
A Cross-Sectional Study of Factors Predicting the Duration of the Efficacy of Viscosupplementation in Knee Osteoarthritis

Abstract
:1. Introduction
2. Patients and Methods
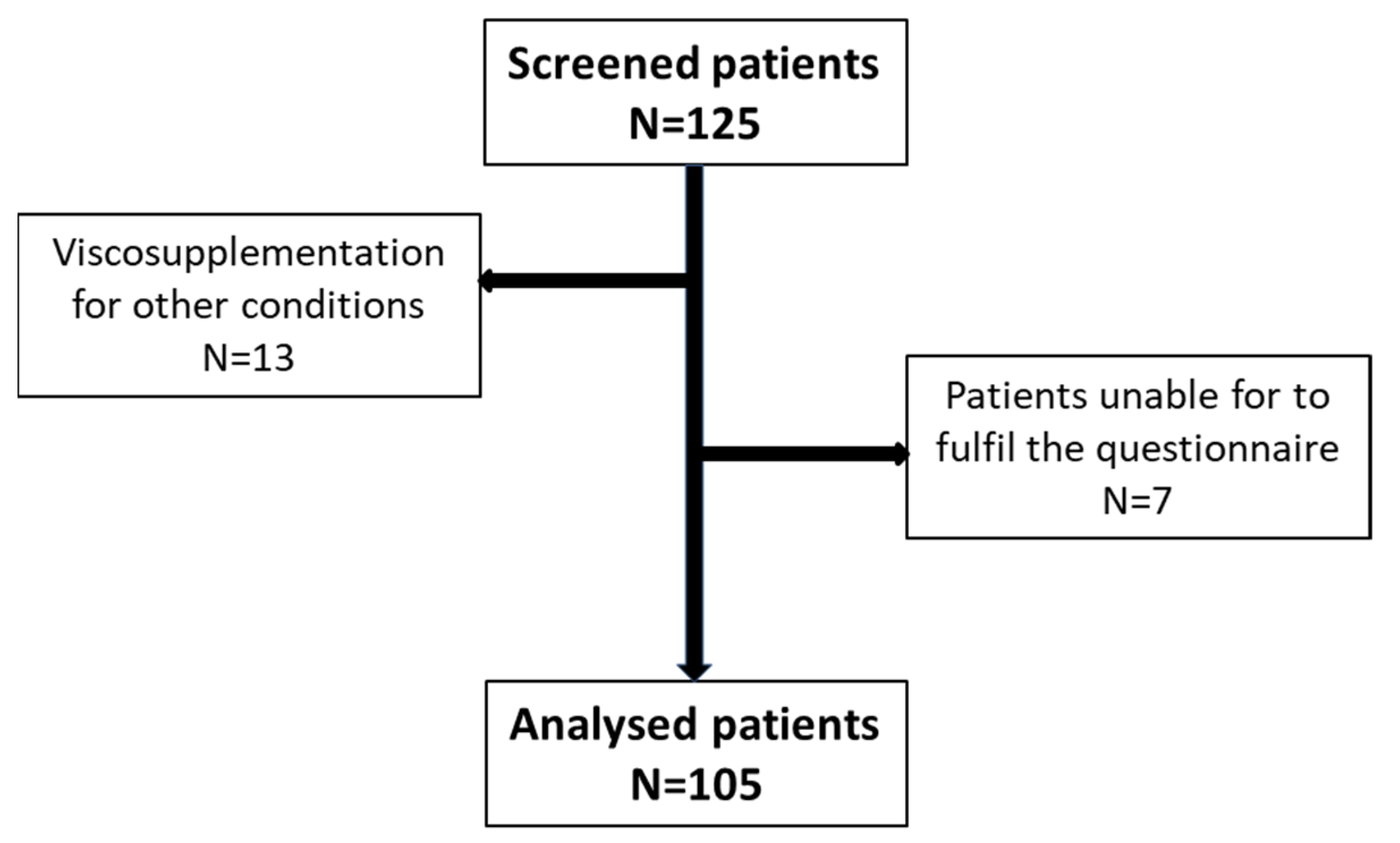
2.1. Patient Inclusion/Exclusion Criteria
2.2. Study Progression
- -
- Self-assessment of the duration of treatment efficacy (DE = number of weeks during which viscosupplementation was effective on symptoms);
- -
- The degree of satisfaction with the treatment on a numerical scale from 0 to 10;
- -
- Activity level: sedentary, active, or athletic;
- -
- Physical activity practised and intensity: light, moderate, or intense.
