Body Fatness and Cardiovascular Health in Newborn Infants

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Body Composition and Anthropometry
2.3. Maternal and Infant Demographics
2.4. Aortic Intima-Media Thickness
2.5. Heart Rate Variability
2.6. Cardiac Ultrasound
2.7. Statistical Analysis
3. Results
3.1. Participant Characteristics
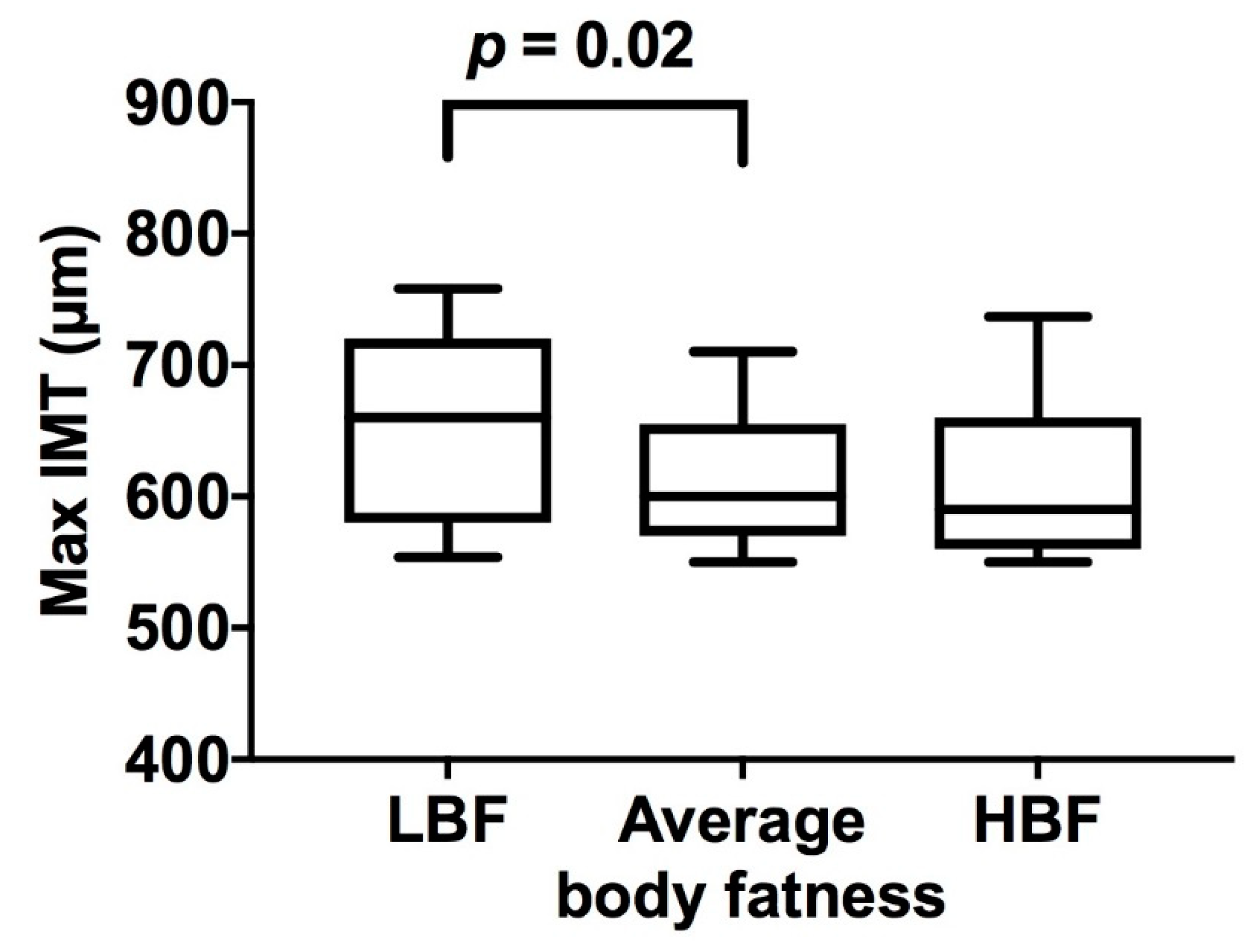
3.2. Aortic Intima-Media Thickness
3.3. Heart Rate Variability
3.4. Cardiac Structure and Function
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Naghavi, M.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Adetokunboh, O.; Arnlov, J.; Afshin, A.; et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the global burden of disease study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef]
- Huxley, R.; Owen, C.G.; Whincup, P.H.; Cook, D.G.; Rich-Edwards, J.; Smith, G.D.; Collins, R. Is birth weight a risk factor for ischemic heart disease in later life? Am. J. Clin. Nutr. 2007, 85, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Skilton, M.R.; Siitonen, N.; Würtz, P.; Viikari, J.S.A.; Juonala, M.; Seppälä, I.; Laitinen, T.; Lehtimäki, T.; Taittonen, L.; Kähönen, M.; et al. High birth weight is associated with obesity and increased carotid wall thickness in young adults: The cardiovascular risk in young finns study. Arterioscler. Thromb. Vasc. Boil. 2014, 34, 1064–1068. [Google Scholar] [CrossRef] [PubMed]
- Koklu, E.; Akcakus, M.; Kurtoglu, S.; Koklu, S.; Yikilmaz, A.; Coskun, A.; Gunes, T. Aortic intima-media thickness and lipid profile in macrosomic newborns. Eur. J. Pediatr. 2007, 166, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, J.; Forsén, T.; Tuomilehto, J.; Osmond, C.; Barker, D. Size at birth, childhood growth and obesity in adult life. Int. J. Obes. 2001, 25, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Lemini, M.; Crispi, F.; Valenzuela-Alcaraz, B.; Figueras, F.; Sitges, M.; Bijnens, B.; Gratacos, E. Fetal cardiovascular remodeling persists at 6 months in infants with intrauterine growth restriction. Ultrasound Obstet. Gynecol. 2016, 48, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, A.; Doctor, T.; Menahem, S. Cardiac function and arterial biophysical properties in small for gestational age infants: Postnatal manifestations of fetal programming. J. Pediatr. 2013, 163, 1296–1300. [Google Scholar] [CrossRef] [PubMed]
- Skilton, M.R.; Evans, N.; Griffiths, K.A.; Harmer, J.A.; Celermajer, D.S. Aortic wall thickness in newborns with intrauterine growth restriction. Lancet 2005, 365, 1484–1486. [Google Scholar] [CrossRef]
- Crispi, F.; Bijnens, B.; Figueras, F.; Bartrons, J.; Eixarch, E.; Le Noble, F.; Ahmed, A.; Gratacos, E. Fetal growth restriction results in remodeled and less efficient hearts in children. Circulation 2010, 121, 2427–2436. [Google Scholar] [CrossRef] [PubMed]
