
Parenteral, Non-Intravenous Analgesia in Acute Traumatic Pain—A Narrative Review Based on a Systematic Literature Search
 ,
, {kind=link}
Abstract
:1. Introduction
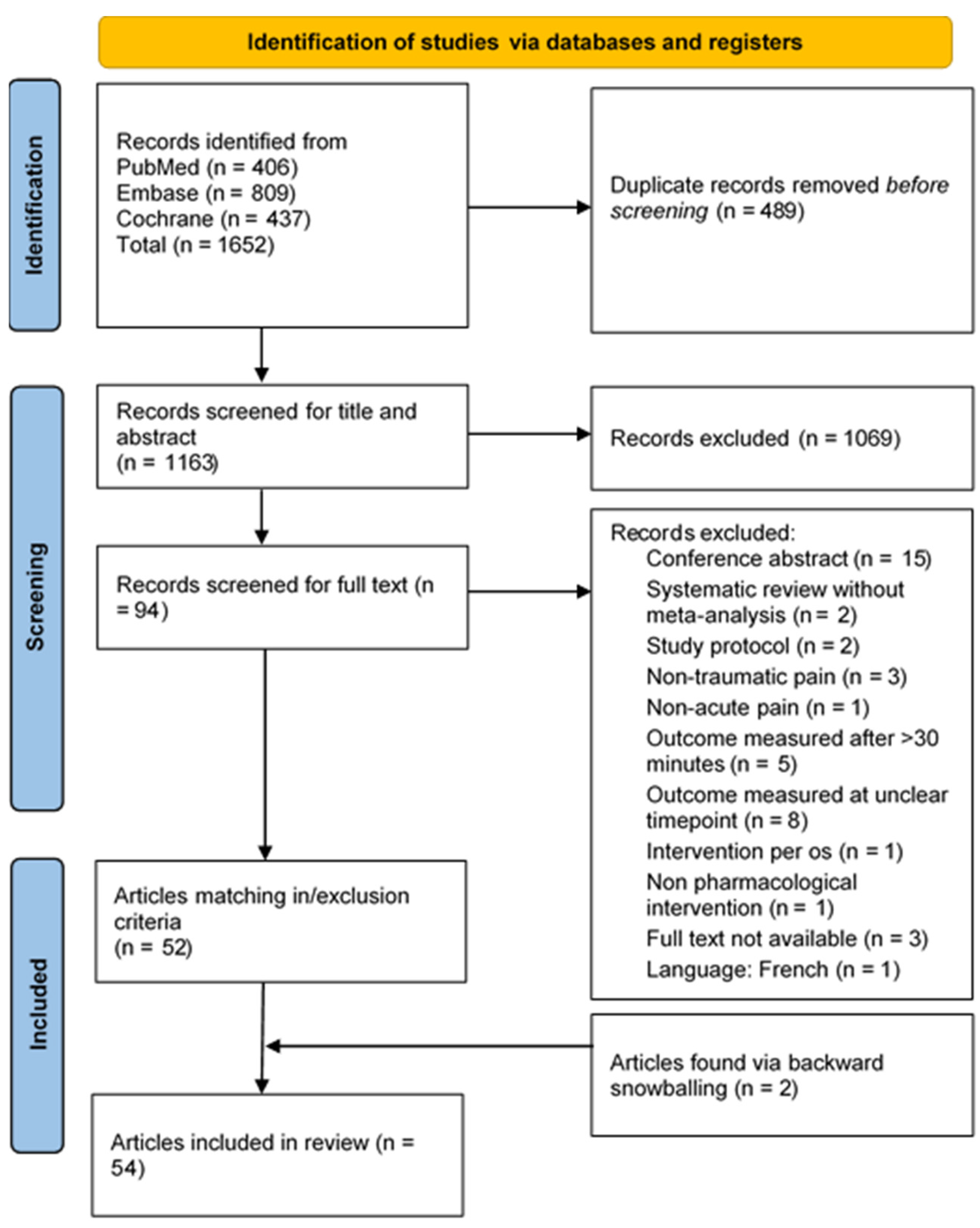
2. Methods
2.1. Search
2.2. Inclusion and Exclusion Criteria
2.3. Article Screening
3. Results
4. Routes of Administration
4.1. Inhalation
4.2. Intranasal Administration
4.3. Oromucosal Administration
5. Analgesics
5.1. Methoxyflurane
Conclusion
5.2. Nitrous Oxide
Conclusion
5.3. Fentanyl
5.3.1. Intranasal Fentanyl
5.3.2. Fentanyl Buccal Tablets
5.3.3. Oral Transmucosal Fentanyl Citrate
5.3.4. Nebulized Fentanyl
5.3.5. Conclusion
5.4. Ketamine
5.4.1. Intranasal Ketamine
5.4.2. Nebulized Ketamine
5.4.3. Conclusion
5.5. Sufentanil
5.5.1. Intranasal Sufentanil
5.5.2. Sublingual Sufentanil Tablets
5.5.3. Conclusion
6. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Berben, S.A.; Meijs, T.H.; van Dongen, R.T.; van Vugt, A.B.; Vloet, L.C.; Mintjes-de Groot, J.J.; van Achterberg, T. Pain prevalence and pain relief in trauma patients in the Accident & Emergency department. Injury 2008, 39, 578–585. [Google Scholar] [PubMed]
- Dhir, S.; Sondekoppam, R.V.; Ganapathy, S. Pharmacologic management of acute pain in trauma. In Trauma Anesthesia, 2nd ed.; Smith, C.E., Ed.; Cambridge University Press: Cambridge, UK, 2015; pp. 244–266. [Google Scholar]
- Ritter, J.; Lewis, L.; Mant, T.; Ferro, A. A Textbook of Clinical Pharmacology and Therapeutics; CRC Press: London, UK, 2008; Available online: https://www.pharmaresearchlibrary.com/wp-content/uploads/2013/03/A-Textbook-of-Clinical-Pharmacology-and-Therapeutics-5th-edition.pdf (accessed on 4 January 2024).
- Prottengeier, J.; Albermann, M.; Heinrich, S.; Birkholz, T.; Gall, C.; Schmidt, J. The prehospital intravenous access assessment: A prospective study on intravenous access failure and access delay in prehospital emergency medicine. Eur. J. Emerg. Med. 2016, 23, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Carr, B.G.; Brachet, T.; David, G.; Duseja, R.; Branas, C.C. The time cost of prehospital intubation and intravenous access in trauma patients. Prehospital Emerg. Care 2008, 12, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Engels, P.T.; Passos, E.; Beckett, A.N.; Doyle, J.D.; Tien, H.C. IV access in bleeding trauma patients: A performance review. Injury 2014, 45, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Olsen, M.F.; Bjerre, E.; Hansen, M.D.; Hilden, J.; Landler, N.E.; Tendal, B.; Hróbjartsson, A. Pain relief that matters to patients: Systematic review of empirical studies assessing the minimum clinically important difference in acute pain. BMC Med. 2017, 15, 35. [Google Scholar] [CrossRef]
- Hickey, A.J. Back to the future: Inhaled drug products. J. Pharm. Sci. 2013, 102, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Newman, S.P. Drug delivery to the lungs: Challenges and opportunities. Ther. Deliv. 2017, 8, 647–661. [Google Scholar] [CrossRef] [PubMed]
- Grassin-Delyle, S.; Buenestado, A.; Naline, E.; Faisy, C.; Blouquit-Laye, S.; Couderc, L.-J.; Le Guen, M.; Fischler, M.; Devillier, P. Intranasal drug delivery: An efficient and non-invasive route for systemic administration: Focus on opioids. Pharmacol. Ther. 2012, 134, 366–379. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Yoo, J.-W.; Roh, H.-J.; Lee, M.-K.; Chung, S.-J.; Shim, C.-K.; Kim, D.-D. Transport of anti-allergic drugs across the passage cultured human nasal epithelial cell monolayer. Eur. J. Pharm. Sci. 2005, 26, 203–210. [Google Scholar] [CrossRef]
- Kundoor, V.; Dalby, R.N. Effect of formulation- and administration-related variables on deposition pattern of nasal spray pumps evaluated using a nasal cast. Pharm. Res. 2011, 28, 1895–1904. [Google Scholar] [CrossRef]
- Foo, M.Y.; Cheng, Y.-S.; Su, W.-C.; Donovan, M.D. The influence of spray properties on intranasal deposition. J. Aerosol Med. 2007, 20, 495–508. [Google Scholar] [CrossRef] [PubMed]
- Pires, A.; Fortuna, A.; Alves, G.; Falcão, A. Intranasal drug delivery: How, why and what for? J. Pharm. Pharm. Sci. 2009, 12, 288–311. [Google Scholar] [CrossRef] [PubMed]
- National Association of State EMS Officials (NANEMSO). National Model EMS Clinical Guidelines 2022. Available online: https://nasemso.org/wp-content/uploads/National-Model-EMS-Clinical-Guidelines_2022.pdf (accessed on 2 January 2024).
