Intermittent Use of Portable NIV Increases Exercise Tolerance in COPD: A Randomised, Cross-Over Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Population
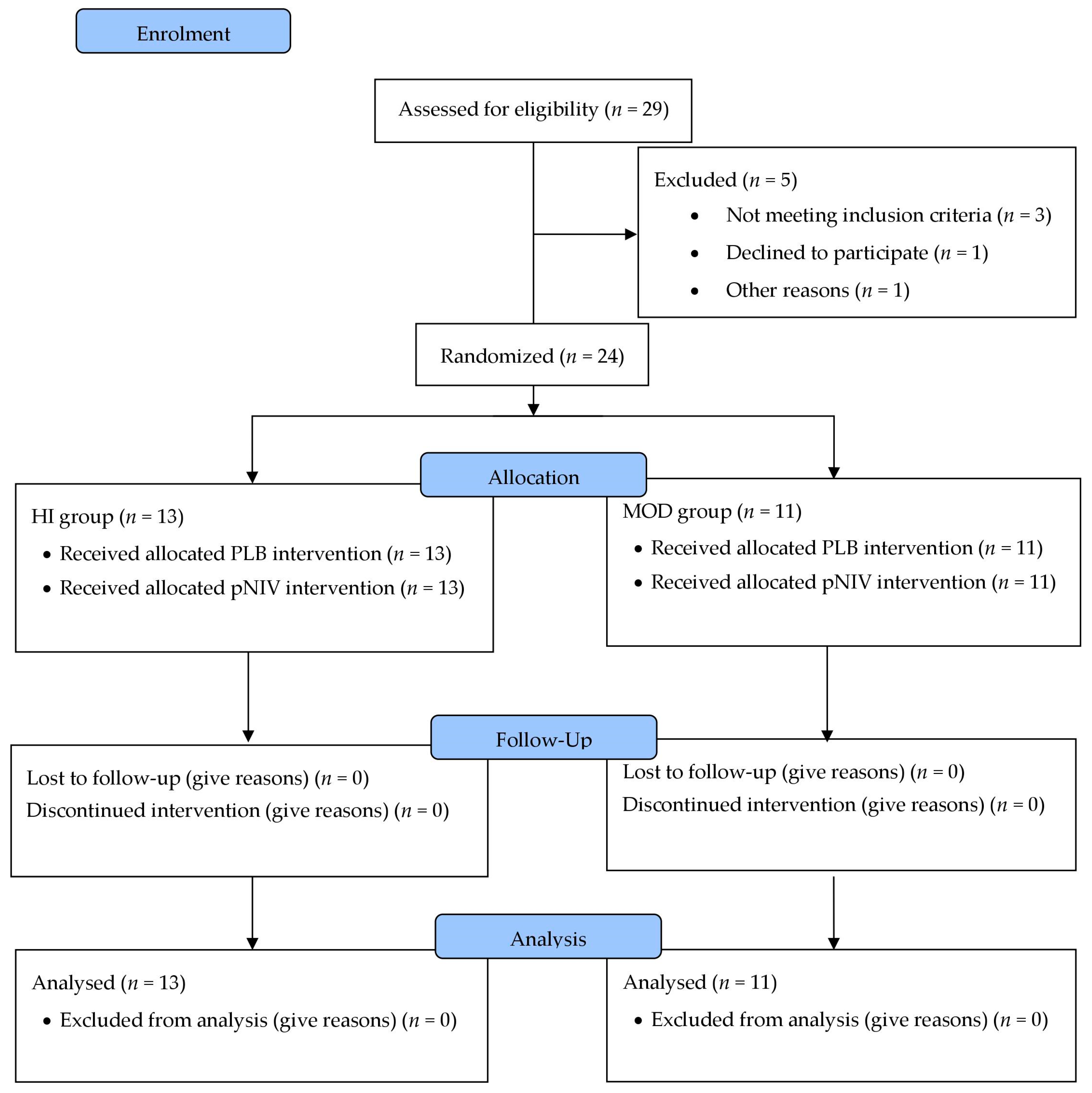
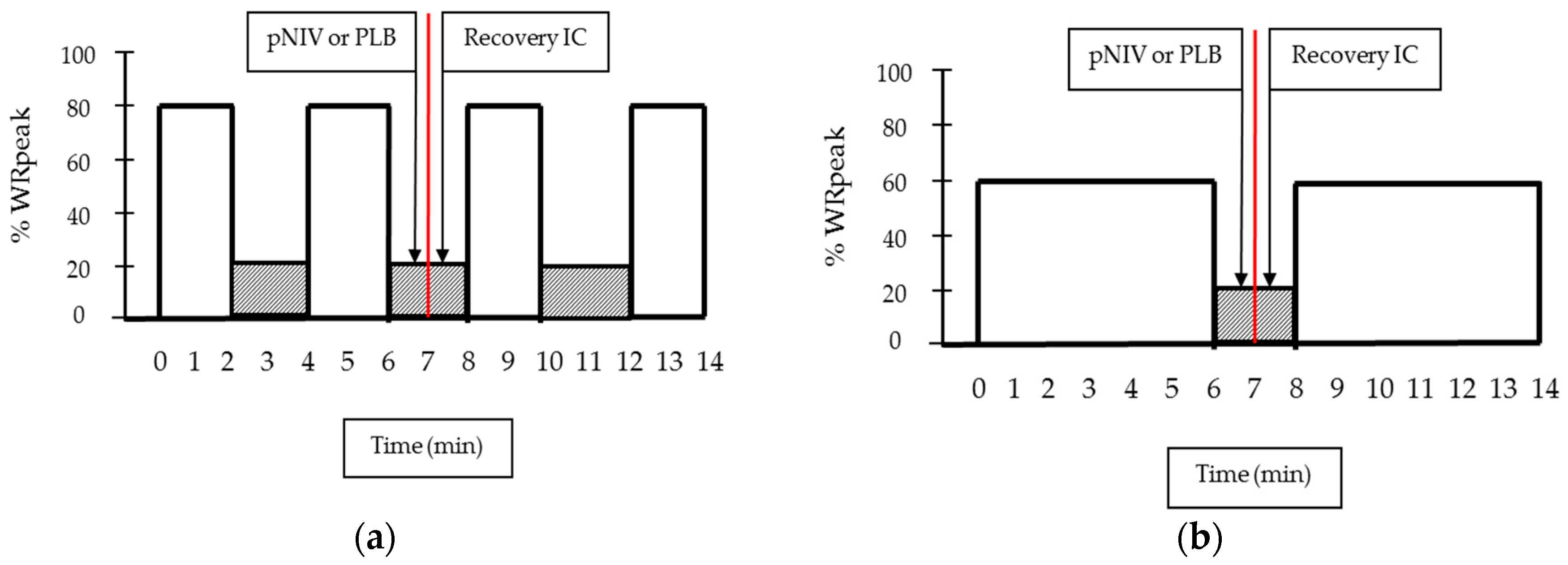
2.2. Study Design
2.3. Assessments
2.4. Interventions
2.5. Statistics
3. Results
3.1. Study Population
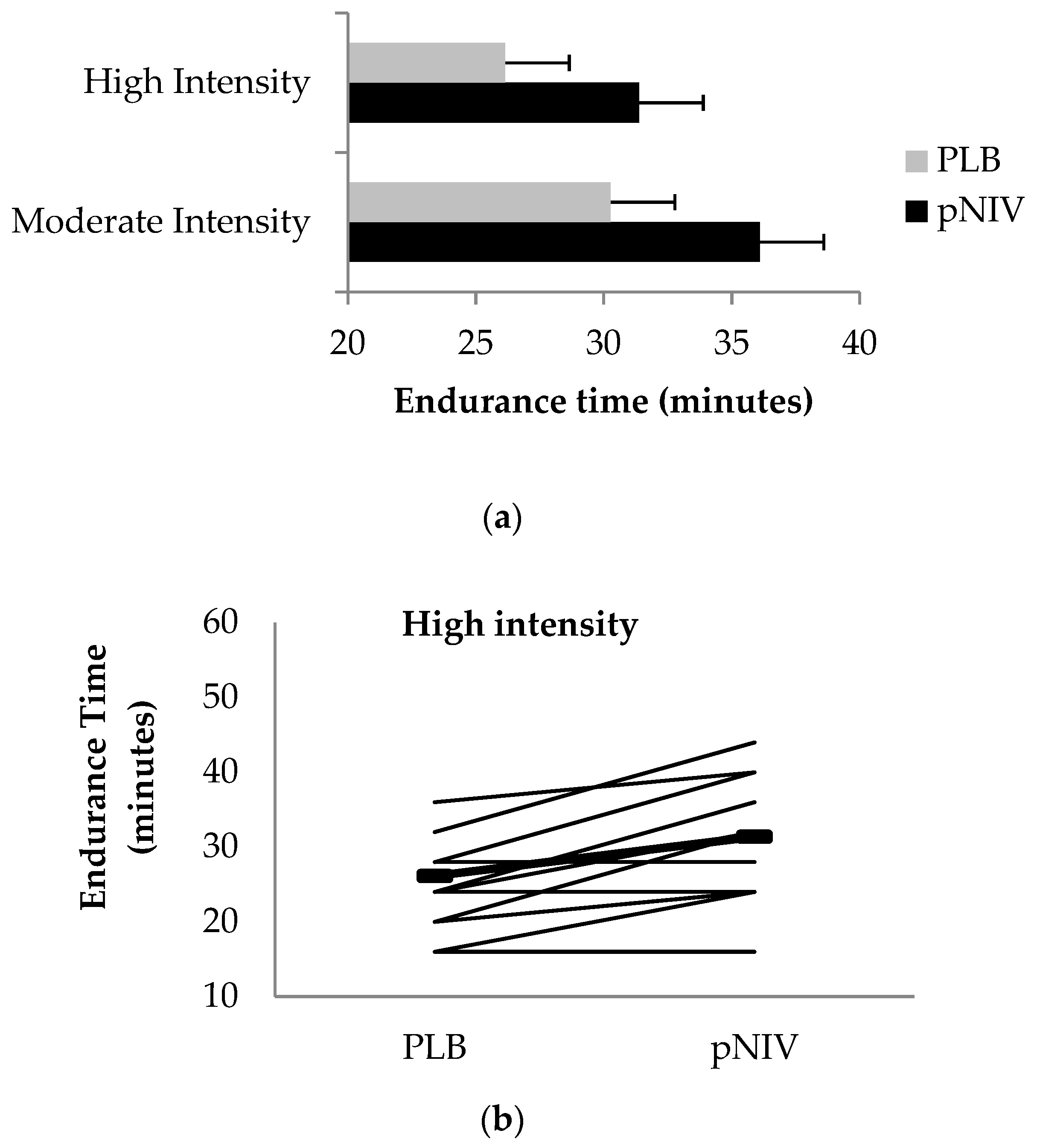
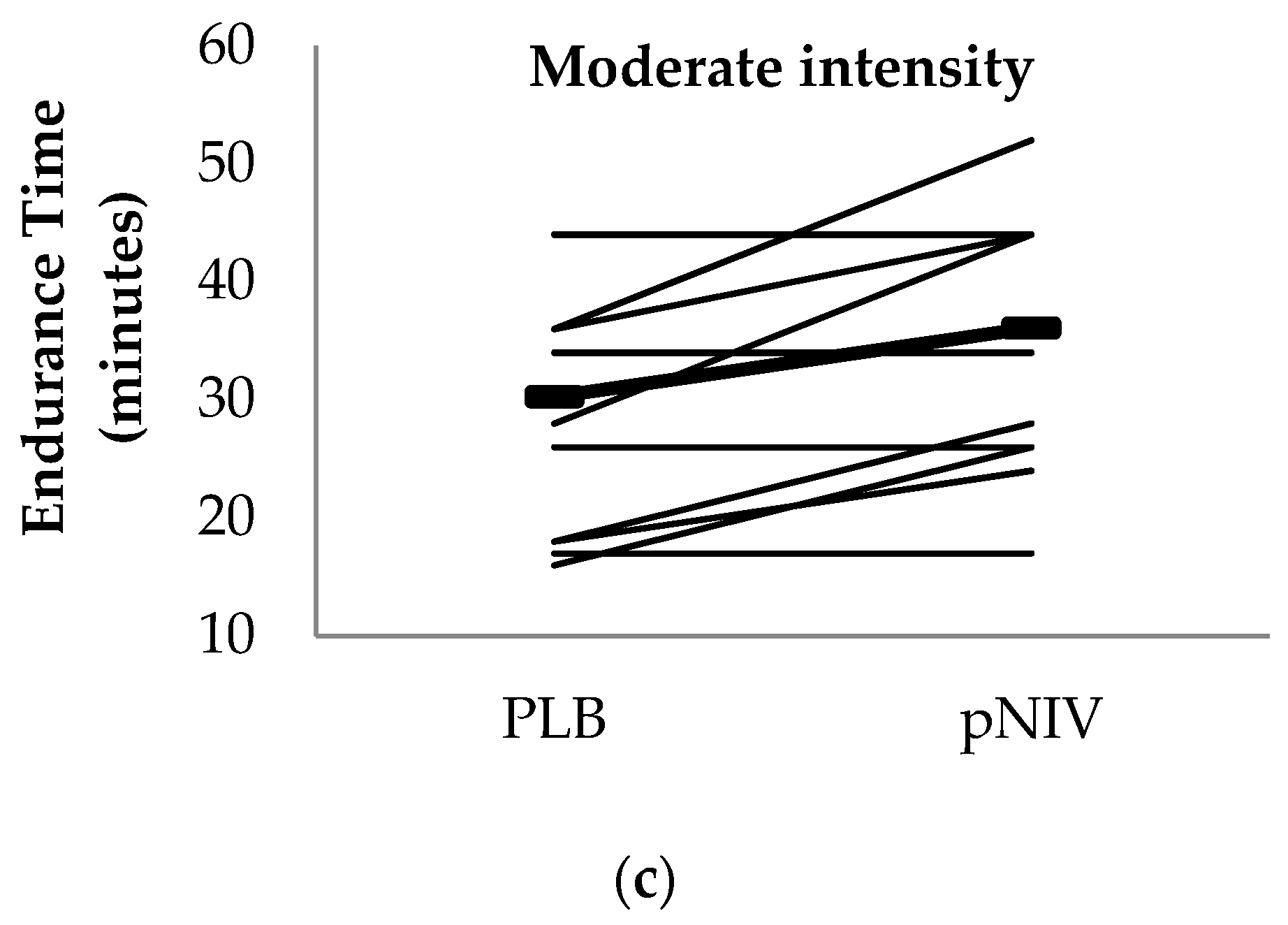
3.2. Endurance Time
3.3. Other Outcomes
3.4. Use and Perceived Benefits of the VitaBreath Device
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A: Methods
Appendix A.1. Study Population
- Male or female aged 40 years or older.
- Current or previous smoking history: 10 or more pack years.
- Spirometry confirmed stable COPD (GOLD stages II–IV) under optimal medical therapy.
- Exhibit substantial exercise-induced DH (ΔIC baseline > 0.15 L).
- Orthopaedic, neurological or other concomitant diseases that significantly impair normal biomechanical movement patterns, as judged by the investigator.
- Moderate or severe COPD exacerbation within 6 weeks.
- Unstable cardiac arrhythmia.
- Unstable ischaemic heart disease, including myocardial infarction within 6 weeks.
- Moderate or severe aortic stenosis or hypertrophic obstructive cardiomyopathy.
- Uncontrolled hypertension.
- Uncontrolled hypotension (systolic blood pressure (SBP) < 85 mmHg).
- Uncontrolled diabetes.
- Intolerance of the VitaBreath device.
Appendix A.2. Ramp Incremental Cardiopulmonary Exercise Testing (CPET)
Appendix A.3. Central Hemodynamics
Appendix A.4. Sample Size Justification
References
- Spruit, M.A.; Pitta, F.; McAuley, E.; ZuWallack, R.L.; Nici, L. Pulmonary rehabilitation and physical activity in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2015, 192, 924–933. [Google Scholar] [CrossRef]
