Association between Cigarette Smoking Status and Composition of Gut Microbiota: Population-Based Cross-Sectional Study

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
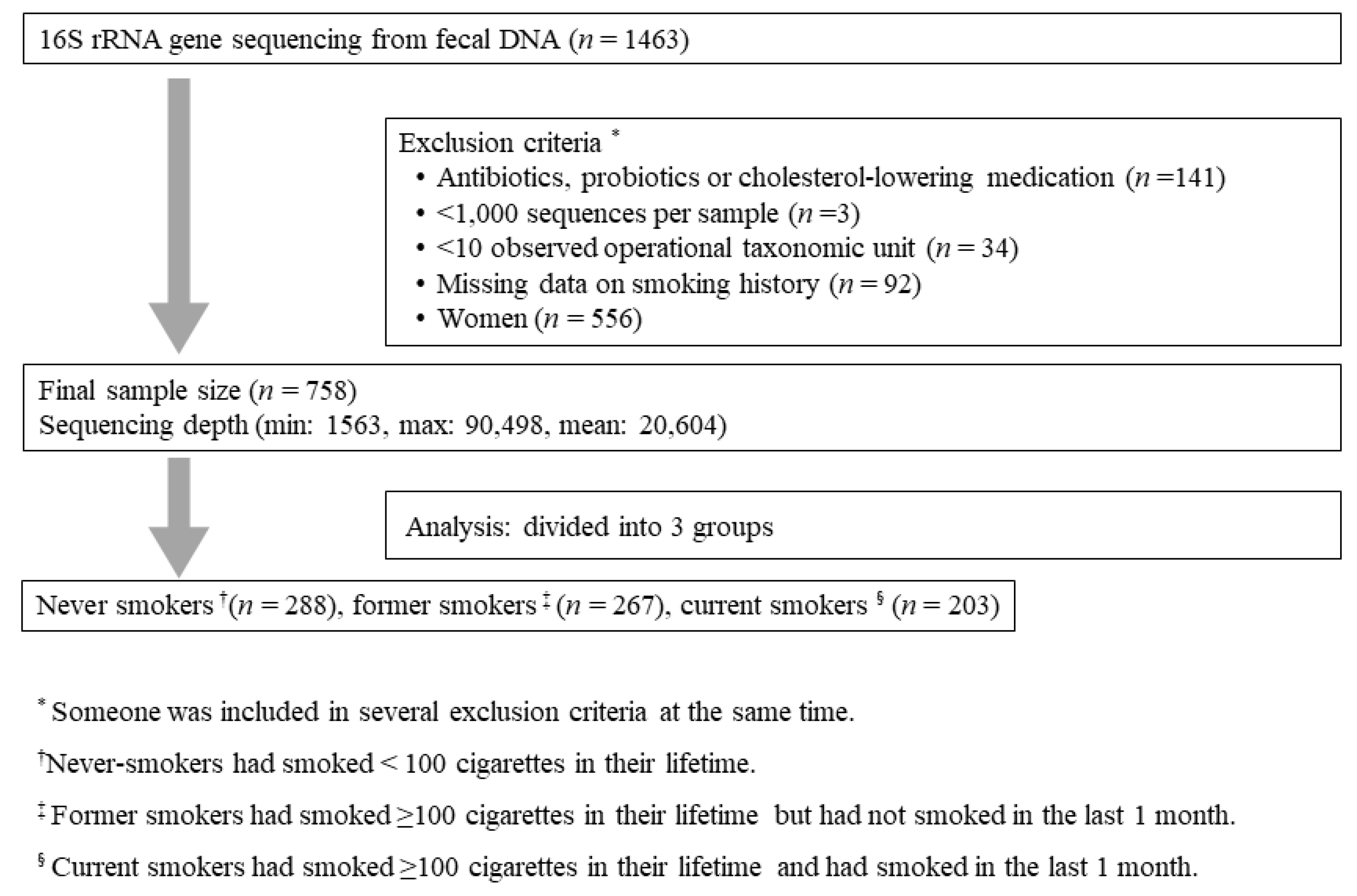
2.1. Study Population and Study Design
2.2. DNA Extraction from Fecal Samples and Sequencing of the Bacterial 16S rRNA Gene
2.3. 16S rRNA Gene Compositional Analysis
2.4. Statistical Analysis
2.6. Ethics Approval and Consent to Participate
2.7. Availability of Data and Materials
