Body Composition Changes Following a Concurrent Exercise Intervention in Perimenopausal Women: The FLAMENCO Project Randomized Controlled Trial

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
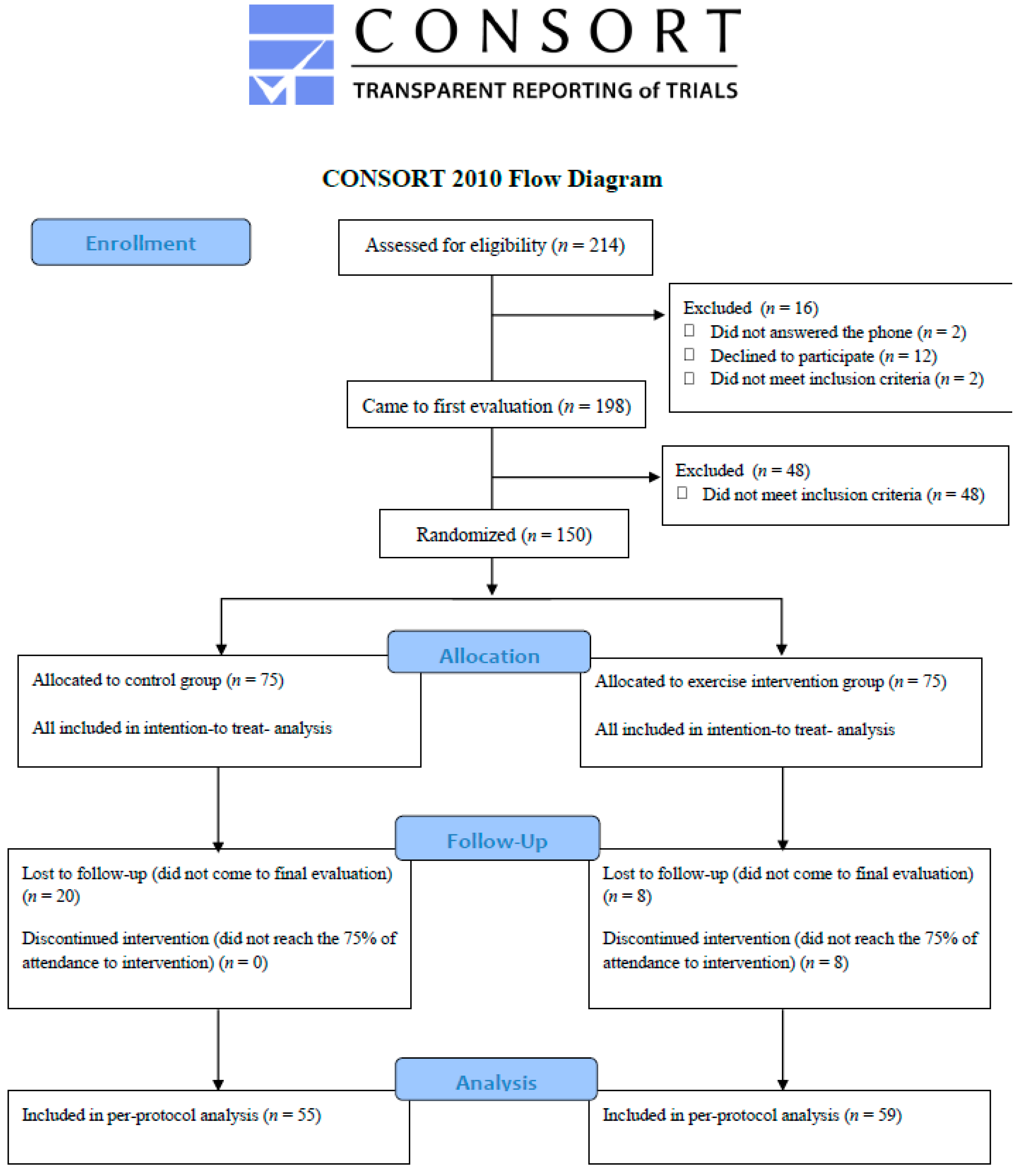
2.1. Participants
2.2. Randomization
2.3. Procedures
2.4. Exercise Intervention
2.5. Control Group
2.6. Outcomes
2.6.1. Anthropometry and Body Composition
2.6.2. Pharmaceutical Costs
2.6.3. Physical Activity Levels
2.6.4. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Mandrup, C.M.; Egelund, J.; Nyberg, M.; Slingsby, M.H.L.; Andersen, C.; Løgstrup, S.; Bangsbo, J.; Suetta, C.; Stallknecht, B.; Hellsten, Y. Effects of high-intensity training on cardiovascular risk factors in pre- and postmenopausal women. Am. J. Obstet. Gynecol. 2016, 216, 384.e1–384.e11. [Google Scholar]
- Seifert-Klauss, V.; Fillenberg, S.; Schneider, H.; Luppa, P.; Mueller, D.; Kiechle, M. Bone loss in premenopausal, perimenopausal and postmenopausal women: Results of a prospective observational study over 9 years. Climacteric 2012, 15, 433–440. [Google Scholar] [CrossRef]
- Ramezani Tehrani, F.; Behboudi-Gandevani, S.; Ghanbarian, A.; Azizi, F. Effect of menopause on cardiovascular disease and its risk factors: A 9-year follow-up study. Climacteric 2014, 17, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Després, J.-P. Abdominal obesity: The most prevalent cause of the metabolic syndrome and related cardiometabolic risk. Eur. Heart J. Suppl. 2006, 8, B4–B12. [Google Scholar] [CrossRef]
- Ervin, R.B. Prevalence of metabolic syndrome among adults 20 years of age and over, by sex, age, race and ethnicity, and body mass index: United States, 2003–2006. Natl. Health Stat. Report. 2009, 5, 1–7. [Google Scholar]
- Gadelha, A.B.; Myers, J.; Moreira, S.; Dutra, M.T.; Safons, M.P.; Lima, R.M. Comparison of adiposity indices and cut-off values in the prediction of metabolic syndrome in postmenopausal women. Diabetes Metab. Syndr. 2016, 10, 143–148. [Google Scholar] [CrossRef]
- Heidari, B.; Hosseini, R.; Javadian, Y.; Bijani, A.; Sateri, M.H.; Nouroddini, H.G. Factors affecting bone mineral density in postmenopausal women. Arch. Osteoporos. 2015, 10, 10–15. [Google Scholar] [CrossRef]
- Ahlborg, H.G.; Johnell, O.; Turner, C.H.; Rannevik, G.; Karlsson, M.K. Bone Loss and Bone Size after Menopause. N. Engl. J. Med. 2003, 349, 327–334. [Google Scholar] [CrossRef]
- Lorentzon, M.; Cummings, S.R. Osteoporosis: The evolution of a diagnosis. J. Intern. Med. 2015, 277, 650–661. [Google Scholar] [CrossRef]
- Maillard, F.; Rousset, S.; Pereira, B.; Traore, A.; de Pradel Del Amaze, P.; Boirie, Y.; Duclos, M.; Boisseau, N. High-intensity interval training reduces abdominal fat mass in postmenopausal women with type 2 diabetes. Diabetes Metab. 2016, 42, 433–441. [Google Scholar] [CrossRef]
