Breast Cancer Systemic Treatments and Upper Limb Lymphedema: A Risk-Assessment Platform Encompassing Tumor-Specific Pathological Features Reveals the Potential Role of Trastuzumab

 ,
, 
 , ,
, , 
Abstract
1. Background
2. Materials and Methods
2.1. Study Cohort
2.2. BCRL Assessment
2.3. Histological Review
2.4. Statistical Analyses
3. Results
3.1. Tumor-Specific Biological Features Associated with BCRL
3.2. The Type of Axillary Surgical Dissection But Not the Type of Breast Surgery Impacts on BCRL
3.3. Extra-Axillary Radiotherapy Does Not Increase the Risk of BCRL
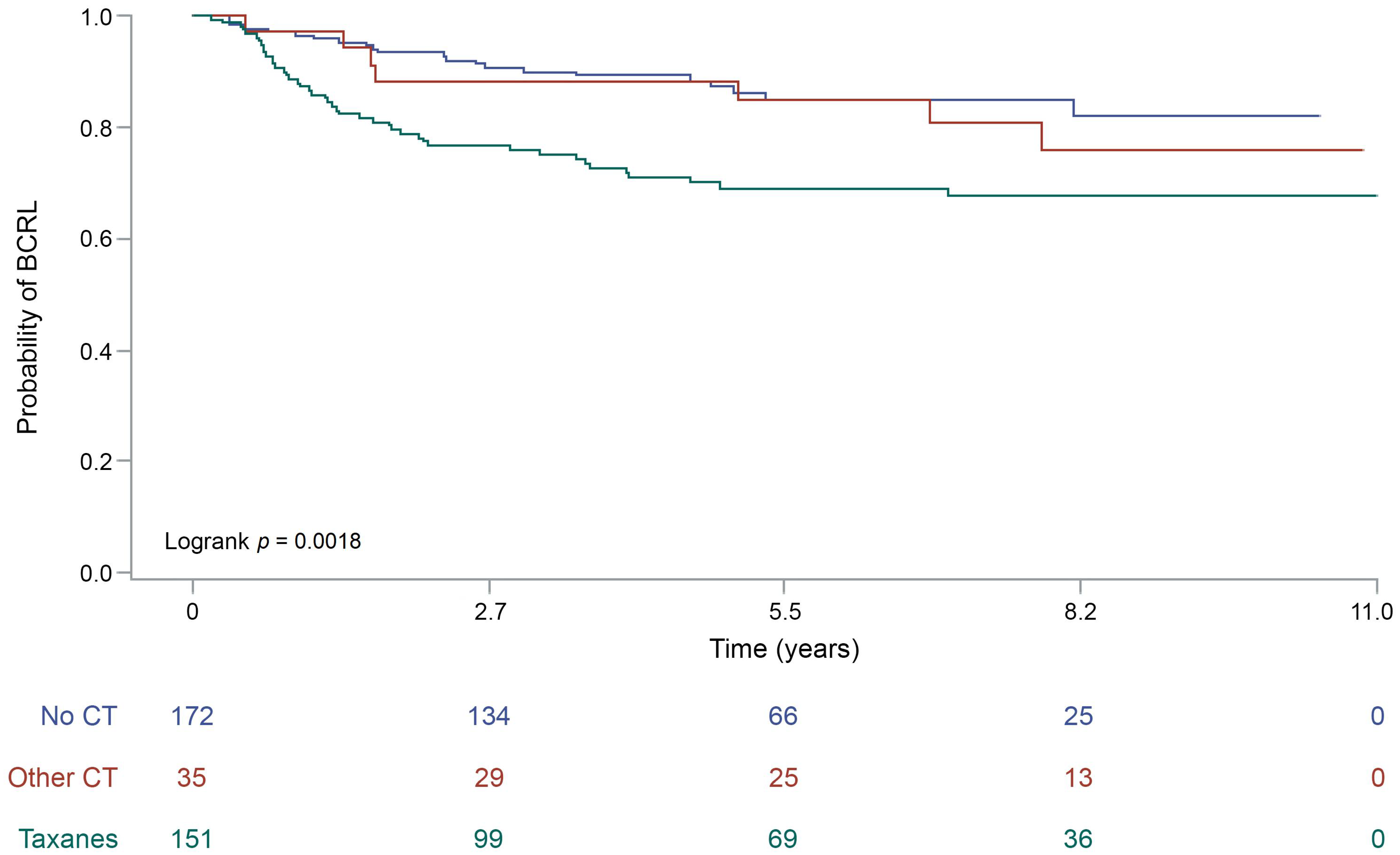
3.4. Taxanes-Based Chemotherapy Is Associated with BCRL Occurrence
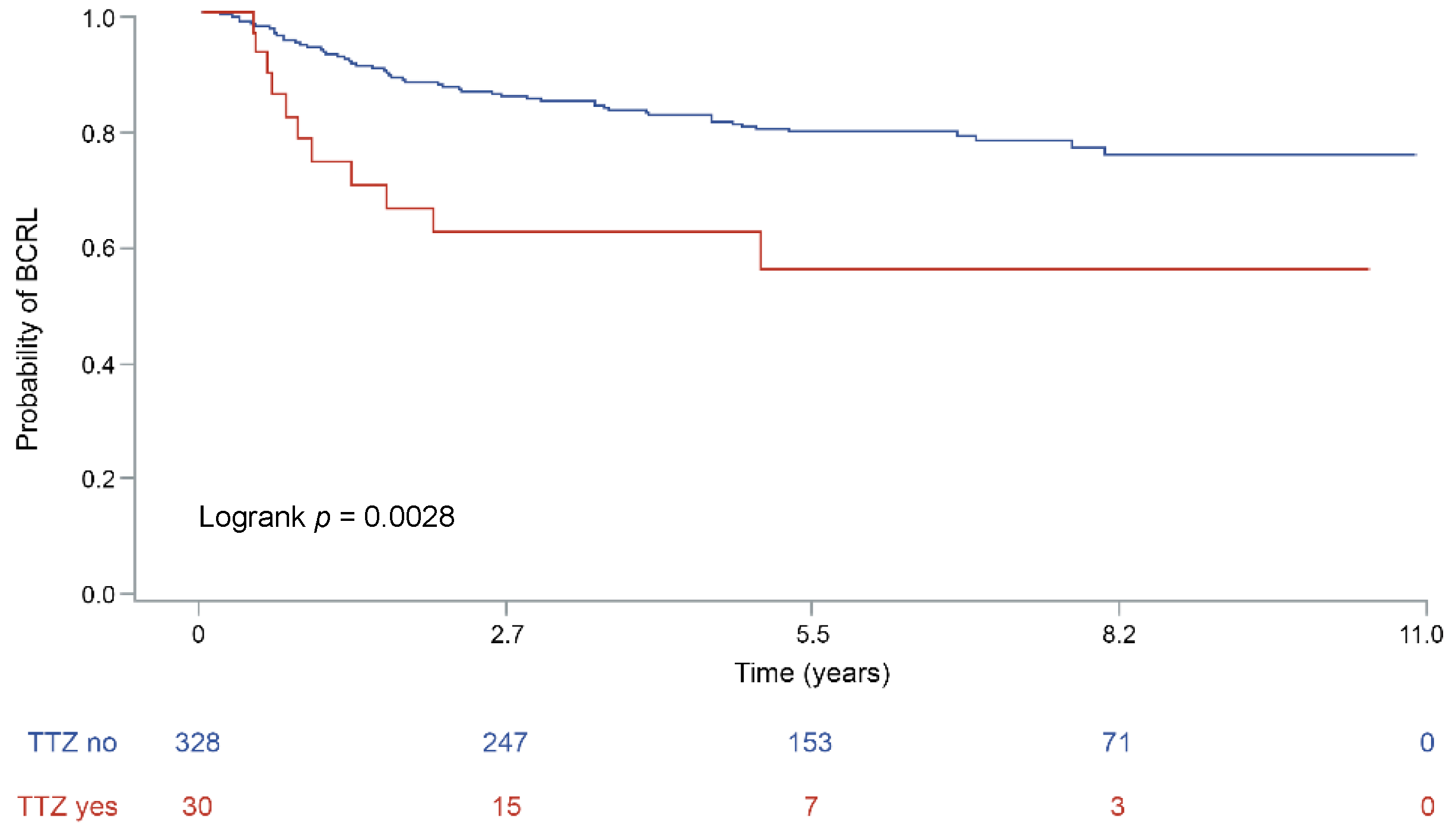
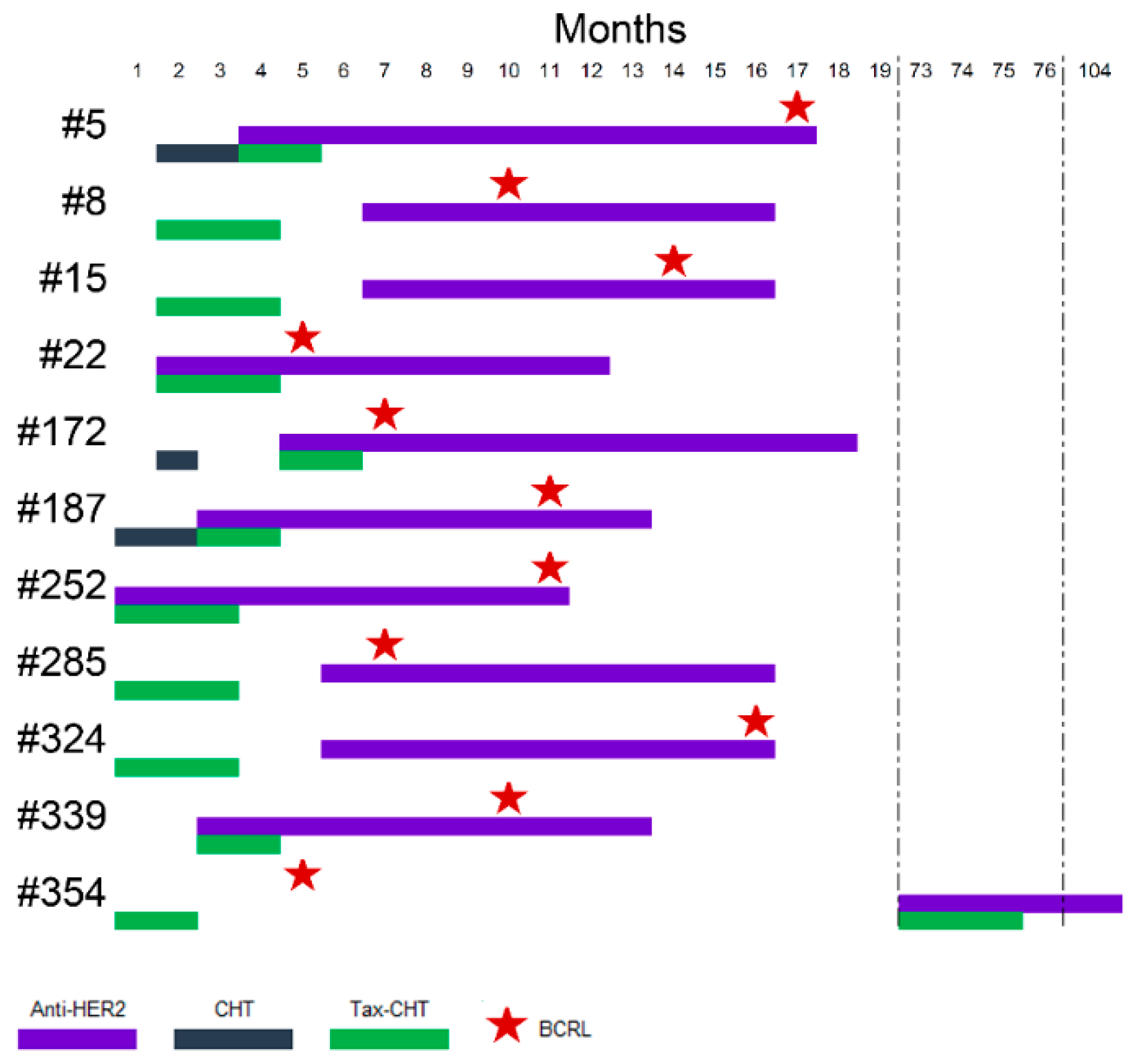
3.5. Anti-Human Epidermal Growth Factor Receptor 2 (HER2) Monoclonal Antibodies Administration Increase the Risk of BCRL
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- De Abreu, F.B.; Schwartz, G.N.; Wells, W.A.; Tsongalis, G.J. Personalized therapy for breast cancer. Clin. Genet. 2014, 86, 62–67. [Google Scholar] [CrossRef]
- American Cancer Society. Global Cancer Facts & Figures, 4th ed.; American Cancer Society: Atlanta, GA, USA, 2018. [Google Scholar]
- Runowicz, C.D.; Leach, C.R.; Henry, N.L.; Henry, K.S.; Mackey, H.T.; Cowens-Alvarado, R.L.; Cannady, R.S.; Pratt-Chapman, M.L.; Edge, S.B.; Jacobs, L.A.; et al. American Cancer Society/American Society of Clinical Oncology Breast Cancer Survivorship Care Guideline. J. Clin. Oncol. 2016, 34, 611–635. [Google Scholar] [CrossRef] [PubMed]
- Halsted, C.P.; Benson, J.R.; Jatoi, I. A historical account of breast cancer surgery: Beware of local recurrence but be not radical. Future Oncol. 2014, 10, 1649–1657. [Google Scholar] [CrossRef] [PubMed]
- Sakorafas, G.H.; Safioleas, M. Breast cancer surgery: An historical narrative. Part III. From the sunset of the 19th to the dawn of the 21st century. Eur. J. Cancer Care (Engl.) 2010, 19, 145–166. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, T.C.; Sayegh, H.E.; Brunelle, C.L.; Daniell, K.M.; Taghian, A.G. Breast cancer-related lymphedema: Risk factors, precautionary measures, and treatments. Gland Surg. 2018, 7, 379–403. [Google Scholar] [CrossRef]
