Validation and Adaptation of the Multidimensional Prognostic Index in an Older Australian Cohort


1
Discipline of Clinical Pharmacology, College of Medicine and Public Health, Flinders University and Flinders Medical Centre, Bedford Park, 5042, South Australia, Australia
2
Flinders Centre for Epidemiology and Biostatistics, College of Medicine and Public Health, Flinders University, Bedford Park, 5042, South Australia, Australia
*
Authors to whom correspondence should be addressed.
J. Clin. Med. 2019, 8(11), 1820; https://doi.org/10.3390/jcm8111820
Submission received: 6 September 2019
/
Revised: 29 October 2019
/
Accepted: 29 October 2019
/
Published: 1 November 2019
(This article belongs to the Section Epidemiology & Public Health)
Abstract
:Background and aims: The Multidimensional Prognostic Index (MPI), an objective and quantifiable tool based on the Comprehensive Geriatric Assessment, has been shown to predict adverse outcomes in European cohorts. We conducted a validation study of the original MPI, and of adapted versions that accounted for the use of specific drugs and cultural diversity in the assessment of cognition, in older Australians. Methods: The capacity of the MPI to predict 12-month mortality was assessed in 697 patients (median age: 80 years; interquartile range: 72–86) admitted to a metropolitan teaching hospital between September 2015 and February 2017. Results: In simple logistic regression analysis, the MPI was associated with 12-month mortality (Low risk: OR reference group; moderate risk: OR 2.50, 95% CI: 1.67–3.75; high risk: OR 4.24, 95% CI: 2.28–7.88). The area under the receiver operating characteristic curve (AUC) for the unadjusted MPI was 0.61 (0.57–0.65) and 0.64 (95% CI: 0.59–0.68) with age and sex adjusted. The adapted versions of the MPI did not significantly change the AUC of the original MPI. Conclusion: The original and adapted MPI were strongly associated with 12-month mortality in an Australian cohort. However, the discriminatory performance was lower than that reported in European studies.
1. Introduction
The global population is continuously expanding and ageing as a result of significant advances in human health and favourable economic conditions [1]. However, this phenomenon also imposes significant public health and financial challenges [2]. For example, older adults often suffer from the unwanted consequences of acute and chronic diseases, particularly reduced quality of life, disability and loss of independence [3]. The introduction of the Comprehensive Geriatric Assessment (CGA) into geriatric care and the establishment of dedicated hospital wards and staff has improved the standard of care for older patients [4]. At the same time, hospitalists are ever more expected to accelerate patient turn-over, reduce the length of hospital stay and readmission rate, and arrange appropriate post-discharge follow-up. However, accurately predicting and identifying the most suitable care pathways for older in-patients, with multiple co-morbidities and significant inter-individual variability in organ function and homeostatic capacity, is problematic.
The addition of screening tools being implemented alongside the CGA has furthermore contributed to improved care [5,6,7,8]. This has led to the development of clinical prediction rules that combine previously established tools for predicting adverse outcomes in older adults. One of them, the Multidimensional Prognostic Index (MPI), is an objective and quantifiable CGA-based tool, based on eight domains, that is used to estimate short- and medium-term adverse outcomes in older patients [9].
A number of studies have validated the MPI in different sub-populations suffering from acute and chronic conditions either in hospital or in the community [10,11,12,13,14,15,16,17,18,19]. However, there are some potential limitations of the MPI. Firstly, the MPI has not been investigated in non-European populations by investigators not involved in the original studies. The latter have primarily been conducted within the same area of Italy [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30] with the exception of two studies that were conducted in France [31] and Sweden [32]. An important reason for validating the MPI in different geographical settings is due to possible variations in admission criteria and thresholds under different health care settings. This may result in in-hospital patient populations that are substantially different, particularly regarding co-morbidity burden and frailty, from those investigated in the original studies.
Additional potential limitations are related to two specific MPI domains, medication use and cognitive function. The medications domain of the MPI collects information regarding the total number of medications a patient is currently taking [9]. The concomitant use of ≥5 medications, known as polypharmacy, has been shown to independently predict adverse outcomes, such as falls and mortality in older adults [33,34]. However, other studies have failed to show significant associations between the total number of medications and the previously mentioned adverse outcomes [35,36,37,38]. Assessing exposure to specific drugs known to increase the risk of physical and/or cognitive decline, such as anticholinergics, with validated scoring systems could identify an area of the MPI to potentially further improve the predictive accuracy [39]. The assessment of cognitive function in the MPI is based on the short portable mental state questionnaire (SPMSQ); however, using this instrument might be problematic in a culturally diverse patient population as the SPMSQ relies on known cultural knowledge. Using a cognitive assessment tool that is not influenced by language, gender or educational status such as the Rowland University Dementia Assessment Scale (RUDAS) might allow a more accurate assessment of cognitive function and, therefore, better predictive capacity [40].
As no information is currently available about the applicability, predictive accuracy and validity of the MPI in Australian cohorts we conducted a validation study of the original instrument, and of adapted versions that accounted for the use of specific drug classes and cultural diversity in the assessment of cognitive function, in a population of older in-patients. This information is essential to determine whether this instrument could be easily and accurately applied to Australian patient populations or whether additional modifications are warranted.
2. Methods
2.1. Study Population
This was a prospective cohort study conducted according to the Declaration of Helsinki and guidelines for Good Clinical Practice. Approval for the study was obtained from local Ethics Committee (reference number 170.15). The study was conducted at Flinders Medical Centre (FMC), a 593-bed metropolitan teaching and trauma hospital within the Southern Adelaide Local Health Network that has a catchment area of approximately 350,000 people. All patients aged ≥ 65 years who presented to Flinders Emergency Department, were admitted to FMC Acute Medical Unit (AMU) and then transferred under either General Medical or Acute Care of the Elderly (ACE) wards from 14 September 2015 to 17 February 2017, were screened for eligibility. ACE wards provide a comprehensive individualised approach in assessing older frail medical in-patients using a multidisciplinary team involving physiotherapists, occupational therapists, social workers, nutrition and dietetics, nursing staff, and geriatricians. Inclusion criteria were: (i) ability to provide informed consent or ability of a proxy for informed consent; and (ii) no diagnosis of dementia prior to hospital admission.