- Sarvari, S.I.; Rodriguez-Lopez, M.; Nunez-Garcia, M.; Sitges, M.; Sepulveda-Martinez, A.; Camara, O.; Butakoff, C.; Gratacos, E.; Bijnens, B.; Crispi, F. Persistence of cardiac remodeling in preadolescents with fetal growth restriction. Circ. Cardiovasc. Imaging 2017, 10, e005270. [Google Scholar] [CrossRef] [PubMed]
- Cohen, E.; Wong, F.Y.; Horne, R.S.C.; Yiallourou, S.R. Intrauterine growth restriction: Impact on cardiovascular development and function throughout infancy. Pediatr. Res. 2016, 79, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Rakow, A.; Katz-Salamon, M.; Ericson, M.; Edner, A.; Vanpée, M.; Kth. Decreased heart rate variability in children born with low birth weight. Pediatr. Res. 2013, 74, 339. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.; Gluckman, P.D.; Godfrey, K.M.; Harding, J.E.; Owens, J.A.; Robinson, J.S. Fetal nutrition and cardiovascular disease in adult life. Lancet 1993, 341, 938–941. [Google Scholar] [CrossRef]
- Shields, B.M.; Knight, B.A.; Powell, R.J.; Hattersley, A.T.; Wright, D.E. Assessing newborn body composition using principal components analysis: Differences in the determinants of fat and skeletal size. BMC Pediatr. 2006, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Catalano, P.M.; Thomas, A.; Huston-Presley, L.; Amini, S.B. Increased fetal adiposity: A very sensitive marker of abnormal in utero development. Am. J. Obstet. Gynecol. 2003, 189, 1698–1704. [Google Scholar] [CrossRef]
- Guihard-Costa, A.M.; Papiernik, E.; Kolb, S. Maternal predictors of subcutaneous fat in the term newborn. Acta Paediatr. 2004, 93, 346–349. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, C.P.; Hourihane, J.O.B.; Kenny, L.C.; Irvine, A.D.; Kiely, M.; Murray, D.M. Gender- and gestational age-specific body fat percentage at birth. Pediatrics 2011, 128, e645–e651. [Google Scholar] [CrossRef] [PubMed]
- Ma, G.; Yao, M.; Liu, Y.; Lin, A.; Zou, H.; Urlando, A.; Wong, W.W.; Nommsen-Rivers, L.; Dewey, K.G. Validation of a new pediatric air-displacement plethysmograph for assessing body composition in infants. Am. J. Clin. Nutr. 2004, 79, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Roggero, P.; Gianni, M.L.; Amato, O.; Piemontese, P.; Morniroli, D.; Wong, W.W.; Mosca, F. Evaluation of air-displacement plethysmography for body composition assessment in preterm infants. Pediatr. Res. 2012, 72, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Ellis, K.J.; Yao, M.; Shypailo, R.J.; Urlando, A.; Wong, W.W.; Heird, W.C. Body-composition assessment in infancy: Air-displacement plethysmography compared with a reference 4-compartment model. Am. J. Clin. Nutr. 2007, 85, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Skilton, M.R. Intrauterine risk factors for precocious atherosclerosis. Pediatrics 2008, 121, 570–574. [Google Scholar] [CrossRef] [PubMed]