- Michelotti, A.; Invernizzi, M.; Lopez, G.; Lorenzini, D.; Nesa, F.; De Sire, A.; Fusco, N. Tackling the diversity of breast cancer related lymphedema: Perspectives on diagnosis, risk assessment, and clinical management. Breast 2018, 44, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Mortimer, P.S. The pathophysiology of lymphedema. Cancer 1998, 83, 2798–2802. [Google Scholar] [CrossRef]
- Rogan, S.; Taeymans, J.; Luginbuehl, H.; Aebi, M.; Mahnig, S.; Gebruers, N. Therapy modalities to reduce lymphoedema in female breast cancer patients: A systematic review and meta-analysis. Breast Cancer Res. Treat. 2016, 159, 1–14. [Google Scholar] [CrossRef]
- DiSipio, T.; Rye, S.; Newman, B.; Hayes, S. Incidence of unilateral arm lymphoedema after breast cancer: A systematic review and meta-analysis. Lancet Oncol. 2013, 14, 500–515. [Google Scholar] [CrossRef]
- Schrenk, P.; Rieger, R.; Shamiyeh, A.; Wayand, W. Morbidity following sentinel lymph node biopsy versus axillary lymph node dissection for patients with breast carcinoma. Cancer 2000, 88, 608–614. [Google Scholar] [CrossRef]
- Langer, I.; Guller, U.; Berclaz, G.; Koechli, O.R.; Schaer, G.; Fehr, M.K.; Hess, T.; Oertli, D.; Bronz, L.; Schnarwyler, B.; et al. Morbidity of sentinel lymph node biopsy (SLN) alone versus SLN and completion axillary lymph node dissection after breast cancer surgery: A prospective Swiss multicenter study on 659 patients. Ann. Surg. 2007, 245, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, J.I.; Riedel, E.R.; Morrow, M.; Van Zee, K.J. Morbidity of sentinel node biopsy: Relationship between number of excised lymph nodes and patient perceptions of lymphedema. Ann. Surg. Oncol. 2011, 18, 2866–2872. [Google Scholar] [CrossRef] [PubMed]
- Invernizzi, M.; Corti, C.; Lopez, G.; Michelotti, A.; Despini, L.; Gambini, D.; Lorenzini, D.; Guerini-Rocco, E.; Maggi, S.; Noale, M.; et al. Lymphovascular invasion and extranodal tumour extension are risk indicators of breast cancer related lymphoedema: An observational retrospective study with long-term follow-up. BMC Cancer 2018, 18, 935. [Google Scholar] [CrossRef] [PubMed]