- Arsenault, B.J.; Côté, M.; Cartier, A.; Lemieux, I.; Després, J.-P.; Ross, R.; Earnest, C.P.; Blair, S.N.; Church, T.S. Effect of exercise training on cardiometabolic risk markers among sedentary, but metabolically healthy overweight or obese post-menopausal women with elevated blood pressure. Atherosclerosis 2009, 207, 530–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Blasio, A.; Ripari, P.; Bucci, I.; Di Donato, F.; Izzicupo, P.; D’Angelo, E.; Di Nenno, B.; Taglieri, M.; Napolitano, G. Walking training in postmenopause: Effects on both spontaneous physical activity and training-induced body adaptations. Menopause 2012, 19, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Houston, M.C.; Fazio, S.; Chilton, F.H.; Wise, D.E.; Jones, K.B.; Barringer, T.A.; Bramlet, D.A. Nonpharmacologic Treatment of Dyslipidemia. Prog. Cardiovasc. Dis. 2009, 52, 61–94. [Google Scholar] [CrossRef] [PubMed]
- Grossman, J.A.C.; Payne, E.K. A randomized comparison study regarding the impact of short-duration, high-intensity exercise and traditional exercise on anthropometric and body composition measurement changes in post-menopausal women—A pilot study. Post Reprod. Health 2016, 22, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, M. [Role of physical activity in the prevention of osteoporosis]. Med. Monatsschr. Pharm. 2008, 31, 259–264. [Google Scholar] [PubMed]
- Aparicio, V.A.; Ruiz-Cabello, P.; Borges-Cosic, M.; Andrade, A.; Coll-Risco, I.; Acosta-Manzano, P.; Soriano-Maldonado, A. Association of physical fitness, body composition, cardiometabolic markers and adherence to the Mediterranean diet with bone mineral density in perimenopausal women. The FLAMENCO project. J. Sports Sci. 2016, 35, 880–887. [Google Scholar] [CrossRef]
- Zhao, R.; Zhao, M.; Xu, Z. The effects of differing resistance training modes on the preservation of bone mineral density in postmenopausal women: A meta-analysis. Osteoporos. Int. 2015, 26, 1605–1618. [Google Scholar] [CrossRef]
- Heinonen, A.; Oja, P.; Sievänen, H.; Pasanen, M.; Vuori, I. Effect of Two Training Regimens on Bone Mineral Density in Healthy Perimenopausal Women: A Randomized Controlled Trial. J. Bone Miner. Res. 1998, 13, 483–490. [Google Scholar] [CrossRef]
- Wen, H.J.; Huang, T.H.; Li, T.L.; Chong, P.N.; Ang, B.S. Effects of short-term step aerobics exercise on bone metabolism and functional fitness in postmenopausal women with low bone mass. Osteoporos. Int. 2017, 28, 539–547. [Google Scholar] [CrossRef]
- Kjerulff, K.H.; Frick, K.D.; Rhoades, J.A.; Hollenbeak, C.S. The cost of being a woman. A National Study of Health Care Utilization and Expenditures for Female-Specific Conditions. Women Health Issues 2007, 17, 13–21. [Google Scholar] [CrossRef]