2.2. Original MPI
The 63-item MPI, a prognostic tool based on a standard CGA, was assessed in all study participants in General Medical or ACE wards within the first three days of hospital admission [9]. The MPI score, ranging from 0 to 1, is based on averaging the standardised scores obtained from the eight core domains of the CGA. These eight domains consist of co-habitation status (living alone, with family/friends or in an institute); the total number of medications (taken at admission); functional status evaluated with activities of daily living (ADL) [6] and the instrumental ADL (IADL) [41] scales; cognitive status evaluated by the Short Portable Mental Status Questionnaire (SPMSQ) [42]; evaluation of pressure sores using the Exton Smith Scale (ESS) [43]; co-morbidities assessed using the Cumulative Illness Rating Scale (CIRS) [44]; and nutritional status evaluated by the Mini Nutritional Assessment (MNA) [45]. Each of the domains were given conventional cut-off points derived from the literature with points then allocated as 0 = no problems, 0.5 = minor problems and 1 = major problems. The continuous MPI score (based on the sum of the eight domains’ points and then divided by eight) was then categorised into three risk groups (mild = 0.0–0.33; moderate = 0.34–0.66; severe = 0.66–1.0) [9]. A printable version was used for bedside interviews, with minor adaptations to the SPMSQ domain where ‘President/Pope’ was changed to ‘Prime Minister’.
2.3. Adapted MPI
2.3.1. Medications with Anticholinergic Effects
In addition to assessing the total number of medications, medication use was further characterised by identifying specific drugs with anticholinergic effects, using the validated exposure scoring system Anticholinergic Risk Scale (ARS) [39]. The ARS ranks the anticholinergic effect of each drug on a scale of 0 (limited or none), 1 (moderate), 2 (strong), and 3 (very strong), based on the dissociation constant for the muscarinic receptor, rates of anticholinergic effects vs. placebo in experimental studies and a literature review on anticholinergic adverse effects. The ARS score is calculated by summing the ARS rankings assigned for each of the prescribed drugs in a patient [9].
2.3.2. RUDAS
The six-item RUDAS was used as an additional assessment for cognitive function with a score out of 30 points [46]. Due to the array of cultural, religious, and language backgrounds in the Australian population this tool has been specifically designed to minimise these effects and gain a more accurate assessment of cognitive function. It takes approximately 10 minutes to complete.
2.3.3. Adapted MPI Models
Three models were assessed:
- MPI with number of medications domain substituted with the ARS score. Cut-off points were applied to the ARS score with 0 points for patients not on any anticholinergics, 0.5 points for patients on 1–2 anticholinergics, and 1 point for patients taking >2 anticholinergics.
- MPI with SPMSQ domain substituted with the RUDAS score. Cut-off points were applied to the RUDAS score with 0 points for patients who had a RUDAS score >25 points, 0.5 points for patients who had a RUDAS score between 25 and 17 points, and 1 point for patients who had a RUDAS score < 17 points.
- MPI with both the number of medications and SPMSQ domains substituted with ARS and RUDAS scores using the above cut-off points.
2.4. Outcome Measures
The primary outcome was all-cause mortality within 12-months. All-cause mortality was defined as death from any cause. This was obtained using the Australian national death registry. This information was collected and updated every three months.
A number of secondary outcomes were included: in-hospital all-cause mortality, in-hospital falls, and delirium. In-hospital falls were defined as any fall reported in the medical notes. Information regarding the number of falls during the assessment admission was collected together with time elapsed (in days) until first fall and consequences of the fall (none, soft tissue damage, fracture). Delirium was identified as present if the medical team stated this diagnosis in the medical notes. The presence of delirium at admission was recorded to determine if delirium was present pre-admission or developed during admission. Any uncertainties were discussed with a qualified clinician (A. A. M.). This method has been recently highlighted as a more reliable way of capturing the incidence of delirium as opposed to using IDC coding [47]. Other secondary outcomes were length of hospital stay (in days) and hospital re-admission rates for one-, three-, and six-months.
2.5. Statistical Analysis
Based on Pilotto’s derivation study, a sample size of N = 750 patients was sufficient to provide 80% statistical power to detect an odds ratio of 1.55 for each category increase in the original MPI using a two-sided Type 1 error rate of p < 0.05, assuming a 12-month mortality rate of 5.7% in the lowest MPI category [9].
Patients’ baseline characteristics were reported as mean ± standard deviations (SD), or frequency and percentages. Comparison of baseline values of the original MPI, RUDAS, ARS, and AMT for subjects that completed follow-up and those that were lost to follow-up were assessed using a Mann–Whitney U test. Differences in in-hospital mortality, gender and mortality at 1-, 3-, 6-, and 12-months were compared using chi-squared tests (see supplementary file). A Kruskall–Wallis test was used to compare age and length of hospital stay (LOS, in days) across MPI risk categories. In-hospital mortality, mortality at 1-, 3-, 6-, and 12-months, falls, and the incidence of delirium was compared across the MPI risk categories using chi-squared tests of independence.
Simple and multiple logistic regression with adjustment for age and sex was conducted to assess the association between the original MPI and 12-month all-cause mortality. We adjusted for these variables as neither age nor sex is included in the original MPI. Furthermore, a recent study reported a higher prevalence of women in the severe risk category [48].
Area under the receiver operating characteristic (ROC) curve was used to measure the diagnostic accuracy of the original MPI. In order to assess whether the diagnostic value of the adapted MPI was superior to original MPI, comparison of the resultant area under the ROC curves was conducted. Secondary outcomes (in-hospital falls, in-hospital delirium, in-hospital mortality, one-, three-, six-month all-cause mortality, and one-month re-admission rate) were also assessed using logistic regression and area under ROC curves.
Cox proportional hazards analysis adjusted for age and sex was conducted as a sensitivity analysis to assess the risk of all-cause mortality across the original MPI risk categories whilst accounting for total follow-up time. Follow-up time was defined as the time since hospital discharge (when the original MPI was assessed) until the end of follow-up (30 June 2018) or death, whichever occurred first. Estimated survival was also presented graphically using Kaplan–Meier curves.
Simple and multiple Poisson regression adjusted for age and sex was conducted to compare incidence of in-hospital falls, and readmissions within three- and six-months across the original MPI risk groups.
Data analyses were performed using the STATA statistical software Version 15.1 (StataCorp©, College City, Texas, USA).