- Vieira, R.A.; da Costa, A.M.; de Souza, J.L.; Coelho, R.R.; de Oliveira, C.Z.; Sarri, A.J.; Junior, R.J.; Zucca-Matthes, G. Risk Factors for Arm Lymphedema in a Cohort of Breast Cancer Patients Followed up for 10 Years. Breast Care 2016, 11, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Tsai, R.J.; Dennis, L.K.; Lynch, C.F.; Snetselaar, L.G.; Zamba, G.K.; Scott-Conner, C. The risk of developing arm lymphedema among breast cancer survivors: A meta-analysis of treatment factors. Ann. Surg. Oncol. 2009, 16, 1959–1972. [Google Scholar] [CrossRef]
- Curigliano, G.; Burstein, H.J.; P Winer, E.; Gnant, M.; Dubsky, P.; Loibl, S.; Colleoni, M.; Regan, M.M.; Piccart-Gebhart, M.; Senn, H.J.; et al. De-escalating and escalating treatments for early-stage breast cancer: The St. Gallen International Expert Consensus Conference on the Primary Therapy of Early Breast Cancer 2017. Ann. Oncol. 2017, 28, 1700–1712. [Google Scholar] [CrossRef]
- Cariati, M.; Bains, S.K.; Grootendorst, M.R.; Suyoi, A.; Peters, A.M.; Mortimer, P.; Ellis, P.; Harries, M.; Van Hemelrijck, M.; Purushotham, A.D. Adjuvant taxanes and the development of breast cancer-related arm lymphoedema. Br. J. Surg. 2015, 102, 1071–1078. [Google Scholar] [CrossRef]
- Lee, M.J.; Beith, J.; Ward, L.; Kilbreath, S. Lymphedema following taxane-based chemotherapy in women with early breast cancer. Lymphat. Res. Biol. 2014, 12, 282–288. [Google Scholar] [CrossRef]
- Swaroop, M.N.; Ferguson, C.M.; Horick, N.K.; Skolny, M.N.; Miller, C.L.; Jammallo, L.S.; Brunelle, C.L.; O’Toole, J.A.; Isakoff, S.J.; Specht, M.C.; et al. Impact of adjuvant taxane-based chemotherapy on development of breast cancer-related lymphedema: Results from a large prospective cohort. Breast Cancer Res. Treat 2015, 151, 393–403. [Google Scholar] [CrossRef]
- Zhu, W.; Li, D.; Li, X.; Ren, J.; Chen, W.; Gu, H.; Shu, Y.; Wang, D. Association between adjuvant docetaxel-based chemotherapy and breast cancer-related lymphedema. Anticancer Drugs 2017, 28, 350–355. [Google Scholar] [CrossRef]
- Jammallo, L.S.; Miller, C.L.; Singer, M.; Horick, N.K.; Skolny, M.N.; Specht, M.C.; O’Toole, J.; Taghian, A.G. Impact of body mass index and weight fluctuation on lymphedema risk in patients treated for breast cancer. Breast Cancer Res. Treat. 2013, 142, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Hidding, J.T.; Viehoff, P.B.; Beurskens, C.H.; van Laarhoven, H.W.; Nijhuis-van der Sanden, M.W.; van der Wees, P.J. Measurement Properties of Instruments for Measuring of Lymphedema: Systematic Review. Phys. Ther. 2016, 96, 1965–1981. [Google Scholar] [CrossRef] [PubMed]
