Pre-Operative Frailty Status Is Associated with Cardiac Rehabilitation Completion: A Retrospective Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Ethics and Study Population
2.3. Cardiac Rehabilitation Program
2.4. Measurements and Outcomes
2.4.1. Frailty Assessment
2.4.2. Primary Outcome
2.4.3. Secondary Outcomes
2.5. Statistical Analysis
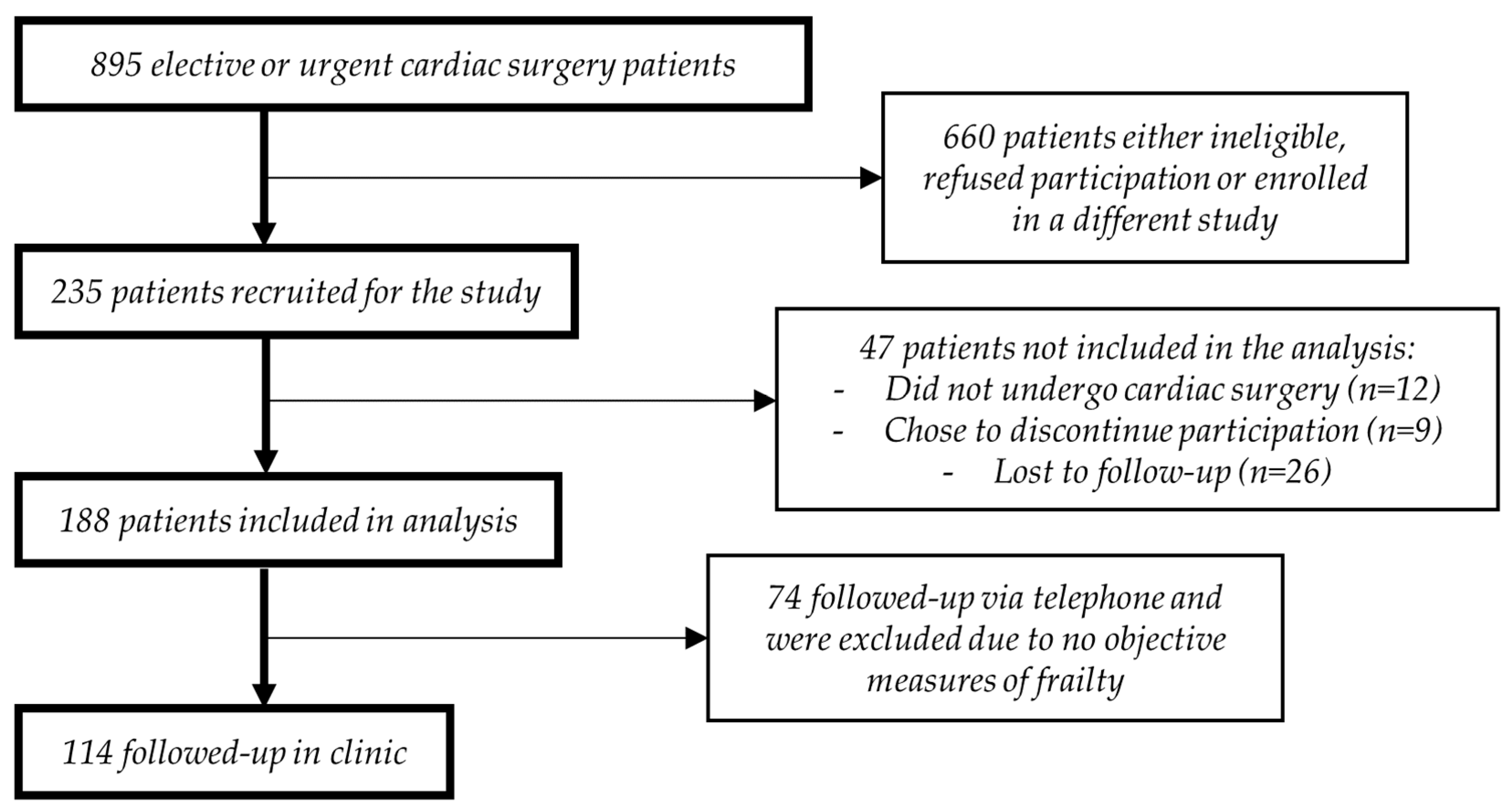
3. Results
3.1. Baseline Characteristics
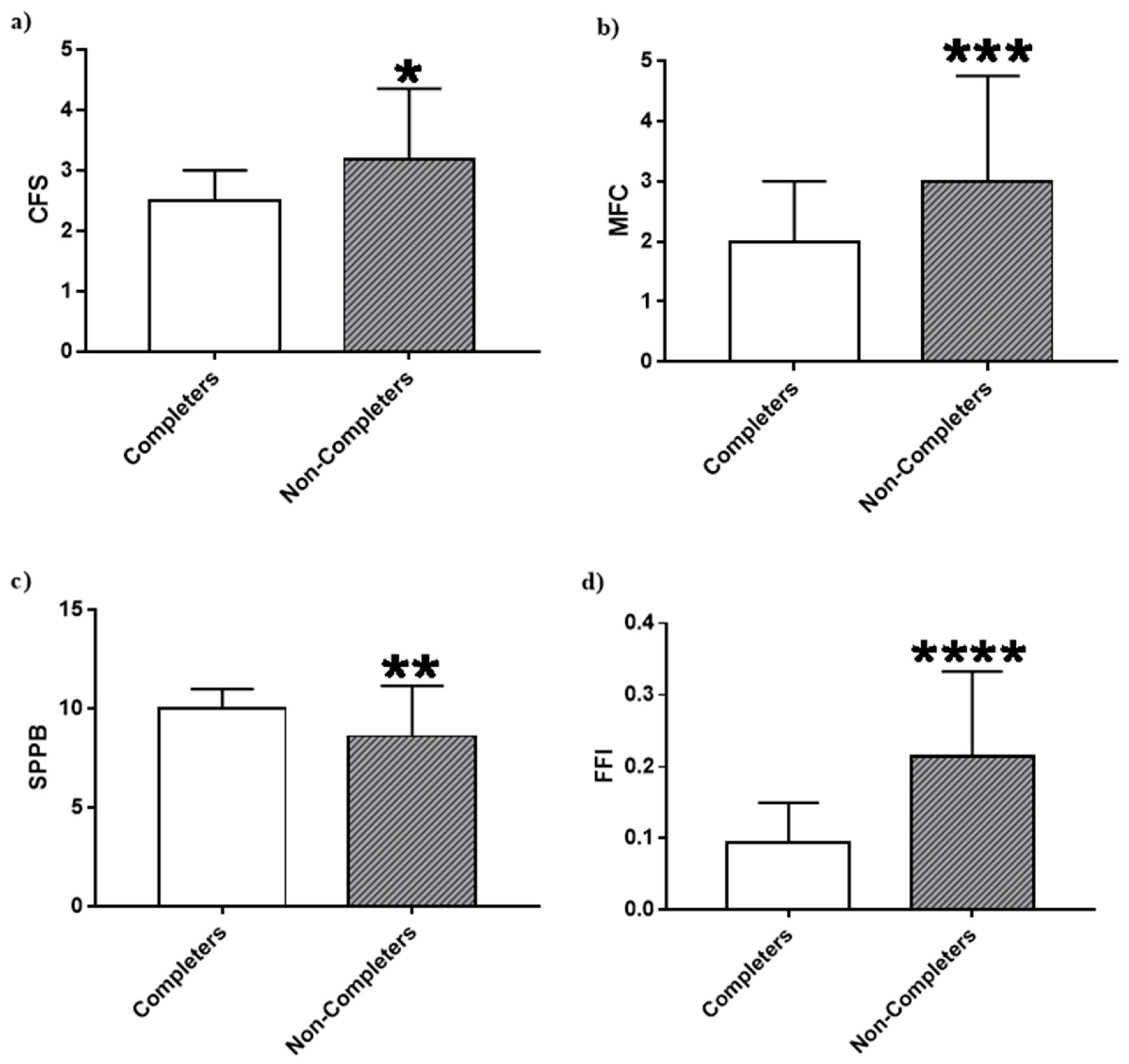
3.2. Pre-Operative Frailty and Post-Operative CR Completion
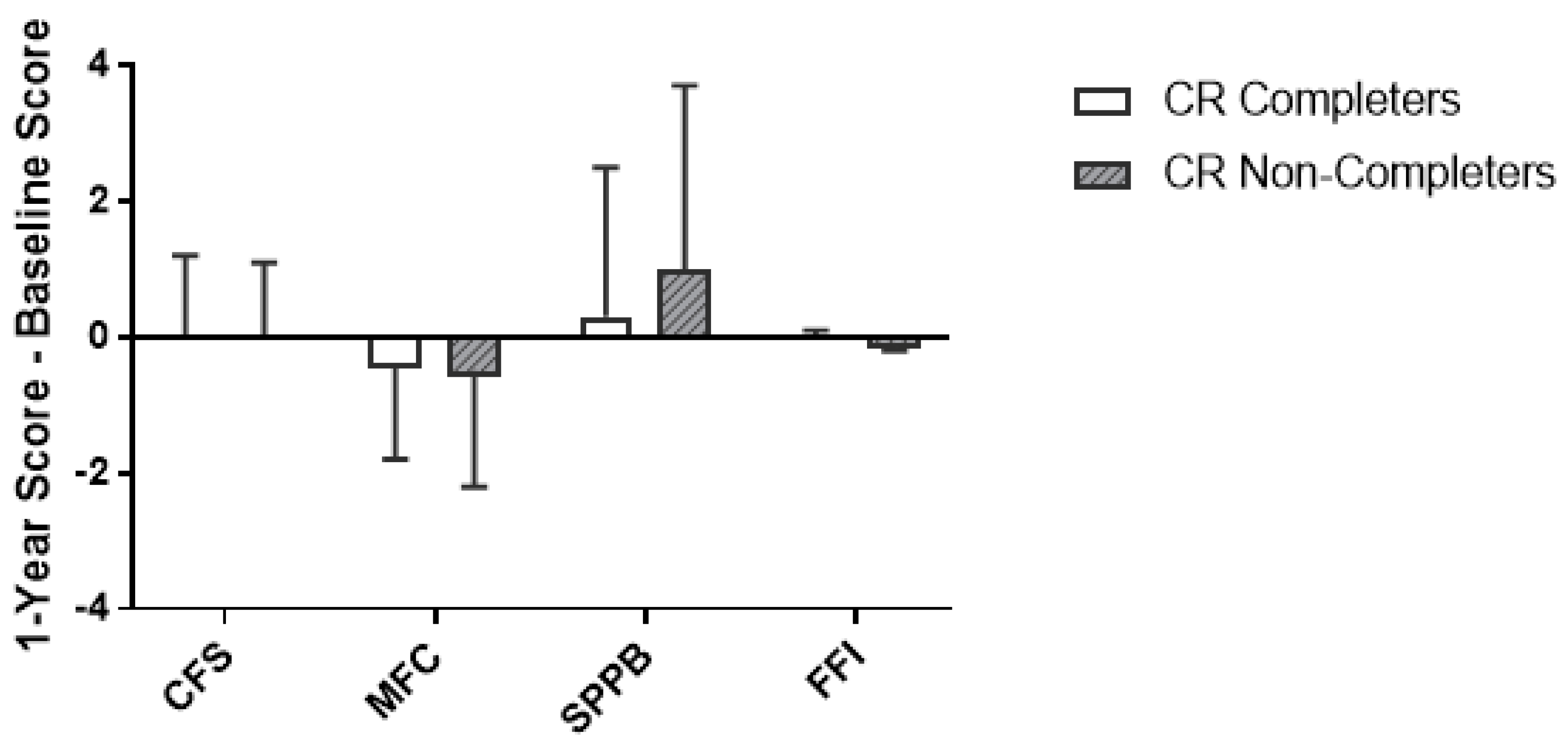
3.3. Changes in Frailty
3.4. Changes in Frailty Domains
3.5. CR Attendance and Frailty
4. Discussion
4.1. CR and ∆Frailty
4.2. Frailty Domains
4.3. CR Attendance
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Domain | Tool Used to Measure | Variable | Cut-Off Point | References/Justification | |
|---|---|---|---|---|---|
| 1 | Physical | SPPB | Balance (Side-by-side, semi-tandem, tandem) | Unable to complete = 1 Side-by-Side = 0.67 Semi-Tandem = 0.33 Tandem = 0 | Participants unable to hold side by side stance for 10 seconds (HR: 3.54 95% CI 3.04–4.13) and those unable to hold semi-tandem stance for 10 seconds (HR: 1.78 95% CI 1.51–2.09) more likely to die compared to those able to complete the tandem balance task [52]. |
| 2 | Physical | SPPB | Chair Stand | Unable = 1 ≥16.7 s = 0.75 13.7–16.6 s = 0.5 11.2–13.6 s = 0.25 ≤11.1 s = 0 | Compared to participants in the highest quartile, those in the lowest quartile (HR: 1.96 95% CI 1.56–2.46), second quartile (HR: 1.40 95% CI 1.18–1.66) and third quartile (HR: 1.24 95% CI 1.08–1.42) at a higher risk of mortality [52]. |
