Human Soluble Recombinant Thrombomodulin, ART-123, Resolved Early Phase Coagulopathies, but Did Not Significantly Alter the 28 Day Outcome in the Treatment of DIC Associated with Infectious Systemic Inflammatory Response Syndromes


Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Guidelines
2.2. Subjects
2.3. Treatment Assignments
2.4. Evaluation of Patients
2.5. Statistics
3. Results
3.1. Baseline Characteristics
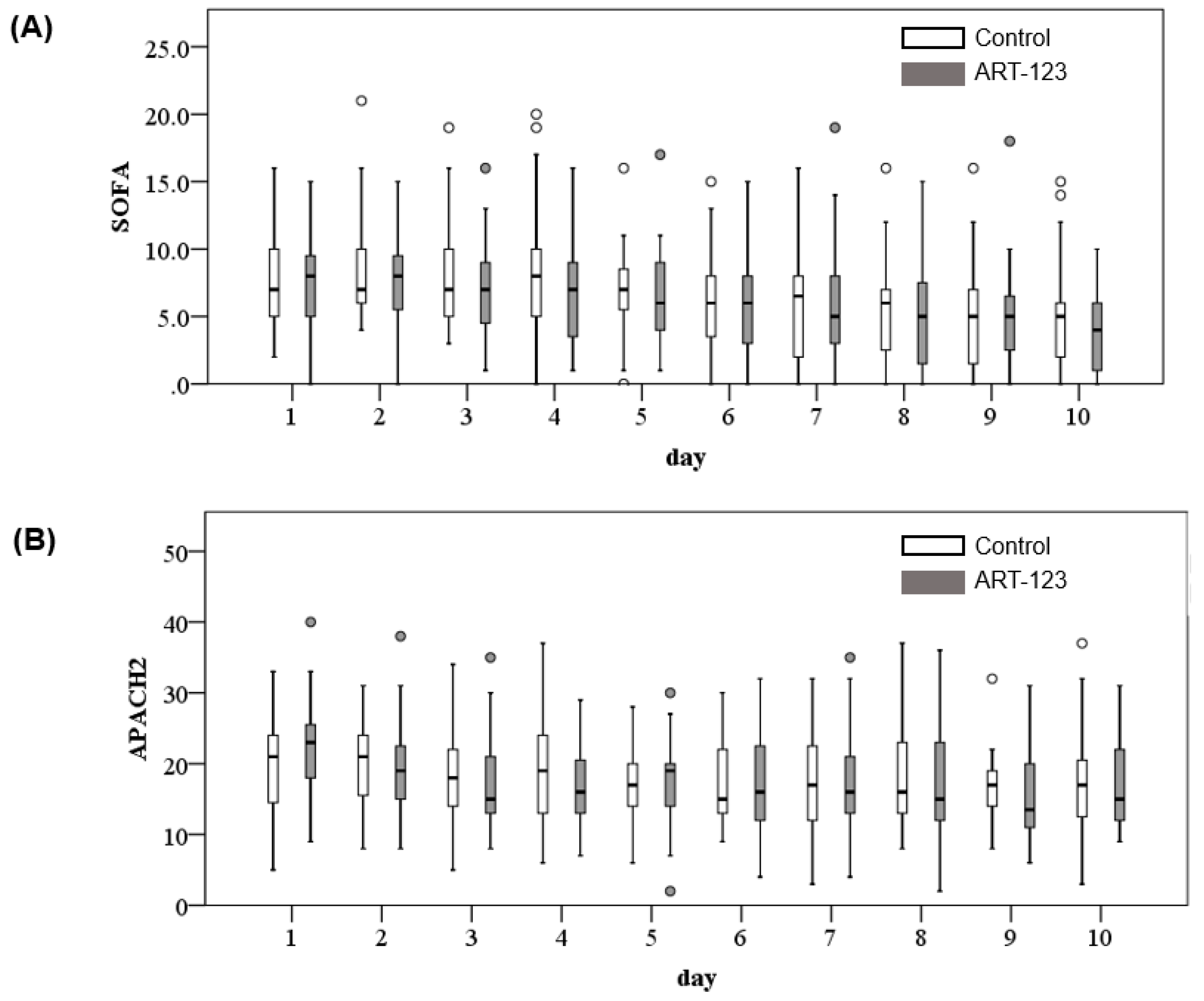
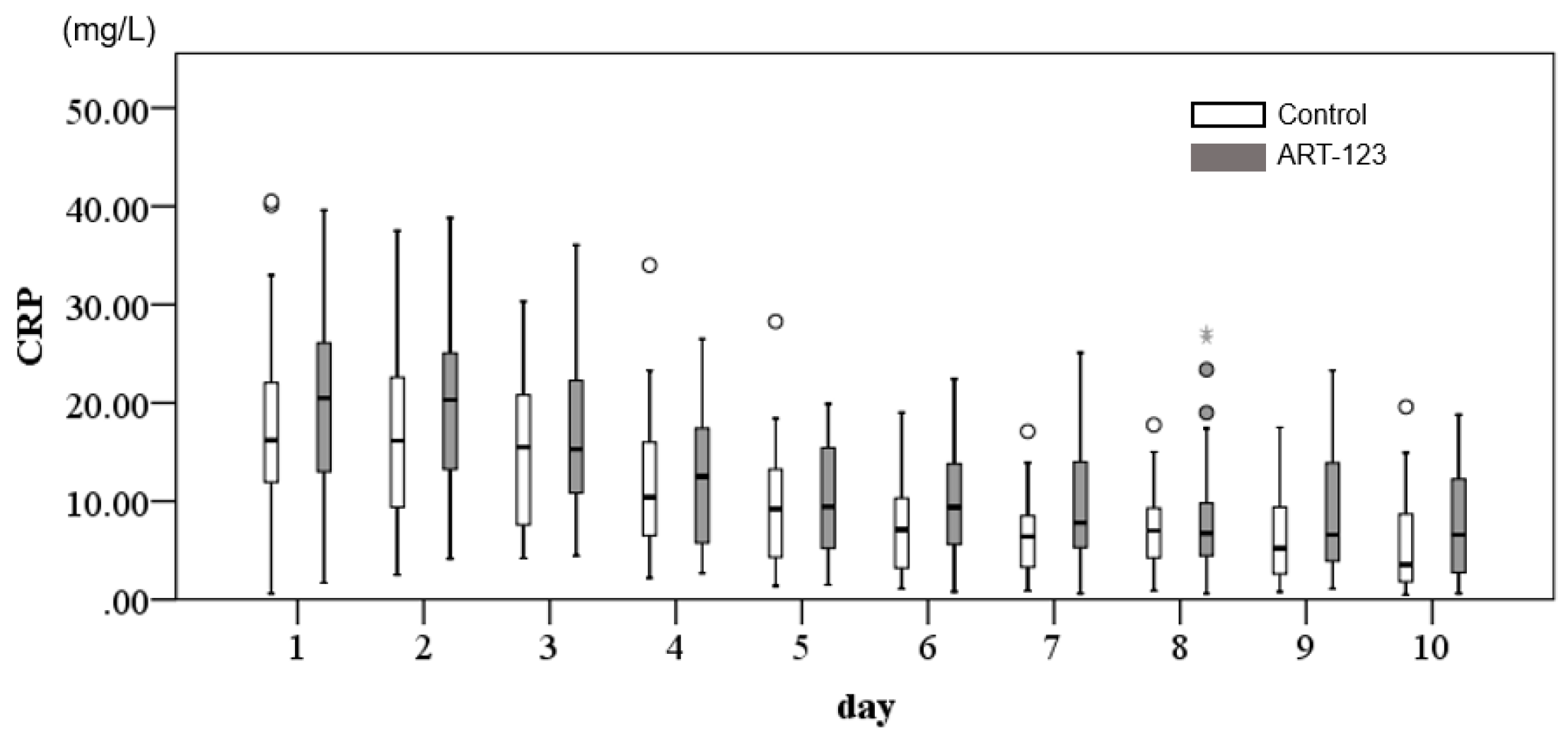
3.2. Overall General Clinical Conditions
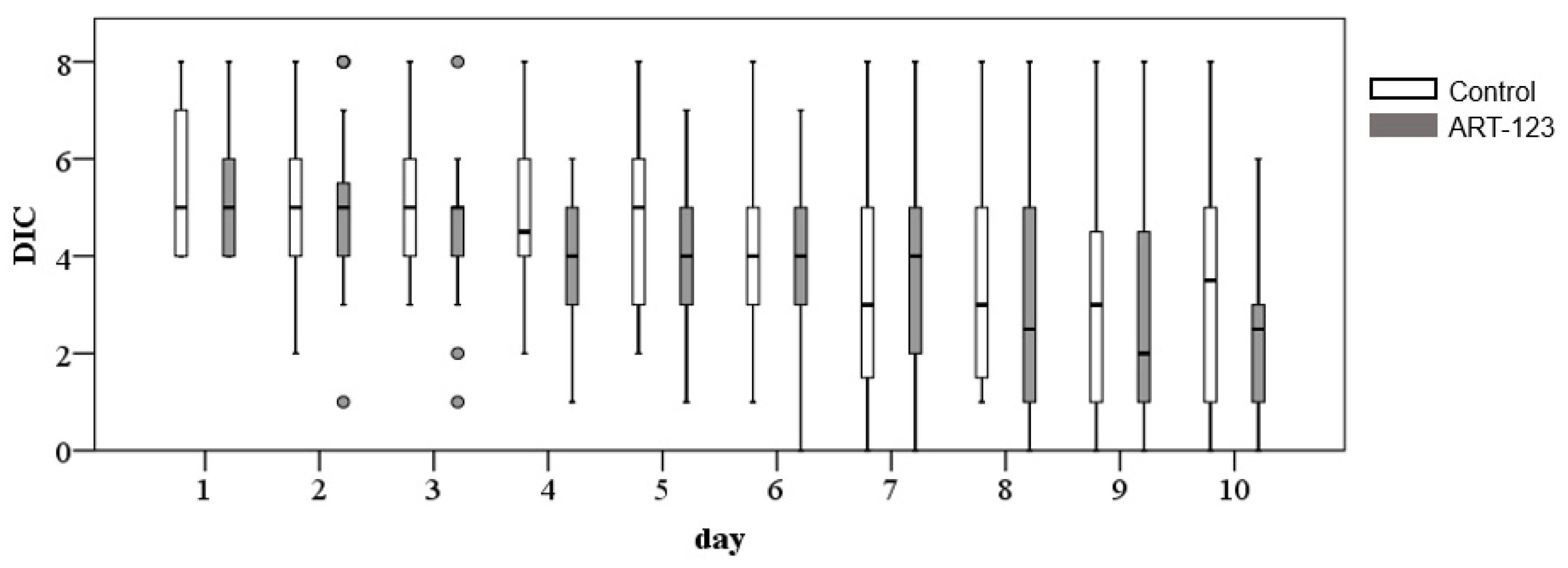
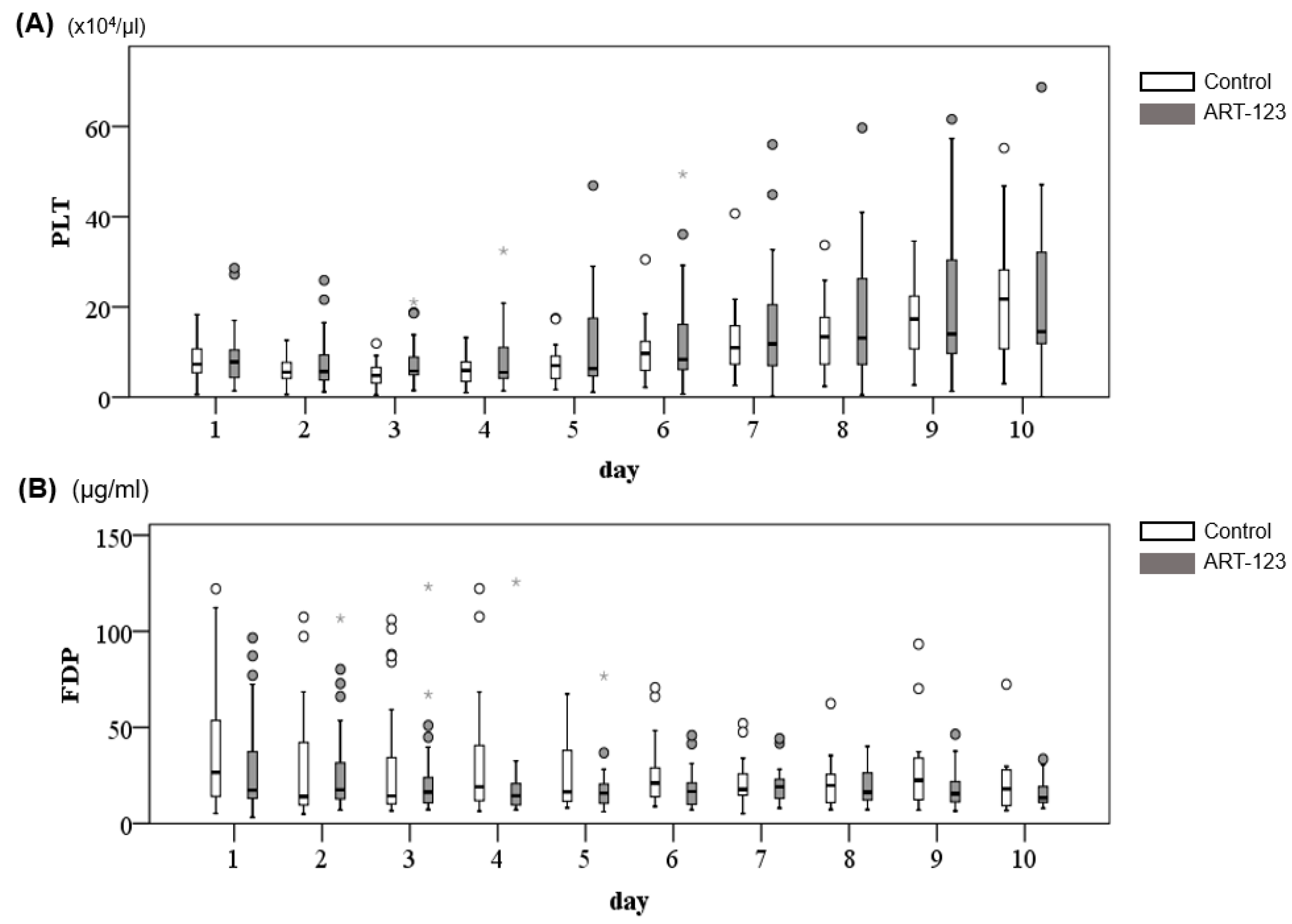
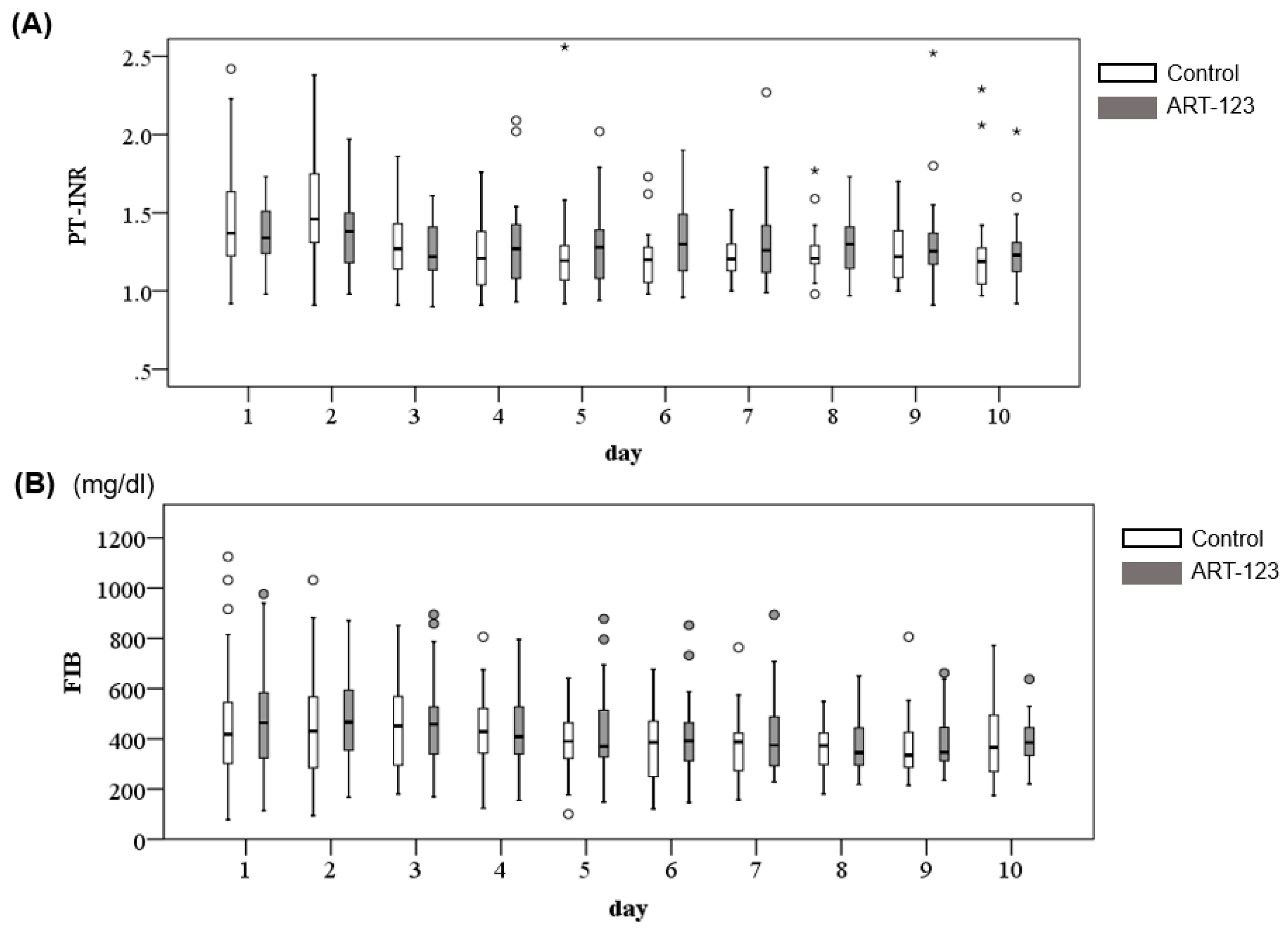
3.3. Change of DIC Parameters
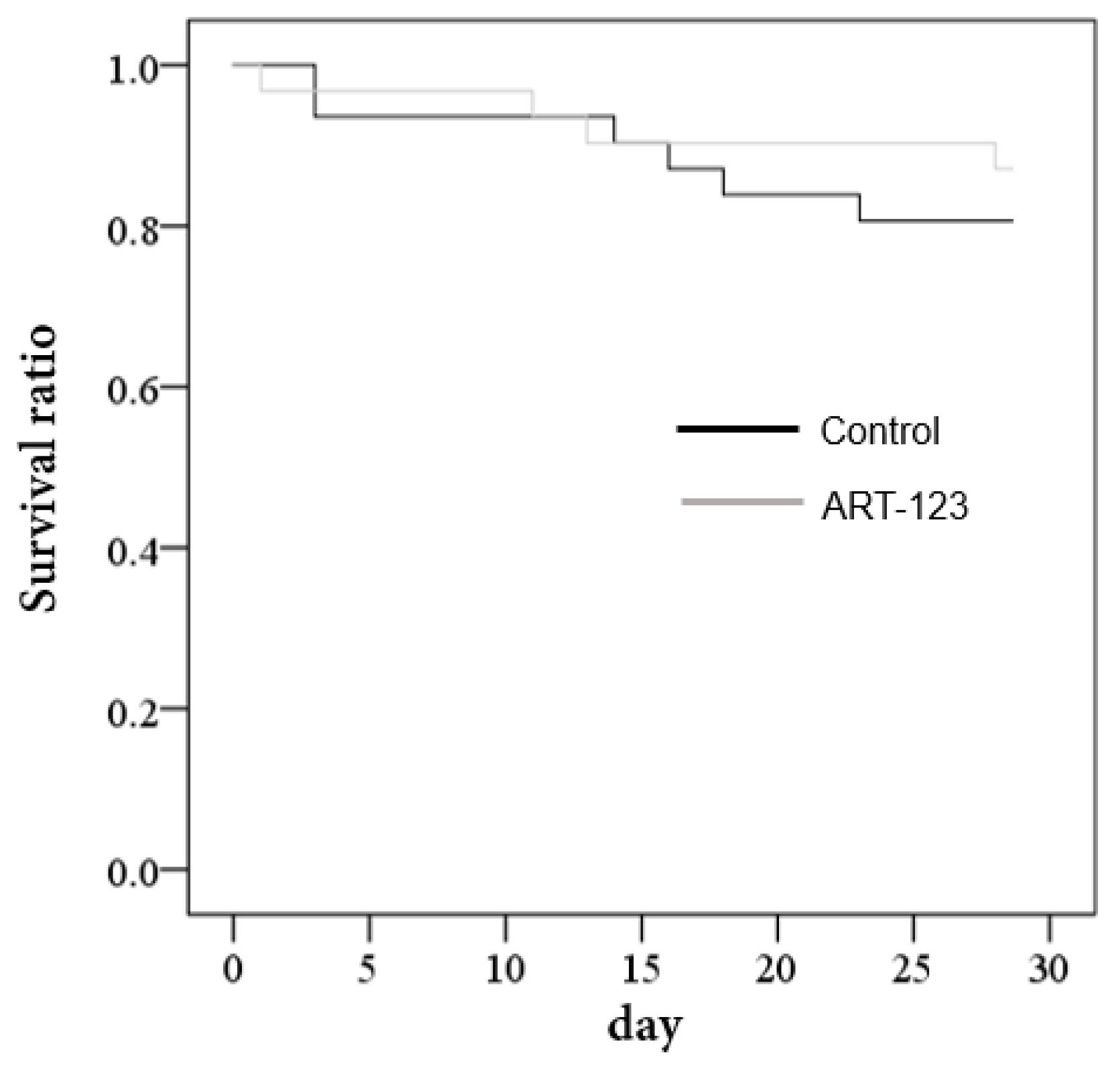
3.4. Overall Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Levi, M.; Ten Cate, H. Disseminated intravascular coagulation. N. Engl. J Med. 1999, 341, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, C.; Jourdi, G.; Adjambri, E.; Walborn, A.; Patel, P.; Fareed, J. Disseminated Intravascular Coagulation: An Update on Pathogenesis, Diagnosis, and Therapeutic Strategies. Clin. Appl. Thromb. Hemost. 2018, 1076029618806424. [Google Scholar] [CrossRef]
- Hayakawa, M.; Yamakawa, K.; Saito, S.; Uchino, S.; Kudo, D.; Iizuka, Y. Recombinant human soluble thrombomodulin and mortality in sepsis-induced disseminated intravascular coagulation. A multicentre retrospective study. Thromb. Haemost. 2016, 115, 1157–1166. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; Toh, C.H.; Thachil, J.; Watson, H.G. Guidelines for the diagnosis and management of disseminated intravascular coagulation. British Committee for Standards in Haematology. Br. J. Haematol. 2009, 145, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Taylor, F.B., Jr.; Toh, C.H.; Hoots, W.K.; Wada, H.; Levi, M. Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb. Haemost. 2001, 86, 1327–1330. [Google Scholar] [CrossRef] [PubMed]