- Smoot, B.J.; Wong, J.F.; Dodd, M.J. Comparison of diagnostic accuracy of clinical measures of breast cancer-related lymphedema: Area under the curve. Arch. Phys. Med. Rehabil. 2011, 92, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, S.R.; Ellis, I.O.; Schnitt, S.J.; Tan, P.H.; van de Vijver, M.J. WHO Classification of Tumours of the Breast, 4th ed.; IARC Press: Lyon, France, 2012. [Google Scholar]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.H.; Pinder, S.E.; Macmillan, R.D.; Mitchell, M.; Ellis, I.O.; Elston, C.W.; Blamey, R.W. Prognostic value of lymphovascular invasion in women with lymph node negative invasive breast carcinoma. Eur. J. Cancer 2006, 42, 357–362. [Google Scholar] [CrossRef]
- Rosen, P.P. Tumor emboli in intramammary lymphatics in breast carcinoma: Pathologic criteria for diagnosis and clinical significance. Pathol. Annu. 1983, 18 Pt 2, 215–232. [Google Scholar]
- Gooch, J.; King, T.A.; Eaton, A.; Dengel, L.; Stempel, M.; Corben, A.D.; Morrow, M. The extent of extracapsular extension may influence the need for axillary lymph node dissection in patients with T1-T2 breast cancer. Ann. Surg. Oncol. 2014, 21, 2897–2903. [Google Scholar] [CrossRef]
- Gruber, G.; Cole, B.F.; Castiglione-Gertsch, M.; Holmberg, S.B.; Lindtner, J.; Golouh, R.; Collins, J.; Crivellari, D.; Thürlimann, B.; Simoncini, E.; et al. Extracapsular tumor spread and the risk of local, axillary and supraclavicular recurrence in node-positive, premenopausal patients with breast cancer. Ann. Oncol. 2008, 19, 1393–1401. [Google Scholar] [CrossRef]
- Gruber, G.; Bonetti, M.; Nasi, M.L.; Price, K.N.; Castiglione-Gertsch, M.; Rudenstam, C.M.; Holmberg, S.B.; Lindtner, J.; Golouh, R.; Collins, J.; et al. Prognostic value of extracapsular tumor spread for locoregional control in premenopausal patients with node-positive breast cancer treated with classical cyclophosphamide, methotrexate, and fluorouracil: Long-term observations from International Breast Cancer Study Group Trial VI. J. Clin. Oncol. 2005, 23, 7089–7097. [Google Scholar] [CrossRef]