3. Results
3.1. Baseline Characteristics of the Subjects
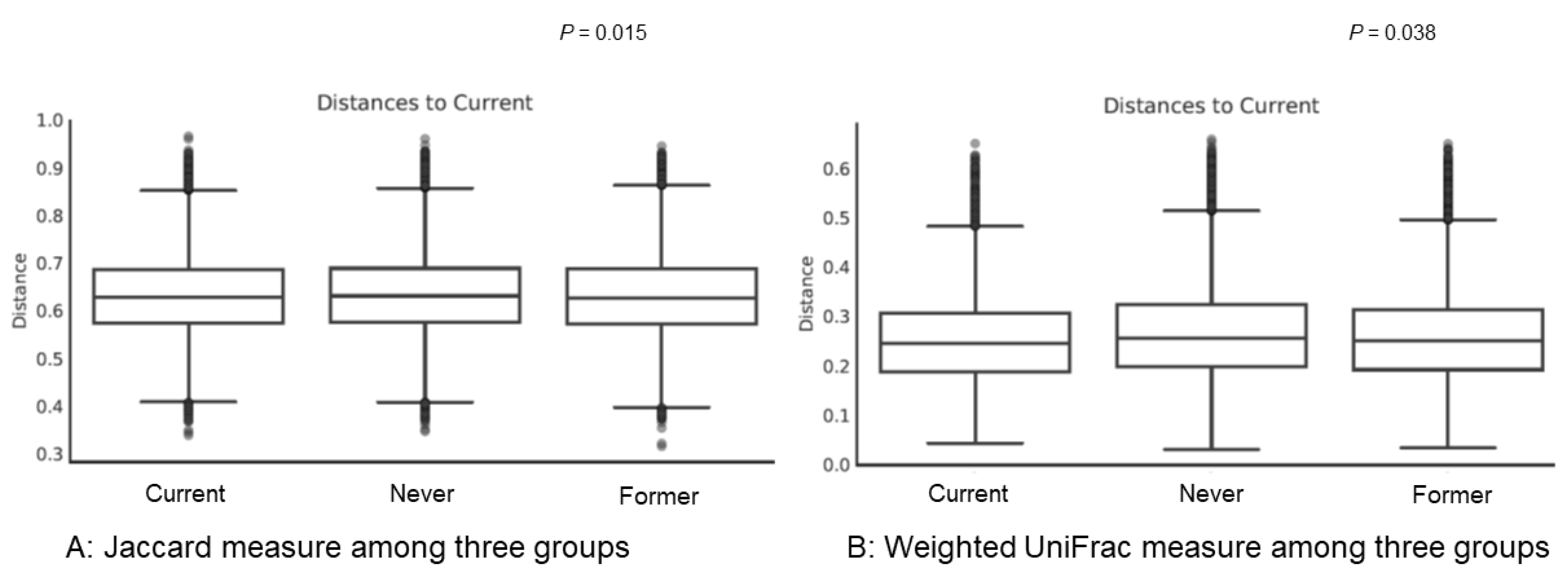
3.2. Diversity within and among Groups
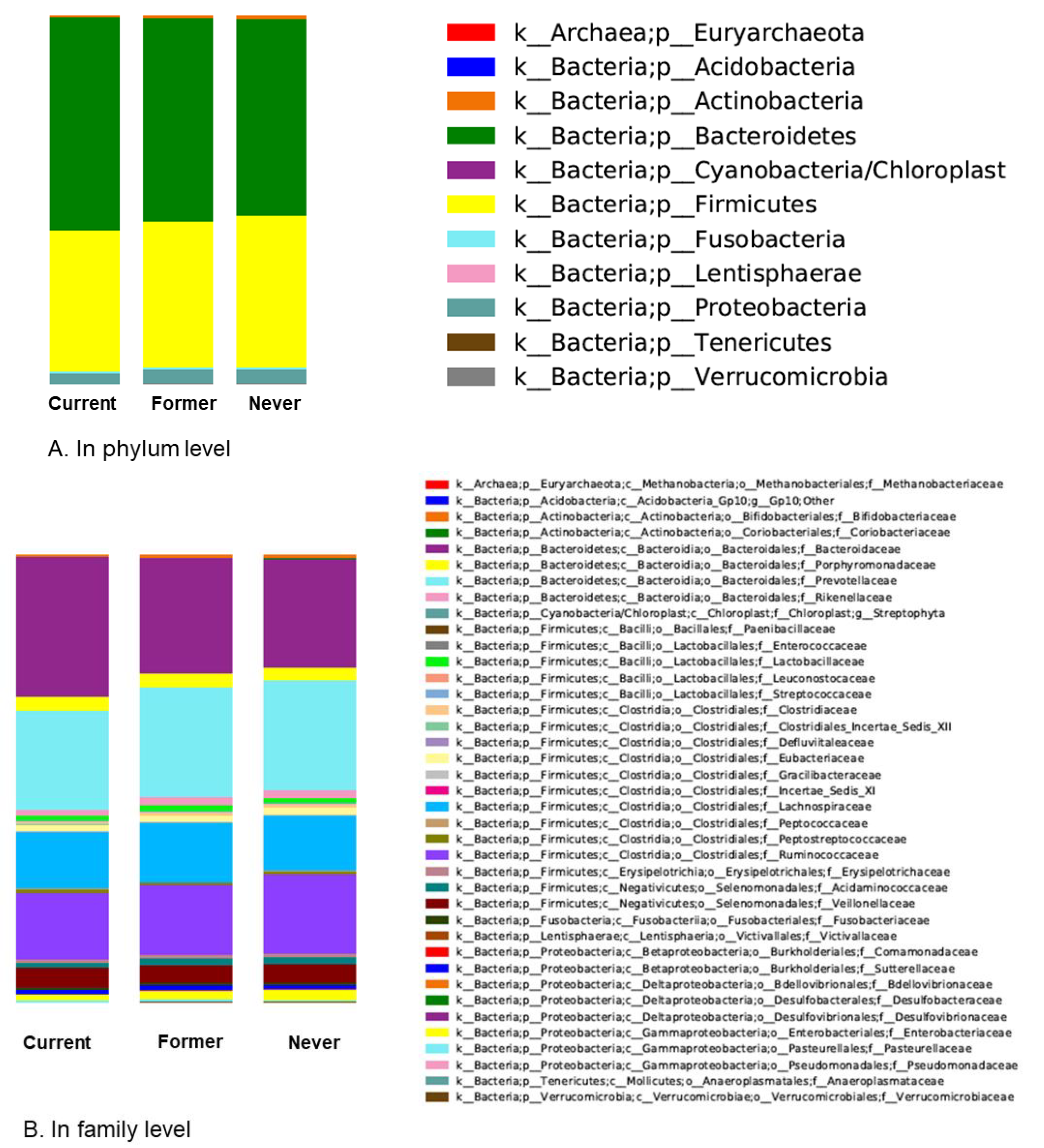
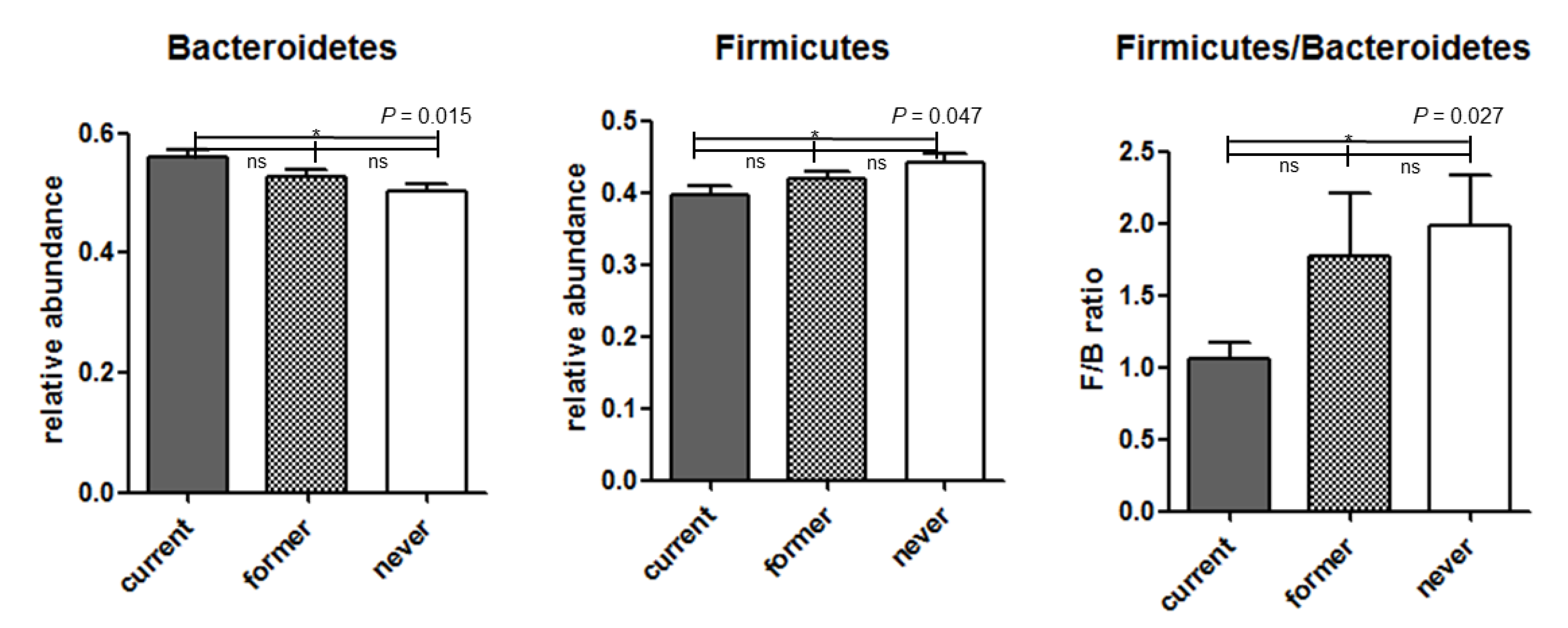
3.3. Analysis of Microbiota Composition
3.4. Additional Analysis of Subjects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Alberg, A.J.; Shopland, D.R.; Cummings, K.M. The 2014 surgeon general’s report: Commemorating the 50th anniversary of the 1964 report of the advisory committee to the us surgeon general and updating the evidence on the health consequences of cigarette smoking. Am. J. Epidemiol. 2014, 179, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (US); National Center for Chronic Disease Prevention and Health Promotion (US); Office on Smoking and Health (US). Publications and Reports of the Surgeon General. How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General; Centers for Disease Control and Prevention (US): Atlanta, GA, USA, 2010.