- O’Donnell, D.E.; Revill, S.M.; Webb, K.A. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2001, 164, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Maltais, F.; Decramer, M.; Casaburi, R.; Barreiro, E.; Burelle, Y.; Debigare, R.; Dekhuijzen, P.N.; Franssen, F.; Gayan-Ramirez, G.; Gea, J.; et al. An official American thoracic society/European respiratory society statement: Update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2014, 189, 15–62. [Google Scholar] [CrossRef] [PubMed]
- Vogiatzis, I.; Zakynthinos, S. Factors limiting exercise tolerance in chronic lung diseases. Compr. Physiol. 2012, 2, 1779–1817. [Google Scholar] [PubMed]
- Beauchamp, M.K.; Nonoyama, M.; Goldstein, R.S.; Hill, K.; Dolmage, T.E.; Mathur, S.; Brooks, D. Interval versus continuous training in individuals with chronic obstructive pulmonary disease—A systematic review. Thorax 2010, 65, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Morris, N.R.; Walsh, J.; Adams, L.; Alision, J. Exercise training in COPD: What is it about intensity? Respirology 2016, 21, 1185–1192. [Google Scholar] [CrossRef] [Green Version]
- Puente-Maestu, L.; Palange, P.; Casaburi, R.; Laveneziana, P.; Maltais, F.; Neder, J.A.; O’Donnell, D.E.; Onorati, P.; Porszasz, J.; Rabinovich, R.; et al. Use of exercise testing in the evaluation of interventional efficacy: An official ERS statement. Eur. Respir. J. 2016, 47, 429–460. [Google Scholar] [CrossRef]
- Sabapathy, S.; Kingsley, R.A.; Schneider, D.A.; Adams, L.; Morris, N.R. Continuous and intermittent exercise responses in individuals with chronic obstructive pulmonary disease. Thorax 2004, 59, 1026–1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, D.E.; D’Arsigny, C.; Webb, K.A. Effects of hyperoxia on ventilatory limitation during exercise in advanced chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2001, 163, 892–898. [Google Scholar] [CrossRef]
- Palange, P. Lighter than air: Heliox breathing improves exercise tolerance in COPD. Eur. Respir. Rev. 2010, 19, 1–3. [Google Scholar] [CrossRef]
- Ambrosino, N.; Cigni, P. Non invasive ventilation as an additional tool for exercise training. Multidiscip. Respir. Med. 2015, 10, 14. [Google Scholar] [CrossRef] [PubMed]