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Steinmetz, J.D.; Culbreth, G.T.; Haile, L.M.; Rafferty, Q.; Lo, J.; Fukutaki, K.G.; Cruz, J.A.; Smith, A.E.; Vollset, S.E.; Brooks, P.M.; et al. Global, regional, and national burden of osteoarthritis, 1990–2020 and projections to 2050: A systematic analysis for the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023, 5, e508–e522. [Google Scholar] [CrossRef] [PubMed]
- Cleveland, R.J.; Nelson, A.E.; Callahan, L.F. Knee and hip osteoarthritis as predictors of premature death: A review of the evidence. Clin. Exp. Rheumatol. 2019, 37 (Suppl. 120), 24–30. [Google Scholar] [PubMed]
- Sellam, J.; Courties, A.; Eymard, F.; Ferrero, S.; Latourte, A.; Ornetti, P.; Bannwarth, B.; Baumann, L.; Berenbaum, F.; Chevalier, X.; et al. Recommendations of the French Society of Rheumatology on pharmacological treatment of knee osteoarthritis. Jt. Bone Spine 2020, 87, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Bruyère, O.; Cooper, C.; Pelletier, J.-P.; Branco, J.; Brandi, M.L.; Guillemin, F.; Hochberg, M.C.; Kanis, J.A.; Kvien, T.K.; Martel-Pelletier, J.; et al. An algorithm recommendation for the management of knee osteoarthritis in Europe and internationally: A report from a task force of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Semin. Arthritis Rheum. 2014, 44, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Jordan, K.M.; Arden, N.K.; Doherty, M.; Bannwarth, B.; Bijlsma, J.W.; Dieppe, P.; Gunther, K.; Hauselmann, H.; Herrero-Beaumont, G.; Kaklamanis, P.; et al. EULAR recommendations 2003: An evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann. Rheum. Dis. 2003, 62, 1145–1155. [Google Scholar] [CrossRef] [PubMed]
- Bannuru, R.R.; Schmid, C.H.; Kent, D.M.; Vaysbrot, E.E.; Wong, J.B.; McAlindon, T.E. Comparative effectiveness of pharmacologic interventions for knee osteoarthritis: A systematic review and network meta-analysis. Ann. Intern. Med. 2015, 162, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Balazs, E.A.; Denlinger, J.L. Viscosupplementation: A new concept in the treatment of osteoarthritis. J. Rheumatol. 1993, 39, 3–9. [Google Scholar]
- Altman, R.D.; Manjoo, A.; Fierlinger, A.; Niazi, F.; Nicholls, M. The mechanism of action for hyaluronic acid treatment in the osteoarthritic knee: A systematic review. BMC Musculoskelet. Disord. 2015, 16, 321. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.E.; Bhattacharyya, S.; Parrish, W.R.; Fredericson, M.; Bisson, B.; Altman, R.D. Safety of Intra-Articular Hyaluronic Acid for Knee Osteoarthritis: Systematic Review and Meta-Analysis of Randomized Trials Involving More than 8000 Patients. Cartilage 2019, 13, 351S–363S. [Google Scholar] [CrossRef] [PubMed]
- Migliore, A.; Bizzi, E.; Herrero-Beaumont, J.; Petrella, R.J.; Raman, R.; Chevalier, X. The discrepancy between recommendations and clinical practice for viscosupplementation in osteoarthritis: Mind the gap! Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 1124–1129. [Google Scholar] [PubMed]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol. 2020, 72, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Eymard, F.; Chevalier, X.; Conrozier, T. Obesity and radiological severity are associated with viscosupplementation failure in patients with knee osteoarthritis. J. Orthop. Res. 2017, 35, 2269–2274. [Google Scholar] [CrossRef] [PubMed]
- Conrozier, T.; Eymard, F.; Chouk, M.; Chevalier, X. Impact of obesity, structural severity and their combination on the efficacy of viscosupplementation in patients with knee osteoarthritis. BMC Musculoskelet. Disord. 2019, 20, 376. [Google Scholar] [CrossRef] [PubMed]
- Felson, D.T.; Niu, J.; Guermazi, A.; Sack, B.; Aliabadi, P. Defining radiographic incidence and progression of knee osteoarthritis: Suggested modifications of the Kellgren and Lawrence scale. Ann. Rheum. Dis. 2011, 70, 1884–1886. [Google Scholar] [CrossRef] [PubMed]
- Buckwalter, J.A.; Lane, N.E. Athletics and osteoarthritis. Am. J. Sports Med. 1997, 25, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Shumnalieva, R.; Kotov, G.; Monov, S. Obesity-Related Knee Osteoarthritis—Current Concepts. Life 2023, 13, 1650. [Google Scholar] [CrossRef] [PubMed]