3. Results
3.1. Study Patient Characteristics
Between 14 September 2015 and 17 February 2017, 738 medical in-patients received an MPI assessment at FMC. Forty-one patients were excluded from the analysis (N = 1 with incomplete original MPI, and N = 40 lost to follow-up). The final study cohort included 697 patients (348 men and 349 women) with a median age of 80 (Interquartile range (IQR): 72–86), and an age range between 65 and 102 years. No difference in patient characteristics was observed in the 40 patients lost to follow-up compared to the included patient cohort (n = 697) (Supplementary Table S1).
Most patients were included in the moderate MPI risk category (57.8%) while a third were in the mild risk category (33.9%) and a relatively small proportion in the severe risk category (8.3%) (Table 1). Higher original MPI scores were significantly associated with older age (p < 0.001), female sex (p < 0.001), in-hospital mortality (p < 0.001), delirium (p < 0.001), falls (p = 0.021), longer LOS (p = 0.001), and higher mortality after one month (p < 0.001), 3 months (p < 0.001), six months (p < 0.001), and 12 months (p < 0.001). Re-admission within three months (p = 0.022), and six months (p = 0.0079) were also significantly different across the MPI risk groups. Re-admission rates for one-month did not significantly differ between MPI risk groups (p = 0.1572).
3.2. Validation of Original MPI—12-Month All-Cause Mortality
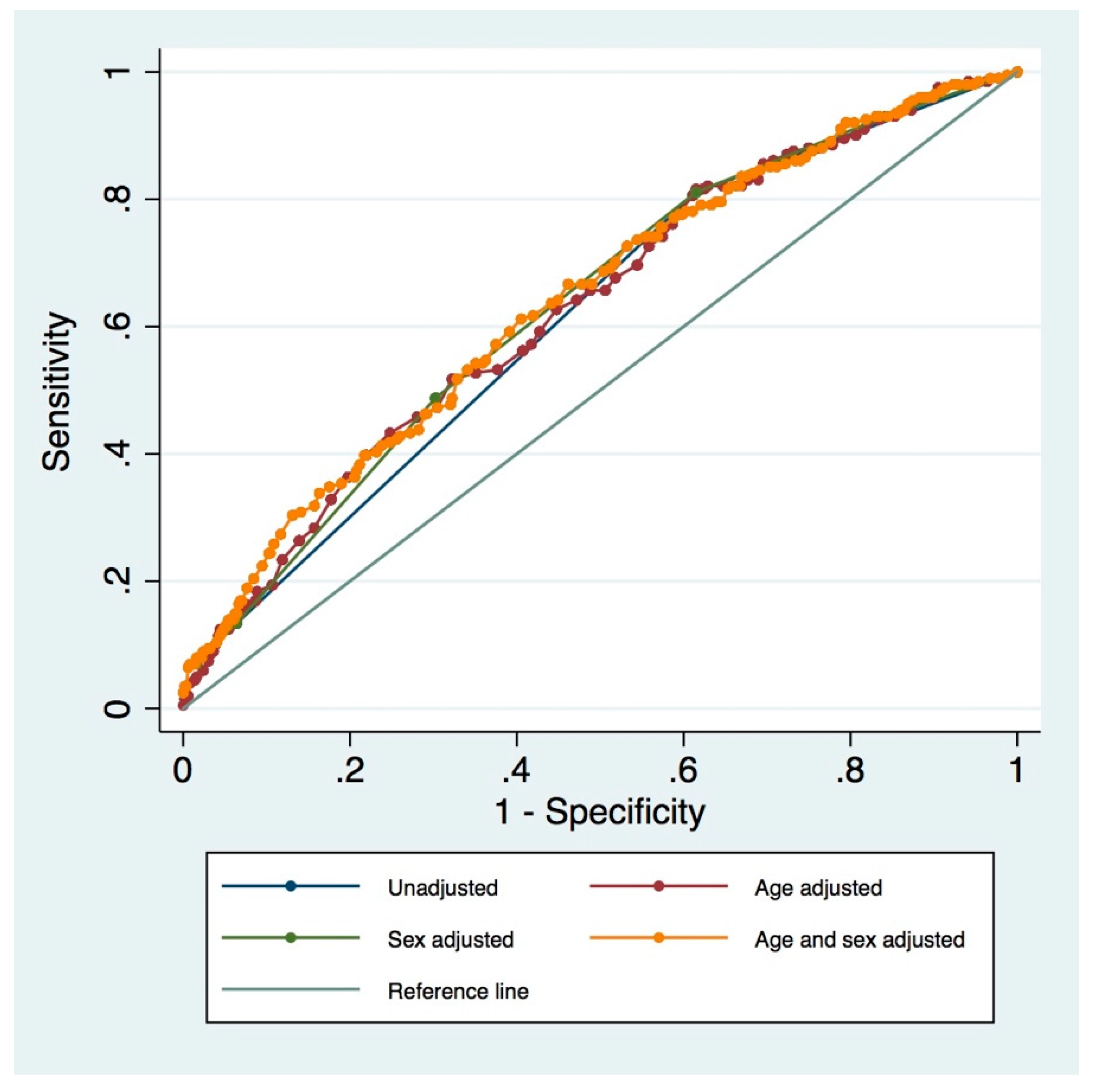
In simple logistic regression analysis, the MPI was associated with 12-month all-cause mortality (mild: OR reference group; moderate: OR 2.50, 95% CI: 1.67–3.75; severe: OR 4.24, 95% CI: 2.28–7.88). Multiple logistic regression adjusted for age and sex were significant for 12-month all-cause mortality (Supplementary Table S2). The median (inter-quartile range) of follow-up time was 1.62 (0.74–2.45) years and the hazard ratios for all-cause mortality from the Cox proportional hazards regression analysis were similar, although slightly smaller, to the odds ratios for all-cause mortality (Supplementary Table S3 and Figure 1).
The diagnostic accuracy (area under the ROC curve) for the MPI adjusted for age and sex was 0.639 (95% CI: 0.593–0.684; Figure 1).