- Hardy, W.; Jasko, J.; MS Clinical Research; Respironics, P. Available online: https://usermanual.wiki/Philips/vitabreathwhitepapera4final.3771554293.pdf (accessed on 7 October 2018).
- Bolton, C.E.; Bevan-Smith, E.F.; Blakey, J.D.; Crowe, P.; Elkin, S.L.; Garrod, R.; Greening, N.J.; Heslop, K.; Hull, J.H.; Man, W.D.; et al. British thoracic society guideline on pulmonary rehabilitation in adults. Thorax 2013, 68 (Suppl. 2), 1–30. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.; et al. An official American thoracic society/European respiratory society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, 13–64. [Google Scholar] [CrossRef] [PubMed]
- Declaration of Helsinki. Available online: https://www.wma.net/what-we-do/medical-ethics/declaration-of-helsinki/ (accessed on 14 January 2019).
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Borghi-Silva, A.; Oliveira, C.C.; Carrascosa, C.; Maia, J.; Berton, D.C.; Queiroga, F., Jr.; Ferreira, E.M.; Almeida, D.R.; Nery, L.E.; Neder, J.A. Respiratory muscle unloading improves leg muscle oxygenation during exercise in patients with COPD. Thorax 2008, 63, 910–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charloux, A.; Lonsdorfer-Wolf, E.; Richard, R.; Lampert, E.; Oswald-Mammosser, M.; Mettauer, B.; Geny, B.; Lonsdorfer, J. A new impedance cardiograph device for the non-invasive evaluation of cardiac output at rest and during exercise: Comparison with the “direct” Fick method. Eur. J. Appl. Physiol. 2000, 82, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Espersen, K.; Jensen, E.W.; Rosenborg, D.; Thomsen, J.K.; Eliasen, K.; Olsen, N.V.; Kanstrup, I.L. Comparison of cardiac output measurement techniques: Thermodilution, Doppler, CO2-rebreathing and the direct Fick method. Acta Anaesthesiol. Scand. 1995, 39, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Nasis, I.; Kortianou, E.; Vasilopoulou, M.; Spetsioti, S.; Louvaris, Z.; Kaltsakas, G.; Davos, C.H.; Zakynthinos, S.; Koulouris, N.G.; Vogiatzis, I. Hemodynamic effects of high intensity interval training in COPD patients exhibiting exercise-induced dynamic hyperinflation. Respir. Physiol. Neurobiol. 2015, 217, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.H.; Lai, F.O.; Hwang, N.C. Measurement of cardiac output using physio flow with different positions of electrode placement. Singap. Med. J. 2006, 47, 967–970. [Google Scholar]