| 3 | Physical | Fried Criteria | 5-meter Gait Speed | Males Height >173 cm: GS ≤6.56 s = 1, GS >6.56 s = 0 Height ≤173 cm: GS ≤7.66 s = 1, GS >7.66 s = 0 Females Height >159 cm: GS ≤6.56 s = 1, GS > 6.56 s = 0 Height ≤159 cm: GS ≤7.66 s = 1, GS >7.66 s = 0 | Gait speed associated with survival (HR per 0.1 m/sec: 0.88 95% CI 0.87–0.90) [17,53]. |
| 4 | Physical | Timed Up-and-Go | Mobility | Freely mobile ≤10 s = 0 Mostly independent 11–20 s = 0.25 Variable mobility 21–29 s = 0.75 Impaired mobility ≥30 s = 1 | [54,55] |
| 5 | Physical | Paffenbarger Physical Activity Questionnaire | Self-Report Physical Activity | Males <383 kcal/week = 1 ≥383 kcal/week = 0 Females <270 kcal/week = 1 ≥270 kcal/week = 0 | Questionnaires providing measures of activity in kcal/week recommended in frailty assessment using these cut-offs [56]. Confirmed validity of the Paffenbarger Physical Activity Questionnaire in community-dwelling adults [57]. |
| 6 | Functional | OARS Functional Assessment Questionnaire | Help Eating | Dependent = 1, Assisted = 0.5, Independent = 0 | [58] |
| 7 | Functional | OARS Functional Assessment Questionnaire | Help Dressing | Dependent = 1, Assisted = 0.5, Independent = 0 | [58] |
| 8 | Functional | OARS Functional Assessment Questionnaire | Help Cleaning | Dependent = 1, Assisted = 0.5, Independent = 0 | [58] |
| 9 | Functional | OARS Functional Assessment Questionnaire | Help Bathing | Dependent = 1, Assisted = 0.5, Independent = 0 | [58] |
| 10 | Functional | OARS Functional Assessment Questionnaire | Help Toileting | Dependent = 1, Assisted = 0.5, Independent = 0 | [58] |
| 11 | Functional | OARS Functional Assessment Questionnaire | Help Shopping | Dependent = 1, Assisted = 0.5, Independent = 0 | [58] |