- Pre-Hospital Emergency Care Council (PHECC). Clinical Practice Guidelines—2021 Edition (Updated June 2023). Naas, Co Kildare, Ireland. 2021. Available online: https://www.phecit.ie/PHECC/Clinical_Resources/Clinical_Practice_Guidelines__CPGs_/2021_edition_CPGs.aspx (accessed on 2 January 2024).
- St John Ambulance Australia Ltd. Clinical Practice Guidelines for Health Professionals 2022. Available online: https://stjohn.org.au/assets/uploads/media%20releases/CPGsHP%20v4%202022%20for%20website.pdf (accessed on 2 January 2024).
- Zhang, H.; Zhang, J.; Streisand, J.B. Oral Mucosal Drug Delivery. Clin. Pharmacokinet. 2002, 41, 661–680. [Google Scholar] [CrossRef] [PubMed]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 4116, Methoxyflurane 2023. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Methoxyflurane (accessed on 15 September 2023).
- Medical Developments UK Limited. PENTHROX 99.9%, 3 mL Inhalation Vapour, Liquid SmPC. 2020. Available online: https://www.medicines.org.uk/emc/product/1939/smpc (accessed on 15 September 2023).
- Fabbri, A.; Borobia, A.M.; Ricard-Hibon, A.; Coffey, F.; Caumont-Prim, A.; Montestruc, F.; Soldi, A.; Lugilde, S.T.; Dickerson, S. Low-dose methoxyflurane versus standard of care analgesics for emergency trauma pain: A systematic review and meta-analysis of pooled data. J. Pain Res. 2021, 14, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Fu, X.; Ren, Y.-F.; Tan, S.-Y.; Xiang, S.-R.; Zheng, C.; You, F.-M.; Shi, W.; Li, L.-J. Does Inhaled Methoxyflurane Implement Fast and Efficient Pain Management in Trauma Patients? A Systematic Review and Meta-Analysis. Pain Ther. 2021, 10, 651–674. [Google Scholar] [CrossRef] [PubMed]
- Coffey, F.; Dissmann, P.; Mirza, K.; Lomax, M. Methoxyflurane Analgesia in Adult Patients in the Emergency Department: A Subgroup Analysis of a Randomized, Double-blind, Placebo-controlled Study (STOP!). Adv. Ther. 2016, 33, 2012–2031. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, S.; Voza, A.; Serra, S.; Ruggiano, G.; Carpinteri, G.; Gangitano, G.; Intelligente, F.; Bonafede, E.; Sblendido, A.; Farina, A.; et al. Analgesic Efficacy, Practicality and Safety of Inhaled Methoxyflurane versus Standard Analgesic Treatment for Acute Trauma Pain in the Emergency Setting: A Randomised, Open-Label, Active-Controlled, Multicentre Trial in Italy (MEDITA). Adv. Ther. 2019, 36, 3030–3046. [Google Scholar] [CrossRef]
- Ricard-Hibon, A.; Lecoules, N.; Savary, D.; Jacquin, L.; Wiel, E.; Deschamps, P.; Douplat, M.; Montestruc, F.; Chomier, B.; Tazarourte, K.; et al. Inhaled methoxyflurane for the management of trauma related pain in patients admitted to hospital emergency departments: A randomised, double-blind placebo-controlled trial (PenASAP study). Eur. J. Emerg. Med. Off. J. Eur. Soc. Emerg. Med. 2020, 27, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Borobia, A.M.; Collado, S.G.; Cardona, C.C.; Pueyo, R.C.; Alonso, C.F.; Torres, I.P.; González, M.C.; Codesido, J.R.C.; Betegón, M.A.; Barcela, L.A.; et al. Inhaled Methoxyflurane Provides Greater Analgesia and Faster Onset of Action versus Standard Analgesia in Patients with Trauma Pain: InMEDIATE: A Randomized Controlled Trial in Emergency Departments. Ann. Emerg. Med. 2020, 75, 315–328. [Google Scholar] [CrossRef]
- Brichko, L.; Gaddam, R.; Roman, C.; O’reilly, G.; Luckhoff, C.; Jennings, P.; Smit, D.V.; Cameron, P.; Mitra, B. Rapid Administration of Methoxyflurane to Patients in the Emergency Department (RAMPED) Study: A Randomized Controlled Trial of Methoxyflurane versus Standard Care. Acad. Emerg. Med. 2021, 28, 164–171. [Google Scholar] [CrossRef]