- Bianchi, L.; Foglio, K.; Pagani, M.; Vitacca, M.; Rossi, A.; Ambrosino, N. Effects of proportional assist ventilation on exercise tolerance in COPD patients with chronic hypercapnia. Eur. Respir. J. 1998, 11, 422–427. [Google Scholar] [CrossRef] [Green Version]
- Bestall, J.C.; Paul, E.A.; Garrod, R.; Garnham, R.; Jones, P.W.; Wedzicha, J.A. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax 1999, 54, 581–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steer, J.; Gibson, J.; Bourke, S.C. The decaf score: Predicting hospital mortality in exacerbations of chronic obstructive pulmonary disease. Thorax 2012, 67, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.W.; Beeh, K.M.; Chapman, K.R.; Decramer, M.; Mahler, D.A.; Wedzicha, J.A. Minimal clinically important differences in pharmacological trials. Am. J. Respir. Crit. Care Med. 2014, 189, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Ambrosino, N.; Xie, L. The use of non-invasive ventilation during exercise training in COPD patients. COPD 2017, 14, 396–400. [Google Scholar] [CrossRef]
- Hawkins, P.; Johnson, L.C.; Nikoletou, D.; Hamnegard, C.H.; Sherwood, R.; Polkey, M.I.; Moxham, J. Proportional assist ventilation as an aid to exercise training in severe chronic obstructive pulmonary disease. Thorax 2002, 57, 853–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, J.E.; Gavin, D.J.; Adams-Dramiga, S. Effects of training with heliox and noninvasive positive pressure ventilation on exercise ability in patients with severe COPD. Chest 2002, 122, 464–472. [Google Scholar] [CrossRef]
- Menadue, C.; Piper, A.J.; van’t Hul, A.J.; Wong, K.K. Non-invasive ventilation during exercise training for people with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef] [Green Version]