- Dobi, E.; Bazan, F.; Dufresne, A.; Demarchi, M.; Villanueva, C.; Chaigneau, L.; Montcuquet, P.; Ivanaj, A.; Sautière, J.L.; Maisonnette-Escot, Y.; et al. Is extracapsular tumour spread a prognostic factor in patients with early breast cancer? Int. J. Clin. Oncol. 2013, 18, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Fusco, N.; Lopez, G.; Corti, C.; Pesenti, C.; Colapietro, P.; Ercoli, G.; Gaudioso, G.; Faversani, A.; Gambini, D.; Michelotti, A.; et al. Mismatch Repair Protein Loss as a Prognostic and Predictive Biomarker in Breast Cancers Regardless of Microsatellite Instability. JNCI Cancer Spectr. 2018, 2, pky056. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S.; May, S. Applied Survival Analysis: Regression Modeling of Time-to-Event Data; Wiley: Hoboken, NJ, USA, 2011. [Google Scholar]
- Vittinghoff, E.; McCulloch, C.E. Relaxing the rule of ten events per variable in logistic and Cox regression. Am. J. Epidemiol. 2007, 165, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Denis, D.J. Applied Univariate, Bivariate, and Multivariate Statistics; Wiley: Hoboken, NJ, USA, 2015. [Google Scholar]
- Fusco, N.; Guerini-Rocco, E.; Del Gobbo, A.; Franco, R.; Zito-Marino, F.; Vaira, V.; Bulfamante, G.; Ercoli, G.; Nosotti, M.; Palleschi, A.; et al. The Contrasting Role of p16Ink4A Patterns of Expression in Neuroendocrine and Non-Neuroendocrine Lung Tumors: A Comprehensive Analysis with Clinicopathologic and Molecular Correlations. PLoS ONE 2015, 10, e0144923. [Google Scholar] [CrossRef] [PubMed]
- Semb, K.A.; Aamdal, S.; Oian, P. Capillary protein leak syndrome appears to explain fluid retention in cancer patients who receive docetaxel treatment. J. Clin. Oncol. 1998, 16, 3426–3432. [Google Scholar] [CrossRef] [PubMed]
- Fusco, N.; Bosari, S. HER2 aberrations and heterogeneity in cancers of the digestive system: Implications for pathologists and gastroenterologists. World J. Gastroenterol. 2016, 22, 7926–7937. [Google Scholar] [CrossRef]