- Coffey, F.; Wright, J.; Hartshorn, S.; Hunt, P.; Locker, T.; Mirza, K.; Dissmann, P. STOP!: A randomised, double-blind, placebo-controlled study of the efficacy and safety of methoxyflurane for the treatment of acute pain. Emerg. Med. J. 2014, 31, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Hartshorn, S.; Dissmann, P.; Coffey, F.; Lomax, M. Low-dose methoxyflurane analgesia in adolescent patients with moderate-to-severe trauma pain: A subgroup analysis of the STOP! study. J. Pain Res. 2019, 12, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Serra, S.; Voza, A.; Ruggiano, G.; Fabbri, A.; Bonafede, E.; Sblendido, A.; Soldi, A.; Farina, A. Efficacy, practicality, and safety of inhaled methoxyflurane in elderly patients with acute trauma pain: Subgroup analysis of a randomized, controlled, multicenter, open-label trial (medita). J. Pain Res. 2020, 13, 1777–1784. [Google Scholar] [CrossRef]
- Voza, A.; Ruggiano, G.; Serra, S.; Carpinteri, G.; Gangitano, G.; Intelligente, F.; Bonafede, E.; Sblendido, A.; Farina, A.; Soldi, A.; et al. Inhaled methoxyflurane versus intravenous morphine for severe trauma pain in the emergency setting: Subgroup analysis of MEDITA, a multicenter, randomized, controlled, open-label trial. J. Pain Res. 2020, 13, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.D.; Rowan, E.; Spaight, R.; Siriwardena, A.N. Evaluation of the effectiveness and costs of inhaled methoxyflurane versus usual analgesia for prehospital injury and trauma: Non-randomised clinical study. BMC Emerg. Med. 2022, 22, 122. [Google Scholar] [CrossRef] [PubMed]
- Hass, S.A.; Andersen, S.T.; Andersen, M.P.S.; Nielsen, O.J. Atmospheric Chemistry of Methoxyflurane (CH3OCF2CHCl2): Kinetics of the gas-phase reactions with OH radicals, Cl atoms and O3. Chem. Phys. Lett. 2019, 722, 119–123. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 948, Nitrous Oxide 2023. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Nitrous-Oxide (accessed on 20 September 2023).
- Kariman, H.; Majidi, A.; Amini, A.; Dolatabadi, A.A.; Derakhshanfar, H.; Hatamabadi, H.; Shahrami, A.; Yaseri, M.; Sheibani, K. Nitrous oxide/oxygen compared with fentanyl in reducing pain among adults with isolated extremity trauma: A randomized trial. Emerg. Med. Australas. 2011, 23, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Motamed, H.; Barzegari, H.; Verki, M.M.; Behdadfar, A. A Comparison between the analgesic—Sedative effects of ketamine and nitrous oxide in Bones’ fracture pain control: A randomized clinical trial. Jundishapur J. Nat. Pharm. Prod. 2017, 12, e17395. [Google Scholar] [CrossRef]
- Ducassé, J.; Siksik, G.; Durand-Béchu, M.; Couarraze, S.; Vallé, B.; Lecoules, N.; Marco, P.; Lacombe, T.; Bounes, V. Nitrous oxide for early analgesia in the emergency setting: A randomized, double-blind multicenter prehospital trial. Acad. Emerg. Med. 2013, 20, 178–184. [Google Scholar] [CrossRef]
- Porter, K.M.; Siddiqui, M.K.; Sharma, I.; Dickerson, S.; Eberhardt, A. Management of trauma pain in the emergency setting: Low-dose methoxyflurane or nitrous oxide? A systematic review and indirect treatment comparison. J. Pain Res. 2018, 11, 11–21. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 3345, Fentanyl 2023. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Fentanyl (accessed on 19 October 2023).
- Hachimi-Idrissi, S.; Dobias, V.; Hautz, W.E.; Leach, R.; Sauter, T.C.; Sforzi, I.; Coffey, F. Approaching acute pain in emergency settings; European Society for Emergency Medicine (EUSEM) guidelines-part 2: Management and recommendations. Intern. Emerg. Med. 2020, 15, 1141–1155. [Google Scholar] [CrossRef] [PubMed]
- Schug, S.A.; Mott, J.F.; Halliwell, R.; Palmer, G.M.; Alcock, M.; APM:SE Working Group of the Australian and New Zealand College of Anaesthetists and Faculty of Pain Medicine. Acute Pain Management: Scientific Evidence, 5th ed.; ANZCA & FPM: Melbourne, Australia, 2020. [Google Scholar]
- Committee on Tactical Combat Casualty Care (CoTCCC). Tactical Combat Casualty Care (TCCC) Guidelines for Medical Personnel 2021. Available online: https://learning-media.allogy.com/api/v1/pdf/1045f287-baa4-4990-8951-de517a262ee2/contents (accessed on 19 October 2023).