| 12 | Functional | OARS Functional Assessment Questionnaire | Help Cooking | Dependent = 1, Assisted = 0.5, Independent = 0 | [58] |
| 13 | Functional | OARS Functional Assessment Questionnaire | Help Driving | Dependent = 1, Assisted = 0.5, Independent = 0 | [58] |
| 14 | Functional | OARS Functional Assessment Questionnaire | Help Taking Medication | Dependent = 1, Assisted = 0.5, Independent = 0 | [58] |
| 15 | Functional | OARS Functional Assessment Questionnaire | Help Banking | Dependent = 1, Assisted = 0.5, Independent = 0 | [58] |
| 16 | Exhaustion | CES-D | Feel everything is an effort | Most of the time = 1, Some of the time = 0.5, Rarely = 0 | [58] |
| 17 | Exhaustion | CES-D | Have trouble getting going | Most of the time = 1, Some of the time = 0.5, Rarely = 0 | [58] |
| 18 | Nutrition | Self-Report | Unintentional weight loss in Past 3 months | Yes = 1, No = 0 | [33] |
| 19 | Nutrition | Self-Report | Unintentional weight loss more than 10 lbs in the past year | Yes = 1, No = 0 | [58] |
| 20 | Nutrition | Self-Report | Decline in food intake in past 3 months | Severe decrease = 1, Moderate decrease = 0.5, None = 0 | [33] |
| 21 | Quality of life | Self-report | Rating of own health | Very poor = 1 Poor = 0.8 Average = 0.6 Good = 0.4 Very good = 0.2 | [58] |
| 22 | Depression | HADS —Just using depression score | HADS | Depression 11–21 = 1 8–10 = 0.5 0–7 = 0 | [59] |
| 23 | Anxiety | HADS —Just using anxiety score | HADS | Anxiety 11–21 = 1 8–10 = 0.5 0–7 = 0 | [59] |
| 24 | Cognition | MoCA | MoCA | ≥26 = 1 ≤25 = 0 | As per MoCA scoring protocol, a cut-off score of 26 has a sensitivity of 90% and a specificity of 87% in identifying mild cognitive impairment. This is a clinical state that often progresses to dementia [60]. |