- Reuveny, R.; Ben-Dov, I.; Gaides, M.; Reichert, N. Ventilatory support during training improves training benefit in severe chronic airway obstruction. Isr. Med. Assoc. J. 2005, 7, 151–155. [Google Scholar] [CrossRef]
- Van’t Hul, A.; Gosselink, R.; Hollander, P.; Postmus, P.; Kwakkel, G. Training with inspiratory pressure support in patients with severe COPD. Eur. Respir. J. 2006, 27, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Ricci, C.; Terzoni, S.; Gaeta, M.; Sorgente, A.; Destrebecq, A.; Gigliotti, F. Physical training and noninvasive ventilation in COPD patients: A meta-analysis. Respir. Care 2014, 59, 709–717. [Google Scholar] [CrossRef]
- Porszasz, J.; Cao, R.; Morishige, R.; van Eykern, L.A.; Stenzler, A.; Casaburi, R. Physiologic effects of an ambulatory ventilation system in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2013, 188, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Dolmage, T.E.; Goldstein, R.S. Proportional assist ventilation and exercise tolerance in subjects with COPD. Chest 1997, 111, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Hussain, O.; Collins, E.G.; Adiguzel, N.; Langbein, W.E.; Tobin, M.J.; Laghi, F. Contrasting pressure-support ventilation and helium-oxygen during exercise in severe COPD. Respir. Med. 2011, 105, 494–505. [Google Scholar] [CrossRef] [PubMed]
- Van’t Hul, A.; Gosselink, R.; Hollander, P.; Postmus, P.; Kwakkel, G. Acute effects of inspiratory pressure support during exercise in patients with COPD. Eur. Respir. J. 2004, 23, 34–40. [Google Scholar] [CrossRef] [Green Version]
- Berton, D.C.; Barbosa, P.B.; Takara, L.S.; Chiappa, G.R.; Siqueira, A.C.; Bravo, D.M.; Ferreira, L.F.; Neder, J.A. Bronchodilators accelerate the dynamics of muscle O2 delivery and utilisation during exercise in COPD. Thorax 2010, 65, 588–593. [Google Scholar] [CrossRef] [PubMed]