- Isfahani, M.N.; Shokoohi, O.; Golshani, K. Intranasal ketamine versus intranasal fentanyl on pain management in isolated traumatic patients. J. Res. Med. Sci. 2022, 27, 1. [Google Scholar]
- Lynch, T.V.; Callas, P.W.; Peterson, T.D.; Schlein, S.M. Intranasal Fentanyl for On-the-Hill Analgesia by Ski Patrol. Wilderness Environ. Med. 2022, 33, 296–303. [Google Scholar] [CrossRef]
- Chew, K.; Shaharudin, A. An open-label randomised controlled trial on the efficacy of adding intranasal fentanyl to intravenous tramadol in patients with moderate to severe pain following acute musculoskeletal injuries. Singap. Med. J. 2017, 58, 601–605. [Google Scholar] [CrossRef]
- Shear, M.L.; Adler, J.N.; Shewakramani, S.; Ilgen, J.; Soremekun, O.A.; Nelson, S.; Thomas, S.H. Transbuccal fentanyl for rapid relief of orthopedic pain in the ED. Am. J. Emerg. Med. 2010, 28, 847–852. [Google Scholar] [CrossRef]
- Arthur, A.O.; Mushtaq, N.; Mumma, S.; Thomas, S.H. Fentanyl buccal tablet versus oral oxycodone for Emergency Department treatment of musculoskeletal pain. J. Emerg. Med. Trauma Acute Care 2015, 2015, 6. [Google Scholar] [CrossRef]
- Wedmore, I.S.; Kotwal, R.S.; McManus, J.G.; Pennardt, A.; Talbot, T.S.; Fowler, M.; McGhee, L. Safety and efficacy of oral transmucosal fentanyl citrate for prehospital pain control on the battlefield. J. Trauma Acute Care Surg. 2012, 73, S490–S495. [Google Scholar] [CrossRef]
- Farahmand, S.; Shiralizadeh, S.; Talebian, M.-T.; Bagheri-Hariri, S.; Arbab, M.; Basirghafouri, H.; Saeedi, M.; Sedaghat, M.; Mirzababai, H. Nebulized fentanyl vs. intravenous morphine for ED patients with acute limb pain: A randomized clinical trial. Am. J. Emerg. Med. 2014, 32, 1011–1015. [Google Scholar] [CrossRef] [PubMed]
- Verki, M.M.; Mozafari, J.; Tirandaz, F.; Motamed, H.; Khazaeli, A. Efficacy of nebulized fentanyl and low dose ketamine for pain control of patients with long bone fractures: A randomized, double-blind, clinical trial. Afr. J. Emerg. Med. 2019, 9, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.D. The epidemic of fentanyl misuse and overdoses: Challenges and strategies. World Psychiatry 2021, 20, 195–196. [Google Scholar] [CrossRef]
- Mauermann, E.; Filitz, J.; Dolder, P.; Rentsch, K.M.; Bandschapp, O.; Ruppen, W. Does Fentanyl Lead to Opioid-induced Hyperalgesia in Healthy Volunteers? A Double-blind, Randomized, Crossover Trial. Anesthesiology 2016, 124, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Silverman, S.M.; Hansen, H.; Patel, V.B.; Manchikanti, L. A comprehensive review of opioid-induced hyperalgesia. Pain Physician 2011, 14, 145–161. [Google Scholar] [CrossRef]
- Lyons, P.J.; Rivosecchi, R.M.; Nery, J.P.; Kane-Gill, S.L. Fentanyl-induced hyperalgesia in acute pain management. J. Pain Palliat. Care Pharmacother. 2015, 29, 153–160. [Google Scholar] [CrossRef]
- Oye, I.; Paulsen, O.; Maurset, A. Effects of ketamine on sensory perception: Evidence for a role of N-methyl-D-aspartate receptors. J. Pharmacol. Exp. Ther. 1992, 260, 1209–1213. [Google Scholar] [PubMed]
- Pfenninger, E.; Baier, C.; Claus, S.; Hege, G. Psychometric changes as well as analgesic action and cardiovascular adverse effects of ketamine racemate versus s-(+)-ketamine in subanesthetic doses. Anaesthesist 1994, 43 (Suppl. 2), S68–S75. [Google Scholar] [PubMed]
- McIntyre, R.S.; Rosenblat, J.D.; Nemeroff, C.B.; Sanacora, G.; Murrough, J.W.; Berk, M.; Brietzke, E.; Dodd, S.; Gorwood, P.; Ho, R.; et al. Synthesizing the evidence for ketamine and esketamine in treatment-resistant depression: An international expert opinion on the available evidence and implementation. Am. J. Psychiatry 2021, 178, 383–399. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 182137, Esketamine 2024. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Esketamine (accessed on 4 January 2024).