- Kleinman, N.L.; Rohrbacker, N.J.; Bushmakin, A.G.; Whiteley, J.; Lynch, W.D.; Shah, S.N. Direct and indirect costs of women diagnosed with menopause symptoms. J. Occup. Environ. Med. 2013, 55, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Carbonell-Baeza, A.; Soriano-Maldonado, A.; Gallo, F.J.; López del Amo, M.P.; Ruiz-Cabello, P.; Andrade, A.; Borges-Cosic, M.; Peces-Rama, A.R.; Spacírová, Z.; Álvarez-Gallardo, I.C.; et al. Cost-effectiveness of an exercise intervention program in perimenopausal women: The Fitness League Against MENopause COst (FLAMENCO) randomized controlled trial. BMC Public Health 2015, 15, 555. [Google Scholar] [CrossRef] [PubMed]
- Špacírová, Z.; Epstein, D.; Mochón, L.G.; Aparicio, V.A.; Borges, M.; Ruiz-cabello, P.; López, M.P.; Martín, J.J.M. Cost-effectiveness of a primary care-based exercise interventionin perimenopausal women. The Flamenco Project. Gac. Sanit. 2018. [Google Scholar] [CrossRef]
- Mataix, J.; Martinez de Victoria, E.; Montellano, M.; Lopez, M.; Aranda, P.; Lopez, M. Valoración del Estado Nutricional de la Comunidad Autónoma de Andalucía; Junta de Andalucía, Consejeria de Salud: Sevilla, Spain, 2000.
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary patterns: A Mediterranean diet score and its relation to clinical and biological markers of cardiovascular disease risk. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 559–568. [Google Scholar] [CrossRef]
- Kupperman, H.S.; Blatt, M.H.G.; Wiesbader, H.; Filler, W. Comparative clinical evaluation of estrogenic preparations by the menopausal and amenorrheal indices. J. Clin. Endocrinol. Metab. 1953, 13, 688–703. [Google Scholar] [CrossRef]
- Balady, G.J.; Arena, R.; Sietsema, K.; Myers, J.; Coke, L.; Fletcher, G.F.; Forman, D.; Franklin, B.; Guazzi, M.; Gulati, M.; et al. Clinician’s Guide to Cardiopulmonary Exercise Testing in Adults: A Scientific Statement From the American Heart Association. Circulation 2010, 122, 191–225. [Google Scholar] [CrossRef]
- Bruce, R.A.; Kusumi, F.; Hosmer, D. Maximal oxygen intake and nomographic assessment of functional aerobic impairment in cardiovascular disease. Am. Heart J. 1973, 85, 546–562. [Google Scholar] [CrossRef]
- Rikli, R.; Jones, C. Development and validation of a functional fitness test for community-residing older adults. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef]
- Ruiz-Ruiz, J.; Mesa, J.L.M.; Gutiérrez, A.; Castillo, M.J. Hand size influences optimal grip span in women but not in men. J. Hand Surg. 2002, 27, 897–901. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, B. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2013; ISBN 978-1-60913-605-5. [Google Scholar]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci Sport. Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Diraya—Servicio Andaluz de Salud. Available online: http://www.juntadeandalucia.es/servicioandaluzdesalud/principal/documentosacc.asp?pagina=pr_diraya (accessed on 17 October 2017).
