Systematic Review and Pragmatic Clinical Approach to Oral and Nasal Vitamin B12 (Cobalamin) Treatment in Patients with Vitamin B12 Deficiency Related to Gastrointestinal Disorders

 ,
, 
Abstract
:1. Introduction
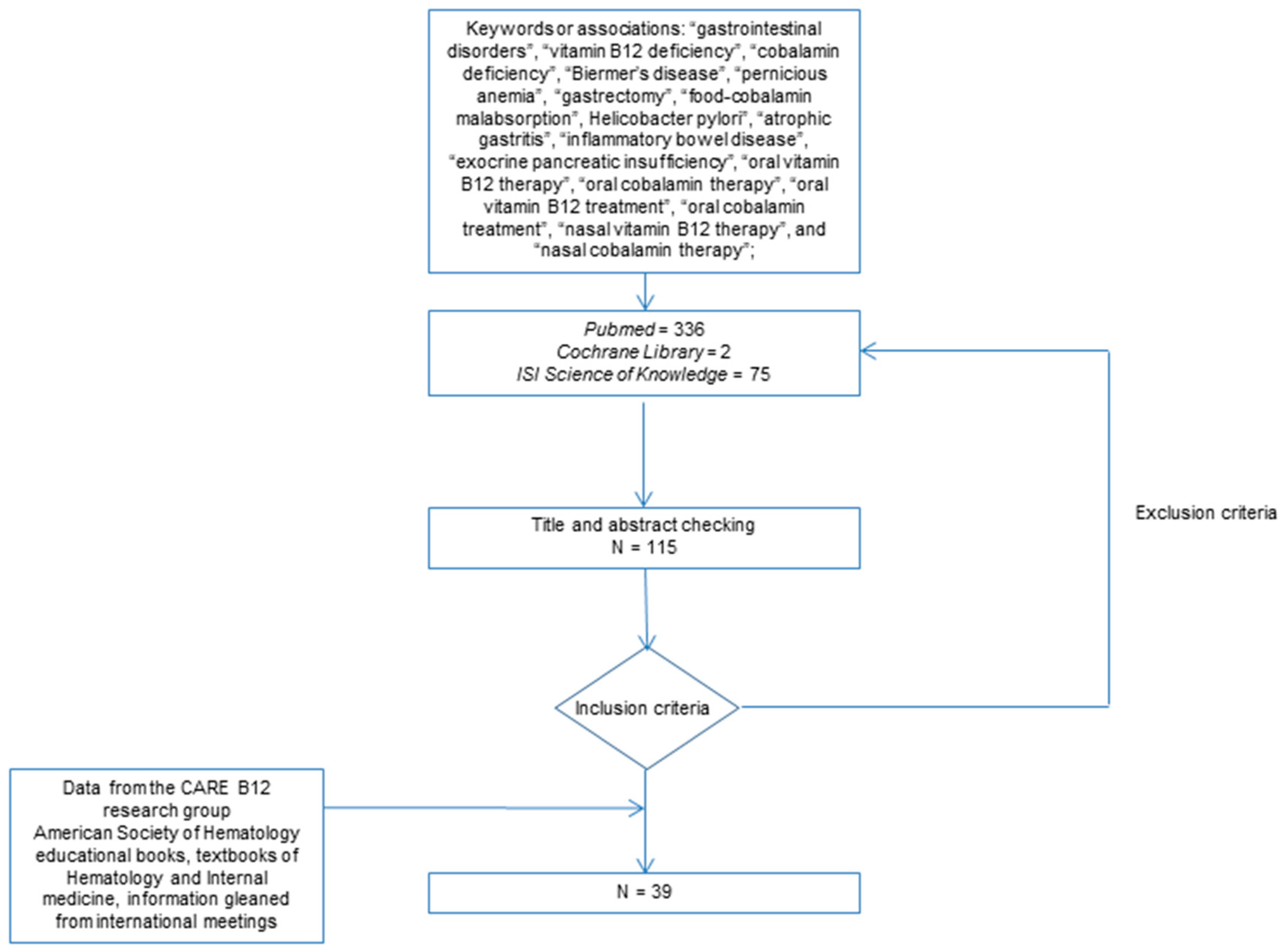
2. Methodology of the Literature Search
3. Results of the Literature Search
3.1. Synthetic Results of the Systematic Research
3.2. Randomized Controlled Studies of Oral Vitamin B12 Treatment in Vitamin B12 Deficiency
3.3. Systematic Reviews of Oral Vitamin B12 Treatment in Vitamin B12 Deficiency
3.4. Prospective Studies of Oral Vitamin B12 Treatment in Patients with Food-Cobalamin Malabsorption and Biermer’s Disease
3.5. Oral Vitamin B12 Treatment in Vegans or Vegetarians
3.6. Oral Vitamin B12 Treatment in Patients with Total Gastrectomy after Roux-en-Y Gastric Bypass
3.7. Oral Vitamin B12 Treatment in Patients with Crohn’s Disease
3.8. Oral Vitamin B12 Treatment in a Reference Academic Center
3.9. Nasal Vitamin B12 Treatment
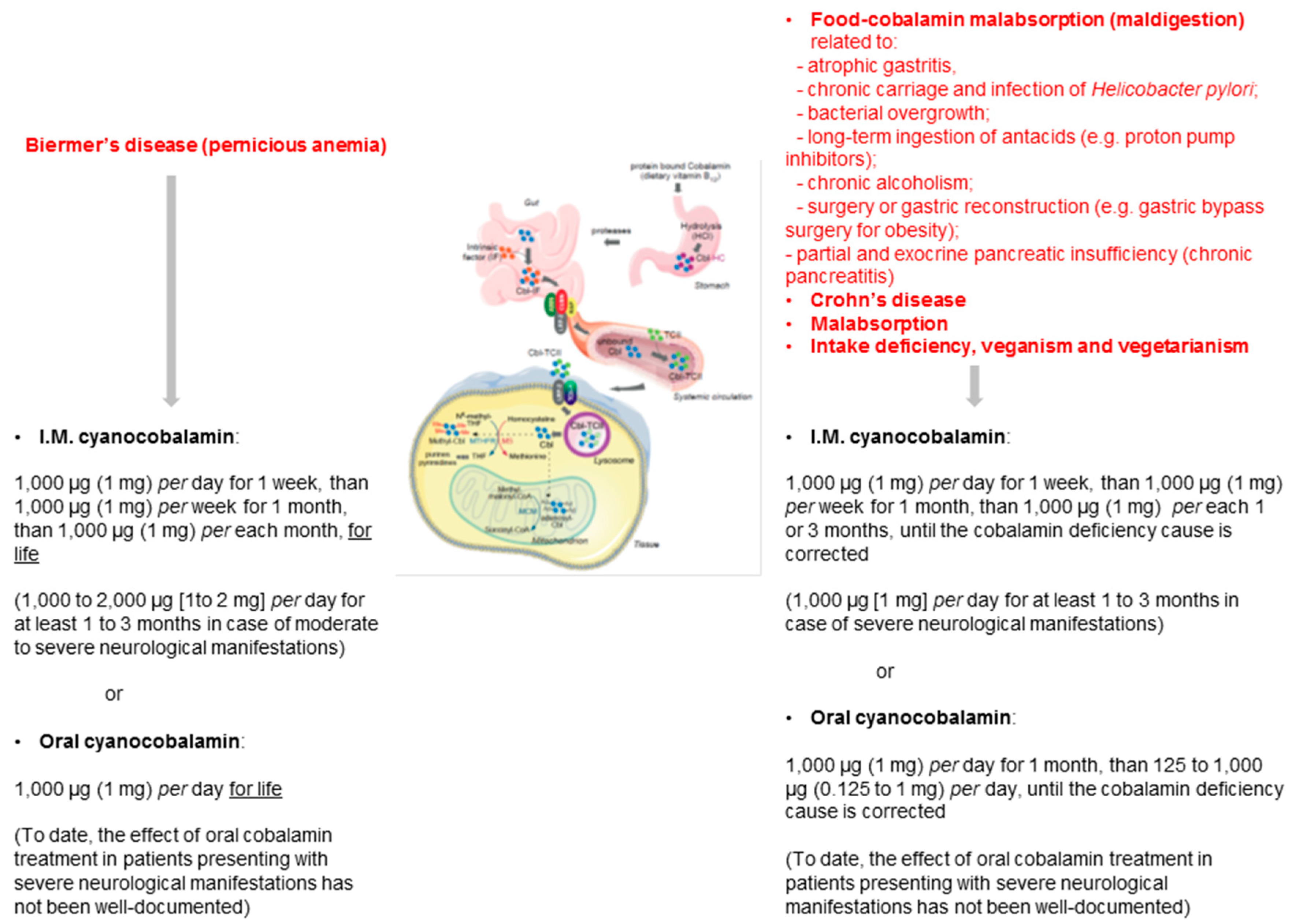
4. Conclusions and Recommendations
Perspectives and Direction of Future Research
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jones, R.H. Clinical economics review: Gastrointestinal disease in primary care. Aliment. Pharmacol. Ther. 1996, 10, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Alpers, D.H.; Kalloo, A.N. Textbook of Gastroenterology, 5th ed.; Blackwell Publication: Chichester, UK, 2009; pp. 2774–2784. [Google Scholar]
- Briani, C.; Dalla Torre, C.; Citton, V.; Manara, R.; Pompanin, S.; Binotto, G.; Adami, F. Cobalamin deficiency: Clinical picture and radiological findings. Nutrients 2013, 5, 4521–4539. [Google Scholar] [CrossRef] [PubMed]
- Toh, B.H. Pathophysiology and laboratory diagnosis of pernicious anemia. Immunol. Res. 2017, 65, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Lane, L.A.; Rojas-Fernandez, C. Treatment of vitamin B12 deficiency anemia: Oral versus parenteral therapy. Ann. Pharmacother. 2002, 36, 1268–1272. [Google Scholar] [CrossRef] [PubMed]
- Graham, I.D.; Jette, N.; Tetroe, J.; Robinson, N.; Milne, S.; Mitchell, S.L. Oral cobalamin remains medicine’s best kept secret. Arch. Gerontol. Geriatr. 2007, 44, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Kuzminski, A.M.; Del Giacco, E.I.; Allen, R.H.; Stabler, S.P.; Lindenbaum, J. Effective treatment of cobalamin deficiency with oral cobalamin. Blood 1998, 92, 1191–1198. [Google Scholar] [PubMed]
- Bolaman, Z.; Kadikoylu, G.; Yukselen, V.; Yavasoglu, I.; Barutca, S.; Senturk, T. Oral versus intramuscular cobalamin treatment in megaloblastic anemia: A single-center, prospective, randomized, open-label study. Clin. Ther. 2003, 25, 3124–3134. [Google Scholar] [CrossRef]