- National Center for Biotechnology Information. PubChem Compound Summary for CID 3821, Ketamine 2024. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Ketamine (accessed on 4 January 2024).
- Shimonovich, S.; Gigi, R.; Shapira, A.; Sarig-Meth, T.; Nadav, D.; Rozenek, M.; West, D.; Halpern, P. Intranasal ketamine for acute traumatic pain in the Emergency Department: A prospective, randomized clinical trial of efficacy and safety. BMC Emerg. Med. 2016, 16, 43. [Google Scholar] [CrossRef]
- Parvizrad, R.; Pakniyat, A.; Malekianzadeh, B.; Almasi-Hashiani, A. Comparing the analgesic effect of intranasal with intravenous ketamine in isolated orthopedic trauma: A randomized clinical trial. Turk. J. Emerg. Med. 2017, 17, 99–103. [Google Scholar] [CrossRef]
- Mohammadshahi, A.; Abdolrazaghnejad, A.; Nikzamir, H.; Safaie, A. Intranasal Ketamine Administration for Narcotic Dose Decrement in Patients Suffering from Acute Limb Trauma in Emergency Department: A Double-Blind Randomized Placebo-Controlled Trial. Adv. J. Emerg. Med. 2018, 2, e30. [Google Scholar]
- Bouida, W.; Ali, K.B.H.; Ben Soltane, H.; Msolli, M.A.; Boubaker, H.; Sekma, A.; Beltaief, K.; Grissa, M.H.; Methamem, M.; Boukef, R.; et al. Effect on Opioids Requirement of Early Administration of Intranasal Ketamine for Acute Traumatic Pain. Clin. J. Pain 2020, 36, 458–462. [Google Scholar] [CrossRef]
- Shrestha, R.; Pant, S.; Shrestha, A.; Batajoo, K.H.; Thapa, R.; Vaidya, S. Intranasal ketamine for the treatment of patients with acute pain in the emergency department. World J. Emerg. Med. 2016, 7, 19–24. [Google Scholar] [CrossRef]
- Arumugam, C.; Muhamad, N.A.N. Comparing nebulized ketamine with Entonox for acute traumatic pain in the Emergency Department: A pilot randomized trial. J. Emerg. Med. Trauma Acute Care 2022, 2022, 27. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 41693, Sufentanil 2023. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Sufentanil (accessed on 18 October 2023).
- Miner, J.R.; Rafique, Z.; Minkowitz, H.S.; DiDonato, K.P.; Palmer, P.P. Sufentanil sublingual tablet 30mcg for moderate-to-severe acute pain in the ED. Am. J. Emerg. Med. 2018, 36, 954–961. [Google Scholar] [CrossRef]
- Helmers, J.H.J.H.; Noorduin, H.; Van Peer, A.; Van Leeuwen, L.; Zuurmond, W.W.A. Comparison of intravenous and intranasal sufentanil absorption and sedation. Can. J. Anaesth. 1989, 36, 494–497. [Google Scholar] [CrossRef]
- Blancher, M.; Maignan, M.; Clapé, C.; Quesada, J.-L.; Collomb-Muret, R.; Albasini, F.; Ageron, F.-X.; Fey, S.; Wuyts, A.; Banihachemi, J.-J.; et al. Intranasal sufentanil versus intravenous morphine for acute severe trauma pain: A double-blind randomized non-inferiority study. PLoS Med. 2019, 16, e1002849. [Google Scholar] [CrossRef] [PubMed]
- Malinverni, S.; Kreps, B.; Lucaccioni, T.; Bouazza, F.-Z.; Bartiaux, M.; Plumacker, A.; Pascu, A.; Towo, P.Y. Effect of intranasal sufentanil on acute post-traumatic pain in the emergency department: A randomised controlled trial. Emerg. Med. J. 2024, 41, 83–88. [Google Scholar] [CrossRef]
- Lemoel, F.; Contenti, J.; Cibiera, C.; Rapp, J.; Occelli, C.; Levraut, J. Intranasal sufentanil given in the emergency department triage zone for severe acute traumatic pain: A randomized double-blind controlled trial. Intern. Emerg. Med. 2019, 14, 571–579. [Google Scholar] [CrossRef]
- Bitter, C. Transmucosal Nasal Drug Delivery: Pharmacokinetics and Pharmacodynamics of Nasally Applied Esketamine. Ph.D. Thesis, University of Basel, Basel, Switzerland, 2011; pp. 57–78. [Google Scholar]