- Goran, M.I.; Poehlman, E.T. Endurance training does not enhance total energy expenditure in healthy elderly persons. Am. J. Physiol. 1992, 263, E950–E957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouchonville, M.; Armamento-Villareal, R.; Shah, K.; Napoli, N.; Sinacore, D.R.; Qualls, C.; Villareal, D.T. Weight loss, exercise or both and cardiometabolic risk factors in obese older adults: Results of a randomized controlled trial. Int. J. Obes. 2014, 38, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Abbenhardt, C.; Mctiernan, A.; Alfano, C.M.; Wener, M.H.; Campbell, K.L.; Duggan, C.; Foster-Schubert, K.E.; Kong, A.; Toriola, A.T.; Potter, J.D.; et al. Effects of individual and combined dietary weight loss and exercise interventions in postmenopausal women on adiponectin and leptin levels. J. Intern. Med. 2013, 274, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Foster-Schubert, K.E.; Alfano, C.M.; Duggan, C.R.; Xiao, L.; Campbell, K.L.; Kong, A.; Bain, C.E.; Wang, C.-Y.; Blackburn, G.L.; McTiernan, A. Effect of Diet and Exercise, Alone or Combined, on Weight and Body Composition in Overweight-to-Obese Postmenopausal Women. Obesity 2012, 20, 1628–1638. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Sui, X.; Lavie, C.J.; Blair, S.N. Body Mass Index, the Most Widely Used But Also Widely Criticized Index: Would a Criterion Standard Measure of Total Body Fat Be a Better Predictor of Cardiovascular Disease Mortality? Mayo Clin. Proc. 2016, 91, 443–455. [Google Scholar] [CrossRef] [PubMed]
- Vogel, T.; Brechat, P.H.; Leprêtre, P.M.; Kaltenbach, G.; Berthel, M.; Lonsdorfer, J. Health benefits of physical activity in older patients: A review. Int. J. Clin. Pract. 2009, 63, 303–320. [Google Scholar] [CrossRef]
- Cheung, C.-L.; Tan, K.C.B.; Bow, C.H.; Soong, C.S.S.; Loong, C.H.N.; Kung, A.W.-C. Low handgrip strength is a predictor of osteoporotic fractures: Cross-sectional and prospective evidence from the Hong Kong Osteoporosis Study. Age (Omaha) 2012, 34, 1239–1248. [Google Scholar] [CrossRef]
- May, A.M.; Bosch, M.J.C.; Velthuis, M.J.; van der Wall, E.; Steins Bisschop, C.N.; Los, M.; Erdkamp, F.; Bloemendal, H.J.; de Roos, M.A.J.; Verhaar, M.; et al. Cost-effectiveness analysis of an 18-week exercise program for patients with breast and colon cancer undergoing adjuvant chemotherapy: The randomised PACT study. BMJ Open 2017, 7, e012187. [Google Scholar] [CrossRef]
- Moriwaki, K.; Mouri, M.; Hagino, H. Cost-effectiveness analysis of once-yearly injection of zoledronic acid for the treatment of osteoporosis in Japan. Osteoporos. Int. 2017, 28, 1939–1950. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Control Group | Exercise Group | ||
|---|---|---|---|
| Mean (SD) | Mean (SD) | p | |
| (n = 75) | (n = 75) | ||
| Age (years) | 52.7 (4.5) | 52.8 (4.5) | 0.877 |
| Height (cm) | 159.2 (5.8) | 159.7 (6.0) | 0.492 |
| Sedentary time (mins/week) | 3293.0 (525) | 3421.1 (728) | 0.344 |
| Light PA (mins/week) | 2968.6 (576) | 2962.7 (596) | 0.751 |
| Moderately vigorous PA (mins/week) | 180.8 (145.5) | 178.6 (157.2) | 0.759 |
