Risk Stratification of Sudden Cardiac Death in Patients with Heart Failure: An update

Abstract
:1. Introduction
2. Research Strategy
3. Epidemiology of SCD
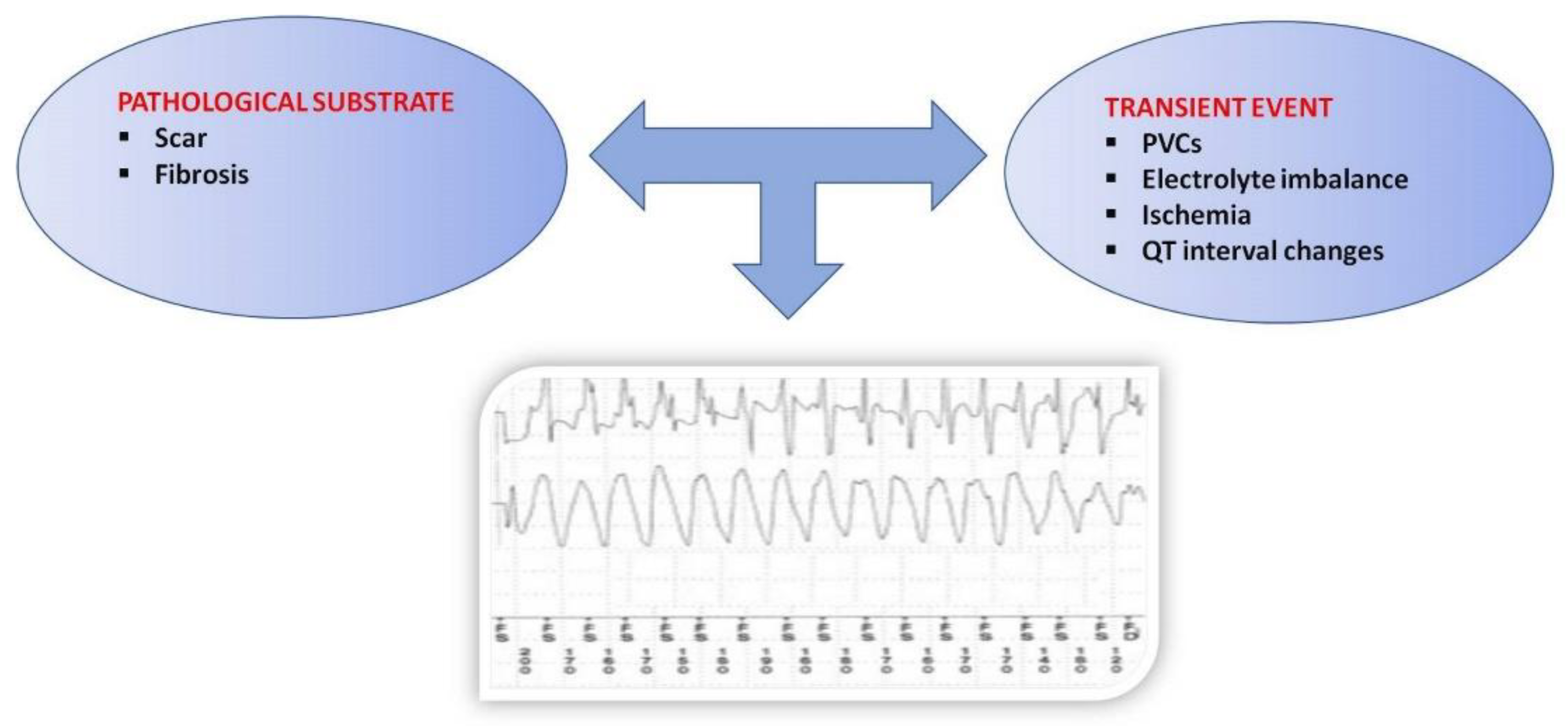
4. Pathophysiology of SCD
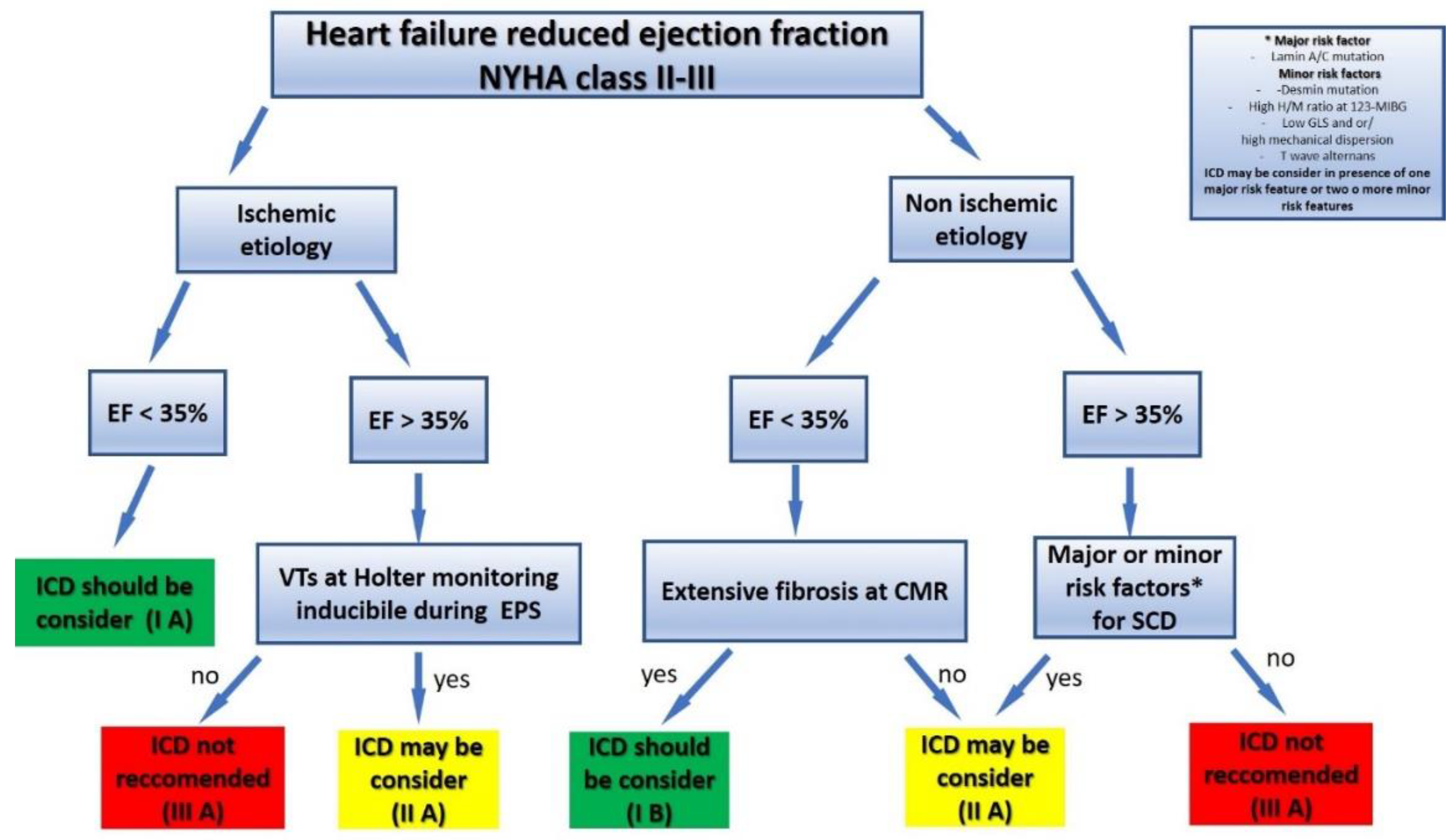
5. Risk Stratification of SCD in HFrEF
6. Cardiac Imaging
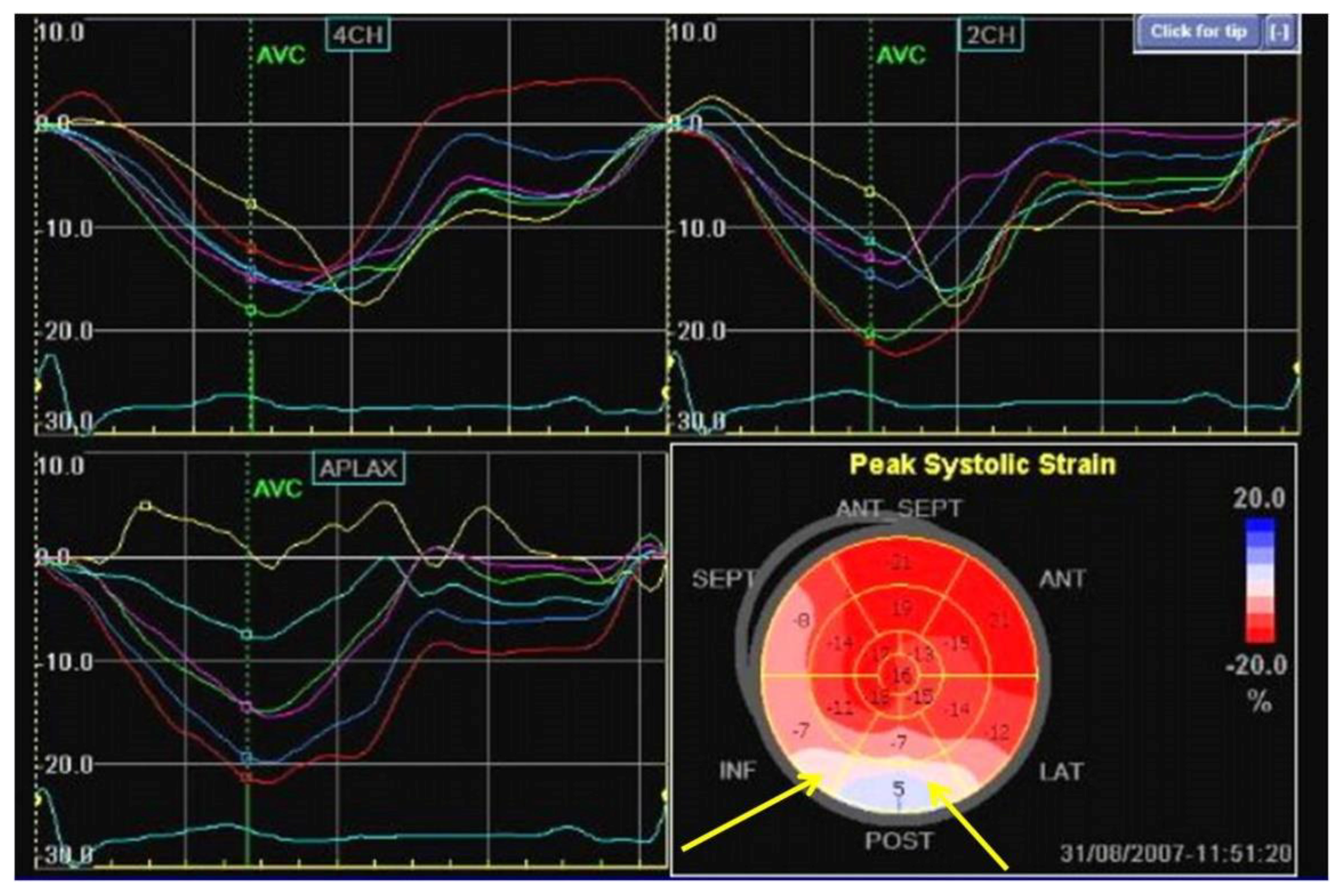
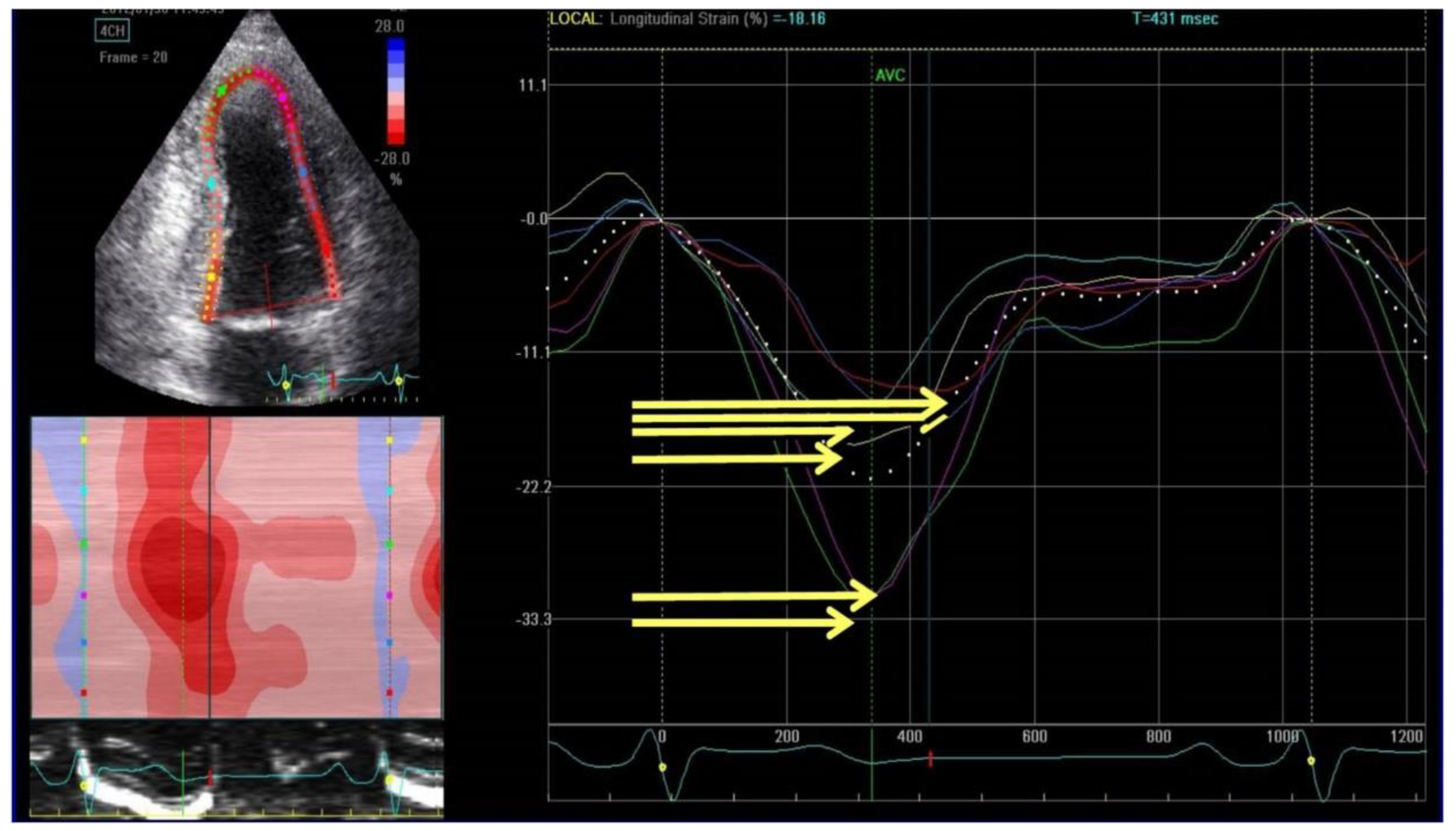
6.1. Speckle Echocardiography
6.2. Cardiac Magnetic Resonance
6.3. Myocardial Sympathetic Innervation Imaging
7. ECG and Electrophysiology
7.1. Resting ECG
7.2. Ambulatory Electrocardiogram
7.3. Autonomic Function Test
7.4. Microvolt T wave Alternans
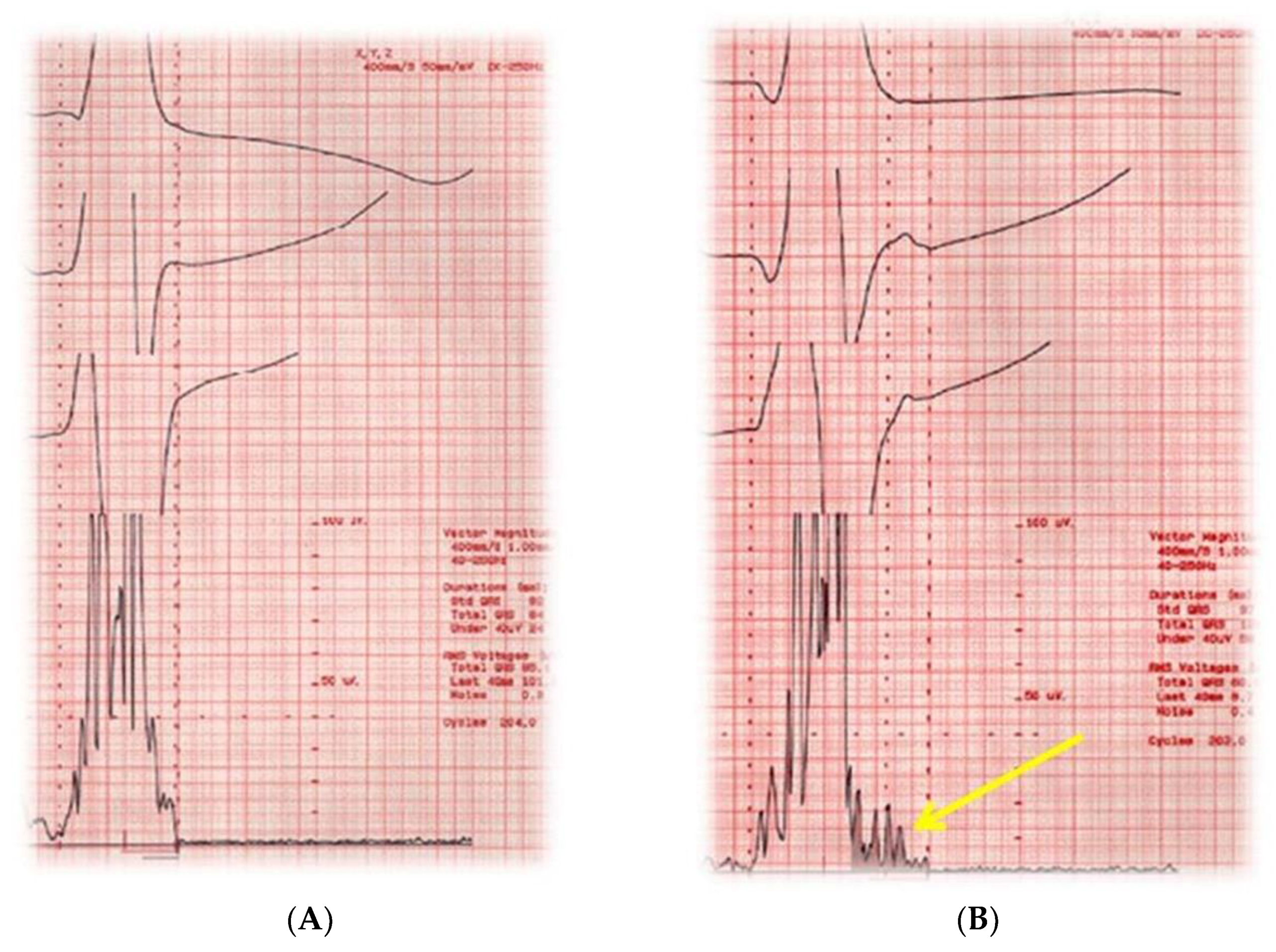
7.5. Signal-Averaged Electrocardiography
7.6. Electrophysiologic Study
8. Biomarkers
9. Genetics and Genomics
10. Artificial intelligence and machine learning
11. Risk stratification of SCD in HFpEF
12. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Metra, M.; Teerlink, J.R. Heart Failure. Lancet 2017, 390, 1981–1995. [Google Scholar] [CrossRef]
- Ziaeian, B.; Fonarow, G.C. Epidemiology and aetiology of heart failure. Nat. Rev. Cardiol. 2016, 13, 368–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidenreich, P.A.; Albert, N.M.; Allen, L.A.; Bluemke, D.A.; Butler, J.; Fonarow, G.C.; Ikonomidis, J.S.; Khavjou, O.; Konstam, M.A.; Maddox, T.M.; et al. Forecasting the impact of heart failure in the United States: A policy statement from the American Heart Association. Circ. Heart Fail. 2013, 6, 606–619. [Google Scholar] [CrossRef] [PubMed]
- Ceia, F.; Fonseca, C.; Mota, T.; Morais, H.; Matias, F.; de Sousa, A.; Oliveira, A.; EPICA Investigators. Prevalence of chronic heart failure in Southwestern Europe: The EPICA study. Eur. J. Heart Fail. 2002, 4, 531–539. [Google Scholar] [CrossRef]
- Vaduganathan, M.; Patel, R.B.; Michel, A.; Shah, S.J.; Senni, M.; Gheorghiade, M. Mode of death in heart failure with preserved ejection fraction. J. Am. Coll. Cardiol. 2017, 69, 556–569. [Google Scholar] [CrossRef] [PubMed]
- Al-Khatib, S.M.; Stevenson, W.G.; Ackerman, M.J.; Bryant, W.J.; Callans, D.J.; Curtis, A.B.; Deal, B.J.; Dickfeld, T.; Field, M.E.; Fonarow, G.C.; et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: Executive summary: A report of the American college of cardiology/American heart association task force on clinical practice guidelines and the heart rhythm society. J. Am. Coll. Cardiol. 2017, 1097, 41305–413020. [Google Scholar]
- Hayashi, M.; Shimizu, W.; Albert, C.M. The spectrum of epidemiology underlying sudden cardiac death. Circ. Res. 2015, 116, 1887–1906. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [PubMed]
- Vaduganathan, M.; Michel, A.; Hall, K.; Mulligan, C.; Nodari, S.; Shah, S.J.; Senni, M.; Triggiani, M.; Butler, J.; Gheorghiade, M.; et al. Spectrum of epidemiological and clinical findings in patients with heart failure with preserved ejection fraction stratified by study design: A systematic review. Eur. J. Heart Fail. 2016, 18, 54–65. [Google Scholar] [CrossRef] [PubMed]
- Uretsky, B.F.; Sheahan, R.G. Primary prevention of sudden cardiac death in heart failure: Will the solution be shocking? J. Am. Coll. Cardiol. 1997, 30, 1589–1597. [Google Scholar] [CrossRef]