- Wong, K.Y.; Lau, J.S.K.; Siu, A.Y.C.; Kan, P.G. A randomized non-inferiority pilot study on the use of methoxyflurane (Penthrox) for pain control in the emergency department. Hong Kong J. Emerg. Med. 2022, 29, 203–211. [Google Scholar] [CrossRef]
- Lim, K.; Koh, Z.; Ng, Y.; Fook-Chong, S.; Ho, A.; Doctor, N.; Said, N.; Ong, M. Comparison of inhalational methoxyflurane (Penthrox) and intramuscular tramadol for prehospital analgesia. Singap. Med. J. 2021, 62, 281–286. [Google Scholar] [CrossRef]
- Egger, A.; Huber, T.; Heschl, S.; Fiegl, J.; Burger, J.; Trimmel, H.; Schreiber, W.; Niederer, M.; Tscherny, K.; Roth, D. Efficacy and Safety of Methoxyflurane for Treatment of Acute Traumatic Pain by EMTs during Alpine Rescue Operations: The “PainDrop” Trial. Prehospital Emerg. Care 2023, 27, 987–992. [Google Scholar] [CrossRef]
- Trimmel, H.; Egger, A.; Doppler, R.; Pimiskern, M.; Voelckel, W.G. Usability and effectiveness of inhaled methoxyflurane for prehospital analgesia—A prospective, observational study. BMC Emerg. Med. 2022, 22, 8. [Google Scholar] [CrossRef]
- Rydlöv, H.S.; Fjose, L.O.; Heyerdahl, F. Pain Management with Inhalation of Methoxyflurane Administrated by Non-Medical Ski Patrol: A Quality Assessment Study. Pain Ther. 2023, 12, 1455–1463. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.-L.; Yu, J.-Q.; Liu, Q.; Gao, H.-X.; Dai, Y.-L.; Zhang, J.-J.; Wang, Y.-L.; Zhang, T.-T.; Yang, J.-J.; Li, Y.-X. Analgesic Effect of Nitrous Oxide/Oxygen Mixture for Traumatic Pain in the Emergency Department: A Randomized, Double-Blind Study. J. Emerg. Med. 2019, 57, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Jokar, A.; Ahmadi, K.; Hajimaghsoodi, L.; Ketabi, S. Use of fentanyl patch and intravenous morphine for treatment of leg bone fracture: Treatment profile, and clinical effectiveness. Open Access Maced. J. Med. Sci. 2018, 6, 2301–2305. [Google Scholar] [CrossRef] [PubMed]
- Kreps, B.; Malinverni, S.; Carles, E.; Bartiaux, M.; Towo, P.Y. Intranasal sufentanil compared with a classic protocol for acute pain management in an emergency department: A prospective sequential study. Trauma 2023, 25, 23–28. [Google Scholar] [CrossRef]
- Steenblik, J.; Goodman, M.; Davis, V.; Gee, C.; Hopkins, C.L.; Stephen, R.; Madsen, T. Intranasal sufentanil for the treatment of acute pain in a winter resort clinic. Am. J. Emerg. Med. 2012, 30, 1817–1821. [Google Scholar] [CrossRef] [PubMed]
- Jalili, M.; Fathi, M.; Moradi-Lakeh, M.; Zehtabchi, S. Sublingual buprenorphine in acute pain management: A double-blind randomized clinical trial. Ann. Emerg. Med. 2012, 59, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Pietsch, U.; Berger, Y.; Schurter, D.; Theiler, L.; Wenzel, V.; Meuli, L.; Grünenfelder, A.; Albrecht, R. Nasal nalbuphine analgesia in prehospital trauma managed by first-responder personnel on ski slopes in Switzerland: An observational cohort study. Scand. J. Trauma Resusc. Emerg. Med. 2021, 29, 36. [Google Scholar] [CrossRef]
- Scott, J.L.; Smith, M.S.; Sanford, S.M.; Shesser, R.F.; Rosenthal, R.E.; Smith, J.P.; Feied, C.F.; Ghezzi, K.T.; Hunt, D.M. Effectiveness of transnasal butorphanol for the treatment of musculoskeletal pain. Am. J. Emerg. Med. 1994, 12, 469–471. [Google Scholar] [CrossRef]
- Wermeling, D.P.; Clinch, T.; Rudy, A.C.; Dreitlein, D.; Suner, S.; Lacouture, P.G. A Multicenter, Open-Label, Exploratory Dose-Ranging Trial of Intranasal Hydromorphone for Managing Acute Pain from Traumatic Injury. J. Pain 2010, 11, 24–31. [Google Scholar] [CrossRef]