- Louvaris, Z.; Vogiatzis, I.; Aliverti, A.; Habazettl, H.; Wagner, H.; Wagner, P.; Zakynthinos, S. Blood flow does not redistribute from respiratory to leg muscles during exercise breathing heliox or oxygen in COPD. J. Appl. Physiol. 2014, 117, 267–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Marco, F.; Sotgiu, G.; Santus, P.; O’Donnell, D.E.; Beeh, K.M.; Dore, S.; Roggi, M.A.; Giuliani, L.; Blasi, F.; Centanni, S. Long-acting bronchodilators improve exercise capacity in COPD patients: A systematic review and meta-analysis. Respir. Res. 2018, 19, 18. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, D.E.; Elbehairy, A.F.; Berton, D.C.; Domnik, N.J.; Webb, K.A.; Neder, J.A. Exercise testing in the evaluation of pharmachotherapy in COPD. In Ers Monograph: Clinical Exercise Testing, 1st ed.; Palange, P., Laveneziana, P., Neder, J.A., Ward, S.A., Eds.; European Respiratory Society: Sheffield, UK, 2018; pp. 235–250. [Google Scholar]
- Vogiatzis, I.; Georgiadou, O.; Golemati, S.; Aliverti, A.; Kosmas, E.; Kastanakis, E.; Geladas, N.; Koutsoukou, A.; Nanas, S.; Zakynthinos, S.; et al. Patterns of dynamic hyperinflation during exercise and recovery in patients with severe chronic obstructive pulmonary disease. Thorax 2005, 60, 723–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borghi-Silva, A.; Carrascosa, C.; Oliveira, C.C.; Barroco, A.C.; Berton, D.C.; Vilaca, D.; Lira-Filho, E.B.; Ribeiro, D.; Nery, L.E.; Neder, J.A. Effects of respiratory muscle unloading on leg muscle oxygenation and blood volume during high-intensity exercise in chronic heart failure. Am. J. Physiol. Heart Circ. Physiol. 2008, 294, 2465–2472. [Google Scholar] [CrossRef]
- Chow, S.C.; Wang, H.; Shao, J. Sample Size Calculations in Clinical Research, 1st ed.; Headquarter: New York, NY, USA; Eastern Hemisphere Distribution: Basel, Switzerland, 2003. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | High-Intensity (n = 13) | Moderate-Intensity (n = 11) | p-Value |
|---|---|---|---|
| Gender (M/F) | 5/8 | 5/6 | |
| Age (years) | 66 ± 7 | 68 ± 10 | 0.510 |
| BMI | 26.9 ± 6.9 | 25.6 ± 6.8 | 0.659 |
| FEV1 (% predicted) | 46 ± 15 | 46 ± 21 | 0.948 |
| FVC (% predicted) | 87 ± 18 | 91 ± 21 | 0.605 |
| FEV1/FVC (%) | 43 ± 14 | 37 ± 12 | 0.487 |