- Klein, L.; Hsia, H. Sudden cardiac death in heart failure. Cardiol. Clin. 2014, 32, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Rosanio, S.; Schwarz, E.R.; Vitarelli, A.; Zarraga, I.G.; Kunapuli, S.; Ware, D.L.; Birnbaum, Y.; Tuero, E.; Uretsky, B.F. Sudden death prophylaxis in heart failure. Int. J. Cardiol. 2007, 119, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Saour, B.; Smith, B.; Yancy, C.W. Heart failure and sudden cardiac death. Card. Electrophysiol. Clin. 2017, 9, 709–723. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Claggett, B.L.; Chatterjee, N.A.; Anand, I.S.; Sweitzer, N.K.; Fang, J.C.; O’Meara, E.; Shah, S.J.; Hegde, S.M.; Desai, A.S.; et al. Sudden death in heart failure with preserved ejection fraction: A competing risks analysis from the TOPCAT Trial. JACC Heart Fail. 2018, 6, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Masarone, D.; Limongelli, G.; Rubino, M.; Valente, F.; Vastarella, R.; Ammendola, E.; Gravino, R.; Verrengia, M.; Salerno, G.; Pacileo, G. Management of arrhythmias in heart failure. J. Cardiovasc. Dev. Dis. 2017, 28, 3. [Google Scholar] [CrossRef] [PubMed]
- Burke, A.P.; Virmani, R. Pathophysiology of acute myocardial infarction. Med. Clin. N. Am. 2007, 91, 553–572. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Cooper, D.H.; Desouza, K.A.; Cuculich, P.S.; Woodard, P.K.; Smith, T.W.; Rudy, Y. Electrophysiologic scar substrate in relation to VT: Noninvasive high-resolution mapping and risk assessment with ECGI. Pacing Clin. Electrophysiol. 2016, 39, 781–791. [Google Scholar] [CrossRef] [PubMed]
- Mendonca Costa, C.; Plank, G.; Rinaldi, C.A.; Niederer, S.A.; Bishop, M.J. Modeling the electrophysiological properties of the infarct border zone. Front. Physiol. 2018, 9, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Zaman, S.; Kovoor, P. Sudden cardiac death early after myocardial infarction: Pathogenesis, risk stratification, and primary prevention. Circulation 2017, 129, 2426–2435. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European society of cardiology (ESC). Eur. Heart J. 2017, 39, 119–177. [Google Scholar]
- Priori, S.G.; Blomström-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European society of cardiology (ESC). Endorsed by: Association for European paediatric and congenital cardiology (AEPC). Eur Heart J. 2015, 36, 2793–2867. [Google Scholar] [PubMed]
- Liuba, I.; Marchlinski, F.E. The substrate and ablation of ventricular tachycardia in patients with nonischemic cardiomyopathy. Circ. J. 2014, 77, 1957–1966. [Google Scholar] [CrossRef]
- Pogwizd, S.M.; McKenzie, J.P.; Cain, M.E. Mechanisms underlying spontaneous and induced ventricular arrhythmias in patients with idiopathic dilated cardiomyopathy. Circulation 1998, 98, 2404–2414. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, J.J.; Subačius, H.; Patel, T.; Cunnane, R.; Kadish, A.H. Sudden cardiac death risk stratification in patients with nonischemic dilated cardiomyopathy. J. Am. Coll. Cardiol. 2014, 63, 1879–1889. [Google Scholar] [CrossRef] [PubMed]
- Santangeli, P.; Rame, J.E.; Birati, E.Y.; Marchlinski, F.E. Management of ventricular arrhythmias in patients with advanced heart failure. J. Am. Coll. Cardiol. 2017, 69, 1842–1860. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Song, D.; Dong, J.; Zhu, P.; Liu, J.; Liu, W.; Ma, X.; Zhao, L.; Ling, S. Current understanding of the pathophysiology of myocardial fibrosis and its quantitative assessment in heart failure. Front. Physiol. 2017, 24, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Patel, R.B.; Shah, S.J.; Butler, J. Sudden cardiac death in heart failure with preserved ejection fraction: A target for therapy? Heart Fail Rev. 2016, 21, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Chugh, S.S. Disrupting the approach to sudden cardiac death: From vulnerable ejection fraction to vulnerable patient. Circulation 2018, 137, 7–9. [Google Scholar] [CrossRef] [PubMed]