| 25 | Falling | FES | Falling concern | ≥19 = 1 <19 = 0 | [61] |
| Odds Ratio | 95% Confidence Interval | p-Value | |
|---|---|---|---|
| CFS | |||
| Univariable Regression | |||
| Baseline Clinical Frailty Scale (Per Point Increase) | 0.62 | 0.43–0.88 | 0.008 |
| Multivariable Regression | |||
| Age | 0.98 | 0.92–1.04 | 0.473 |
| EuroSCORE II (%) | 1.01 | 0.95–1.08 | 0.686 |
| Baseline Clinical Frailty Scale (Per Point Increase) | 0.65 | 0.44–0.96 | 0.030 |
| MFC | |||
| Univariable Regression | |||
| Baseline Modified Fried Score (Per Point Increase) | 0.66 | 0.51–0.84 | 0.001 |
| Multivariable Regression | |||
| Age | 0.97 | 0.92–1.04 | 0.408 |
| EuroSCORE II (%) | 1.01 | 0.95–1.08 | 0.743 |
| Baseline Modified Fried Score (Per Point Increase) | 0.68 | 0.52–0.88 | 0.003 |
| SPPB | |||
| Univariable Regression | |||
| Baseline SPPB Score (Per Point Increase) | 1.21 | 1.02–1.44 | 0.034 |
| Multivariable Regression | |||
| Age | 0.96 | 0.91–1.02 | 0.217 |
| EuroSCORE II (%) | 1.01 | 0.95–1.07 | 0.820 |
| Baseline SPPB Score (Per Point Increase) | 1.17 | 0.98–1.41 | 0.084 |
| FFI | |||
| Univariable Regression | |||
| Baseline FFI (Per 0.10 Increase) | 0.41 | 0.26–0.64 | <0.001 |
| Multivariable Regression | |||
| Age | 0.99 | 0.92–1.05 | 0.666 |
| EuroSCORE II (%) | 1.02 | 0.95–1.09 | 0.684 |
| Baseline FFI (Per 0.10 Increase) | 0.41 | 0.26–0.67 | <0.001 |
References
- Statistics Canada. Canadians in Context—Aging Population. Available online: https://www150-statcan-gc-ca.uml.idm.oclc.org/n1/pub/11-402-x/2010000/chap/pop/pop02-eng.htm (accessed on 24 October 2018).