- Wada, H.; Asakura, H.; Okamoto, K.; Iba, T.; Uchiyama, T.; Kawasugi, K. Expert consensus for the treatment of disseminated intravascular coagulation in Japan. Thromb. Res. 2010, 125, 6–11. [Google Scholar] [CrossRef]
- Levi, M. Japanese consensus for disseminated intravascular coagulation (DIC): Is it a small world after all? Thromb. Res. 2010, 125, 4–5. [Google Scholar] [CrossRef]
- Kisiel, W. Human plasma protein C: Isolation, characterization, and mechanism of activation by alpha-thrombin. J. Clin Investig. 1979, 64, 761–769. [Google Scholar] [CrossRef]
- Saito, H.; Maruyama, I.; Shimazaki, S.; Yamamoto, Y.; Aikawa, N.; Ohno, R. Efficacy and safety of recombinant human soluble thrombomodulin (ART-123) in disseminated intravascular coagulation: Results of a phase III, randomized, double-blind clinical trial. J. Thromb. Haemost. 2007, 5, 31–41. [Google Scholar] [CrossRef]
- Aikawa, N.; Shimazaki, S.; Yamamoto, Y.; Saito, H.; Maruyama, I.; Ohno, R. Thrombomodulin alfa in the treatment of infectious patients complicated by disseminated intravascular coagulation: Subanalysis from the phase 3 trial. Shock 2011, 35, 349–354. [Google Scholar] [CrossRef]
- Vincent, J.L.; Ramesh, M.K.; Ernest, D.; LaRosa, S.P.; Pachl, J.; Aikawa, N. A randomized, double-blind, placebo-controlled, Phase 2b study to evaluate the safety and efficacy of recombinant human soluble thrombomodulin, ART-123, in patients with sepsis and suspected disseminated intravascular coagulation. Crit. Care Med. 2013, 41, 2069–2079. [Google Scholar] [CrossRef]