- Begg, L.M.; Palma-Dias, R.; Wang, J.; Chin-Dusting, J.P.F.; Skilton, M.R. Maternal adiposity and newborn vascular health. Arch. Dis. Child. Fetal Neonatal Ed. 2013, 98, F279–F280. [Google Scholar] [CrossRef] [PubMed]
- Malik, M. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use: Task force of the European Society of Cardiology and the North American Society for Pacing and Electrophysiology. Ann. Noninvasive Electrocardiol. 1996, 1, 151–181. [Google Scholar] [CrossRef]
- Polson, J.W.; McCallion, N.; Waki, H.; Thorne, G.; Tooley, M.A.; Paton, J.F.R.; Wolf, A.R. Evidence for cardiovascular autonomic dysfunction in neonates with coarctation of the aorta. Circulation 2006, 113, 2844–2850. [Google Scholar] [CrossRef] [PubMed]
- Koklu, E.; Kurtoglu, S.; Akcakus, M.; Koklu, S.; Buyukkayhan, D.; Gumus, H.; Yikilmaz, A. Increased aortic intima-media thickness is related to lipid profile in newborns with intrauterine growth restriction. Horm. Res. 2006, 65, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Stergiotou, I.; Crispi, F.; Valenzuela-Alcaraz, B.; Cruz-Lemini, M.; Bijnens, B.; Gratacos, E. Aortic and carotid intima-media thickness in term small-for-gestational-age newborns and relationship with prenatal signs of severity. Ultrasound Obstet. Gynecol. 2014, 43, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Skilton, M.R.; Viikari, J.S.; Juonala, M.; Laitinen, T.; Lehtimäki, T.; Taittonen, L.; Kähönen, M.; Celermajer, D.S.; Raitakari, O.T. Fetal growth and preterm birth influence cardiovascular risk factors and arterial health in young adults: The cardiovascular risk in young finns study. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 2975–2981. [Google Scholar] [CrossRef] [PubMed]
- McCloskey, K.; Burgner, D.; Carlin, J.B.; Skilton, M.R.; Cheung, M.; Dwyer, T.; Vuillermin, P.; Ponsonby, A.L.; BIS Investigator Group. Infant adiposity at birth and early postnatal weight gain predict increased aortic intima-media thickness at 6 weeks of age: A population-derived cohort study. Clin. Sci. 2016, 130, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Davis, P.H.; Dawson, J.D.; Blecha, M.B.; Mastbergen, R.K.; Sonka, M. Measurement of aortic intimal-medial thickness in adolescents and young adults. Ultrasound Med. Boil. 2010, 36, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.W.; Markus, H.S.; Bots, M.L.; Rosvall, M.; Sitzer, M.; Lund, U.; Folkhälsa; Public, H.; Lunds, U. Prediction of clinical cardiovascular events with carotid intima-media thickness: A systematic review and meta-analysis. Circulation 2007, 115, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Souza, L.V.; Oliveira, V.; Meneck, F.D.; Ana Paula Grotti, C.; Maria Wany Louzada, S.; Maria do Carmo, F. Birth weight and its relationship with the cardiac autonomic balance in healthy children. PLoS ONE 2017, 12, e0167328. [Google Scholar] [CrossRef] [PubMed]