- Wellens, H.J.; Schwartz, P.J.; Lindemans, F.W.; Buxton, A.E.; Goldberger, J.J.; Hohnloser, S.H.; Huikuri, H.V.; Kääb, S.; La Rovere, M.T.; Malik, M.; et al. Risk stratification for sudden cardiac death: Current status and challenges for the future. Eur. Heart J. 2014, 35, 1642–1651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabbag, A.; Suleiman, M.; Laish-Farkash, A.; Samania, N.; Kazatsker, M.; Goldenberg, I.; Glikson, M.; Beinart, R.; Israeli Working Group of Pacing; Electrophysiology. Contemporary rates of appropriate shock therapy in patients who receive implantable device therapy in a real-world setting: From the Israeli ICD registry. Heart Rhythm 2015, 12, 2426–2433. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.; Stevenson, L.W.; Stewart, G.C.; Bhatt, D.L.; Desai, M.; Seeger, J.D.; Williams, L.; Jalbert, J.J.; Setoguchi, S. Real-world effectiveness of primary implantable cardioverter defibrillators implanted during hospital admissions for exacerbation of heart failure or other acute co-morbidities: Cohort study of older patients with heart failure. BMJ 2015, 351, 3529–3533. [Google Scholar] [CrossRef] [PubMed]
- Stecker, E.C.; Vickers, C.; Waltz, J.; Socoteanu, C.; John, B.T.; Mariani, R.; McAnulty, J.H.; Gunson, K.; Jui, J.; Chugh, S.S. Population-based analysis of sudden cardiac death with and without left ventricular systolic dysfunction: Two-year findings from the Oregon Sudden Unexpected Death Study. J. Am. Coll. Cardiol. 2015, 47, 1161–1166. [Google Scholar] [CrossRef] [PubMed]
- Salvo, G.D.; Pergola, V.; Fadel, B.; Bulbul, Z.A.; Caso, P. Strain echocardiography, and myocardial mechanics: From basics to clinical applications. J. Cardiovasc. Echogr. 2015, 25, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Collier, P.; Phelan, D.; Klein, A. A test in context: Myocardial strain measured by speckle-tracking echocardiography. J. Am. Coll. Cardiol. 2017, 2869, 1043–1056. [Google Scholar] [CrossRef] [PubMed]
- Van der Bijl, P.; Delgado, V.; Bax, J.J. Sudden cardiac death: The role of imaging. Int. J. Cardiol. 2017, 237, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Haugaa, K.H.; Goebel, B.; Dahlslett, T.; Meyer, K.; Jung, C.; Lauten, A.; Figulla, H.R.; Poerner, T.C.; Edvardsen, T. Risk assessment of ventricular arrhythmias in patients with nonischemic dilated cardiomyopathy by strain echocardiography. J. Am. Soc. Echocardiogr. 2012, 25, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Haugaa, K.H.; Smedsrud, M.K.; Steen, T.; Kongsgaard, E.; Loennechen, J.P.; Skjaerpe, T.; Voigt, E.; Willems, R.; Smith, G.; Smiseth, O.A.; et al. Mechanical dispersion assessed by myocardial strain in patients after myocardial infarction for risk prediction of ventricular arrhythmia. JACC Cardiovasc. Imaging 2010, 3, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Banasik, G.; Segiet, O.; Elwart, M.; Szulik, M.; Lenarczyk, R.; Kalarus, Z.; Kukulski, T. LV mechanical dispersion as a predictor of ventricular arrhythmia in patients with advanced systolic heart failure LV mechanical dispersion as a predictor of ventricular arrhythmia in patients with advanced systolic heart failure: A pilot study. Herz 2016, 41, 599–604. [Google Scholar] [CrossRef] [PubMed]
- Ersboll, M.; Valeur, N.; Andersen, M.J.; Mogensen, U.M.; Vinther, M.; Svendsen, J.H.; Møller, J.E.; Kisslo, J.; Velazquez, E.J.; Hassager, C.; et al. Early echocardiographic deformation analysis for the prediction of sudden cardiac death and life-threatening arrhythmias after myocardial infarction. JACC Cardiovasc. Imaging 2013, 6, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.P.; Qu, Z.; Weiss, J.N. Cardiac fibrosis and arrhythmogenesis: The road to repair is paved with perils. J. Mol. Cell. Cardiol. 2014, 70, 83–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- From, A.M.; Maleszewski, J.J.; Rihal, C.S. Current status of endomyocardial biopsy. Mayo Clin. Proc. 2011, 86, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.T., Jr. Role of left ventricular biopsy in the management of heart disease. Circulation 2013, 128, 1492–1499. [Google Scholar] [CrossRef] [PubMed]