- Sanz-Cuesta, T.; González-Escobar, P.; Riesgo-Fuertes, R.; Garrido-Elustondo, S.; del Cura-González, I.; Martín-Fernández, J.; Escortell-Mayor, E.; Rodríguez-Salvanés, F.; García-Solano, M.; González-González, R.; et al. Oral versus intramuscular administration of vitamin B12 for the treatment of patients with vitamin B12 deficiency: A pragmatic, randomized, multicenter, non-inferiority clinical trial undertaken in the primary healthcare setting (Project OB12). BMC Public Health 2012, 12, 394. [Google Scholar] [CrossRef] [PubMed]
- Eussen, S.J.; de Groot, L.C.; Clarke, R.; Schneede, J.; Ueland, P.M.; Hoefnagels, W.H.; van Staveren, W.A. Oral cyanocobalamin supplementation in older people with vitamin B12 deficiency: A dose-finding trial. Arch. Intern. Med. 2005, 165, 1167–1172. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Alaball, J.; Butler, C.C.; Cannings-John, R.; Goringe, A.; Hood, K.; McCaddon, A.; McDowell, I.; Papaioannou, A. Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency. Cochrane Database Syst. Rev. 2005, 20, CD004655. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.C.; Vidal-Alaball, J.; Cannings-John, R.; McCaddon, A.; Hood, K.; Papaioannou, A.; McDowell, I.; Goringe, A. Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency: A systematic review of randomized controlled trials. Fam. Pract. 2006, 23, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, L.; Qin, L.L.; Song, Y.; Vidal-Alaball, J.; Liu, T.H. Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency. Cochrane Database Syst. Rev. 2018, 3. [Google Scholar] [CrossRef] [PubMed]
- Andrès, E.; Fothergill, H.; Mecili, M. Efficacy of oral cobalamin (vitamin B12) therapy. Expert Opin. Pharmacother. 2010, 11, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Andrès, E.; Dali-Youcef, N.; Vogel, T.; Serraj, K.; Zimmer, J.G. Oral cobalamin (vitamin B12) treatment. An update. Int. J. Lab. Hematol. 2009, 31, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masucci, L.; Goeree, R. Vitamin B12 intramuscular injections versus oral supplements: A budget impact analysis. Ont. Health Technol. Assess. Ser. 2013, 13, 1–24. [Google Scholar] [PubMed]
- Arendt, J.; Nexø, E. Treatment response in vitamin B12 deficiency depends on the chosen vitamin B12 preparation. Ugeskr. Laeger. 2011, 173, 2634–2635. [Google Scholar] [PubMed]