| Women meeting PA recommendations * pre-test (%) | 54.5 | 45.5 | 0.383 |
| Mediterranean Diet score pre-test | 31.1 (5.1) | 31.1 (3.9) | 0.610 |
| Mediterranean Diet Score post-test | 33.3 (0.6) | 33.7 (0.5) | 0.403 |
| Kupperman global score (0–45) | 15.0 (10.2) | 16.7 (10.8) | 0.456 |
| Fitness at pre-test | |||
| VO2max (mL/kg/min) | 21.3 (5.3) | 19.6 (4.7) | 0.064 |
| Strength legs (repetitions) | 15.2 (2.2) | 15.5 (2.3) | 0.526 |
| Handgrip (kg) | 27.0 (4.2) | 25.8 (3.9) | 0.113 |
| Medicines/supplements | |||
| Women taking hormone treatment (thyroid) (%) | 4.0 | 2.7 | 0.620 |
| Women taking vitamin D (%) | 2.7 | 0.0 | 0.224 |
| Women taking calcium carbonate, yes (%) | 9.4 | 2.7 | 0.135 |
| Women taking zoledronic acid (%) | 2.7 | 1.3 | 0.654 |
| Baseline body composition | |||
| Weight (kg) | 70.1 (12.0) | 69.7 (12.8) | 0.616 |
| Body Mass Index (kg/m2) | 27.6 (4.2) | 27.5 (4.9) | 0.523 |
| Lean mass (kg) | 37.7 (4.8) | 37.4 (4.9) | 0.534 |
| Fat mass (kg) | 29.4 (7.6) | 29.2 (7.9) | 0.689 |
| Fat Mass Index (kg/m2) | 11.6 (2.9) | 11.3 (2.8) | 0.543 |
| Fat mass percentage, % | 42.0 (4.9) | 41.9 (4.8) | 0.862 |
| Visceral adipose tissue (kg) | 0.71 (0.3) | 0.66 (0.3) | 0.175 |
| Gynoid fat mass (kg) | 5.1 (6.3) | 5.2 (1.3) | 0.589 |
| Android fat mass (kg) | 2.5 (0.9) | 2.5 (0.9) | 0.538 |
| Total bone mineral density (g/cm2) | 1.14 (0.1) | 1.15 (0.1) | 0.329 |
| Total bone mineral content (g) | 2117.2 (286) | 2157.2 (294) | 0.297 |
| Bone mineral content of pelvis (g) | 185.8 (43.7) | 191.3 (43.6) | 0.316 |
| Bone mineral density of pelvis (g/cm2) | 1.12 (0.1) | 1.12 (0.1) | 0.829 |
| Bone mineral density of lumbar spine (g/cm2) | 0.88 (0.1) | 0.89 (0.1) | 0.831 |
| Costs of medication | |||
| Monthly pharmaceutical expenditure pre-test (€) | 20.1 (38.0) | 27.7 (54.9) | 0.245 |
| Monthly pharmaceutical expenditure post-test (€) | 32.4 (72.4) | 30.7 (90.7) | 0.299 |
| Body Composition | Control (n = 75) | Exercise (n = 75) | Between-Group Difference (95% CI) | p |
|---|---|---|---|---|
| Change from Baseline at Week 16 (SD) | Change from Baseline at Week 16 (SD) | |||
| Weight * (kg) | −0.07 (3.48) | −1.52 (6.30) | −1.45 (−3.32 to 0.39) | 0.121 |
| Body Mass Index * (kg/m2) | 0.00 (1.34) | −0.75 (1.96) | −0.75 (−1.29 to −0.22) | 0.006 |
| Lean mass * (g) | 471 (1280) | 314 (1416) | −157 (−592 to 284) | 0.489 |
| Fat mass * (g) | −544 (1081) | −903 (2159) | −359 (−903 to 175) | 0.184 |
| Fat Mass Index (kg/m2) | −0.29 (0.48) | −0.41 (0.88) | −0.13 (−0.39 to 1.30) | 0.325 |
| Fat mass percentage * (%) | −0.72 (1.24) | −0.95 (2.20) | −0.23 (−0.80 to 0.32) | 0.396 |
| Visceral adipose tissue * (g) | −21.3 (67.0) | −30.5 (88.3) | −9.2 (−37.1 to 12.1) | 0.315 |
| Gynoid fat mass * (g) | −98.3 (221) | −213 (414) | −115 (−209 to −3.86) | 0.042 |
| Android fat mass * (g) | −46.1 (152) | −139 (268) | −92.9 (−164 to −26.9) | 0.007 |
| Total bone mineral density a (g/cm2) | −0.01 (0.02) | 0.00 (0.02) | 0.01 (−0.00 to 0.02) | 0.114 |
| Total bone mineral content a (g) | −23.6 (104) | −8.65 (34.5) | 15.0 (−6.20 to 43.69) | 0.140 |
| Bone mineral content of pelvis a (g) | −2.85 (10.2) | 1.13 (11.5) | 3.98 (0.93 to 7.81) | 0.013 |