- Mewton, N.; Liu, C.Y.; Croisille, P.; Bluemke, D.; Lima, J.A. Assessment of myocardial fibrosis with cardiovascular magnetic resonance. J. Am. Coll. Cardiol. 2011, 22, 891–903. [Google Scholar] [CrossRef] [PubMed]
- Disertori, M.; Rigoni, M.; Pace, N.; Casolo, G.; Masè, M.; Gonzini, L.; Lucci, D.; Nollo, G.; Ravelli, F. Myocardial fibrosis assessment by LGE is a powerful predictor of ventricular tachyarrhythmias in ischemic and nonischemic LV dysfunction: A meta-analysis. JACC Cardiovasc. Imaging 2016, 9, 1046–1055. [Google Scholar] [CrossRef] [PubMed]
- Pontone, G.; Guaricci, A.I.; Andreini, D.; Solbiati, A.; Guglielmo, M.; Mushtaq, S.; Baggiano, A.; Beltrama, V.; Fusini, L.; Rota, C.; et al. Prognostic benefit of cardiac magnetic resonance over transthoracic echocardiography for the assessment of ischemic and nonischemic dilated cardiomyopathy patients referred for the evaluation of primary prevention implantable cardioverter—Defibrillator therapy. Circ. Cardiovasc. Imaging 2016, 9. [Google Scholar] [CrossRef]
- Puntmann, V.O.; Peker, E.; Chandrashekhar, Y.; Nagel, E. T1 mapping in characterizing myocardial disease: A comprehensive review. Circ. Res. 2016, 119, 277–299. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Sohal, M.; Voigt, T.; Sammut, E.; Tobon-Gomez, C.; Child, N.; Jackson, T.; Shetty, A.; Bostock, J.; Cooklin, M.; et al. Myocardial tissue characterization by cardiac magnetic resonance imaging using T1 mapping predicts ventricular arrhythmia in ischemic and non-ischemic cardiomyopathy patients with implantable cardioverter-defibrillators. Heart Rhythm 2015, 12, 792–801. [Google Scholar] [CrossRef] [PubMed]
- Triposkiadis, F.; Karayannis, G.; Giamouzis, G.; Skoularigis, J.; Louridas, G.; Butler, J. The sympathetic nervous system in heart failure physiology, pathophysiology, and clinical implications. J. Am. Coll. Cardiol. 2009, 54, 1747–1762. [Google Scholar] [CrossRef] [PubMed]
- Carrió, I.; Cowie, M.R.; Yamazaki, J.; Udelson, J.; Camici, P.G. Cardiac sympathetic imaging with mIBG in heart failure. JACC Cardiovasc. Imaging 2010, 3, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, K.; Nakata, T.; Doi, T.; Kadokami, T.; Matsuo, S.; Konno, T.; Yamada, T.; Jacobson, A.F. Validation of 2-year 123I-meta-iodobenzylguanidine-based cardiac mortality risk model in chronic heart failure. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, S.; Yamada, T.; Okuyama, Y.; Morita, T.; Sanada, S.; Tsukamoto, Y.; Masuda, M.; Okuda, K.; Iwasaki, Y.; Yasui, T.; et al. Cardiac iodine-123 metaiodobenzylguanidine imaging predicts sudden cardiac death independently of left ventricular ejection fraction in patients with chronic heart failure and left ventricular systolic dysfunction: Results from a comparative study with signal-averaged electrocardiogram, heart rate variability, and QT dispersion. J. Am. Coll. Cardiol. 2009, 53, 426–435. [Google Scholar] [PubMed]
- Varma, N. Left ventricular conduction delays and relation to QRS configuration in patients with left ventricular dysfunction. Am. J. Cardiol. 2009, 103, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Marume, K.; Noguchi, T.; Tateishi, E.; Morita, Y.; Kamakura, K.; Ishibashi, K.; Noda, T.; Miura, H.; Nishimura, K.; Nakai, M.; et al. Mortality and sudden cardiac death risk stratification using the noninvasive combination of wide QRS duration and late gadolinium enhancement in idiopathic dilated cardiomyopathy. Circ. Arrhythm. Electrophysiol. 2018, 11. [Google Scholar] [CrossRef] [PubMed]