- Schoppmann, S.F.; Tamandl, D.; Roberts, L.; Jomrich, G.; Schoppmann, A.; Zwrtek, R.; Dubsky, P.; Gnant, M.; Jakesz, R.; Birner, P. HER2/neu expression correlates with vascular endothelial growth factor-C and lymphangiogenesis in lymph node-positive breast cancer. Ann. Oncol. 2010, 21, 955–960. [Google Scholar] [CrossRef]
- Marino, D.; Angehrn, Y.; Klein, S.; Riccardi, S.; Baenziger-Tobler, N.; Otto, V.I.; Pittelkow, M.; Detmar, M. Activation of the epidermal growth factor receptor promotes lymphangiogenesis in the skin. J. Dermatol. Sci. 2013, 71, 184–194. [Google Scholar] [CrossRef]
- Deltombe, T.; Jamart, J.; Recloux, S.; Legrand, C.; Vandenbroeck, N.; Theys, S.; Hanson, P. Reliability and limits of agreement of circumferential, water displacement, and optoelectronic volumetry in the measurement of upper limb lymphedema. Lymphology 2007, 40, 26–34. [Google Scholar]
- Borthwick, Y.; Paul, L.; Sneddon, M.; McAlpine, L.; Miller, C. Reliability and validity of the figure-of-eight method of measuring hand size in patients with breast cancer-related lymphoedema. Eur. J. Cancer Care (Engl.) 2013, 22, 196–201. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| BCRL+ (n = 75) | BCRL− (n = 293) | p-Value | |
|---|---|---|---|
| Age at diagnosis, years, mean ± SD | 57.9 ± 13.1 | 59.5 ± 12.9 | 0.3879 |
| Menopause, n (%) | |||
| Peri- | 1 (1.4) | 9 (3.1) | 0.6845 |
| Post- | 49 (67.1) | 195 (67.7) | |
| Pre- | 23 (31.5) | 84 (29.1) | |
| Smoking status, current smoker, n (%) | 8 (10.7) | 29 (9.9) | 0.8433 |
| BMI, mean ± SD | 27.0 ± 5.6 | 26.9 ± 5.4 | 0.9572 |
| Obesity, BMI ≥ 30 kg/m2 n (%) | 16 (21.3) | 78 (26.6) | 0.3488 |
| Diabetes mellitus, n (%) | 7 (9.3) | 19 (6.5) | 0.3903 |
| Cardiovascular diseases, n (%) | 25 (33.3) | 83 (28.3) | 0.3956 |
| Systemic infections, n (%) | 10 (13.3) | 18 (6.1) | 0.0361 |
| Blood disorders, n (%) | 6 (8.0) | 25 (8.5) | 0.8822 |
| Bone and joints diseases, n (%) | 7 (9.3) | 32 (10.9) | 0.6901 |
| Dyslipidemia, n (%) | 5 (6.7) | 44 (15.0) | 0.0575 |
| Gastrointestinal diseases, n (%) | 14 (18.7) | 51 (17.4) | 0.7984 |
| Diseases of the urinary tract, n (%) | 4 (5.3) | 16 (5.5) | 1.0000 |
| Diseases of the reproductive tract, n (%) | 12 (16.0) | 49 (16.7) | 0.8805 |
| Central nervous system diseases, n (%) | 1 (1.3) | 25 (8.5) | 0.0299 |
| Other neoplasms, n (%) | 10 (13.3) | 42 (14.3) | 0.8242 |
