Georgia, M.; von Kummer, R. ‘Malignant’ middle cerebral artery territory infarction: Clinical course and prognostic signs. Arch. Neurol. 1996, 53, 309–315. [Google Scholar] [CrossRef]
- Heinsius, T.; Bogousslavsky, J.; Van Melle, G. Large infarcts in the middle cerebral artery territory. Etiology and outcome patterns. Neurology 1998, 50, 341–350. [Google Scholar] [CrossRef]
- Liesz, A.; Dalpke, A.; Mracsko, E.; Antoine, D.J.; Roth, S.; Zhou, W.; Yang, H.; Na, S.Y.; Akhisaroglu, M.; Fleming, T.; et al. DAMP signaling is a key pathway inducing immune modulation after brain injury. J. Neurosci. 2015, 35, 583–598. [Google Scholar] [CrossRef]
- Seong, S.Y.; Matzinger, P. Hydrophobicity: An ancient damage-associated molecular pattern that initiates innate immune responses. Nat. Rev. Immunol. 2004, 4, 469–478. [Google Scholar] [CrossRef]
- Janeway, C. Immunogenicity signals 1,2,3 … and 0. Immunol. Today 1989, 10, 283–286. [Google Scholar] [CrossRef]
- Sung, P.H.; Lee, F.Y.; Lin, L.C.; Chen, K.H.; Lin, H.S.; Shao, P.L.; Li, Y.C.; Chen, Y.L.; Lin, K.C.; Yuen, C.M.; et al. Melatonin attenuated brain death tissue extract-induced cardiac damage by suppressing DAMP signaling. Oncotarget 2018, 9, 3531–3548. [Google Scholar] [CrossRef] [PubMed]
- Bulcao, C.F.; D’Souza, K.M.; Malhotra, R.; Staron, M.; Duffy, J.Y.; Pandalai, P.K.; Jeevanandam, V.; Akhter, S.A. Activation of JAK-STAT and nitric oxide signaling as a mechanism for donor heart dysfunction. J. Heart Lung Transplant. 2010, 29, 346–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Zhan, X.; Chen, M.; Lei, H.; Wang, Y.; Wei, D.; Jiang, X. The prognostic value of combined NT-pro-BNP levels and NIHSS scores in patients with acute ischemic stroke. Intern. Med. 2012, 51, 2887–2892. [Google Scholar] [CrossRef]
- Bai, J.; Sun, H.; Xie, L.; Zhu, Y.; Feng, Y. Detection of cardioembolic stroke with B-type natriuretic peptide or N-terminal pro-BNP: A comparative diagnostic meta-analysis. Int. J. Neurosci. 2018, 128, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Chen, Y.; Lei, D.; Zhang, Y.; Weng, X.; Zhou, Y.; Zhang, L. Plasma brain natriuretic peptide is a biomarker for screening ischemic cerebral small vessel disease in patients with hypertension. Medicine 2018, 97, e12088. [Google Scholar] [CrossRef] [PubMed]
- Yip, H.K.; Sun, C.K.; Chang, L.T.; Chen, M.C.; Liou, C.W. Time course and prognostic value of plasma levels of N-terminal pro-brain natriuretic peptide in patients after ischemic stroke. Circ. J. 2006, 70, 447–452. [Google Scholar] [CrossRef]
- Lyden, P.D.; Lu, M.; Levine, S.R.; Brott, T.G.; Broderick, J. A modified National Institutes of Health Stroke Scale for use in stroke clinical trials: Preliminary reliability and validity. Stroke 2001, 32, 1310–1317. [Google Scholar] [CrossRef]
- Rost, N.S.; Bottle, A.; Lee, J.M.; Randall, M.; Middleton, S.; Shaw, L.; Thijs, V.; Rinkel, G.J.; Hemmen, T.M. Stroke Severity Is a Crucial Predictor of Outcome: An International Prospective Validation Study. J. Am. Heart Assoc. 2016, 5, e002433. [Google Scholar] [CrossRef] [Green Version]
- Jauch, E.C.; Saver, J.L.; Adams, H.P., Jr.; Bruno, A.; Connors, J.J.; Demaerschalk, B.M.; Khatri, P.; McMullan, P.W., Jr.; Qureshi, A.I.; Rosenfield, K.; et al. Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 870–947. [Google Scholar] [CrossRef]
- Hankey, G.J.; Norrving, B.; Hacke, W.; Steiner, T. Management of acute stroke in patients taking novel oral anticoagulants. Int. J. Stroke 2014, 9, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Galderisi, M.; Henein, M.Y.; D’Hooge, J.; Sicari, R.; Badano, L.P.; Zamorano, J.L.; Roelandt, J.R. Recommendations of the European Association of Echocardiography: How to use echo-Doppler in clinical trials: Different modalities for different purposes. Eur. J. Echocardiogr. 2011, 12, 339–353. [Google Scholar] [CrossRef] [PubMed]