- Vincent, J.L.; Francois, B.; Zabolotskikh, I.; Daga, M.K.; Lascarrou, J.B.; Kirov, M.Y. Effect of a Recombinant Human Soluble Thrombomodulin on Mortality in Patients with Sepsis-Associated Coagulopathy The SCARLET Randomized Clinical Trial. JAMA-J. Am. Med. Assoc. 2019, 321, 1993–2002. [Google Scholar] [CrossRef]
- Kato, T.; Matsuura, K. Recombinant human soluble thrombomodulin improves mortality in patients with sepsis especially for severe coagulopathy: A retrospective study. Thromb. J. 2018, 16, 19. [Google Scholar] [CrossRef]
- Yoshihiro, S.; Sakuraya, M.; Hayakawa, M.; Ono, K.; Hirata, A.; Takaba, A. Recombinant Human Soluble Thrombomodulin Contributes to Reduced Mortality in Sepsis Patients with Severe Respiratory Failure: A Retrospective Observational Study Using a Multicenter Dataset. Shock 2018. [Google Scholar] [CrossRef]
- Yamakawa, K.; Ogura, H.; Fujimi, S.; Morikawa, M.; Ogawa, Y.; Mohri, T. Recombinant human soluble thrombomodulin in sepsis-induced disseminated intravascular coagulation: A multicenter propensity score analysis. Intensive Care Med. 2013, 39, 644–652. [Google Scholar] [CrossRef]
- Wada, H.; Gabazza, E.C.; Asakura, H.; Koike, K.; Okamoto, K.; Maruyama, I. Comparison of diagnostic criteria for disseminated intravascular coagulation (DIC): Diagnostic criteria of the International Society of Thrombosis and Hemostasis and of the Japanese Ministry of Health and Welfare for overt DIC. Am. J. Hematol. 2003, 74, 17–22. [Google Scholar] [CrossRef]
- Bone, R.C.; Balk, R.A.; Cerra, F.B.; Dellinger, R.P.; Fein, A.M.; Knaus, W.A. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 1992, 101, 1644–1655. [Google Scholar] [CrossRef]
- Vincent, J.L.; de Mendonca, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef]