- Ferguson, T.B.; Hammill, B.G.; Peterson, E.D.; DeLong, E.R.; Grover, F.L.; STS National Database Committee. A decade of change—risk profiles and outcomes for isolated coronary artery bypass grafting procedures, 1990–1999: A report from the STS National Database Committee and the Duke Clinical Research Institute. Society of Thoracic Surgeons. Ann. Thorac. Surg. 2002, 73, 480–489. [Google Scholar] [PubMed]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef]
- Lytwyn, J.; Stammers, A.N.; Kehler, D.S.; Jung, P.; Alexander, B.; Hiebert, B.M.; Dubiel, C.; Kimber, D.; Hamm, N.; Clarke, M.; et al. The impact of frailty on functional survival in patients 1 year after cardiac surgery. J. Thorac. Cardiovasc. Surg. 2017, 154, 1990–1999. [Google Scholar] [CrossRef] [PubMed]
- Sepehri, A.; Beggs, T.; Hassan, A.; Rigatto, C.; Shaw-Daigle, C.; Tangri, N.; Arora, R.C. The impact of frailty on outcomes after cardiac surgery: A systematic review. J. Thorac. Cardiovasc. Surg. 2014, 148, 3110–3117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szalewska, D.; Tomaszewski, J.; Kusiak-Kaczmarek, M.; Niedoszytko, P.; Gierat-Haponiuk, K.; Haponiuk, I.; Bakuła, S. Influence of a hybrid form of cardiac rehabilitation on exercise tolerance in coronary artery disease patients with and without diabetes. Kardiol. Pol. 2015, 73, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Goel, K.; Lennon, R.J.; Tilbury, R.T.; Squires, R.W.; Thomas, R.J. Impact of cardiac rehabilitation on mortality and cardiovascular events after percutaneous coronary intervention in the community. Circulation 2011, 123, 2344–2352. [Google Scholar] [CrossRef]
- Taylor, R.S.; Brown, A.; Ebrahim, S.; Jolliffe, J.; Noorani, H.; Rees, K.; Skidmore, B.; Stone, J.A.; Thompson, D.R.; Oldridge, N. Exercise-based rehabilitation for patients with coronary heart disease: Systematic review and meta-analysis of randomized controlled trials. Am. J. Med. 2004, 116, 682–692. [Google Scholar] [CrossRef]
- Cardiac Sciences Program. Available online: http://www.umanitoba.ca/faculties/health_sciences/medicine/units/cardiac_sciences/Cardiac%20Rehab%20Report%2020152016/Cardiac%20Rehab%20Report.htm (accessed on 31 December 2016).
- Vigorito, C.; Abreu, A.; Ambrosetti, M.; Belardinelli, R.; Corrà, U.; Cupples, M.; Davos, C.H.; Hoefer, S.; Iliou, M.-C.; Schmid, J.-P.; et al. Frailty and cardiac rehabilitation: A call to action from the EAPC Cardiac Rehabilitation Section. Eur. J. Prev. Cardiol. 2017, 24, 577–590. [Google Scholar] [CrossRef]
- Muscedere, J.; Andrew, M.K.; Bagshaw, S.M.; Estabrooks, C.; Hogan, D.; Holroyd-Leduc, J.; Howlett, S.; Lahey, W.; Maxwell, C.; McNally, M.; et al. Canadian Frailty Network (CFN) Screening for Frailty in Canada’s Health Care System: A Time for Action. Can. J. Aging 2016, 35, 281–297. [Google Scholar] [CrossRef]
- Canadian Frailty Network—Geriatric Research. Available online: http://www.cfn-nce.ca/engaging-canadians/helping-to-set-frailty-priorities/top-ten-frailty-priorities-identified-by-citizens/ (accessed on 3 April 2018).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- CACPR-Guidelines. Available online: https://cacpr.ca/Guidelines (accessed on 11 December 2018).
- Morley, J.E.; Vellas, B.; van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.C.; Doehner, W.; Evans, J.; et al. Frailty consensus: A call to action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Bergman, H.; Ferrucci, L.; Guralnik, J.; Hogan, D.B.; Hummel, S.; Karunananthan, S.; Wolfson, C. Frailty: An emerging research and clinical paradigm—Issues and controversies. J. Gerontol. Med. Sci. 2007, 62, 731–737. [Google Scholar] [CrossRef]
- Da Câmara, S.M.A.; Alvarado, B.E.; Guralnik, J.M.; Guerra, R.O.; Maciel, A.C.C. Using the Short Physical Performance Battery to screen for frailty in young-old adults with distinct socioeconomic conditions. Geriatr. Gerontol. Int. 2013, 13, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of deficits as a proxy measure of aging. Sci. World J. 2001, 1, 323–336. [Google Scholar] [CrossRef]
- Rockwood, K.; Mitnitski, A. Frailty in relation to the accumulation of deficits. J. Gerontol. Med. Sci. 2007, 62, 722–727. [Google Scholar] [CrossRef]
- Grace, S.L.; Poirier, P.; Norris, C.M.; Oakes, G.H.; Somanader, D.S.; Suskin, N.; Canadian Association of Cardiac Rehabilitation. Pan-Canadian development of cardiac rehabilitation and secondary prevention quality indicators. Can. J. Cardiol. 2014, 30, 945–948. [Google Scholar] [CrossRef]
- Martin, B.-J.; Hauer, T.; Arena, R.; Austford, L.D.; Galbraith, P.D.; Lewin, A.M.; Knudtson, M.L.; Ghali, W.A.; Stone, J.A.; Aggarwal, S.G. Cardiac rehabilitation attendance and outcomes in coronary artery disease patients. Circulation 2012, 126, 677–687. [Google Scholar] [CrossRef]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice, 3rd ed.; Pearson Education Inc.: Upper Saddle River, NJ, USA, 2009. [Google Scholar]
- Government of Canada, C.I. of H.R. Health Research Roadmap II: Capturing Innovation to Produce Better Health and Health Care for Canadians—CIHR. Available online: http://www.cihr-irsc.gc.ca/e/48964.html#a4 (accessed on 27 October 2016).