- Hays, A.G.; Sacco, R.L.; Rundek, T.; Sciacca, R.R.; Jin, Z.; Liu, R.; Homma, S.; Di Tullio, M.R. Left ventricular systolic dysfunction and the risk of ischemic stroke in a multiethnic population. Stroke 2006, 37, 1715–1719. [Google Scholar] [CrossRef] [PubMed]
- Cuadrado-Godia, E.; Ois, A.; Roquer, J. Heart failure in acute ischemic stroke. Curr. Cardiol. Rev. 2010, 6, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Haeusler, K.G.; Laufs, U.; Endres, M. Chronic heart failure and ischemic stroke. Stroke 2011, 42, 2977–2982. [Google Scholar] [CrossRef] [PubMed]
- Ois, A.; Gomis, M.; Cuadrado-Godia, E.; Jimenez-Conde, J.; Rodriguez-Campello, A.; Bruguera, J.; Molina, L.; Comin, J.; Roquer, J. Heart failure in acute ischemic stroke. J. Neurol. 2008, 255, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Park, H.K.; Kim, B.J.; Yoon, C.H.; Yang, M.H.; Han, M.K.; Bae, H.J. Left Ventricular Diastolic Dysfunction in Ischemic Stroke: Functional and Vascular Outcomes. J. Stroke 2016, 18, 195–202. [Google Scholar] [CrossRef] [Green Version]
- Fang, Y.N.; Tong, M.S.; Sung, P.H.; Chen, Y.L.; Chen, C.H.; Tsai, N.W.; Huang, C.J.; Chang, Y.T.; Chen, S.F.; Chang, W.N.; et al. Higher neutrophil counts and neutrophil-to-lymphocyte ratio predict prognostic outcomes in patients after non-atrial fibrillation-caused ischemic stroke. Biomed. J. 2017, 40, 154–162. [Google Scholar] [CrossRef]
- Yip, H.K.; Lee, M.S.; Sun, C.K.; Chen, K.H.; Chai, H.T.; Sung, P.H.; Lin, K.C.; Ko, S.F.; Yuen, C.M.; Liu, C.F.; et al. Therapeutic effects of adipose-derived mesenchymal stem cells against brain death-induced remote organ damage and post-heart transplant acute rejection. Oncotarget 2017, 8, 108692–108711. [Google Scholar] [CrossRef]
- Florea, V.G.; Cohn, J.N. The autonomic nervous system and heart failure. Circ. Res. 2014, 114, 1815–1826. [Google Scholar] [CrossRef]
- Korpelainen, J.T.; Sotaniemi, K.A.; Myllylä, V.V. Autonomic nervous system disorders in stroke. Clin. Auton. Res. 1999, 9, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Al-Qudah, Z.A.; Yacoub, H.A.; Souayah, N. Disorders of the Autonomic Nervous System after Hemispheric Cerebrovascular Disorders: An Update. J. Vasc. Interv. Neurol. 2015, 8, 43–52. [Google Scholar] [PubMed]
- Hilz, M.J.; Moeller, S.; Akhundova, A.; Marthol, H.; Pauli, E.; De Fina, P.; Schwab, S. High NIHSS values predict impairment of cardiovascular autonomic control. Stroke 2011, 42, 1528–1533. [Google Scholar] [CrossRef] [PubMed]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sung, P.-H.; Chen, K.-H.; Lin, H.-S.; Chu, C.-H.; Chiang, J.Y.; Yip, H.-K. The Correlation between Severity of Neurological Impairment and Left Ventricular Function in Patients after Acute Ischemic Stroke. J. Clin. Med. 2019, 8, 190. https://doi.org/10.3390/jcm8020190
Sung P-H, Chen K-H, Lin H-S, Chu C-H, Chiang JY, Yip H-K. The Correlation between Severity of Neurological Impairment and Left Ventricular Function in Patients after Acute Ischemic Stroke. Journal of Clinical Medicine. 2019; 8(2):190. https://doi.org/10.3390/jcm8020190
Chicago/Turabian StyleSung, Pei-Hsun, Kuan-Hung Chen, Hung-Sheng Lin, Chi-Hsiang Chu, John Y Chiang, and Hon-Kan Yip. 2019. "The Correlation between Severity of Neurological Impairment and Left Ventricular Function in Patients after Acute Ischemic Stroke" Journal of Clinical Medicine 8, no. 2: 190. https://doi.org/10.3390/jcm8020190