- Raith, E.P.; Udy, A.A.; Bailey, M.; McGloughlin, S.; MacIsaac, C.; Bellomo, R. Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality Among Adults with Suspected Infection Admitted to the Intensive Care Unit. JAMA 2017, 317, 290–300. [Google Scholar] [CrossRef]
- Knaus, W.A.; Zimmerman, J.E.; Wagner, D.P.; Draper, E.A.; Lawrence, D.E. APACHE-acute physiology and chronic health evaluation: A physiologically based classification system. Crit. Care Med. 1981, 9, 591–597. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Cardiac Arrhythmia Suppression Trial I. Preliminary report: effect of encainide and flecainide on mortality in a randomized trial of arrhythmia suppression after myocardial infarction. N. Engl. J. Med. 1989, 321, 406–412. [Google Scholar] [CrossRef]
- Warren, B.L.; Eid, A.; Singer, P.; Pillay, S.S.; Carl, P.; Novak, I. Caring for the critically ill patient. High-dose antithrombin III in severe sepsis: A randomized controlled trial. JAMA 2001, 286, 1869–1878. [Google Scholar] [CrossRef]
- Bernard, G.R.; Vincent, J.L.; Laterre, P.F.; LaRosa, S.P.; Dhainaut, J.F.; Lopez-Rodriguez, A. Efficacy and safety of recombinant human activated protein C for severe sepsis. N. Engl. J. Med. 2001, 344, 699–709. [Google Scholar] [CrossRef]
- Abraham, E.; Laterre, P.F.; Garg, R.; Levy, H.; Talwar, D.; Trzaskoma, B.L. Drotrecogin alfa (activated) for adults with severe sepsis and a low risk of death. N. Engl. J. Med. 2005, 353, 1332–1341. [Google Scholar] [CrossRef]
- Bernard, G.R.; Margolis, B.D.; Shanies, H.M.; Ely, E.W.; Wheeler, A.P.; Levy, H. Extended evaluation of recombinant human activated protein C United States Trial (ENHANCE US): A single-arm, phase 3B, multicenter study of drotrecogin alfa (activated) in severe sepsis. Chest 2004, 125, 2206–2216. [Google Scholar] [CrossRef]