| Bone mineral density of pelvis a (g/cm2) | −0.03 (0.03) | 0.00 (0.03) | 0.03 (−0.00 to 0.02) | 0.171 |
| Bone mineral density of lumbar spine a (g/cm2) | −0.01 (0.07) | 0.00 (0,08) | 0.01 (−0.01 to 0.03) | 0.319 |
| Pharmaceutical expenditure per woman * (€/month) | 12.3 (34.4) | 2.95 (35.8) | −9.35 (−19.4 to 3.22) | 0.160 |
| Body Composition | Control (n = 55) Differences from Baseline to 16 Weeks (SD) | Exercise (n = 59) Differences from Baseline to 16 Weeks (SD) | Between-Group Difference (95% CI) | p |
|---|---|---|---|---|
| Weight * (kg) | −0.01 (3.49) | −1.69 (6.65) | −1.68 (−3.18 to 0.23) | 0.090 |
| Body Mass Index * (kg/m2) | 0.03 (1.61) | −0.91 (2.16) | −0.79 (−1.46 to −0.12) | 0.022 |
| Lean mass * (g) | 655 (1474) | 344 (1478) | −311 (−841 to 288) | 0.334 |
| Fat mass * (g) | −758 (1213) | −1063 (2257) | −305 (−984 to 426) | 0.435 |
| Fat Mass Index (kg/m2) | −0.41 (1.46) | −0.44 (1.05) | −0.08 (−4.83 to 3.21) | 0.692 |
| Fat mass percentage * (%) | −1.00 (1.37) | −1.12 (2.26) | −0.02 (−0.82 to 0.60) | 0.743 |
| Visceral adipose tissue * (g) | −29.7 (77.6) | −32.6 (92.0) | −2.9 (−37.8 to 27.6) | 0.759 |
| Gynoid fat mass * (g) | −136 (250) | −242 (435) | −106 (−213 to 55.1) | 0.245 |
| Android fat mass * (g) | −64.2 (176) | −162 (283) | −97.8 (−197 to −18.5) | 0.018 |
| Total bone mineral density (g/cm2) | −0.01 (0.02) | 0.00 (0.02) | 0.01 (0.00 to 0.01) | 0.110 |
| Total bone mineral content a (g) | −32.9 (121) | −9.38 (34.9) | 23.5 (0.38 to 69.0) | 0.048 |
| Bone mineral content of pelvis a (g) | −3.97 (11.9) | 1.51 (12.2) | 5.48 (0.67 to 9.70) | 0.025 |
| Bone mineral density of pelvis a (g/cm2) | 0.00 (0.03) | 0.01 (0.03) | 0.01 (−0.01 to 0.01) | 0.734 |
| Bone mineral density of lumbar spine a (g/cm2) | −0.01 (0.08) | 0.00 (0.08) | 0.01 (−0.01 to 0.05) | 0.200 |
| Pharmaceutical expenditure per woman * (€/month) | 13.6 (34.5) | −2.01 (28.3) | −15.7 (−27.5 to −2.77) | 0.017 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coll-Risco, I.; Acosta-Manzano, P.; Borges-Cosic, M.; Camiletti-Moiron, D.; Aranda, P.; Soriano-Maldonado, A.; Aparicio, V.A. Body Composition Changes Following a Concurrent Exercise Intervention in Perimenopausal Women: The FLAMENCO Project Randomized Controlled Trial. J. Clin. Med. 2019, 8, 1678. https://doi.org/10.3390/jcm8101678
Coll-Risco I, Acosta-Manzano P, Borges-Cosic M, Camiletti-Moiron D, Aranda P, Soriano-Maldonado A, Aparicio VA. Body Composition Changes Following a Concurrent Exercise Intervention in Perimenopausal Women: The FLAMENCO Project Randomized Controlled Trial. Journal of Clinical Medicine. 2019; 8(10):1678. https://doi.org/10.3390/jcm8101678
Chicago/Turabian StyleColl-Risco, Irene, Pedro Acosta-Manzano, Milkana Borges-Cosic, Daniel Camiletti-Moiron, Pilar Aranda, Alberto Soriano-Maldonado, and Virginia A. Aparicio. 2019. "Body Composition Changes Following a Concurrent Exercise Intervention in Perimenopausal Women: The FLAMENCO Project Randomized Controlled Trial" Journal of Clinical Medicine 8, no. 10: 1678. https://doi.org/10.3390/jcm8101678