- Ad, N.; Holmes, S.D.; Halpin, L.; Shuman, D.J.; Miller, C.E.; Lamont, D. The Effects of Frailty in Patients Undergoing Elective Cardiac Surgery. J. Card. Surg. 2016, 31, 187–194. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.H.; Buth, K.J.; Martin, B.-J.; Yip, A.M.; Hirsch, G.M. Frail patients are at increased risk for mortality and prolonged institutional care after cardiac surgery. Circulation 2010, 121, 973–978. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.-S.; Watts, J.N.; Peel, N.M.; Hubbard, R.E. Frailty and post-operative outcomes in older surgical patients: A systematic review. BMC Geriatr. 2016, 16, 157. [Google Scholar] [CrossRef] [PubMed]
- Murphy, B.M.; Elliott, P.C.; Le Grande, M.R.; Higgins, R.O.; Ernest, C.S.; Goble, A.J.; Tatoulis, J.; Worcester, M.U.C. Living alone predicts 30-day hospital readmission after coronary artery bypass graft surgery. Eur. J. Prev. Cardiovasc. 2008, 15, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Yamanashi, H.; Shimizu, Y.; Nelson, M.; Koyamatsu, J.; Nagayoshi, M.; Kadota, K.; Tamai, M.; Ariyoshi, K.; Maeda, T. The association between living alone and frailty in a rural Japanese population: The Nagasaki Islands study. J. Prim. Health Care 2015, 7, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H.J.; Smith, D.; Sun, C.-L.; Tew, W.; Mohile, S.G.; Owusu, C.; Klepin, H.D.; Gross, C.P.; Lichtman, S.M.; Gajra, A.; et al. Frailty as determined by a comprehensive geriatric assessment-derived deficit-accumulation index in older patients with cancer who receive chemotherapy. Cancer 2016, 122, 3865–3872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heran, B.S.; Chen, J.M.; Ebrahim, S.; Moxham, T.; Oldridge, N.; Rees, K.; Thompson, D.R.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2011, 7, CD001800. [Google Scholar] [CrossRef]
- Jung, P.; Pereira, M.A.; Hiebert, B.; Song, X.; Rockwood, K.; Tangri, N.; Arora, R.C. The impact of frailty on postoperative delirium in cardiac surgery patients. J. Thorac. Cardiovasc. Surg. 2015, 149, 869–875. [Google Scholar] [CrossRef]
- Dedeyne, L.; Deschodt, M.; Verschueren, S.; Tournoy, J.; Gielen, E. Effects of multi-domain interventions in (pre)frail elderly on frailty, functional, and cognitive status: A systematic review. Clin. Interv. Aging 2017, 12, 873–896. [Google Scholar] [CrossRef]
- Sutton, J.L.; Gould, R.L.; Daley, S.; Coulson, M.C.; Ward, E.V.; Butler, A.M.; Nunn, S.P.; Howard, R.J. Psychometric properties of multicomponent tools designed to assess frailty in older adults: A systematic review. BMC Geriatr. 2016, 16, 55. [Google Scholar] [CrossRef]
- Aguayo, G.A.; Vaillant, M.T.; Donneau, A.-F.; Schritz, A.; Stranges, S.; Malisoux, L.; Chioti, A.; Guillaume, M.; Muller, M.; Witte, D.R. Comparative analysis of the association between 35 frailty scores and cardiovascular events, cancer, and total mortality in an elderly general population in England: An observational study. PLoS Med. 2018, 15, e1002543. [Google Scholar] [CrossRef]
- De Vries, N.M.; Staal, J.B.; van Ravensberg, C.D.; Hobbelen, J.S.M.; Olde Rikkert, M.G.M.; Nijhuis-van der Sanden, M.W.G. Outcome instruments to measure frailty: A systematic review. Ageing Res. Rev. 2011, 10, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Buta, B.J.; Walston, J.D.; Godino, J.G.; Park, M.; Kalyani, R.R.; Xue, Q.-L.; Bandeen-Roche, K.; Varadhan, R. Frailty assessment instruments: Systematic characterization of the uses and contexts of highly-cited instruments. Ageing Res. Rev. 2016, 26, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Lautenschlager, N.T.; Almeida, O.P. Physical activity and cognition in old age. Curr. Opin. Psychiatry 2006, 19, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Angevaren, M.; Aufdemkampe, G.; Verhaar, H.J.J.; Aleman, A.; Vanhees, L. Physical activity and enhanced fitness to improve cognitive function in older people without known cognitive impairment. Cochrane Database Syst. Rev. 2008, 3, CD005381. [Google Scholar] [CrossRef]