- Abraham, E.; Reinhart, K.; Opal, S.; Demeyer, I.; Doig, C.; Rodriguez, A.L. Efficacy and safety of tifacogin (recombinant tissue factor pathway inhibitor) in severe sepsis: a randomized controlled trial. JAMA 2003, 290, 238–347. [Google Scholar] [CrossRef]
- Jaimes, F.; De la Rosa, G.; Arango, C.; Fortich, F.; Morales, C.; Aguirre, D. A randomized clinical trial of unfractioned heparin for treatment of sepsis (the HETRASE study): Design and rationale [NCT00100308]. Trials 2006, 7, 19. [Google Scholar] [CrossRef][Green Version]
- Jaimes, F.; De La Rosa, G.; Morales, C.; Fortich, F.; Arango, C.; Aguirre, D. Unfractioned heparin for treatment of sepsis: A randomized clinical trial (The HETRASE Study). Crit. Care Med. 2009, 37, 1185–1196. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Kitajima, Y.; Miyauchi, Y.; Izawa, K.; Tanaka, M.; Hirata, M. Assessment of bleeding in patients with disseminated intravascular coagulation after receiving surgery and recombinant human soluble thrombomodulin: A cohort study using a database. PLoS ONE 2018, 13, e0205146. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Gando, S.; Levi, M.; Toh, C.H. Disseminated intravascular coagulation. Nat. Rev. Dis. Primers 2016, 2, 16037. [Google Scholar] [CrossRef]
- Hato, T.; Maier, B.; Syed, F.; Myslinski, J.; Zollman, A.; Plotkin, Z. Bacterial sepsis triggers an antiviral response that causes translation shutdown. J. Clin. Invest. 2019, 129, 296–309. [Google Scholar] [CrossRef]
- Cohen, J. A Power Primer. Psychol Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Napolitano, L.M. Sepsis 2018: Definitions and Guideline Changes. Surg Infect. 2018, 19, 117–125. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Points | |