- Bilano, V.; Gilmour, S.; Moffiet, T.; d’Espaignet, E.T.; Stevens, G.A.; Commar, A.; Tuyl, F.; Hudson, I.; Shibuya, K. Global trends and projections for tobacco use, 1990–2025: An analysis of smoking indicators from the who comprehensive information systems for tobacco control. Lancet 2015, 385, 966–976. [Google Scholar] [CrossRef]
- Allais, L.; Kerckhof, F.M.; Verschuere, S.; Bracke, K.R.; De Smet, R.; Laukens, D.; Van den Abbeele, P.; De Vos, M.; Boon, N.; Brusselle, G.G.; et al. Chronic cigarette smoke exposure induces microbial and inflammatory shifts and mucin changes in the murine gut. Environ. Microbiol. 2016, 18, 1352–1363. [Google Scholar] [CrossRef] [PubMed]
- Biedermann, L.; Brulisauer, K.; Zeitz, J.; Frei, P.; Scharl, M.; Vavricka, S.R.; Fried, M.; Loessner, M.J.; Rogler, G.; Schuppler, M. Smoking cessation alters intestinal microbiota: Insights from quantitative investigations on human fecal samples using fish. Inflamm. Bowel Dis. 2014, 20, 1496–1501. [Google Scholar] [CrossRef] [PubMed]
- Biedermann, L.; Zeitz, J.; Mwinyi, J.; Sutter-Minder, E.; Rehman, A.; Ott, S.J.; Steurer-Stey, C.; Frei, A.; Frei, P.; Scharl, M.; et al. Smoking cessation induces profound changes in the composition of the intestinal microbiota in humans. PLoS ONE 2013, 8, e59260. [Google Scholar] [CrossRef] [PubMed]
- Browne, H.P.; Neville, B.A.; Forster, S.C.; Lawley, T.D. Transmission of the gut microbiota: Spreading of health. Nat. Rev. Microbiol. 2017, 15, 531–543. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Izard, J.; Walsh, E.; Batich, K.; Chongsathidkiet, P.; Clarke, G.; Sela, D.A.; Muller, A.J.; Mullin, J.M.; Albert, K.; et al. The host microbiome regulates and maintains human health: A primer and perspective for non-microbiologists. Cancer Res. 2017, 77, 1783–1812. [Google Scholar] [CrossRef] [PubMed]
- Claus, S.P.; Guillou, H.; Ellero-Simatos, S. The gut microbiota: A major player in the toxicity of environmental pollutants? NPJ Biofilms Microbiomes 2016, 2, 16003. [Google Scholar] [CrossRef] [PubMed]
- Faith, J.J.; Guruge, J.L.; Charbonneau, M.; Subramanian, S.; Seedorf, H.; Goodman, A.L.; Clemente, J.C.; Knight, R.; Heath, A.C.; Leibel, R.L.; et al. The long-term stability of the human gut microbiota. Science 2013, 341, 1237439. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Diao, H.; Jia, L.; Yuan, Y.; Thamm, D.H.; Wang, H.; Jin, Y.; Pei, S.; Zhou, B.; Yu, F.; et al. Proteus mirabilis inhibits cancer growth and pulmonary metastasis in a mouse breast cancer model. PLoS ONE 2017, 12, e0188960. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, J.A.; Quinn, R.A.; Debelius, J.; Xu, Z.Z.; Morton, J.; Garg, N.; Jansson, J.K.; Dorrestein, P.C.; Knight, R. Microbiome-wide association studies link dynamic microbial consortia to disease. Nature 2016, 535, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Ley, R.E. Obesity and the human microbiome. Curr. Opin. Gastroenterol. 2010, 26, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Capurso, G.; Lahner, E. The interaction between smoking, alcohol and the gut microbiome. Best Pract. Res. Clin. Gastroenterol. 2017, 31, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.A.; Greene, M.T.; Saint, S.; Chenoweth, C.E.; Malani, P.N.; Trivedi, I.; Aronoff, D.M. Higher rates of clostridium difficile infection among smokers. PLoS ONE 2012, 7, e42091. [Google Scholar] [CrossRef] [PubMed]