- Lautenschlager, N.T.; Cox, K.L.; Flicker, L.; Foster, J.K.; van Bockxmeer, F.M.; Xiao, J.; Greenop, K.R.; Almeida, O.P. Effect of physical activity on cognitive function in older adults at risk for Alzheimer disease: A randomized trial. JAMA 2008, 300, 1027–1037. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Britton, A.R.; Marmot, M. Vascular disease and cognitive function: Evidence from the Whitehall II Study. J. Am. Geriatr. Soc. 2003, 51, 1445–1450. [Google Scholar] [CrossRef]
- Samper-Ternent, R.; Al Snih, S.; Raji, M.A.; Markides, K.S.; Ottenbacher, K.J. Relationship between frailty and cognitive decline in older Mexican Americans. J. Am. Geriatr. Soc. 2008, 56, 1845–1852. [Google Scholar] [CrossRef] [PubMed]
- Van Iersel, M.B.; Munneke, M.; Esselink, R.A.J.; Benraad, C.E.M.; Olde-Rikkert, M.G.M. Gait velocity and the Timed-Up-and-Go test were sensitive to changes in mobility in frail elderly patients. J. Clin. Epidemiol. 2008, 61, 186–191. [Google Scholar] [CrossRef]
- Suaya, J.A.; Stason, W.B.; Ades, P.A.; Normand, S.-L.T.; Shepard, D.S. Cardiac rehabilitation and survival in older coronary patients. J. Am. Coll. Cardiol. 2009, 54, 25–33. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Boxer, R.S.; Wang, Z.; Walsh, S.J.; Hager, D.; Kenny, A.M. The utility of the 6-minute walk test as a measure of frailty in older adults with heart failure. Am. J. Geriatr. Cardiol. 2008, 17, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Sawatzky, J.-A.V.; Kehler, D.S.; Ready, A.E.; Lerner, N.; Boreskie, S.; Lamont, D.; Luchik, D.; Arora, R.C.; Duhamel, T.A. Prehabilitation program for elective coronary artery bypass graft surgery patients: A pilot randomized controlled study. Clin. Rehabil. 2014, 28, 648–657. [Google Scholar] [CrossRef] [PubMed]
- Ramadi, A.; Buijs, D.M.; Threlfall, T.G.; Aggarwal, S.G.; Arena, R.; Rodgers, W.M.; Haennel, R.G. Long-term Physical Activity Behavior After Completion of Traditional Versus Fast-track Cardiac Rehabilitation. J. Cardiovasc. Nurs. 2016, 31, E1–E7. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.M.; Dolansky, M.A.; Ruland, C.M.; Pashkow, F.J.; Blackburn, G.G. Predictors of women’s exercise maintenance after cardiac rehabilitation. J. Cardpulm. Rehabil. 2003, 23, 40–49. [Google Scholar] [CrossRef]
- Kehler, D.S.; Kent, D.; Beaulac, J.; Strachan, L.; Wangasekara, N.; Chapman, S.; Hiebert, B.; Lamont, D.; Lerner, N.; Boreskie, S.; et al. Examining Patient Outcome Quality Indicators Based on Wait Time From Referral to Entry Into Cardiac Rehabilitation: A pilot observational study. J. Cardiopulm. Rehabil. Prev. 2017, 37, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait Speed and Survival in Older Adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Mathias, S.; Nayak, U.S.; Isaacs, B. Balance in elderly patients: The “get-up and go” test. Arch. Phys. Med. Rehabil. 1986, 67, 387–389. [Google Scholar]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Afilalo, J.; Alexander, K.P.; Mack, M.J.; Maurer, M.S.; Green, P.; Allen, L.A.; Popma, J.J.; Ferrucci, L.; Forman, D.E. Frailty Assessment in the Cardiovascular Care of Older Adults. J. Am. Coll. Cardiol. 2014, 63, 747–762. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Leon, A.S.; Jacobs, D.R.; Montoye, H.J.; Sallis, J.F.; Paffenbarger, R.S. Compendium of physical activities: Classification of energy costs of human physical activities. Med. Sci. Sports Exerc. 1993, 25, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Searle, S.D.; Mitnitski, A.; Gahbauer, E.A.; Gill, T.M.; Rockwood, K. A standard procedure for creating a frailty index. BMC Geriatr. 2008, 8, 24. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Richman, D.; Powell, L. Falls efficacy as a measure of fear of falling. J. Gerontol. 1990, 45, P239–P243. [Google Scholar] [CrossRef] [PubMed]



| Tool | Variables Considered | Frailty Cut Point |
|---|---|---|
| CFS | Subjective 9-point scale | ≥4 points out of 9 |
| MFC | Slowness, weakness, weight loss, exhaustion, depression, low physical activity, cognitive impairment | ≥3 of the 7 variables present |
| SPPB | 5 m gait speed, balance tests, repeated chair stand test | ≤9 points out of 12 |