3.3. Adapted MPI
Substituting the total number of medications and the SPMSQ domain with the ARS/RUDAS scores, respectively, into the original MPI, also resulted in an association with 12-month all-cause mortality (Supplementary Table S4). There were no differences when comparing the original MPI to the adapted MPI’s area under the ROC curve (original MPI/adapted MPI with ARS substitution p = 0.619; original MPI/adapted MPI with RUDAS substitution p = 0.958; original MPI/adapted MPI with ARS and RUDAS substitution p = 0.673). Adjusting for age and sex did not substantially change the area under the ROC curves (Supplementary Table S4).
3.4. MPI and Secondary Outcomes
The MPI was associated with one-, three-, and six-month all-cause mortality (Table 2). The area under the ROC curve for the MPI and one-, three-, and six-month all-cause mortality was 0.708 (95% CI: 0.63–0.79), 0.671 (95% CI: 0.61–0.73), and 0.621 (95% CI: 0.58–0.66), respectively.
In simple logistic regression, the MPI was associated with in-hospital all-cause mortality, but not with in-hospital delirium and one-month re-admission rate (Table 2). The area under the ROC curve for the MPI and in-hospital all-cause mortality and in-hospital delirium was 0.719 (95% CI: 0.64–0.80) and 0.634 (95% CI: 0.57–0.70), respectively.
A total of 95 (13.6%) patients were re-admitted within one-month of which 77 (11.0%) had a single re-admission and 18 (2.6%) had multiple re-admissions. The top three most common reasons for readmission within one month were congestive heart failure (CHF; 7.4%), non-ST elevation myocardial infarction (NSTEMI; 3.2%), hypotension (3.2%), pneumonia unspecified (3.2%), chronic obstructive pulmonary disease (COPD) with acute lower respiratory infection (3.2%), acute kidney failure (3.2%), and neoplastic (malignant) related fatigue (3.2%). A total of 206 (29.56%) patients were re-admitted within three months, of which 133 (19.08%) had a single re-admission and 73 (10.47%) had multiple re-admissions. The top three most common reasons for readmission within three months were CHF (10.2%), COPD with acute lower respiratory infection (10.2%), and pneumonia unspecified (5.8%). A total of 291 (41.75%) patients were re-admitted within six months, of which 159 (22.81%) had a single re-admission and 132 (18.93%) had multiple re-admissions. The top three most common reasons for readmission within 6 months were COPD with acute lower respiratory infection (13.4%), CHF (10%), and pneumonia unspecified (8.2%). The IRR for the original MPI for re-admissions within 1 month was not significant for any risk group (Table 2). The IRR for the original MPI for re-admissions within there or six months was significant for the moderate risk group compared to the mild risk group but not compared to the severe risk group (Table 2).
Amongst the 20 (2.9%) patients who had a fall in-hospital, 19 (2.73%) were single fallers and one1 (0.14%) was a recurrent faller. The IRR for the MPI was not associated with number of in-hospital falls (Table 2).
4. Discussion
In this study of medical in-patients aged ≥65 years we demonstrated that the original MPI in a geographically different patient population showed inferior discrimination to that of the original derivation and validation study for 12-month mortality [9]. A relatively low discrimination was also observed with secondary outcomes (one-, three-, six-month all-cause mortality, delirium, and number of re-admissions within one month). However, in-hospital all-cause mortality showed similar discrimination to that observed in the original MPI derivation study [9]. Adaptations to the MPI with SPMSQ and number of medications domains substituted with ARS and RUDAS scores did not significantly change discrimination for 12-month all-cause mortality.
For our FMC hospital cohort, the predictive performance of 12-month all-cause mortality for the MPI was relatively lower compared to other validation studies [11,16,18,24,25]. These studies were similar in design to the original MPI derivation study [9]. However, caution is required when interpreting the results of those studies as three studies had a small sample size, between 134–262 patients [11,24,25], and all studies were conducted in patient populations with specific medical conditions (CAP [11], dementia [25], TIA [18], and oncology patients [24] with higher overall mortality risk. Although most of the clinical and demographic characteristics in our cohort were similar to those in Pilotto’s cohort [9], some differences were also identified. For example, in our study cohort a greater proportion of patients were allocated into the moderate risk group than in Pilotto’s cohort. Furthermore, for low and moderate risk patients in the FMC cohort, higher mortality rates were seen for six- and 12-month all-cause mortality when compared to Pilotto’s cohort. Additionally, the original MPI in our study was characterized by higher scores of the CIRS components and a greater number of medications when compared to Pilotto’s cohort.
An arising concern in geriatric patients is the increasing evidence that certain medications, in particular anticholinergics, with specific pharmacological effects might more strongly predict physical and cognitive decline and mortality in older adults than the total number of drugs [49,50]. Therefore, the MPI was also adapted in this study by substituting the number of drugs with the ARS score [39]. In addition, the cognitive screen test (SPMSQ) in the MPI was substituted with the RUDAS which is a frontal lobe assessment tool, suitable for a multicultural population [46]. Although the adapted MPI was associated with 12-month mortality, the diagnostic accuracy was not significantly different to that of the original MPI.
The original MPI was also associated with one- , three-, and six-month all-cause mortality and the discrimination for six-month all-cause mortality was similar to that for 12-month all-cause mortality. Discrimination for one- and three-month all-cause mortality was slightly higher and discrimination for one-month mortality was similar to the original MPI for similar patient population studies [10,11,18,25]. Again, these other studies were small sample size (ranging from 134 to 654 patients) and all studies were conducted in patient populations with specific medical conditions (GI bleed [10], CAP [11], dementia [25], and TIA patients [18]).
The original MPI was also associated with in-hospital all-cause mortality and the discrimination was similar to other studies [21,26]. At present, no study has assessed the performance of the original MPI in predicting in-hospital falls and delirium and we observed no association within this study. However, the study was not specifically powered for these two outcomes and there were only a relatively small number of these events that occurred.
There was a significant association between the original MPI and LOS with patients in the higher MPI categories having an increased length of stay. The mean LOS for our cohort was shorter within each MPI category when compared to other validation studies [21,26]. These findings agree with that of another study in which the original MPI performance for LOS was similar to that for 12-month all-cause mortality when LOS was treated as a binary outcome (≤10 days versus >10 days). However, the study excluded patients who died within hospital [26].
At present, there are no studies that have assessed the performance of the MPI for predicting re-admission rate for one-, three- and six-months. Within our study, only the original MPI moderate risk category was associated with the three- and six-month re-admission rates. However, our study was not specifically powered for either of these secondary outcomes.