| BCRL+ (n = 75) | BCRL− (n = 293) | p-Value | |
|---|---|---|---|
| Breast surgery, n (%) | |||
| Conservative | 47 (62.7) | 177 (60.4) | 0.7208 |
| Mastectomy | 28 (37.3) | 116 (39.6) | |
| Axillary surgery, n (%) | |||
| En bloc dissection | 75 (100.0) | 274 (93.5) | 0.0178 |
| Sentinel lymph node | 0 (0.0) | 19 (6.5) | |
| Radiotherapy, n (%) | |||
| No WBI WBI + SCF SCF + CW | 21 (28.0) 36 (48.0) 7 (9.3) 11 (14.7) | 78 (26.6) 153 (52.2) 16 (5.5) 46 (15.7) | 0.6318 |
| Chemotherapy, n (%) | |||
| No Taxanes Other protocols | 22 (29.3) 45 (60.0) 8 (10.7) | 153 (52.2) 110 (37.5) 30 (10.2) | 0.0010 |
| Hormone therapy, n (%) | |||
| No SERM Aromatase inhibitors SERM + Aromatase inhibitors SERM + LHRH agonists | 14 (18.7) 6 (8.0) 34 (45.3) 11 (14.7) 10 (13.3) | 36 (12.3) 43 (14.7) 135 (46.1) 44 (15.0) 35 (12.0) | 0.4206 |
| Duration of the intake (days), median (Q1, Q3) | |||
| SERM Aromatase inhibitors LHRH agonists | 301 (252; 349) 1586 (1095; 1827) 1200 (731; 1358) | 300 (216; 371) 1544 (967; 1836) 989 (708; 1765) | 1.0000 0.8658 0.9343 |
| Trastuzumab, n (%) | 11 (14.7) | 19 (6.5) | 0.0209 |
| Breast surgery, n (%) | |||
| Conservative | 47 (62.7) | 177 (60.4) | 0.7208 |
| Mastectomy | 28 (37.3) | 116 (39.6) | |
| Axillary surgery, n (%) | |||
| En bloc dissection | 75 (100.0) | 274 (93.5) | 0.0178 |
| Sentinel lymph node | 0 (0.0) | 19 (6.5) | |
| Radiotherapy, n (%) | |||
| No WBI WBI + SCF SCF + CW | 21 (28.0) 36 (48.0) 7 (9.3) 11 (14.7) | 78 (26.6) 153 (52.2) 16 (5.5) 46 (15.7) | 0.6318 |
| Chemotherapy, n (%) | |||
| No Taxanes Other protocols | 22 (29.3) 45 (60.0) 8 (10.7) | 153 (52.2) 110 (37.5) 30 (10.2) | 0.0010 |
| Hormone therapy, n (%) | |||
| No SERM Aromatase inhibitors SERM + Aromatase inhibitors SERM + LHRH agonists | 14 (18.7) 6 (8.0) 34 (45.3) 11 (14.7) 10 (13.3) | 36 (12.3) 43 (14.7) 135 (46.1) 44 (15.0) 35 (12.0) | 0.4206 |
| Duration of the intake (days), median (Q1, Q3) | |||
| SERM Aromatase inhibitors LHRH agonists | 301 (252; 349) 1586 (1095; 1827) 1200 (731; 1358) | 300 (216; 371) 1544 (967; 1836) 989 (708; 1765) | 1.0000 0.8658 0.9343 |
| Trastuzumab, n (%) | 11 (14.7) | 19 (6.5) | 0.0209 |
| HR | 95% CI | p-Value | ||
|---|---|---|---|---|