- Aziz, W.; Schlindwein, F.S.; Wailoo, M.; Biala, T.; Rocha, F.C. Heart rate variability analysis of normal and growth restricted children. Clin. Auton. Res. 2012, 22, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Martini, G.; Riva, P.; Rabbia, F.; Molini, V.; Ferrero, G.B.; Cerutti, F.; Carra, R.; Veglio, F. Heart rate variability in childhood obesity. Clin. Auton. Res. 2001, 11, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, A.A.; do Carmo, J.; Dubinion, J.; Hall, J.E. The role of the sympathetic nervous system in obesity-related hypertension. Curr. Hypertens. Rep. 2009, 11, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Rabbia, F.; Silke, B.; Conterno, A.; Grosso, T.; De Vito, B.; Rabbone, I.; Chiandussi, L.; Veglio, F. Assessment of cardiac autonomic modulation during adolescent obesity. Obes. Res. 2003, 11, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, A.; Allison, B.J.; Gwini, S.M.; Miller, S.L.; Polglase, G.R. Cardiac morphology and function in preterm growth restricted infants: Relevance for clinical sequelae. J. Pediatr. 2017, 188, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Verburg, B.O.; Jaddoe, V.W.; Wladimiroff, J.W.; Hofman, A.; Witteman, J.C.; Steegers, E.A. Fetal hemodynamic adaptive changes related to intrauterine growth: The generation r study. Circulation 2008, 117, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Fouzas, S.; Karatza, A.A.; Davlouros, P.A.; Chrysis, D.; Alexopoulos, D.; Mantagos, S.; Dimitriou, G. Neonatal cardiac dysfunction in intrauterine growth restriction. Pediatr. Res. 2014, 75, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Arnott, C.; Skilton, M.R.; Ruohonen, S.; Juonala, M.; Viikari, J.S.; Kahonen, M.; Lehtimaki, T.; Laitinen, T.; Celermajer, D.S.; Raitakari, O.T. Subtle increases in heart size persist into adulthood in growth restricted babies: The cardiovascular risk in young finns study. Open Heart 2015, 2, e000265. [Google Scholar] [CrossRef] [PubMed]
- Skilton, M.R. Fetal growth and the ethnic origins of type 2 diabetes. Diabetologia 2015, 58, 422–424. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Lopez, M.; Osorio, L.; Acosta-Rojas, R.; Figueras, J.; Cruz-Lemini, M.; Figueras, F.; Bijnens, B.; Gratacos, E.; Crispi, F. Influence of breastfeeding and postnatal nutrition on cardiovascular remodeling induced by fetal growth restriction. Pediatr. Res. 2016, 79, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Skilton, M.R.; Mikkila, V.; Wurtz, P.; Ala-Korpela, M.; Sim, K.A.; Soininen, P.; Kangas, A.J.; Viikari, J.S.; Juonala, M.; Laitinen, T.; et al. Fetal growth, omega-3 (n-3) fatty acids, and progression of subclinical atherosclerosis: Preventing fetal origins of disease? The cardiovascular risk in young finns study. Am. J. Clin. Nutr. 2013, 97, 58–65. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Average BF | Low BF | Low BF vs. Average BF p Value | High BF | High BF vs. Average BF p Value | Low BF vs. High BF p Value | |
|---|---|---|---|---|---|---|