This study has several limitations. Not all patient outcomes may have been captured since the data was obtained from a South Australia specific database and, therefore, patients that moved outside of South Australia (SA) or were admitted to a private hospital within SA or interstate may have been missed, resulting in an underestimation of deaths and potential bias in our estimates. In addition, our findings represent current practices at a single centre and may not be a true representation of other Australian populations. In particular, thresholds for FMC hospital admission could differ from the derivation study [9] with FMC potentially only admitting more severely ill patients, resulting in a greater number of patients being assigned into the moderate risk group of the MPI. Another limitation was that no information regarding ethnicity and racial differences was specifically captured in our study population.
Nevertheless, this study has its strengths. Firstly, this is a large cohort outside of Europe that provided well described data and allowed for adjustment for important confounders. Secondly, there were a number of sensitivity analyses performed with different follow-up time-points and adapted versions of the original MPI to analyse its purpose in an Australian population.
5. Conclusions
In conclusion, our study raises some concerns regarding the predictive performance of the MPI for use in an Australian population that included a heterogeneous population of older patients. In particular, the discriminative performance of the MPI for 12-month mortality was lower than that reported in the original MPI studies. Adaptation of the MPI by substituting the number of medications and the SPMSQ with the ARS and RUDAS scores did not substantially improve the performance from the original MPI. An exploratory analysis of in-hospital falls, delirium, and re-admissions suggest that the original MPI might also be of value in assessing these outcomes within future studies. Larger prospective multi-centre studies with similar patient populations are now required to confirm our findings before implementing the use of the MPI into routine clinical practice within Australia.
Supplementary Materials
The following are available online at https://www.mdpi.com/2077-0383/8/11/1820/s1, Figure S1. Survival curve for MPI risk categories; Figure S2. Unadjusted and Adjusted ROC curves for original MPI and 12-month all-cause mortality; Table S1. Baseline characteristics according cohort; Table S2. Unadjusted and adjusted logistic regression for original MPI, adapted MPI, and 12-month all-cause mortality; Table S3. FMC cohort hazard ratios for original MPI risk categories; Table S4. Area under the ROC curves for original and adapted MPI’s.
Author Contributions
Research conception and design: A.A.M., R.J.W.; recruitment and data acquisition: K.B.; data analysis and interpretation: K.B., M.J.S., R.J.W., A.A.M.; statistical analysis: K.B., R.J.W; drafting the manuscript: K.B., M.J.S., R.J.W., A.M.; critical revision of the manuscript: K.B., M.J.S., R.J.W., A.A.M.; All authors approval the final manuscript.
Funding
This research was supported by a PhD scholarship granted to K.B. by Flinders University.
Acknowledgments
We thank C. Horwood and P. Hakendorf for assistance in collecting death registry data and hospital coding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Global Health and Aging. Available online: https://www.who.int/ageing/publications/global_health.pdf?ua=1 (accessed on 12 February 2016).
- Begg, S.J. Health in a ‘post-transition’Australia: Adding years to life or life to years? Aust. Health Rev. 2014, 38, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Nepal, B.; Brown, L. Projection of older Australians with a history of midlife obesity and overweight 2010–2050. Obesity 2013, 21, 2579–2581. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E. A brief history of geriatrics. J. Gerontol. 2004, 59, 1132–1152. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index: A simple index of independence useful in scoring improvement in the rehabilitation of the chronically ill. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged: The index of ADL: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Guigoz, Y.; Vellas, B.; Garry, P.J. Assessing the nutritional status of the elderly: The Mini Nutritional Assessment as part of the geriatric evaluation. Nutr. Rev. 1996, 54, S59–S65. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Pilotto, A.; Ferrucci, L.; Franceschi, M.; D’Ambrosio, L.P.; Scarcelli, C.; Cascavilla, L.; Paris, F.; Placentino, G.; Seripa, D.; Dallapiccola, B. Development and validation of a multidimensional prognostic index for one-year mortality from comprehensive geriatric assessment in hospitalized older patients. Rejuv. Res. 2008, 11, 151–161. [Google Scholar] [CrossRef]
- Pilotto, A.; Addante, F.; D’Onofrio, G.; Sancarlo, D.; Ferrucci, L. The Comprehensive Geriatric Assessment and the multidimensional approach. A new look at the older patient with gastroenterological disorders. Best Pract. Res. Clin. Gastroenterol. 2009, 23, 829–837. [Google Scholar] [CrossRef] [Green Version]
- Pilotto, A.; Addante, F.; Ferrucci, L.; Leandro, G.; D’Onofrio, G.; Corritore, M.; Niro, V.; Scarcelli, C.; Dallapiccola, B.; Franceschi, M. The multidimensional prognostic index predicts short-and long-term mortality in hospitalized geriatric patients with pneumonia. J. Gerontol. 2009, 64, 880–887. [Google Scholar] [CrossRef]