| Systemic infections | 1.88 | 0.95–3.71 | 0.0703 | |
| Chemotherapy, no | 1.00 | |||
| Taxanes Other protocols | 2.24 1.21 | 1.26–3.98 0.50–2.94 | 0.0060 0.6684 | |
| Trastuzumab | 2.70 | 1.31–5.55 | 0.0071 | |
| No radiotherapy, no | 1.00 | |||
| WBI WBI + SCF SCF + CW | 0.73 0.71 0.45 | 0.42–1.28 0.29–1.73 0.20–0.98 | 0.2678 0.4549 0.0446 | |
| Side | ENE | 0.0144 | ||
| Right | Yes vs. No | 3.11 | 1.45–6.65 | |
| Left | Yes vs. No | 0.76 | 0.32–1.78 | |
| Side | LVI | 0.0208 | ||
| Right | Yes vs. No | 1.09 | 0.59–2.00 | |
| Left | Yes vs. No | 3.56 | 1.61–7.87 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Invernizzi, M.; Michelotti, A.; Noale, M.; Lopez, G.; Runza, L.; Giroda, M.; Despini, L.; Blundo, C.; Maggi, S.; Gambini, D.; et al. Breast Cancer Systemic Treatments and Upper Limb Lymphedema: A Risk-Assessment Platform Encompassing Tumor-Specific Pathological Features Reveals the Potential Role of Trastuzumab. J. Clin. Med. 2019, 8, 138. https://doi.org/10.3390/jcm8020138
Invernizzi M, Michelotti A, Noale M, Lopez G, Runza L, Giroda M, Despini L, Blundo C, Maggi S, Gambini D, et al. Breast Cancer Systemic Treatments and Upper Limb Lymphedema: A Risk-Assessment Platform Encompassing Tumor-Specific Pathological Features Reveals the Potential Role of Trastuzumab. Journal of Clinical Medicine. 2019; 8(2):138. https://doi.org/10.3390/jcm8020138
Chicago/Turabian StyleInvernizzi, Marco, Anna Michelotti, Marianna Noale, Gianluca Lopez, Letterio Runza, Massimo Giroda, Luca Despini, Concetta Blundo, Stefania Maggi, Donatella Gambini, and et al. 2019. "Breast Cancer Systemic Treatments and Upper Limb Lymphedema: A Risk-Assessment Platform Encompassing Tumor-Specific Pathological Features Reveals the Potential Role of Trastuzumab" Journal of Clinical Medicine 8, no. 2: 138. https://doi.org/10.3390/jcm8020138
APA StyleInvernizzi, M., Michelotti, A., Noale, M., Lopez, G., Runza, L., Giroda, M., Despini, L., Blundo, C., Maggi, S., Gambini, D., & Fusco, N. (2019). Breast Cancer Systemic Treatments and Upper Limb Lymphedema: A Risk-Assessment Platform Encompassing Tumor-Specific Pathological Features Reveals the Potential Role of Trastuzumab. Journal of Clinical Medicine, 8(2), 138. https://doi.org/10.3390/jcm8020138