- Frank, D.N.; St Amand, A.L.; Feldman, R.A.; Boedeker, E.C.; Harpaz, N.; Pace, N.R. Molecular-phylogenetic characterization of microbial community imbalances in human inflammatory bowel diseases. Proc. Natl. Acad. Sci. USA 2007, 104, 13780–13785. [Google Scholar] [CrossRef] [PubMed]
- Quigley, E.M.M. Gut microbiome as a clinical tool in gastrointestinal disease management: Are we there yet? Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Parkes, G.C.; Whelan, K.; Lindsay, J.O. Smoking in inflammatory bowel disease: Impact on disease course and insights into the aetiology of its effect. J. Crohns Colitis 2014, 8, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.N.; Yun, Y.; Ryu, S.; Chang, Y.; Kwon, M.J.; Cho, J.; Shin, H.; Kim, H.L. Correlation between gut microbiota and personality in adults: A cross-sectional study. Brain Behav. Immun. 2018, 69, 374–385. [Google Scholar] [CrossRef] [PubMed]
- Fadrosh, D.W.; Ma, B.; Gajer, P.; Sengamalay, N.; Ott, S.; Brotman, R.M.; Ravel, J. An improved dual-indexing approach for multiplexed 16s rrna gene sequencing on the illumina miseq platform. Microbiome 2014, 2, 6. [Google Scholar] [CrossRef] [PubMed]
- Kozich, J.J.; Westcott, S.L.; Baxter, N.T.; Highlander, S.K.; Schloss, P.D. Development of a dual-index sequencing strategy and curation pipeline for analyzing amplicon sequence data on the miseq illumina sequencing platform. Appl. Environ. Microbiol. 2013, 79, 5112–5120. [Google Scholar] [CrossRef] [PubMed]
- Edgar, R.C. Uparse: Highly accurate otu sequences from microbial amplicon reads. Nat. Methods 2013, 10, 996–998. [Google Scholar] [CrossRef] [PubMed]
- Navas-Molina, J.A.; Peralta-Sanchez, J.M.; Gonzalez, A.; McMurdie, P.J.; Vazquez-Baeza, Y.; Xu, Z.; Ursell, L.K.; Lauber, C.; Zhou, H.; Song, S.J.; et al. Advancing our understanding of the human microbiome using QIIME. Methods Enzymol. 2013, 531, 371–444. [Google Scholar] [PubMed]
- Chao, A.; Shen, T.-J. Nonparametric estimation of shannon’s index of diversity when there are unseen species in sample. Environ. Ecol. Stat. 2003, 10, 429–443. [Google Scholar] [CrossRef]
- Lozupone, C.; Lladser, M.E.; Knights, D.; Stombaugh, J.; Knight, R. Unifrac: An effective distance metric for microbial community comparison. ISME J. 2011, 5, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.; Van Treuren, W.; White, R.A.; Eggesbo, M.; Knight, R.; Peddada, S.D. Analysis of composition of microbiomes: A novel method for studying microbial composition. Microb. Ecol. Health Dis. 2015, 26, 27663. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Peters, B.A.; Dominianni, C.; Zhang, Y.; Pei, Z.; Yang, L.; Ma, Y.; Purdue, M.P.; Jacobs, E.J.; Gapstur, S.M.; et al. Cigarette smoking and the oral microbiome in a large study of american adults. ISME J. 2016, 10, 2435–2446. [Google Scholar] [CrossRef] [PubMed]
- Opstelten, J.L.; Plassais, J.; van Mil, S.W.C.; Achouri, E.; Pichaud, M.; Siersema, P.D.; Oldenburg, B.; Cervino, A.C.L. Gut microbial diversity is reduced in smokers with Crohn’s disease. Inflamm. Bowel Dis. 2016, 22, 2070–2077. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, J.L.; Hedin, C.R.; Koutsoumpas, A.; Ng, S.C.; McCarthy, N.E.; Prescott, N.J.; Pessoa-Lopes, P.; Mathew, C.G.; Sanderson, J.; Hart, A.L.; et al. Smokers with active Crohn’s disease have a clinically relevant dysbiosis of the gastrointestinal microbiota. Inflamm. Bowel Dis. 2012, 18, 1092–1100. [Google Scholar] [CrossRef] [PubMed]