- Zimetbaum, P.J.; Buxton, A.E.; Batsford, W.; Fisher, J.D.; Hafley, G.E.; Lee, K.L.; O’Toole, M.F.; Page, R.L.; Reynolds, M.; Josephson, M.E. Electrocardiographic predictors of arrhythmic death and total mortality in the multicenter unsustained tachycardia trial. Circulation 2004, 110, 766–769. [Google Scholar] [CrossRef] [PubMed]
- Katritsis, D.G.; Siontis, K.C.; Bigger, J.T.; Kadish, A.H.; Steinman, R.; Zareba, W.; Siontis, G.C.M.; Bardy, G.H.; Ioannidis, J.P.A. Effect of left ventricular ejection fraction and QRS duration on the survival benefit of implantable cardioverter-defibrillators: A meta-analysis of primary prevention trials. Heart Rhythm 2013, 10, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Aro, A.L.; Reinier, K.; Rusinaru, C.; Uy-Evanado, A.; Darouian, N.; Phan, D.; Mack, W.J.; Jui, J.; Soliman, E.Z.; Tereshchenko, L.G.; et al. Electrical risk score beyond the left ventricular ejection fraction: Prediction of sudden cardiac death in the Oregon Sudden Unexpected Death Study and the Atherosclerosis Risk in Communities Study. Eur. Heart J. 2017, 38, 3017–3025. [Google Scholar] [CrossRef] [PubMed]
- Bigger, J.T., Jr.; Fleiss, J.L.; Kleiger, R.; Miller, J.P.; Rolnitzky, L.M. The relationships among ventricular arrhythmias left ventricular dysfunction, and mortality in the 2 years after myocardial infarction. Circulation 1984, 69, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Hohnloser, S.H.; Klingenheben, T.; Zabel, M.; Schöpperl, M.; Mauss, O. Prevalence, characteristics, and prognostic value during long-term follow-up of nonsustained ventricular tachycardia after myocardial infarction in the thrombolytic era. J. Am. Coll. Cardiol. 1999, 33, 1895–1902. [Google Scholar] [CrossRef]
- Zecchin, M.; Di Lenarda, A.; Gregori, D.; Merlo, M.; Pivetta, A.; Vitrella, G.; Sabbadini, G.; Mestroni, L.; Sinagra, G. Are nonsustained ventricular tachycardias predictive of major arrhythmias in patients with dilated cardiomyopathy on optimal medical treatment? Pacing Clin. Electrophysiol. 2008, 31, 290–299. [Google Scholar] [CrossRef] [PubMed]
- Kusmirek, S.L.; Gold, M.R. Sudden cardiac death: The role of risk stratification. Am. Heart J. 2007, 153, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Stys, A.; Stys, T. Current clinical applications of heart rate variability. Clin. Cardiol. 1998, 21, 719–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleiger, R.E.; Miller, J.P.; Bigger, J.T., Jr.; Moss, A.J. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am. J. Cardiol. 1997, 59, 256–262. [Google Scholar] [CrossRef]
- Fauchier, L.; Babuty, D.; Cosnay, P.; Autret, M.L.; Fauchier, J.P. Heart rate variability in idiopathic dilated cardiomyopathy: Characteristics and prognostic value. J. Am. Coll. Cardiol. 1997, 30, 1009–1014. [Google Scholar] [CrossRef]
- Cygankiewicz, I. Heart rate turbulence. Prog. Cardiovasc. Dis. 2013, 56, 160–171. [Google Scholar] [CrossRef] [PubMed]
- Exner, D.V.; Kavanagh, K.M.; Slawnych, M.P.; Mitchell, L.B.; Ramadan, D.; Aggarwal, S.G.; Noullett, C.; Van Schaik, A.; Mitchell, R.T.; Shibata, M.A.; et al. Non-invasive risk assessment early after a myocardial infarction the REFINE study. J. Am. Coll. Cardiol. 2007, 50, 2275–2284. [Google Scholar] [CrossRef] [PubMed]