- Pilotto, A.; Addante, F.; Franceschi, M.; Leandro, G.; Rengo, G.; D’ambrosio, P.; Longo, M.G.; Rengo, F.; Pellegrini, F.; Dallapiccola, B. Multidimensional Prognostic Index based on a comprehensive geriatric assessment predicts short-term mortality in older patients with heart failure. Circ. Heart Fail. 2010, 3, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Pilotto, A.; D’Onofrio, G.; Panza, F.; Copetti, M.; Cascavilla, L.; Paris, F.; Pellegrini, F.; Seripa, D.; Ferrucci, L. Treatment of late-life major depressive disorder with selective serotonin reuptake inhibitors improves the multidimensional prognostic index. J. Clin. Psychopharmacol. 2012, 32, 726–729. [Google Scholar] [CrossRef] [PubMed]
- Pilotto, A.; Ferrucci, L.; Scarcelli, C.; Niro, V.; Di Mario, F.; Seripa, D.; Andriulli, A.; Leandro, G.; Franceschi, M. Usefulness of the comprehensive geriatric assessment in older patients with upper gastrointestinal bleeding: A two-year follow-up study. Dig. Dis. 2007, 25, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Pilotto, A.; Rengo, F.; Marchionni, N.; Sancarlo, D.; Fontana, A.; Panza, F.; Ferrucci, L.; FIRI-SIGG Study Group. Comparing the prognostic accuracy for all-cause mortality of frailty instruments: A multicentre 1-year follow-up in hospitalized older patients. PLoS ONE 2012, 7, e29090. [Google Scholar] [CrossRef] [PubMed]
- Fontana, L.; Addante, F.; Copetti, M.; Paroni, G.; Fontana, A.; Sancarlo, D.; Pellegrini, F.; Ferrucci, L.; Pilotto, A. Identification of a metabolic signature for multidimensional impairment and mortality risk in hospitalized older patients. Aging Cell 2013, 12, 459–466. [Google Scholar] [CrossRef]
- Sancarlo, D.; D’Onofrio, G.; Franceschi, M.; Scarcelli, C.; Niro, V.; Addante, F.; Copetti, M.; Ferrucci, L.; Fontana, L.; Pilotto, A. Validation of a Modified-Multidimensional Prognostic Index (m-MPI) including the Mini Nutritional Assessment Short-Form (MNA-SF) for the prediction of one-year mortality in hospitalized elderly patients. J. Nutr. Health Aging 2011, 15, 169–173. [Google Scholar] [CrossRef]
- Sancarlo, D.; Pilotto, A.; Panza, F.; Copetti, M.; Longo, M.G.; D’Ambrosio, P.; D’Onofrio, G.; Ferrucci, L.; Pilotto, A. A Multidimensional Prognostic Index (MPI) based on a comprehensive geriatric assessment predicts short-and long-term all-cause mortality in older hospitalized patients with transient ischemic attack. J. Neurol. 2012, 259, 670–678. [Google Scholar] [CrossRef]
- Pilotto, A.; Sancarlo, D.; Aucella, F.; Fontana, A.; Addante, F.; Copetti, M.; Panza, F.; Strippoli, G.F.; Ferrucci, L. Addition of the multidimensional prognostic index to the estimated glomerular filtration rate improves prediction of long-term all-cause mortality in older patients with chronic kidney disease. Rejuv. Res. 2012, 15, 82–88. [Google Scholar] [CrossRef]
- Pilotto, A.; Gallina, P.; Fontana, A.; Sancarlo, D.; Bazzano, S.; Copetti, M.; Maggi, S.; Paroni, G.; Marcato, F.; Pellegrini, F. Development and validation of a Multidimensional Prognostic Index for mortality based on a standardized Multidimensional Assessment Schedule (MPI-SVaMA) in community-dwelling older subjects. J. Am. Med. Dir. Assoc. 2013, 14, 287–292. [Google Scholar] [CrossRef]
- Volpato, S.; Bazzano, S.; Fontana, A.; Ferrucci, L.; Pilotto, A. Multidimensional prognostic index predicts mortality and length of stay during hospitalization in the older patients: A multicenter prospective study. J. Gerontol. 2014, 70, 325–331. [Google Scholar] [CrossRef]
- Brunello, A.; Fontana, A.; Zafferri, V.; Panza, F.; Fiduccia, P.; Basso, U.; Copetti, M.; Lonardi, S.; Roma, A.; Falci, C. Development of an oncological-multidimensional prognostic index (Onco-MPI) for mortality prediction in older cancer patients. J. Cancer Res. Clin. Oncol. 2016, 142, 1069–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Onofrio, G.; Sancarlo, D.; Addante, F.; Ciccone, F.; Cascavilla, L.; Paris, F.; Elia, A.C.; Nuzzaci, C.; Picoco, M.; Greco, A. A pilot randomized controlled trial evaluating an integrated treatment of rivastigmine transdermal patch and cognitive stimulation in patients with Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2015, 30, 965–975. [Google Scholar] [CrossRef] [PubMed]
- Giantin, V.; Valentini, E.; Iasevoli, M.; Falci, C.; Siviero, P.; De Luca, E.; Maggi, S.; Martella, B.; Orrù, G.; Crepaldi, G. Does the Multidimensional Prognostic Index (MPI), based on a Comprehensive Geriatric Assessment (CGA), predict mortality in cancer patients? Results of a prospective observational trial. J. Geriatr. Oncol. 2013, 4, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Pilotto, A.; Sancarlo, D.; Panza, F.; Paris, F.; D’Onofrio, G.; Cascavilla, L.; Addante, F.; Seripa, D.; Solfrizzi, V.; Dallapiccola, B. The Multidimensional Prognostic Index (MPI), based on a comprehensive geriatric assessment predicts short-and long-term mortality in hospitalized older patients with dementia. J. Alzheimers Dis. 2009, 18, 191–199. [Google Scholar] [CrossRef]
- Pilotto, A.; Sancarlo, D.; Pellegrini, F.; Rengo, F.; Marchionni, N.; Volpato, S.; Ferrucci, L. The Multidimensional Prognostic Index predicts in-hospital length of stay in older patients: A multicentre prospective study. Age Ageing 2016, 45, 90–96. [Google Scholar] [CrossRef]
- Pilotto, A.; Gallina, P.; Panza, F.; Copetti, M.; Cella, A.; Cruz-Jentoft, A.; Daragjati, J.; Ferrucci, L.; Maggi, S.; Mattace-Raso, F. Relation of statin use and mortality in community-dwelling frail older patients with coronary artery disease. Am. J. Cardiol. 2016, 118, 1624–1630. [Google Scholar] [CrossRef]
- Pilotto, A.; Gallina, P.; Copetti, M.; Pilotto, A.; Marcato, F.; Mello, A.M.; Simonato, M.; Logroscino, G.; Padovani, A.; Ferrucci, L. Warfarin Treatment and All-Cause Mortality in Community-Dwelling Older Adults with Atrial Fibrillation: A Retrospective Observational Study. J. Am. Geriatr. Soc. 2016, 64, 1416–1424. [Google Scholar] [CrossRef]