- Ley, R.E.; Turnbaugh, P.J.; Klein, S.; Gordon, J.I. Microbial ecology: Human gut microbes associated with obesity. Nature 2006, 444, 1022–1023. [Google Scholar] [CrossRef] [PubMed]
- Koliada, A.; Syzenko, G.; Moseiko, V.; Budovska, L.; Puchkov, K.; Perederiy, V.; Gavalko, Y.; Dorofeyev, A.; Romanenko, M.; Tkach, S.; et al. Association between body mass index and firmicutes/bacteroidetes ratio in an adult ukrainian population. BMC Microbiol. 2017, 17, 120. [Google Scholar] [CrossRef] [PubMed]
- Jha, P.; Peto, R. Global effects of smoking, of quitting, and of taxing tobacco. N. Engl. J. Med. 2014, 370, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Tomoda, K.; Kubo, K.; Asahara, T.; Andoh, A.; Nomoto, K.; Nishii, Y.; Yamamoto, Y.; Yoshikawa, M.; Kimura, H. Cigarette smoke decreases organic acids levels and population of bifidobacterium in the caecum of rats. J. Toxicol. Sci. 2011, 36, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhao, J.X.; Hu, N.; Ren, J.; Du, M.; Zhu, M.J. Side-stream smoking reduces intestinal inflammation and increases expression of tight junction proteins. World J. Gastroenterol. 2012, 18, 2180–2187. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, F.J.; Srivastava, E.D.; Rhodes, M.; van Dijk, A.P.; Fogg, F.; Samson, H.J.; Copeman, M.; Russell, M.A.; Feyerabend, C.; Williams, G.T.; et al. Effect of nicotine on rectal mucus and mucosal eicosanoids. Gut 1994, 35, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Verschuere, S.; Bracke, K.R.; Demoor, T.; Plantinga, M.; Verbrugghe, P.; Ferdinande, L.; Lambrecht, B.N.; Brusselle, G.G.; Cuvelier, C.A. Cigarette smoking alters epithelial apoptosis and immune composition in murine galt. Lab. Investig. 2011, 91, 1056–1067. [Google Scholar] [CrossRef] [PubMed]
- Eliakim, R.; Fan, Q.X.; Babyatsky, M.W. Chronic nicotine administration differentially alters jejunal and colonic inflammation in interleukin-10 deficient mice. Eur. J. Gastroenterol. Hepatol. 2002, 14, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Chi, L.; Mahbub, R.; Gao, B.; Bian, X.; Tu, P.; Ru, H.; Lu, K. Nicotine alters the gut microbiome and metabolites of gut-brain interactions in a sex-specific manner. Chem. Res. Toxicol. 2017, 30, 2110–2119. [Google Scholar] [CrossRef] [PubMed]
- Jandhyala, S.M.; Talukdar, R.; Subramanyam, C.; Vuyyuru, H.; Sasikala, M.; Reddy, D.N. Role of the normal gut microbiota. World J. Gastroenterol. 2015, 21, 8787–8803. [Google Scholar] [CrossRef] [PubMed]
- Sopori, M. Effects of cigarette smoke on the immune system. Nat. Rev. Immunol. 2002, 2, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Corrêa-Oliveira, R.; Fachi, J.L.; Vieira, A.; Sato, F.T.; Vinolo, M.A.R. Regulation of immune cell function by short-chain fatty acids. Clin. Transl. Immunol. 2016, 5, e73. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.L.; Heaver, S.L.; Walters, W.A.; Ley, R.E. Microbiome and metabolic disease: Revisiting the bacterial phylum bacteroidetes. J. Mol. Med. 2017, 95, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Morrison, D.J.; Preston, T. Formation of short chain fatty acids by the gut microbiota and their impact on human metabolism. Gut Microbes 2016, 7, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Mariat, D.; Firmesse, O.; Levenez, F.; Guimaraes, V.; Sokol, H.; Dore, J.; Corthier, G.; Furet, J.P. The firmicutes/bacteroidetes ratio of the human microbiota changes with age. BMC Microbiol. 2009, 9, 123. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Kim, Y.; Park, S.; Lee, J.; Oh, K. Trends in cigarette smoking among adolescents and adults in South Korea. Epidemiol. Health 2014, 36, e2014023. [Google Scholar] [CrossRef] [PubMed]
- Savin, Z.; Kivity, S.; Yonath, H.; Yehuda, S. Smoking and the intestinal microbiome. Arch. Microbiol. 2018, 200, 677–684. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Never (N = 288) | Former (N = 267) | Current (N = 203) | p-Value |
|---|---|---|---|---|
| Age, year | 44.2 ± 9.1 | 47.2 ± 8.5 | 45.7 ± 8.2 | <0.001 |
| BMI, kg/m2 | 24.7 ± 3.0 | 24.6 ± 2.6 | 24.8 ± 3.1 | 0.823 |
| Muscle mass, kg | 52.8 ± 5.8 | 52.5 ± 5.4 | 53.2 ± 6.0 | 0.455 |
| Fat mass, kg | 17.3 ± 5.7 | 17.1 ± 4.9 | 17.2 ± 5.7 | 0.864 |
| Smoking history | ||||
| Smoking amount, pack-years | 0 | 12.9 ± 10.2 | 17.6 ± 12.4 | <0.001 |
| Smoking amount, cigarette/day | 0 | 14.5 ± 7.0 | 14.3 ± 7.2 | <0.001 |
| Smoking duration, years | 0 | 16.2 ± 9.0 | 22.9 ± 8.7 | <0.001 |
| Creatinine, mg/dL | 0.99 ± 0.12 | 1.0 ± 0.11 | 0.97 ± 0.13 | 0.011 |
| eGFR, MDRD, /mL min/1.73 m2 | 88.8 ± 13.1 | 86.9 ± 11.5 | 91.5 ± 14.6 | 0.001 |
| Iron, μg/dL | 127.0 ± 37.9 | 127.0 ± 39.3 | 127.9 ± 38.7 | 0.972 |
| Ferritin, ng/mL | 203 ± 111.8 | 218.5 ± 134.1 | 224.8 ± 164.4 | 0.176 |
| C-reactive protein, mg/dL | 0.11 ± 0.17 | 0.12 ± 0.21 | 0.12 ± 0.19 | 0.754 |
| Comorbidities | ||||
| Diabetes mellitus | 11 (3.8) | 27 (10.1) | 15 (7.4) | 0.014 |
| Hypertension | 53 (18.4) | 60 (22.5) | 36 (17.7) | 0.500 |
| COPD | 8 (2.8) | 14 (5.2) | 15 (7.4) | 0.065 |
| Liver disease * | 46 (16) | 58 (21.7) | 33 (16.3) | 0.160 |
| Dyslipidemia | 54 (18.8) | 55 (20.6) | 41 (20.2) | 0.858 |
| Kidney disease † | 10 (3.5) | 14 (5.2) | 7 (3.4) | 0.500 |
| Spirometry | ||||
| FVC, % predicted | 89.2 ± 9.4 | 89.6 ± 8.8 | 90.2 ± 9.5 | 0.489 |
| FEV1, % predicted | 89.6 ± 9.3 | 89.0 ± 9.9 | 88.7 ± 10.7 | 0.583 |
| FEV1/FVC (%) | 81.4 ± 5.9 | 79.5 ± 5.9 | 79.3 ± 6.9 | <0.001 |
| Nutrition | ||||
| Total energy, kcal/day | 1485.6 ± 667.5 | 1417.6 ± 570.4 | 1523.4 ± 634.9 | 0.266 |
| Total protein, g/day | 51.2 ± 28.4 | 48.6 ± 22.1 | 53.1 ± 25.4 | 0.251 |
| Total fat, g/day | 31.0 ± 22.2 | 26.8 ± 15.8 | 30.8 ± 19.3 | 0.054 |
| Total carbohydrate, g/day | 246.1 ± 105.0 | 241.4 ± 101.9 | 253.7 ± 111.3 | 0.557 |
| Total calcium, mg/day | 314.2 ± 215.7 | 287.5 ± 167.9 | 306.6 ± 186.5 | 0.346 |
| Total phosphorus, mg/day | 739.8 ± 380.8 | 700.6 ± 294.4 | 759.1 ± 344.2 | 0.252 |
| Total vitamin A, ug/day | 309.3 ± 210.6 | 311.9 ± 218.0 | 344.8 ± 230.4 | 0.255 |
| Total sodium, mg/day | 1613.4 ± 1032.5 | 1578.2 ± 987.6 | 1809.8 ± 1093.8 | 0.089 |
| Vitamin B1, mg/day | 0.87 ± 0.48 | 0.82 ± 0.41 | 0.91 ± 0.46 | 0.176 |
| Vitamin C, mg/day | 60.5 ± 46.1 | 70.0 ± 59.5 | 66.7 ± 47.2 | 0.158 |
| Folate, mg/day | 141.8 ± 89.4 | 145.7 ± 96.6 | 152.8 ± 93.5 | 0.53 |
| Retinol, ug/day | 75.4 ± 63.8 | 67.0 ± 51.9 | 72.9 ± 60.6 | 0.327 |