- Castelli, M.C.; Friedman, K.; Sherry, J.; Brazzillo, K.; Genoble, L.; Bhargava, P.; Riley, M.G. Comparing the efficacy and tolerability of a new daily oral vitamin B12 formulation and intermittent intramuscular vitamin B12 in normalizing low cobalamin levels: A randomized, open-label, parallel-group study. Clin. Ther. 2011, 33, 358–371. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.Q.; Low, L.L.; Lee, K.H. Oral vitamin B12 replacement for the treatment of pernicious anemia. Front. Med. 2016, 3, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Kelsberg, G.; Safranek, S. Clinical inquiry: Is high-dose oral B12 a safe and effective alternative to a B12 injection? J. Fam. Pract. 2012, 61, 162–163. [Google Scholar] [PubMed]
- Andrès, E.; Kurtz, J.E.; Perrin, A.E.; Maloisel, F.; Demangeat, C.; Goichot, B.; Schlienger, J.L. Oral cobalamin therapy for the treatment of patients with food-cobalamin malabsorption. Am. J. Med. 2001, 111, 126–129. [Google Scholar] [CrossRef]
- Andrès, E.; Kaltenbach, G.; Noel, E.; Noblet-Dick, M.; Perrin, A.E.; Vogel, T.; Schlienger, J.L.; Berthel, M.; Blicklé, F. Efficacy of short-term oral cobalamin therapy for the treatment of cobalamin deficiencies related to food-cobalamin malabsorption. A study of 30 patients. Clin. Lab. Haematol. 2003, 25, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Kaltenbach, G.; Noblet-Dick, M.; Andrès, E.; Barnier-Figue, G.; Noel, E.; Vogel, T.; Perrin, A.E.; Martin-Hunyadi, C.; Berthel, M.; Kuntzmann, F. Réponse précoce au traitement oral par vitamine B12 chez des sujets âgés hypovitaminiques. Ann. Med. Interne (Paris) 2003, 154, 91–95. [Google Scholar] [PubMed]
- Andrès, E.; Kaltenbach, G.; Noblet-Dick, M.; Noel, E.; Perrin, A.E.; Vinzio, S.; Berthel, M.; Blicklé, J.F. Hematological response to short-term oral cyanocobalamin therapy for the treatment of cobalamin deficiencies in elderly patients. J. Nutr. Health Aging 2006, 10, 3–6. [Google Scholar] [PubMed]
- Andrès, E.; Loukili, N.H.; Noel, E.; Maloisel, F.; Vinzio, S.; Kaltenbach, G.; Caro-Sampara, F.; Blicklé, J.F. Oral cobalamin (daily dose of 1000 µg) therapy for the treatment of patients with pernicious anemia. An open label study of 10 patients. Curr. Ther. Res. 2005, 66, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Nyholm, E.; Turpin, P.; Swain, D.; Cunningham, B.; Daly, S.; Nightingale, P.; Fegan, C. Oral vitamin B12 can change our practice. Postgrad. Med. J. 2003, 79, 218–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delpre, G.; Stark, P.; Niv, Y. Sublingual therapy for cobalamin deficiency as an alternative to oral and parenteral cobalamin supplementation. Lancet 1999, 354, 740–741. [Google Scholar] [CrossRef]
- Andrès, E.; Serraj, K.; Federici, L.; Grosu, D.; Blicklé, J.F. Efficacité au long cours d’un traitement par cyanocobalamine administrée par voie orale dans le cadre des carences en vitamine B12: Etude de 22 cas. Rev. Med. Interne 2007, 28, 49. [Google Scholar] [CrossRef]