| Maternal Characteristics | ||||||
| Age, years | 33 (4) | 32 (4) | 0.28 | 35 (5) | 0.14 | 0.03 |
| Pre-pregnancy BMI, kg/m2 | 23 (5) | 22 (3) | 0.34 | 24 (4) | 0.17 | 0.006 |
| Pre-pregnancy weight, Kg | 62 (12) | 57 (9) | 0.04 | 65 (11) | 0.23 | 0.001 |
| Height, cm | 166 (6) | 161 (7) | 0.002 | 167 (10) | 0.92 | 0.01 |
| Weight at first antenatal visit, kg | 63 (12) | 58 (9) | 0.04 | 67 (7) | 0.92 | <0.001 |
| Gestational Diabetes, n (%) | 11 (19) | 5 (15) | 0.78 | 4 (13) | 0.38 | 0.84 |
| Preeclampsia, n (%) | 2 (3) | 2 (6) | 0.61 | 2 (7) | 0.60 | 0.92 |
| Hypertension in pregnancy, n (%) | 2 (3) | 1 (3) | 0.93 | 1 (3) | 0.74 | 0.95 |
| Maternal smoking, n (%) | 1 (2) | 3 (10) | 0.18 | 0 (0) | 0.26 | 0.13 |
| Ethnicity, n (%) | ||||||
| Asian | 12 (20) | 5 (16) | 0.05 | 4 (13) | 0.83 | |
| Caucasian | 40 (68) | 14 (45) | 23 (77) | |||
| Middle Eastern | 1 (2) | 2 (7) | 0 (0) | 0.06 | ||
| South Asian | 3 (5) | 7 (23) | 1 (3) | |||
| Other | 3 (3) | 3 (10) | 2 (7) | |||
| Mode of birth, n (%) | ||||||
| Vaginal | 36 (61) | 20 (61) | 0.99 | 13 (43) | 0.03 | |
| Instrumental vaginal | 13 (22) | 7 (21) | 4 (13) | 0.09 | ||
| Caesarean | 10 (17) | 6 (18) | 13 (43) | |||
| Labour | ||||||
| Spontaneous | 35 (59) | 17 (52) | 0.76 | 10 (33) | 0.001 | |
| Induced | 19 (32) | 13 (39) | 7 (23) | 0.008 | ||
| No Labour | 5 (9) | 3 (9) | 13 (43) | |||
| Infant Characteristics | ||||||
| NICU admissions, n (%) | 3 (6) | 4 (13) | 0.42 | 2 (7) | 0.60 | 0.41 |
| Postnatal age, days | 2 (1) | 3 (2) | 0.19 | 2 (2) | 0.69 | 0.42 |
| Gestational age, weeks | 39.3 (1.2) | 38.7 (0.9) | 0.01 | 39.2 (1.3) | 0.61 | 0.09 |
| Sex, female/male | 33/26 | 18/15 | 1.00 | 15/15 | 0.66 | 0.72 |
| Birth weight, g | 3386 (412) | 2916 (360) | <0.001 | 3983 (435) | <0.001 | <0.001 |
| Apgar score at 1 min | 8.7 (0.84) | 8.2 (1.7) | 0.14 | 8.9 (0.57) | 0.26 | 0.05 |
| Apgar score at 5 min | 9.0 (0.23) | 8.8 (0.58) | 0.07 | 9.0 (0.18) | 0.30 | 0.17 |
| Length, cm | 50 (2) | 48 (2) | <0.001 | 51 (2) | <0.001 | <0.001 |
| Head circumference, cm | 35 (1) | 34 (1) | 0.004 | 36 (1) | <0.001 | <0.001 |
| Body fat, % | 11 (2) | 4 (2) | <0.001 | 18 (2) | <0.001 | <0.001 |
| Low BF (Relative to Average BF) | High BF (Relative to Average BF) | High BF (Relative to Low BF) | ||||
|---|---|---|---|---|---|---|
| β (95% CI) | p Value | β (95% CI) | p Value | β (95% CI) | p Value | |
| Aortic IMT | n = 31 | n = 30 | ||||
| Maximum IMT, µm | 43 (7, 78) | 0.02 | −2 (−37, 33) | 0.91 | −49 (−91, −8) | 0.02 |
| HRV (frequency domain) | n = 25 | n = 26 | ||||
| Ln Total Power | −0.5 (−0.8, −0.1) | 0.01 | −0.8 (−1.1, −0.5) | <0.001 | −0.3 (−0.7, 0.1) | 0.16 |
| Ln LF | −0.3 (−0.7, 0.1) | 0.18 | −0.8 (−1.1, −0.4) | <0.001 | −0.4 (−0.9, −0.0) | 0.05 |
| Ln HF | −0.2 (−0.7, 0.3) | 0.51 | −1.0 (−1.4, −0.4) | <0.001 | −0.7 (−1.2, −0.1) | 0.02 |
| Ln LF: HF | −0.2 (−0.6, 0.2) | 0.38 | 0.3 (−0.1, 0.8) | 0.15 | 0.5 (−0.1, 1.0) | 0.12 |