| Fiber, g/day | 3.5 ± 2.0 | 3.7 ± 2.1 | 3.8 ± 2.1 | 0.42 |
| Cholesterol, mg/day | 171.8 ± 153.1 | 171.3 ± 138.0 | 182.6 ± 151.5 | 0.734 |
| Level | Taxonomic Assignment | w |
|---|---|---|
| Never vs. current | ||
| Phylum | k__Bacteria;p__Bacteroidetes (increased in current smokers) * | 2 |
| k__Bacteria;p__Firmicutes (decreased in current smokers) | 1 | |
| k__Bacteria;p__Proteobacteria (decreased in current smokers) | 2 | |
| Family | k__Bacteria;p__Bacteroidetes;c__Bacteroidia;o__Bacteroidales;f__Bacteroidaceae * (increased in current smokers) * | 5 |
| k__Bacteria;p__Bacteroidetes;c__Bacteroidia;o__Bacteroidales;f__Porphyromonadaceae * (increased in current smokers) * | 1 | |
| k__Bacteria;p__Firmicutes;c__Bacilli;o__Lactobacillales;f__Lactobacillaceae * (increased in current smokers) * | 3 | |
| k__Bacteria;p__Firmicutes;c__Clostridia;o__Clostridiales;f__Clostridiales_Incertae_Sedis_XII (decreased in current smokers) | 3 | |
| k__Bacteria;p__Firmicutes;c__Clostridia;o__Clostridiales;f__Gracilibacteraceae (decreased in current smoker)s | 1 | |
| k__Bacteria;p__Firmicutes;c__Clostridia;o__Clostridiales;f__Peptococcaceae (decreased in current smokers) | 6 | |
| k__Bacteria;p__Firmicutes;c__Clostridia;o__Clostridiales;f__Ruminococcaceae (decreased in current smokers) | 1 | |
| k__Bacteria;p__Fusobacteria;c__Fusobacteriia;o__Fusobacteriales;f__Fusobacteriaceae (decreased in current smokers) | 3 | |
| k__Bacteria;p__Proteobacteria;c__Betaproteobacteria;o__Burkholderiales;f__Comamonadaceae (decreased in current smokers) | 1 | |
| k__Bacteria;p__Proteobacteria;c__Gammaproteobacteria;o__Enterobacteriales;f__Enterobacteriaceae (decreased in current smokers) | 2 | |
| Former vs. current | ||
| Phylum | k__Bacteria;p__Bacteroidetes (increased in current smokers) * | 1 |
| k__Bacteria;p__Tenericutes (increased in current smokers) * | 1 | |
| k__Bacteria;p__Verrucomicrobia (decreased in current smokers) | 2 | |
| Family | None | |
| Never vs. former | ||
| Phylum | None | |
| Family | None | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.H.; Yun, Y.; Kim, S.J.; Lee, E.-J.; Chang, Y.; Ryu, S.; Shin, H.; Kim, H.-L.; Kim, H.-N.; Lee, J.H. Association between Cigarette Smoking Status and Composition of Gut Microbiota: Population-Based Cross-Sectional Study. J. Clin. Med. 2018, 7, 282. https://doi.org/10.3390/jcm7090282
Lee SH, Yun Y, Kim SJ, Lee E-J, Chang Y, Ryu S, Shin H, Kim H-L, Kim H-N, Lee JH. Association between Cigarette Smoking Status and Composition of Gut Microbiota: Population-Based Cross-Sectional Study. Journal of Clinical Medicine. 2018; 7(9):282. https://doi.org/10.3390/jcm7090282
Chicago/Turabian StyleLee, Su Hwan, Yeojun Yun, Soo Jung Kim, Eun-Ju Lee, Yoosoo Chang, Seungho Ryu, Hocheol Shin, Hyung-Lae Kim, Han-Na Kim, and Jin Hwa Lee. 2018. "Association between Cigarette Smoking Status and Composition of Gut Microbiota: Population-Based Cross-Sectional Study" Journal of Clinical Medicine 7, no. 9: 282. https://doi.org/10.3390/jcm7090282
APA StyleLee, S. H., Yun, Y., Kim, S. J., Lee, E.-J., Chang, Y., Ryu, S., Shin, H., Kim, H.-L., Kim, H.-N., & Lee, J. H. (2018). Association between Cigarette Smoking Status and Composition of Gut Microbiota: Population-Based Cross-Sectional Study. Journal of Clinical Medicine, 7(9), 282. https://doi.org/10.3390/jcm7090282