|---|---|
| Temp >38 °C or <36 °C | 1 |
| Heart rate >90 beats per min (bpm) | 1 |
| Respiratory rate >20 bpm or PaCO2 <32 mmHg | 1 |
| White blood cells (WBCs) >12,000/mm3, <4000/mm3, or >10% bands | 1 |
| Meets SIRS definition | ≥2 |
| Point | |
|---|---|
| Underlying disease | 0 |
| Clinical symptoms (SIRS score ≥3) | 1 |
| Platelet count (×104/µL) | |
| 8–12 or 30% reduction in 24 h | 1 |
| <8 or >50% reduction in 24 h | 3 |
| Fibrin-related marker | |
| Fibrinogen degradation products (FDPs) (µg/mL) | |
| 10≤ but <25 | 1 |
| ≥25 | 3 |
| Fibrinogen (mg/dL) | N/A |
| Prothrombin time international-normalized ratio (PT-INR) | |
| ≥1.2 | 1 |
| Diagnosis of disseminated intravascular coagulation (DIC) | ≥4 |
| ART-123 (n = 29) | Placebo (n = 31) | p-Value | ||
|---|---|---|---|---|
| Age, years | 72.9 ± 14.1 | 75.5 ± 11.0 | 0.416 | † |
| Gender (M:F) | 15:14 | 15:16 | 0.667 | †† |
| Severity score | ||||
| APACHE II score | 23.0 (18.0; 26.0) | 21.0 (14.0; 24.0] | 0.217 | ††† |
| SOFA score | 8.0 ± 3.8 | 7.8 ± 3.4 | 0.779 | † |
| DIC score | 5.1 ± 1.2 | 5.7 ± 1.5 | 0.092 | † |
| Laboratory data | ||||
| Platelet (×10) | 8.8 ± 6.3 | 9.3 ± 7.9 | 0.810 | † |
| FDP | 18.3 (13.1; 56.7) | 26.8 (14.3; 79.7) | 0.260 | ††† |
| Fibrinogen | 464.0 (348.0; 588.0) | 418.0 (294.0; 562.0) | 0.673 | ††† |
| PT-INR | 1.3 (1.2; 1.5) | 1.4 (1.2; 1.6) | 0.709 | ††† |
| Antithrombin | 39.1 (30.9; 52.5) | 34.4 (27.5; 44.7) | 0.478 | ††† |
| CRP | 20.5 (12.8; 26.1) | 16.2 (10.7; 22.9) | 0.278 | ††† |
| Primary infection site | ||||
| Lung | 8 | 8 | 1.000 | |
| Digestive system | 7 | 7 | 1.000 | |
| Bile duct | 3 | 3 | 1.000 | |
| Soft tissue | 1 | 3 | 0.614 | |
| Kidney/urinary tract | 3 | 5 | 0.710 | |