| HRV (time domain) | n = 25 | n = 26 | ||||
| HR, bpm | −0.5 (−9.3, 8.4) | 0.92 | 4.4 (−4.3, 13.1) | 0.32 | 3.0 (−7.1, 13.2) | 0.55 |
| Mean NN, ms | 11.4 (−20.9, 43.8) | 0.48 | −18.3 (−50.0, 13.4) | 0.25 | −23.1 (−60.9, 14.8) | 0.23 |
| SDNN, ms | −7.1 (−13.2, −1.0) | 0.02 | −11.2 (−17.2, −5.3) | <0.001 | −3.0 (−9.7, 3.6) | 0.36 |
| Ln SD∆NN | −0.1 (−0.4, 0.2) | 0.52 | −0.5 (−0.7, −0.2) | 0.02 | −0.3 (−0.6, 0.0) | 0.06 |
| Ln RMSSD | −0.1 (−0.4, 0.2) | 0.39 | −0.4 (−0.7, −0.1) | 0.004 | −0.2 (−0.5, 0.1) | 0.14 |
| Cardiac structure | n = 22 | n = 23 | ||||
| LV Base to apex length, mm | −1.3 (−3.1, 0.3) | 0.11 | 2.1 (0.3, 3.8) | 0.02 | 3.8 (1.2, 6.2) | 0.01 |
| LV Diameter, mm | −0.9 (−2.0, 0.3) | 0.13 | 0.1 (−1.1, 1.3) | 0.89 | 1.0 (−0.8, 2.7) | 0.27 |
| LV Sphericity index | 0.1 (−0.1, 0.2) | 0.46 | 0.2 (−0.0, 0.3) | 0.09 | −0.0 (−0.2, 0.2) | 0.93 |
| Septal wall thickness mm/BSA | 2.3 (0.5, 4.1) | 0.01 | −0.0 (−1.8, 1.7) | 0.99 | −2.5 (−4.9, 0.1) | 0.06 |
| Posterior wall thickness mm/BSA | 3.1 (1.6, 4.6) | <0.001 | −1.0 (−2.4, 0.5) | 0.18 | −4.1 (−5.8, −2.4) | <0.001 |
| End-diastolic dimension mm/BSA | 5.5 (1.4, 9.7) | 0.01 | −3.0 (−7.1, 1.0) | 0.14 | −9.0 (−14.0. −4.0) | 0.001 |
| Relative wall thickness | 0.03 (−0.00, 0.7) | 0.08 | −0.01 (−0.04, 0.03) | 0.71 | −0.04 (−0.08, 0.01) | 0.09 |
| RV Base to apex length, mm | −0.8 (−2.6, 1.0) | 0.36 | 2.0 (0.4, 3.7) | 0.02 | 2.9 (0.5, 5.4) | 0.02 |
| RV Diameter, mm | −0.7 (−1.7, 0.4) | 0.19 | 0.4 (−0.5, 1.4) | 0.38 | 1.2 (0.1, 2.2) | 0.03 |
| RV Sphericity index | 0.0 (−0.1, 0.2) | 0.87 | 0.1 (−0.1, 0.2) | 0.23 | 0.3 (−0.2, 0.7) | 0.24 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dissanayake, H.U.; McMullan, R.L.; Kong, Y.; Caterson, I.D.; Celermajer, D.S.; Phang, M.; Raynes-Greenow, C.; Polson, J.W.; Gordon, A.; Skilton, M.R. Body Fatness and Cardiovascular Health in Newborn Infants. J. Clin. Med. 2018, 7, 270. https://doi.org/10.3390/jcm7090270
Dissanayake HU, McMullan RL, Kong Y, Caterson ID, Celermajer DS, Phang M, Raynes-Greenow C, Polson JW, Gordon A, Skilton MR. Body Fatness and Cardiovascular Health in Newborn Infants. Journal of Clinical Medicine. 2018; 7(9):270. https://doi.org/10.3390/jcm7090270
Chicago/Turabian StyleDissanayake, Hasthi U., Rowena L. McMullan, Yang Kong, Ian D. Caterson, David S. Celermajer, Melinda Phang, Camille Raynes-Greenow, Jaimie W. Polson, Adrienne Gordon, and Michael R. Skilton. 2018. "Body Fatness and Cardiovascular Health in Newborn Infants" Journal of Clinical Medicine 7, no. 9: 270. https://doi.org/10.3390/jcm7090270
APA StyleDissanayake, H. U., McMullan, R. L., Kong, Y., Caterson, I. D., Celermajer, D. S., Phang, M., Raynes-Greenow, C., Polson, J. W., Gordon, A., & Skilton, M. R. (2018). Body Fatness and Cardiovascular Health in Newborn Infants. Journal of Clinical Medicine, 7(9), 270. https://doi.org/10.3390/jcm7090270