- Grimm, W.; Schmidt, G.; Maisch, B.; Sharkova, J.; Müller, H.H.; Christ, M. Prognostic significance of heart rate turbulence following ventricular premature beats in patients with idiopathic dilated cardiomyopathy. J. Cardiovasc. Electrophysiol. 2003, 14, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Klingenheben, T.; Ptaszynski, P.; Hohnloser, S.H. Heart rate turbulence and other autonomic risk markers for arrhythmia risk stratification in dilated cardiomyopathy. J. Electrocardiol. 2008, 41, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Narayan, S.M. T-wave alternans and the susceptibility to ventricular arrhythmias. J. Am. Coll. Cardiol. 2006, 47, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Merchant, F.M.; Ikeda, T.; Pedretti, R.F.; Salerno-Uriarte, J.A.; Chow, T.; Chan, P.S.; Bartone, C.; Hohnloser, S.H.; Cohen, R.J.; Armoundas, A.A. Clinical utility of microvolt T-wave alternans testing in identifying patients at high or low risk of sudden cardiac death. Heart Rhythm 2012, 9, 1256–1264. [Google Scholar] [CrossRef] [PubMed]
- De Ferrari, G.M.; Sanzo, A. T-wave alternans in risk stratification of patients with nonischemic dilated cardiomyopathy: Can it help to better select candidates for ICD implantation? Heart Rhythm 2008, 6, S29–S35. [Google Scholar] [CrossRef] [PubMed]
- Gold, M.R.; Ip, J.H.; Costantini, O.; Poole, J.E.; McNulty, S.; Mark, D.B.; Lee, K.L.; Bardy, G.H. Role of microvolt T-wave alternans in the assessment of arrhythmia vulnerability among patients with heart failure and systolic dysfunction: Primary results from the T-wave alternans sudden cardiac death in the heart failure trial substudy. Circulation 2008, 118, 2022–2028. [Google Scholar] [CrossRef] [PubMed]
- Chow, T.; Kereiakes, D.J.; Onufer, J.; Woelfel, A.; Gursoy, S.; Peterson, B.J.; Brown, M.L.; Pu, W.; Benditt, D.G. Does microvolt T-wave alternans testing predict ventricular tachyarrhythmias in patients with ischemic cardiomyopathy and prophylactic defibrillators? The MASTER (Microvolt T Wave Alternans Testing for Risk Stratification of Post-Myocardial Infarction Patients) trial. J. Am. Coll. Cardiol. 2008, 52, 1607–1615. [Google Scholar] [PubMed]
- Jarrett, J.R.; Flowers, N.C. Signal-averaged electrocardiography: History, techniques, and clinical applications. Clin. Cardiol. 1991, 14, 984–994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seale, W.L.; Gang, E.S.; Peter, C.T. The Use of Signal-Averaged Electrocardiography in Predicting Patients at High Risk for Sudden DeathPacing. Clin. Electrophysiol. 1999, 13, 796–807. [Google Scholar] [CrossRef]
- Thomas, K.E.; Josephson, M.E. The role of electrophysiology study in risk stratification of sudden cardiac death. Prog. Cardiovasc. Dis. 2008, 51, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Daubert, J.P.; Zareba, W.; Hall, W.J.; Schuger, C.; Corsello, A.; Leon, A.R.; Andrews, M.L.; McNitt, S.; Huang, D.T.; Moss, A.J.; et al. Predictive value of ventricular arrhythmia inducibility for subsequent ventricular tachycardia or ventricular fibrillation in Multicenter Automatic Defibrillator Implantation Trial (MADIT) II patients. J. Am. Coll. Cardiol. 2006, 47, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Hsia, H.H.; Marchlinski, F.E. Electrophysiology studies in patients with dilated cardiomyopathies. Card. Electrophysiol. Rev. 2002, 6, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Shenasa, M.; Borggrefe, M.; Block, M.; Hindricks, G.; Martinez-Rubio, A.; Haverkamp, W.; Willems, S.; Böcker, D.; Mäkijärvi, M.; et al. Role of programmed ventricular stimulation in patients with idiopathic dilated cardiomyopathy and documented sustained ventricular tachyarrhythmias: Inducibility and prognostic value in 102 patients. Eur. Heart J. 1994, 15, 76–78. [Google Scholar] [CrossRef] [PubMed]