| Liver | 3 | 1 | 0.338 | |
| Others | 2 | 2 | 1.000 | |
| Unknown | 2 | 3 | 1.000 | |
| Surgery | 9 (31%) | 13 (42%) | 0.797 | †† |
| ART-123 (n = 9) | Control (n = 13) | |
|---|---|---|
| Gastrointestinal tract | 5 | 7 |
| Bile duct | 2 | |
| Renal | 1 | 3 |
| Abdominal cyst | 1 | |
| Vascular graft | 1 | |
| Soft tissue | 1 | 1 |
| ART-123 (n = 29) | Control (n = 31) | p-Value | |
|---|---|---|---|
| 28 day mortality | 7 | 7 | 0.56 |
| Adverse event | 1 | 0 | |
| APACHE II score | 14 | 17 | 0.26 |
| SOFA score | 4.8 | 5 | 0.44 |
| DIC score | 2 | 3.5 | 0.36 |
| DIC resolution | 21 | 19 | 0.26 |
| ID | Treatment | Age | Gender | Underlying disease | Surgery | APACHE II | CRP | DIC | Day | Cause |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | ART123 | 82 | M | Pneumonia | None | 24 | 26.1 | 4 | 9 | Pneumonia/sepsis |
| 5 | ART123 | 67 | F | AAA graft infection | None | 26 | 11.9 | 4 | 50 | AAA graft infection/sepsis |
| 7 | ART123 | 71 | F | Pneumonia/cholangitis | None | 24 | 26.9 | 4 | 44 | Pneumonia/MOF |
| 17 | ART123 | 75 | F | Unknown | None | 16 | 12.8 | 5 | 47 | Pneumonia/ARDS |
| 22 | ART123 | 81 | F | Intestine/strangulation | None | 27 | 24.5 | 4 | 26 | ARDS/sepsis |
| 41 | ART123 | 87 | F | Pneumonia | None | 23 | 20.8 | 4 | 12 | Pneumonia/sepsis |
| 51 | ART123 | 77 | M | Brain abscess/miliary TB | None | 33 | 20.6 | 4 | 4 | Tuberculosis/sepsis |
| 8 | Control | 84 | F | Pneumonia | None | 26 | 29.4 | 8 | 13 | Pneumonia/sepsis (autopsy) |
| 16 | Control | 74 | M | Cholecystitis/peritonitis | None | 30 | 14.9 | 6 | 17 | Sepsis |
| 20 | Control | 83 | F | Heat stroke | None | 24 | 15.9 | 7 | 14 | Sepsis |
| 23 | Control | 81 | F | Pneumonia | None | 24 | 5.9 | 4 | 22 | Pneumonia/ARDS |