- Pilotto, A.; Panza, F.; Copetti, M.; Simonato, M.; Sancarlo, D.; Gallina, P.; Strandberg, T.; MPI_AGE Project Investigators. Statin treatment and mortality in community-dwelling frail older patients with diabetes mellitus: A retrospective observational study. PLoS ONE 2015, 10, e0130946. [Google Scholar] [CrossRef]
- Pilotto, A.; Giancristofaro, R.A.; Panza, F.; Daragjati, J.; Prete, C.; Polidori, M.; Cella, A.; Maggi, S. Role of anti-dementia drugs and multidimensional impairment on mortality rates in frail multimorbid older patients with dementia: Results from the European MPI_AGE project. Eur. Geriatr. Med. 2015, 6, S20. [Google Scholar] [CrossRef]
- Bureau, M.-L.; Liuu, E.; Christiaens, L.; Pilotto, A.; Mergy, J.; Bellarbre, F.; Ingrand, P.; Paccalin, M.; Cruz-Jentoft, A.; Maggi, S. Using a multidimensional prognostic index (MPI) based on comprehensive geriatric assessment (CGA) to predict mortality in elderly undergoing transcatheter aortic valve implantation. Int. J. Cardiol. 2017, 236, 381–386. [Google Scholar] [CrossRef]
- Angleman, S.B.; Santoni, G.; Pilotto, A.; Fratiglioni, L.; Welmer, A.-K.; MPI_AGE Project Investigators. Multidimensional prognostic index in association with future mortality and number of hospital days in a population-based sample of older adults: Results of the EU funded MPI_AGE project. PLoS ONE 2015, 10, e0133789. [Google Scholar] [CrossRef] [PubMed]
- Routledge, P.A.; O’mahony, M.; Woodhouse, K. Adverse drug reactions in elderly patients. Br. J. Clin. Pharm. 2004, 57, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Brahma, D.K.; Wahlang, J.B.; Marak, M.D.; Sangma, M.C. Adverse drug reactions in the elderly. J. Pharm. Pharm. 2013, 4, 91. [Google Scholar] [CrossRef]
- Hilmer, S.N.; Mager, D.E.; Simonsick, E.M.; Cao, Y.; Ling, S.M.; Windham, B.G.; Harris, T.B.; Hanlon, J.T.; Rubin, S.M.; Shorr, R.I. A drug burden index to define the functional burden of medications in older people. Arch. Intern. Med. 2007, 167, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Mangoni, A.A.; van Munster, B.C.; Woodman, R.J.; de Rooij, S.E. Measures of anticholinergic drug exposure, serum anticholinergic activity, and all-cause postdischarge mortality in older hospitalized patients with hip fractures. Am. J. Geriatr. Psychiatry 2013, 21, 785–793. [Google Scholar] [CrossRef] [PubMed]
- Lowry, E.; Woodman, R.J.; Soiza, R.L.; Hilmer, S.N.; Mangoni, A.A. Drug burden index, physical function, and adverse outcomes in older hospitalized patients. J. Clin. Pharmacol. 2012, 52, 1584–1591. [Google Scholar] [CrossRef]
- Lowry, E.; Woodman, R.J.; Soiza, R.L.; Mangoni, A.A. Associations between the anticholinergic risk scale score and physical function: Potential implications for adverse outcomes in older hospitalized patients. J. Am. Med. Dir. Assoc. 2011, 12, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, J.L.; Salow, M.J.; Angelini, M.C.; McGlinchey, R.E. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch. Intern. Med. 2008, 168, 508–513. [Google Scholar] [CrossRef]
- Basic, D.; Khoo, A.; Conforti, D.; Rowland, J.; Vrantsidis, F.; LoGiudice, D.; Hill, K.; Harry, J.; Lucero, K.; Prowse, R. Rowland Universal Dementia Assessment Scale, Mini-Mental State Examination and General Practitioner Assessment of Cognition in a multicultural cohort of community-dwelling older persons with early dementia. Aust. Psychol. 2009, 44, 40–53. [Google Scholar] [CrossRef]
- Lawton, M.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Nurs. Res. 1970, 19, 278. [Google Scholar] [CrossRef]
- Pfeiffer, E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Bliss, M.R.; McLaren, R.; Exton-Smith, A.N. Mattresses for preventing pressure sores in geriatric patients. Mon. Bull. Minist. Health Public Health Lab. Serv. 1966, 25, 238. [Google Scholar] [PubMed]
- Linn, B.S.; Linn, M.W.; Gurel, L. Cumulative illness rating scale. J. Am. Geriatr. Soc. 1968, 16, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Guigoz, Y. Mini Nutritional Assessment: A practical assessment tool for grading the nutritional state of elderly patients. Facts Res. Geyontol. 1994, 4, 15–59. [Google Scholar]
- Storey, J.E.; Rowland, J.T.; Conforti, D.A.; Dickson, H.G. The Rowland universal dementia assessment scale (RUDAS): A multicultural cognitive assessment scale. Int. Psychogeriatr. 2004, 16, 13–31. [Google Scholar] [CrossRef]
- Casey, P.; Cross, W.; Mart, M.W.S.; Baldwin, C.; Riddell, K.; Dārziņš, P. Hospital discharge data under-reports delirium occurrence: Results from a point prevalence survey of delirium in a major Australian health service. Intern. Med. J. 2019, 49, 338–344. [Google Scholar] [CrossRef]
- Veronese, N.; Siri, G.; Cella, A.; Daragjati, J.; Cruz-Jentoft, A.J.; Polidori, M.C.; Mattace-Raso, F.; Paccalin, M.; Topinkova, E.; Greco, A. Older women are frailer, but less often die then men: A prospective study of older hospitalized people. Maturitas 2019, 128, 81–86. [Google Scholar] [CrossRef]
- Bostock, C.V.; Soiza, R.L.; Mangoni, A.A. Association between prescribing of antimuscarinic drugs and antimuscarinic adverse effects in older people. Expert Rev. Clin. Pharm. 2010, 3, 441–452. [Google Scholar] [CrossRef]
- Ruxton, K.; Woodman, R.J.; Mangoni, A.A. Drugs with anticholinergic effects and cognitive impairment, falls and all-cause mortality in older adults: A systematic review and meta-analysis. Br. J. Clin. Pharm. 2015, 80, 209–220. [Google Scholar] [CrossRef]
Figure 1.
Unadjusted and adjusted ROC curves for original MPI and 12-month all-cause mortality.

{kind=link}
Table 1.