- Qureshi, I.; A Pathan, S.; Qureshi, R.S.; Thomas, S.H. Intramuscular versus oral diclofenac for acute pain in adults with acute musculoskeletal injuries presenting to the ED setting: A prospective, double-blind, double-dummy, randomised controlled trial. Emerg. Med. J. 2019, 36, 401–406. [Google Scholar] [CrossRef]
- Serinken, M.; Eken, C.; Elicabuk, H. Topical Ketoprofen versus Placebo in Treatment of Acute Ankle Sprain in the Emergency Department. Foot Ankle Int. 2016, 37, 989–993. [Google Scholar] [CrossRef]
- Turner, N.J.; Long, D.A.; Bongiorno, J.R.; Katoski, T.P.; Jin, L.M.; Horsch, J.P.; Ahern, B.J. Comparing two doses of intramuscular ketorolac for treatment of acute musculoskeletal pain in a military emergency department. Am. J. Emerg. Med. 2021, 50, 142–147. [Google Scholar] [CrossRef]
- Turturro, M.A.; Paris, P.M.; Seaberg, D.C. Intramuscular ketorolac versus oral ibuprofen in acute musculoskeletal pain. Ann. Emerg. Med. 1995, 26, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Aksel, G.; Güler, S.; Doğan, N.; Çorbacioğlu, Ş.K. A randomized trial comparing intravenous paracetamol, topical lidocaine, and ice application for treatment of pain associated with scorpion stings. Hum. Exp. Toxicol. 2015, 34, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Mohammadkarimi, N.; Jafari, M.; Mellat, A.; Kazemi, E.; Shirali, A. Evaluation of efficacy of intra-nasal lidocaine for headache relief in patients refer to emergency department. J. Res. Med. Sci. 2014, 19, 331–335. [Google Scholar] [PubMed]
- Turgut, K.; Yavuz, E.; Gülaçtı, U.; Aydın, İ.; Sönmez, C.; Aktaş, N.; Arslan, E. Comparison of Intravenous Paracetamol, Dexketoprofen Trometamol, or Topical Lidocaine Use for Pain Relief in Scorpion Stings: A Placebo-Controlled, Randomized Study. Wilderness Environ. Med. 2022, 33, 379–385. [Google Scholar] [CrossRef]
- Mohammadjani, M.K.; Jafaraghaee, F.; Yosefbeyk, F.; Nejad, E.K.; Javadi-Pashaki, N. Effect of Topical Sesame Oil on the Severity of Pain in Patients with Limb Trauma: A Randomized Controlled Trial. J. Chiropr. Med. 2022, 21, 204–212. [Google Scholar] [CrossRef]
- Kocak, A.O. Intradermal mesotherapy versus systemic therapy in the treatment of musculoskeletal pain: A prospective randomized study. Am. J. Emerg. Med. 2019, 37, 2061–2065. [Google Scholar] [CrossRef]
- Pickering, G.; Moustafa, F.; Macian, N.; Schmidt, J.; Pereira, B.; Dubray, C. A new transmucous-buccal formulation of acetaminophen for acute traumatic pain: A non-inferiority, randomized, double-blind, clinical trial. Pain Physician 2015, 18, 249–257. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Grunt, M.N.; de Jong, B.; Hollmann, M.W.; Ridderikhof, M.L.; Weenink, R.P. Parenteral, Non-Intravenous Analgesia in Acute Traumatic Pain—A Narrative Review Based on a Systematic Literature Search. J. Clin. Med. 2024, 13, 2560. https://doi.org/10.3390/jcm13092560
de Grunt MN, de Jong B, Hollmann MW, Ridderikhof ML, Weenink RP. Parenteral, Non-Intravenous Analgesia in Acute Traumatic Pain—A Narrative Review Based on a Systematic Literature Search. Journal of Clinical Medicine. 2024; 13(9):2560. https://doi.org/10.3390/jcm13092560
Chicago/Turabian Stylede Grunt, Midas N., Bianca de Jong, Markus W. Hollmann, Milan L. Ridderikhof, and Robert P. Weenink. 2024. "Parenteral, Non-Intravenous Analgesia in Acute Traumatic Pain—A Narrative Review Based on a Systematic Literature Search" Journal of Clinical Medicine 13, no. 9: 2560. https://doi.org/10.3390/jcm13092560