| FFI | 25 separate variables (Table A1) | deficits/variables ≥0.25 |
| CR Completers (n = 48) | CR Non-Completers (n = 66) | p-Value | |
|---|---|---|---|
| Demographics | |||
| Age | 70.5 (66–72) | 71.5 (66.3–78) | 0.08 |
| Sex (Female) | 18 (38%) | 24 (36%) | 0.29 |
| BMI (kg/m2) | 29.0 (25.0–31.6) | 28.3 (25.4–32.2) | 0.90 |
| Lives Alone | 6 (13%) | 20 (30%) | 0.02 |
| Education (College or more) | 25 (52%) | 23 (35%) | 0.07 |
| Smoker (Never smoked) | 19 (40%) | 28 (42%) | 0.71 |
| Pre-Surgery Risk | |||
| EuroSCORE II | 1.26 (1–2.1) | 1.77 (1.2–3.0) | 0.07 |
| Comorbidities | |||
| Previous MI | 11 (23%) | 23 (35%) | 0.17 |
| CHF | 23 (48%) | 33 (50%) | 0.70 |
| Diabetes | 6 (13%) | 23 (35%) | 0.006 |
| CRF | 1 (2%) | 3 (5%) | 0.48 |
| COPD | 2 (4%) | 11 (17%) | 0.04 |
| Depression | 5 (10%) | 8 (12%) | 0.78 |
| Surgical Parameters | |||
| Surgery Type | 0.19 | ||
| Isolated CABG | 23 (48%) | 29 (44%) | |
| Isolated Valve | 11 (23%) | 18 (27%) | |
| CABG + Valve | 8 (17%) | 17 (26%) | |
| Other | 6 (12%) | 2 (3%) | |
| ICU Length of Stay (days) | 1 (1–2.25) | 1 (1–3) | 0.39 |
| Length of Hospital Stay (days) | 6 (5–8.5) | 10 (6–14) | 0.002 |
| CR Completers (n = 48) | CR Non-Completers (n = 66) | p-Value | |||
|---|---|---|---|---|---|
| Baseline | 1-Year | Baseline | 1-Year | ||
| MFC | |||||
| Slowness (5-meter gait speed, s) | 4.6 (3.8–5.6) | 4.5 (4–5.4) | 5 (4.2–6.3) | 5.1 (4.7–5.7) | 0.46 |
| Weakness (grip strength; kg) | 36.5 (25.5–41.3) | 32 (22.5–41) | 30 (20–40) | 27 (18–37.5) | 0.72 |
| Weight loss in the past year (kg) | 1.3 (0–4.5) | 0 (0) | 4.5 (2–9.3) | 0 (0) | 0.50 |
| Exhaustion (CESD) | 0 (0–2) | 0 (0–1) | 2 (0–3) | 2 (0–3) | 0.47 |
| Depression (HADS) | 2 (1–4) | 1 (1–2) | 3 (1–6) | 3 (1–5) | 0.32 |
| Cognitive impairment (MOCA) | 25 (23–27) | 25 (22–28) | 24 (21–27) | 23 (18.3–25.8) | 0.005 |
| Low physical activity (Paffenbarger, kcal/wk) | 437.5 (155–886) | 1591 (672–3150) | 96 (28.8–338.8) | 658 (215.8–2105.8) | 0.04 |
| SPPB | |||||
| 5-meter gait speed (points) | 4 (4) | 4 (4) | 4 (4) | 4 (4) | 0.69 |
| Balance (points) | 4 (4) | 4 (4) | 4 (2.3–4) | 4 (3–4) | 0.06 |
| Repeated chair stand (points) | 2 (1–3) | 3 (1.8–4) | 2 (1–3) | 3 (1.3–4) | 0.87 |
| FFI | |||||
| Physical | 0.2 (0.1–0.3) | 0.05 (0–0.17) | 0.35 (0.2–0.45) | 0.1 (0.05–0.31) | 0.009 |
| Functional | 0 (0) | 0 (0) | 0 (0–0.05) | 0 (0) | 0.28 |
| Nutrition and exhaustion | 0.1 (0–0.2) | 0 (0–0.2) | 0.2 (0.1–0.4) | 0.2 (0.03–0.2) | 0.18 |
| Quality of life | 0.2 (0.2–0.3) | 0.2 (0.1–0.3) | 0.35 (0.2–0.78) | 0.2 (0.2–0.3) | 0.18 |
| Mood and cognition | 0.33 (0–0.33) | 0.33 (0–0.33) | 0.33 (0–0.33) | 0.33 (0.33–0.33) | 0.62 |
| CFS | MFC | SPPB | FFI | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 1-Year | Delta | Baseline | 1-Year | Delta | Baseline | 1-Year | Delta | Baseline | 1-Year | Delta | |
| rs | −0.29 | −0.24 | 0.062 | −0.15 | −0.082 | 0.072 | 0.025 | 0.16 | 0.15 | −0.23 | −0.21 | 0.0049 |
| p-value | 0.02 | 0.06 | 0.64 | 0.25 | 0.53 | 0.58 | 0.85 | 0.23 | 0.26 | 0.07 | 0.11 | 0.97 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kimber, D.E.; Kehler, D.S.; Lytwyn, J.; Boreskie, K.F.; Jung, P.; Alexander, B.; Hiebert, B.M.; Dubiel, C.; Hamm, N.C.; Stammers, A.N.; et al. Pre-Operative Frailty Status Is Associated with Cardiac Rehabilitation Completion: A Retrospective Cohort Study. J. Clin. Med. 2018, 7, 560. https://doi.org/10.3390/jcm7120560
Kimber DE, Kehler DS, Lytwyn J, Boreskie KF, Jung P, Alexander B, Hiebert BM, Dubiel C, Hamm NC, Stammers AN, et al. Pre-Operative Frailty Status Is Associated with Cardiac Rehabilitation Completion: A Retrospective Cohort Study. Journal of Clinical Medicine. 2018; 7(12):560. https://doi.org/10.3390/jcm7120560
Chicago/Turabian StyleKimber, Dustin E., D. Scott Kehler, James Lytwyn, Kevin F. Boreskie, Patrick Jung, Bryce Alexander, Brett M. Hiebert, Chris Dubiel, Naomi C. Hamm, Andrew N. Stammers, and et al. 2018. "Pre-Operative Frailty Status Is Associated with Cardiac Rehabilitation Completion: A Retrospective Cohort Study" Journal of Clinical Medicine 7, no. 12: 560. https://doi.org/10.3390/jcm7120560