Patient characteristics according to MPI category.
| Mild Risk | Moderate Risk | Severe Risk | p-Value | |
|---|---|---|---|---|
| Characteristics | 0.0–0.33 | 0.34–0.66 | 0.67–1.0 | |
| Patients, n (%) | 229 (32.86) | 409 (58.68) | 59 (8.46) | |
| Women | 92 (40.17) | 220 (53.79) | 37 (62.71) | <0.001 |
| Men | 137 (59.83) | 189 (46.21) | 22 (37.29) | |
| MPI score | ||||
| Score range | 0.063–0.313 | 0.375–0.625 | 0.688–0.875 | |
| Median (IQR) | 0.250 (0.250–0.313) | 0.438 (0.438–0.500) | 0.688 (0.688–0.750) | |
| Age | ||||
| Range | 65–96 | 65–101 | 67–102 | |
| Median (IQR) | 75 (70–82) | 82 (74–87) | 86 (80–92) | <0.001 |
| Fall, n (%) | 4 (1.75) | 11 (2.69) | 5 (8.47) | 0.021 |
| Delirium, n (%) | 14 (6.11) | 34 (8.31) | 19 (32.20) | <0.001 |
| LOS (days), median (IQR) | 5 (3–8) | 6 (4–11) | 11 (5–18) | 0.001 |
| Mortality, n (%) | ||||
| In-hospital | 1 (0.44) | 16 (3.91) | 8 (13.56) | <0.001 |
| 1-month | 3 (1.31) | 20 (4.89) | 12 (20.34) | <0.001 |
| 3-month | 7 (3.06) | 42 (10.27) | 16 (27.12) | <0.001 |
| 6-month | 22 (9.61) | 95 (23.23) | 20 (33.90) | <0.001 |
| 12-month | 38 (16.59) | 136 (33.25) | 27 (45.76) | <0.001 |
| Re-admission rate, % | ||||
| 1-month | 11.35 | 15.65 | 8.47 | 0.157 |
| 3-month | 23.58 | 33.25 | 27.12 | 0.022 |
| 6-month | 35.37 | 45.72 | 38.98 | 0.008 |
Abbreviations: IQR: Interquartile range; LOS: length of stay; n: number. Kruskal–Wallis H test: age, gender, and LOS; Chi2 test: in-hospital mortality, 1-, 3-, 6-, and 12-month mortality, falls, delirium, re-admissions at 1, 3 and 6 months.
Table 2.
FMC cohort and secondary outcomes for MPI risk categories.
| Unadjusted OR | Adjusted OR * | |||||
|---|---|---|---|---|---|---|
| Variable | ||||||
| Six-month mortality | ||||||
| Mild | Reference group | |||||
| Moderate | 2.85 | 1.73–4.67 | <0.0001 | 2.92 | 1.75–4.87 | <0.0001 |
| Severe | 4.83 | 2.41–9.67 | <0.0001 | 4.88 | 2.34–10.20 | <0.0001 |
| Three-month mortality | ||||||
| Mild | Reference group | |||||
| Moderate | 3.63 | 1.60–8.22 | 0.002 | 3.56 | 1.55–8.20 | 0.003 |
| Severe | 11.80 | 4.58–30.40 | <0.0001 | 11.20 | 4.14–30.32 | <0.0001 |
| One-month mortality | ||||||
| Mild | Reference group | |||||
| Moderate | 3.87 | 1.14–13.18 | 0.030 | 3.91 | 1.13–13.55 | 0.031 |
| Severe | 19.23 | 5.22–70.83 | <0.0001 | 19.43 | 4.96–76.06 | <0.0001 |
| In-hospital mortality | ||||||
| Mild | Reference group | |||||
| Moderate | 9.28 | 1.22–70.46 | 0.031 | 9.19 | 1.19–70.74 | 0.033 |
| Severe | 35.76 | 4.38–292.33 | 0.001 | 34.46 | 4.02–295.78 | 0.001 |
| In-hospital delirium | ||||||
| Mild | Reference group | |||||
| Moderate | 1.39 | 0.73–2.65 | 0.314 | 1.21 | 0.62–2.37 | 0.573 |
| Severe | 7.29 | 3.38–15.73 | <0.0001 | 5.68 | 2.48–13.01 | <0.0001 |
| Unadjusted IRR | Adjusted IRR * | |||||
| IRR | 95% CI | p-value | IRR | 95% CI | p-value | |
| Re-admission rate, one month | ||||||
| Mild | Reference group | |||||
| Moderate | 1.29 | 0.86–1.94 | 0.223 | 1.31 | 0.86–2.00 | 0.215 |
| Severe | 0.59 | 0.23–1.51 | 0.269 | 0.60 | 0.23–1.58 | 0.304 |
| Re-admission rate, three months | ||||||
| Mild | Reference group | |||||
| Moderate | 1.46 | 1.14–1.88 | 0.003 | 1.52 | 1.17–1.97 | 0.002 |
| Severe | 0.88 | 0.53–1.44 | 0.608 | 0.95 | 0.57–1.59 | 0.844 |
| Re-admission rate, six months | ||||||
| Mild | Reference group | |||||
| Moderate | 1.59 | 1.31–1.93 | <0.0001 | 1.69 | 1.39–2.07 | <0.0001 |
| Severe | 1.04 | 0.72–1.50 | 0.830 | 1.18 | 0.81–1.72 | 0.379 |
| In-hospital falls | ||||||
| Mild | Reference group | |||||
| Moderate | 1.24 | 0.40–3.85 | 0.706 | 1.04 | 0.32–3.33 | 0.949 |
| Severe | 2.24 | 0.56–8.95 | 0.254 | 1.69 | 0.40–7.18 | 0.478 |
Abbreviations: IRR: Incidence rate ratio; CI: confidence interval; MPI: Multidimensional Prognostic Index; OR: Odds ratio. Note: * adjusted for age and gender.
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Bryant, K.; Sorich, M.J.; Woodman, R.J.; Mangoni, A.A. Validation and Adaptation of the Multidimensional Prognostic Index in an Older Australian Cohort. J. Clin. Med. 2019, 8, 1820. https://doi.org/10.3390/jcm8111820
AMA Style
Bryant K, Sorich MJ, Woodman RJ, Mangoni AA. Validation and Adaptation of the Multidimensional Prognostic Index in an Older Australian Cohort. Journal of Clinical Medicine. 2019; 8(11):1820. https://doi.org/10.3390/jcm8111820
Chicago/Turabian StyleBryant, Kimberley, Michael J. Sorich, Richard J. Woodman, and Arduino A. Mangoni. 2019. "Validation and Adaptation of the Multidimensional Prognostic Index in an Older Australian Cohort" Journal of Clinical Medicine 8, no. 11: 1820. https://doi.org/10.3390/jcm8111820
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.