| 35 | Control | 45 | F | Neck abscess | None | 29 | 33 | 8 | 32 | Sepsis |
| 47 | Control | 72 | F | Infectious endocarditis | None | 25 | 40.5 | 8 | 41 | IE/sepsis |
| 51 | Control | 72 | F | Unknown * | None | 33 | 14.7 | 6 | 2 | Sepsis |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, S.; Ai, T.; Sera, T.; Ochiai, K.; Otomo, Y. Human Soluble Recombinant Thrombomodulin, ART-123, Resolved Early Phase Coagulopathies, but Did Not Significantly Alter the 28 Day Outcome in the Treatment of DIC Associated with Infectious Systemic Inflammatory Response Syndromes. J. Clin. Med. 2019, 8, 1553. https://doi.org/10.3390/jcm8101553
Mori S, Ai T, Sera T, Ochiai K, Otomo Y. Human Soluble Recombinant Thrombomodulin, ART-123, Resolved Early Phase Coagulopathies, but Did Not Significantly Alter the 28 Day Outcome in the Treatment of DIC Associated with Infectious Systemic Inflammatory Response Syndromes. Journal of Clinical Medicine. 2019; 8(10):1553. https://doi.org/10.3390/jcm8101553
Chicago/Turabian StyleMori, Shusuke, Tomohiko Ai, Toshiki Sera, Kanae Ochiai, and Yasuhiro Otomo. 2019. "Human Soluble Recombinant Thrombomodulin, ART-123, Resolved Early Phase Coagulopathies, but Did Not Significantly Alter the 28 Day Outcome in the Treatment of DIC Associated with Infectious Systemic Inflammatory Response Syndromes" Journal of Clinical Medicine 8, no. 10: 1553. https://doi.org/10.3390/jcm8101553
APA StyleMori, S., Ai, T., Sera, T., Ochiai, K., & Otomo, Y. (2019). Human Soluble Recombinant Thrombomodulin, ART-123, Resolved Early Phase Coagulopathies, but Did Not Significantly Alter the 28 Day Outcome in the Treatment of DIC Associated with Infectious Systemic Inflammatory Response Syndromes. Journal of Clinical Medicine, 8(10), 1553. https://doi.org/10.3390/jcm8101553