| IC (litres) | 1.96 ± 0.56 | 2.03 ± 0.78 | 0.810 |
| IC (% predicted) | 79 ± 22 | 78 ± 23 | 0.807 |
| TLC (% predicted) | 130 ± 29 | 131 ± 15 | 0.975 |
| FRC (% predicted) | 172 ± 49 | 175 ± 37 | 0.845 |
| DLCO (% predicted) | 38 ± 18 | 38 ± 20 | 0.980 |
| Variable | High-Intensity (n = 13) | Moderate-Intensity (n = 11) | p-Value |
|---|---|---|---|
| WR (Watts) | 48 ± 25 | 48 ± 26 | 0.977 |
| WR (% predicted) | 46 ± 19 | 45 ± 26 | 0.883 |
| VO2 (mL/kg/min) | 13.5 ± 3.9 | 13.4 ± 3.2 | 0.808 |
| VO2 (% predicted) | 60 ± 12 | 61 ± 21 | 0.911 |
| VE/MVV (%) | 1.00 ± 0.21 | 0.99 ± 0.26 | 0.787 |
| ΔIC from rest (litres) | 0.60 ± 0.38 | 0.47 ± 0.33 | 0.399 |
| SpO2 (%) | 92 ± 5 | 92 ± 3 | 0.827 |
| CO (L/min) | 10.5 ± 3.9 | 11.2 ± 2.7 | 0.635 |
| HR (beats/min) | 113 ± 15 | 110 ± 18 | 0.728 |
| SV (mL) | 94 ± 30 | 101 ± 19 | 0.513 |
| Dyspnoea (Borg 1–10) | 4.2 ± 1.2 | 3.8 ± 0.7 | 0.269 |
| Leg discomfort (Borg 1–10) | 3.8 ± 1.1 | 3.3 ± 1.6 | 0.442 |
| High-Intensity | Moderate-Intensity | |||||
|---|---|---|---|---|---|---|
| Variable | PLB | pNIV Support | p-Value | PLB | pNIV Support | p-Value |
| Work Rate (watts) | 38 ± 20 | 38 ± 20 | - | 30 ± 17 | 30 ± 17 | - |
| ΔIC (litres) | −0.37 ± 0.31 | −0.37 ± 0.28 | 0.964 | −0.29 ± 0.25 | −0.27 ± 0,24 | 0.819 |
| Dyspnoea (Borg) | 4.8 ± 1.2 | 3.9 ± 1.4 | 0.005 | 4.0 ± 1.1 | 3.3 ± 1.1 | 0.004 |
| Leg Discomfort (Borg) | 4.5 ± 1.5 | 4.1 ± 1.8 | 0.027 | 4.1 ± 1.2 | 3.3 ± 1.6 | 0.011 |
| VO2 (mL/min/kg) | 11.89 ± 3.20 | 11.95 ± 3.45 | 0.879 | 12.82 ± 3.27 | 12.72 ± 3.11 | 0.778 |
| VE (litres/min) | 34.75 ± 18.43 | 36.47 ± 18.12 | 0.206 | 34.57 ± 14.64 | 33.84 ± 14.25 | 0.444 |
| VT (litres) | 1.2 ± 0.5 | 1.2 ± 0.5 | 0.202 | 1.2 ± 0.5 | 1.2 ± 0.5 | 0.549 |
| RF (breaths/min) | 29 ± 5 | 30 ± 5 | 0.256 | 30 ± 5 | 29 ± 3 | 0.409 |
| CO (litres/min) | 9.9 ± 2.6 | 10.5 ± 2.7 | 0.070 | 10.3 ± 2.4 | 10.5 ± 2.3 | 0.193 |
| HR (beats/min) | 105 ± 13 | 108 ± 15 | 0.172 | 114 ± 19 | 114 ± 16 | 0.725 |
| SV (mL/beat) | 94 ± 23 | 96 ± 22 | 0.487 | 90 ± 16 | 91 ± 13 | 0.485 |