- Vest, R.N.; Gold, M.R. Risk stratification of ventricular arrhythmias in patients with systolic heart failure. Curr. Opin. Cardiol. 2010, 25, 268–275. [Google Scholar] [CrossRef] [PubMed]
- D’Alessandro, R.; Masarone, D.; Buono, A.; Gravino, R.; Rea, A.; Salerno, G.; Golia, E.; Ammendola, E.; Del Giorno, G.; Santangelo, L.; et al. Natriuretic peptides: Molecular biology, pathophysiology and clinical implications for the cardiologist. Future Cardiol. 2013, 9, 519–534. [Google Scholar] [CrossRef] [PubMed]
- Vrtovec, B.; Knezevic, I.; Poglajen, G.; Sebestjen, M.; Okrajsek, R.; Haddad, F. Relation of B-type natriuretic peptide level in heart failure to sudden cardiac death in patients with and without QT interval prolongation. Am. J. Cardiol. 2013, 111, 886–890. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, H.; Niwano, S.; Fukaya, H.; Murakami, M.; Kishihara, J.; Satoh, A.; Yoshizawa, T.; Oikawa, J.; Ishizue, N.; Igarashi, T.; et al. Cardiac troponin T as a predictor of cardiac death in patients with left ventricular dysfunction. J. Arrhythm. 2017, 33, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Figal, D.A.; Ordoñez-Llanos, J.; Tornel, P.L.; Vázquez, R.; Puig, T.; Valdés, M.; Cinca, J.; de Luna, A.B.; Bayes-Genis, A. Soluble ST2 for predicting sudden cardiac death in patients with chronic heart failure and left ventricular systolic dysfunction. J. Am. Coll. Cardiol. 2009, 54, 2174–2179. [Google Scholar] [CrossRef] [PubMed]
- Refaat, M.M.; Hotait, M.; London, B. Genetics of sudden cardiac death. Curr. Cardiol. Rep. 2015, 17, 606–615. [Google Scholar] [CrossRef] [PubMed]
- Greene, H.L. Sudden arrhythmic cardiac death, mechanisms, resuscitation and classification: The Seattle Perspective. Am. J. Cardiol. 1990, 65, 4–12. [Google Scholar] [CrossRef]
- Jouven, X.; Desnos, M.; Guerot, C.; Ducimetiere, P. Predicting sudden death in the population: The Paris Prospective Study I. Circulation 1999, 99, 1978–1983. [Google Scholar] [CrossRef] [PubMed]
- Giudicessi, J.R.; Kullo, I.J.; Ackerman, M.J. Precision Cardiovascular Medicine: State of Genetic Testing. Mayo Clin. Proc. 2017, 92, 642–662. [Google Scholar] [CrossRef] [PubMed]
- Cabanelas, N.; Martins, V.P. Laminopathies: A Pandora’s box of heart failure, bradyarrhythmias, and sudden death. Rev. Port. Cardiol. 2015, 34, 139.e1–139.e5. [Google Scholar] [CrossRef] [PubMed]
- Masarone, D.; Ammendola, E.; Rago, A.; Gravino, R.; Salerno, G.; Rubino, M.; Marrazzo, T.; Molino, A.; Calabrò, P.; Pacileo, G.; et al. Management of Bradyarrhythmias in Heart Failure: A Tailored Approach. Adv. Exp. Med. Biol. 2018, 1067, 255–269. [Google Scholar] [PubMed]
- McLendon, P.M.; Robbins, J. Desmin-related cardiomyopathy: An unfolding story. Am. J. Physiol. Heart Circ. Physiol. 2011, 301, 1220–1228. [Google Scholar] [CrossRef] [PubMed]
- Bezzina, C.R.; Lahrouchi, N.; Priori, S.G. Genetics of sudden cardiac death. Circ. Res. 2015, 116, 1919–1936. [Google Scholar] [CrossRef] [PubMed]
- Manis, G.; Nikolopoulos, S.; Arsenos, P.; Gatzoulis, K.A.; Dilaveris, P.; Stefanadis, C. Risk stratification for Arrhythmic Sudden Cardiac Death in heart failure patients using machine learning techniques. Comput. Cardiol. 2013, 42, 141–144. [Google Scholar]
- Awan, S.E.; Sohel, F.; Sanfilippo, F.M.; Bennamoun, M.; Dwivedi, G. Machine learning in heart failure: Ready for prime time. Curr. Opin. Cardiol. 2018, 33, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; Wang, D.; Finn, P.; Skali, H.; Zornoff, L.; McMurray, J.J.; Swedberg, K.; Yusuf, S.; Granger, C.; Michelson, E.; et al. Effect of candesartan on cause-specific mortality in heart failure patients: The Candesartan in Heart failure Assessment of Reduction in Mortality and morbidity (CHARM) program. Circulation 2004, 12, 2180–2183. [Google Scholar] [CrossRef] [PubMed]