- Roth, M.; Orija, I. Oral vitamin B12 therapy in vitamin B12 deficiency. Am. J. Med. 2004, 116, 358. [Google Scholar] [CrossRef] [PubMed]
- Jehl, C.; Vogel, T.; Martin-Hunyadi, C.; Lang, P.O.; Andrès, E.; Berthel, M.; Kaltenbach, G. Effets de la supplémentation orale en vitamine B12 sur les fonctions cognitives de sujets âgés carencés. Ann. Gerontol. 2009, 2, 175–181. [Google Scholar]
- Del Bo, C.; Riso, P.; Gardana, C.; Brusamolino, A.; Battezzati, A.; Ciappellano, S. Effect of two different sublingual dosages of vitamin B12 on cobalamin nutritional status in vegans and vegetarians with a marginal deficiency: A randomized controlled trial. Clin. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Moleiro, J.; Mão de Ferro, S.; Ferreira, S.; Serrano, M.; Silveira, M.; Dias Pereira, A. Efficacy of Long-term Oral Vitamin B12 Supplementation after Total Gastrectomy: Results from a Prospective Study. GE Port. J. Gastroenterol. 2018, 25, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Schijns, W.; Homan, J.; van der Meer, L.; Janssen, I.M.; van Laarhoven, C.J.; Berends, F.J.; Aarts, E.O. Efficacy of oral compared with intramuscular vitamin B-12 supplementation after Roux-en-Y gastric bypass: A randomized controlled trial. Am. J. Clin. Nutr. 2018, 108, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Gomollón, F.; Gargallo, C.J.; Muñoz, J.F.; Vicente, R.; Lue, A.; Mir, A.; García-Alvarado, M.; Gracia, M.; García-López, S. Oral Cyanocobalamin is Effective in the Treatment of Vitamin B12 Deficiency in Crohn’s Disease. Nutrients 2017, 9, 308. [Google Scholar] [CrossRef] [PubMed]
- Monto, R.W.; Rebuck, J.W. Nasal instillation and inhalation of crystalline vitamin B12 in pernicious anemia. JAMA Arch. Intern. Med. 1954, 93, 219–230. [Google Scholar] [CrossRef]
- Slot, W.B.; Merkus, F.W.; Van Deventer, S.J.; Tytgat, G.N. Normalization of plasma vitamin B12 concentration by intranasal hydroxocobalamin in vitamin B12-deficient patients. Gastroenterology 1997, 113, 430–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Asselt, D.Z.; Merkus, F.W.; Russel, F.G.; Hoefnagels, W.H. Nasal absorption of hydroxocobalamin in healthy elderly adults. Br. J. Clin. Pharmacol. 1998, 45, 83–86. [Google Scholar] [CrossRef] [PubMed]
- García-Arieta, A.I.; Torrado-Santiago, S.; Goya, L.; Torrado, J.J. Spray-dried powders as nasal absorption enhancers of cyanocobalamin. Biol. Pharm. Bull. 2001, 24, 1411–1416. [Google Scholar] [CrossRef] [PubMed]
- Tillemans, M.P.; Donders, E.M.; Verweij, S.L.; van der Hoeven, R.T.; Kalisvaart, K.J. Effect of Administration Route on the Pharmacokinetics of Cobalamin in Elderly Patients: A Randomized Controlled Trial. Curr. Ther. Res. Clin. Exp. 2014, 76, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Andrès, E. Oral cobalamin therapy: It may be perhaps time to propose international recommendations? Presse. Med. 2012, 41, 895–898. [Google Scholar] [CrossRef] [PubMed]