| SBP (mmHg) | 146 ± 23 | 158 ± 23 | 0.002 | 142 ± 29 | 148 ± 22 | 0.285 |
| DBP (mmHg) | 82 ± 8 | 89 ± 9 | 0.024 | 78 ± 18 | 84 ± 17 | 0.049 |
| a-VO2 (mL/100 mL) | 8.9 ± 2.9 | 8.3 ± 3.1 | 0.205 | 8.9 ± 2.9 | 8.6 ± 2.9 | 0.371 |
| SpO2 (%) | 92 ± 5 | 93 ± 4 | 0.104 | 94 ± 3 | 93 ± 3 | 0.148 |
| Question | Pre-VitaBreath | Post-VitaBreath | p-Value |
|---|---|---|---|
| How anxious are you about becoming short of breath (SOB)? 1 = Not at all anxious 10 = Very anxious | 7.50 (5.25–8.75) | 4.00 (2–5.75) | 0.001 * 20 improvements 2 worse 2 ties |
| How long did it take you to recover from SOB? | 0.002 * 17 improvements 3 worse 4 ties | ||
| <1 min | 0 (0%) | 6 (25%) | |
| 2–3 min | 7 (29.2%) | 9 (37.5%) | |
| 4–5 min | 3 (12.5%) | 4 (16.7%) | |
| 5–7 min | 5 (20.8%) | 1 (4.2%) | |
| 7–10 min | 5 (20.8%) | 2 (8.3%) | |
| More than 10 min | 4 (16.7%) | 2 (8.3%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vogiatzis, I.; Chynkiamis, N.; Armstrong, M.; Lane, N.D.; Hartley, T.; Gray, W.K.; Bourke, S.C. Intermittent Use of Portable NIV Increases Exercise Tolerance in COPD: A Randomised, Cross-Over Trial. J. Clin. Med. 2019, 8, 94. https://doi.org/10.3390/jcm8010094
Vogiatzis I, Chynkiamis N, Armstrong M, Lane ND, Hartley T, Gray WK, Bourke SC. Intermittent Use of Portable NIV Increases Exercise Tolerance in COPD: A Randomised, Cross-Over Trial. Journal of Clinical Medicine. 2019; 8(1):94. https://doi.org/10.3390/jcm8010094
Chicago/Turabian StyleVogiatzis, Ioannis, Nikolaos Chynkiamis, Matthew Armstrong, Nicholas D. Lane, Tom Hartley, William K. Gray, and Stephen C. Bourke. 2019. "Intermittent Use of Portable NIV Increases Exercise Tolerance in COPD: A Randomised, Cross-Over Trial" Journal of Clinical Medicine 8, no. 1: 94. https://doi.org/10.3390/jcm8010094
APA StyleVogiatzis, I., Chynkiamis, N., Armstrong, M., Lane, N. D., Hartley, T., Gray, W. K., & Bourke, S. C. (2019). Intermittent Use of Portable NIV Increases Exercise Tolerance in COPD: A Randomised, Cross-Over Trial. Journal of Clinical Medicine, 8(1), 94. https://doi.org/10.3390/jcm8010094