- Zile, M.R.; Gaasch, W.H.; Anand, I.S.; Haass, M.; Little, W.C.; Miller, A.B.; Lopez-Sendon, J.; Teerlink, J.R.; White, M.; McMurray, J.J.; et al. Mode of death in patients with heart failure and a preserved ejection fraction: Results from the Irbesartan in Heart Failure with Preserved Ejection Fraction Study (I-Preserve) trial. Circulation 2010, 30, 1393–1405. [Google Scholar] [CrossRef] [PubMed]
- Donal, E.; Lund, L.H.; Oger, E.; Hage, C.; Persson, H.; Reynaud, A.; Ennezat, P.V.; Bauer, F.; Sportouch-Dukhan, C.; Daubert, J.C.; et al. Baseline characteristics of patients with heart failure and preserved ejection fraction included in the Karolinska Rennes (KaRen) study. Arch. Cardiovasc. Dis. 2014, 107, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Bosseau, C.; Donal, E.; Lund, LH.; Oger, E.; Hage, C.; Mulak, G.; Daubert, J.C.; Linde, C. The prognostic significance of atrial fibrillation in heart failure with preserved ejection function: Insights from KaRen, a prospective and multicenter study. Heart Vessel. 2017, 32, 735–749. [Google Scholar] [CrossRef] [PubMed]
- Donal, E.; Lund, L.H.; Oger, E.; Hage, C.; Persson, H.; Reynaud, A.; Ennezat, P.V.; Bauer, F.; Drouet, E.; Linde, C.; et al. New echocardiographic predictors of clinical outcome in patients presenting with heart failure and a preserved left ventricular ejection fraction: A subanalysis of the Ka (Karolinska) Ren (Rennes) Study. Eur. J. Heart Fail. 2015, 17, 680–688. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Familial and Personal History |
| -Prior cardiac arrest |
| -Family history of SCD |
| -Unexplained syncope |
| Electrocardiography |
| -QRS duration |
| -T wave alternans |
| -Signal averaged ECG |
| Autonomic Function |
| -Heart rate variability |
| -Heart rate turbulence |
| Electrophysiologic Study |
| -Inducible ventricular arrhythmias |
| -Extensive low voltage/abnormal signals on electroanatomic mapping |
| -Large mid-epicardial scar burden |
| -Multiple VT morphology |
| Echocardiography |
| -LVEF |
| -Ventricular dyssynchrony |
| -Speckle tracking |
| -Mechanical dispersion |
| Cardiac MRI |
| -Late gadolinium enhancement |
| -T1 mapping |
| Myocardial Sympathetic Innervation Imaging |
| -Heart to mediastal ratio |
| Biomarkers |
| -Natriuretic peptides |
| -High sensitive troponin |
| -Soluble ST2 |
| Genetics |
| -Lamin A/C mutation |
| -Desmin mutation |
| Personal History |
| Age |
| Male sex |
| Insulin-treated diabetes mellitus |
| Prior myocardial infarction |
| Electrocardiogram |
| Left bundle branch block |
| Biomarkers |
| Natriuretic peptides |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masarone, D.; Limongelli, G.; Ammendola, E.; Verrengia, M.; Gravino, R.; Pacileo, G. Risk Stratification of Sudden Cardiac Death in Patients with Heart Failure: An update. J. Clin. Med. 2018, 7, 436. https://doi.org/10.3390/jcm7110436
Masarone D, Limongelli G, Ammendola E, Verrengia M, Gravino R, Pacileo G. Risk Stratification of Sudden Cardiac Death in Patients with Heart Failure: An update. Journal of Clinical Medicine. 2018; 7(11):436. https://doi.org/10.3390/jcm7110436
Chicago/Turabian StyleMasarone, Daniele, Giuseppe Limongelli, Ernesto Ammendola, Marina Verrengia, Rita Gravino, and Giuseppe Pacileo. 2018. "Risk Stratification of Sudden Cardiac Death in Patients with Heart Failure: An update" Journal of Clinical Medicine 7, no. 11: 436. https://doi.org/10.3390/jcm7110436