- Vitetta, L.; Zhou, J.; Manuel, R.; Dal Forno, S.; Hall, S.; Rutolo, D. Route and type of formulation administered influences the absorption and disposition of vitamin B12 levels in serum. J. Funct. Biomater. 2018, 9, 12. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study Characteristics (Number of Patients) | Therapeutic Modalities | Results |
|---|---|---|
| Prospective randomized controlled study including patients with vitamin B12 deficiency related to Biermer’s disease, malabsorption and maldigestion (number of patients (n) = 38) [7]. | Oral crystalline cyanocobalamin: 2000 µg per day, for at least four months (“oral group”) vs. standard treatment with I.M. cyanocobalamin. |
|
| Prospective randomized open-label study including patients with vitamin B12 deficiency related to Biermer’s disease, and food-cobalamin malabsorption (n = 60) [8]. | Oral crystalline cyanocobalamin: 1000 µg, once daily for 10 days (“oral group”) or cobalamin I.M.: 1000 µg once daily for 10 days (“I.M. group”). After 10 days, both treatments were administered once a week for four weeks, and after that, once a month for life. |
|
| Randomized, parallel-group, double-blind, dose-finding trial including patients with vitamin B12 deficiency from not determined cause (n = 120) [10]. | Daily oral doses of 2.5, 100, 250, 500, and 1000 µg of cyanocobalamin administered for 16 weeks. |
|
| Controlled, randomized, multicenter, parallel, non-inferiority clinical trial (OB12 study) 23 primary healthcare centers in Spain (n = 350) [9]. | ‘I.M. vitamin B12 group’: 1000 µg on alternate days in weeks 1 and 2, 1000 µg per week in weeks 3–8, and 1000 µg per month in weeks 9–52 vs. “oral group”: 1000 µg per day in weeks 1–8 and 1000 µg per week in weeks 9–52. |
|
| Study Characteristics (Number of Patients) | Therapeutic Modalities | Results |
|---|---|---|
| Open prospective study of vitamin B12 deficiency related to food-cobalamin malabsorption (n = 10) [21]. | Oral crystalline cyanocobalamin: 650 µg per day, for at least three months. |
|
| Open prospective study of vitamin B12 deficiency related to food-cobalamin malabsorption (n = 30) [22]. | Oral crystalline cyanocobalamin: between 1000 µg and 250 µg per day, for one month. |
|
| Open prospective study of low vitamin B12 levels not related to pernicious anemia (n = 20) [23]. | Oral crystalline cyanocobalamin: between 1000 µg per day for at least one week. |
|
| Open prospective study of low vitamin B12 levels not related to pernicious anemia (n = 30) [24]. | Oral crystalline cyanocobalamin: between 1000 µg and 125 µg per day for at least one week. |
|
| Cohort study of low vitamin B12 levels mainly related to food-cobalamin malabsorption (n = 22) [28]. | Oral crystalline cyanocobalamin: 650 µg per day, for a median of 2.5 years. |
|
| Cohort study of patients with cognitive alteration related to low vitamin B12 levels mainly related to food-cobalamin malabsorption (n = 10) [30]. | Oral crystalline cyanocobalamin: 1000 µg per day, for a week, then 1000 µg per week, for a month, and 1000 µg per month, for at least three months. |
|
| Study Characteristics (Number of Patients) | Therapeutic Modalities | Results |
|---|---|---|
| Open prospective study of low vitamin B12 levels related to pernicious anemia (n = 10) [25]. | Oral crystalline cyanocobalamin: 1000 µg per day, for at least 3 months. |
|
| Prospective, case series of low vitamin B12 levels (n = 40), including 10 patients with Biermer’s disease [26]. | Loading dose of IM vitamin B12 till vitamin B12 level reached lower 25th centile (418 pg/mL) and then converted to oral vitamin B12 1000 μg per day, for 3–18 months. |
|
| Open prospective study of low vitamin B12 levels related to Biermer’s disease (n = 18) [27]. | Sublingual cobalamin for 7–12 days. |
|
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrès, E.; Zulfiqar, A.-A.; Serraj, K.; Vogel, T.; Kaltenbach, G. Systematic Review and Pragmatic Clinical Approach to Oral and Nasal Vitamin B12 (Cobalamin) Treatment in Patients with Vitamin B12 Deficiency Related to Gastrointestinal Disorders. J. Clin. Med. 2018, 7, 304. https://doi.org/10.3390/jcm7100304
Andrès E, Zulfiqar A-A, Serraj K, Vogel T, Kaltenbach G. Systematic Review and Pragmatic Clinical Approach to Oral and Nasal Vitamin B12 (Cobalamin) Treatment in Patients with Vitamin B12 Deficiency Related to Gastrointestinal Disorders. Journal of Clinical Medicine. 2018; 7(10):304. https://doi.org/10.3390/jcm7100304
Chicago/Turabian StyleAndrès, Emmanuel, Abrar-Ahmad Zulfiqar, Khalid Serraj, Thomas Vogel, and Georges Kaltenbach. 2018. "Systematic Review and Pragmatic Clinical Approach to Oral and Nasal Vitamin B12 (Cobalamin) Treatment in Patients with Vitamin B12 Deficiency Related to Gastrointestinal Disorders" Journal of Clinical Medicine 7, no. 10: 304. https://doi.org/10.3390/jcm7100304
APA StyleAndrès, E., Zulfiqar, A.-A., Serraj, K., Vogel, T., & Kaltenbach, G. (2018). Systematic Review and Pragmatic Clinical Approach to Oral and Nasal Vitamin B12 (Cobalamin) Treatment in Patients with Vitamin B12 Deficiency Related to Gastrointestinal Disorders. Journal of Clinical Medicine, 7(10), 304. https://doi.org/10.3390/jcm7100304