- Matta, J.; Carette, C.; Rives Lange, C.; Czernichow, S. Épidémiologie de l’obésité en France et dans le monde [French and worldwide epidemiology of obesity]. Presse Med. 2018, 47, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.T.; Lin, J.; Chang, C.J.; Lin, Y.T.; Hou, S.M. Therapeutic effects of hyaluronic acid on osteoarthritis of the knee: A meta-analysis of randomized controlled trials. J. Bone Jt. Surg. Am. 2004, 86, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Conrozier, T.; Mathieu, P.; Schott, A.M.; Laurent, I.; Hajri, T.; Crozes, P.; Grand, P.; Laurent, H.; Marchand, F.; Meignan, F.; et al. Factors predicting long-term efficacy of Hylan GF-20 viscosupplementation in knee osteoarthritis. Jt. Bone Spine 2003, 70, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.D.; Farrokhyar, F.; Fierlinger, A.; Niazi, F.; Rosen, J. Analysis for prognostic factors from a database for the intra-Articular hyaluronic acid (Euflexxa) treatment for osteoarthritis of the knee. Cartilage 2016, 7, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Perruchet, S.; Balblanc, J.C.; Rapp, C.; Bourgoin, C.; Guillochon, C.; Lohse, A.; Conrozier, T. The Association between Radiographic Features and the Duration of Effectiveness of a Single Injection of Extended-Release Hyaluronic Acid (HANOX-M-XL) in Patients with Knee Osteoarthritis: Preliminary Results of a Prospective Trial. Cartilage 2023, 14, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Bernetti, A.; Agostini, F.; Alviti, F.; Giordan, N.; Martella, F.; Santilli, V.; Paoloni, M.; Mangone, M. New Viscoelastic Hydrogel Hymovis MO.RE. Single Intra-articular Injection for the Treatment of Knee Osteoarthritis in Sportsmen: Safety and Efficacy Study Results. Front. Pharmacol. 2021, 12, 673988. [Google Scholar] [CrossRef]
- McElheny, K.; Toresdahl, B.; Ling, D.; Mages, K.; Asif, I. Comparative Effectiveness of Alternative Dosing Regimens of Hyaluronic Acid Injections for Knee Osteoarthritis: A Systematic Review. Sports Health 2019, 11, 461–466. [Google Scholar] [CrossRef]
- Huang, T.L.; Tsai, C.H. Safety and efficacy of single CHAP Hyaluronan injection versus three injections of linear Hyaluronan in pain relief for knee osteoarthritis: A prospective, 52-week follow-up, randomized, evaluator-blinded study. BMC Musculoskelet. Disord. 2021, 22, 572. [Google Scholar] [CrossRef] [PubMed]
- Suppan, V.K.L.; Tew, M.M.; Wong, B.C.; Chan, H.K.; Chew, Y.W.; Tan, C.S.; Kumar, V.K.N.; Shafie, A.A.; Rao, A.S. One-year follow-up of efficacy and cost of repeated doses versus single larger dose of intra-articular hyaluronic acid for knee osteoarthritis. J. Orthop. Surg. 2020, 28, 2309499019895029. [Google Scholar] [CrossRef]
- Skou, S.T.; Roos, E.M. Physical therapy for patients with knee and hip osteoarthritis: Supervised, active treatment is current best practice. Clin. Exp. Rheumatol. 2019, 37 (Suppl. 120), 112–117. [Google Scholar] [PubMed]
- Restuccia, R.; Ruggieri, D.; Magaudda, L.; Talotta, R. The preventive and therapeutic role of physical activity in knee osteoarthritis. Reumatismo 2022, 74. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, D.; Theysmans, T.; Mottola, R.; Verbrugghe, J. High-Intensity Training for Knee Osteoarthritis: A Narrative Review. Sports 2023, 11, 91. [Google Scholar] [CrossRef] [PubMed]
- HAS, Haute Autorité de Sant. Prise en Charge des Patients Adultes Atteints D’hypertendion Artérielle Essentielle. Available online: https://www.has-sante.fr/upload/docs/application/pdf/hta_patient_adulte_synthese.pdf (accessed on 20 February 2024).
- Tang, Y.; Hu, X.; Lu, X. Captopril, an angiotensin-converting enzyme inhibitor, possesses chondroprotective efficacy in a rat model of osteoarthritis through suppression local renin-angiotensin system. Int. J. Clin. Exp. Med. 2015, 8, 12584–12592. [Google Scholar] [PubMed]
- Wang, Y.; Kou, J.; Zhang, H.; Wang, C.; Li, H.; Ren, Y.; Zhang, Y. The renin-angiotensin system in the synovium promotes periarticular osteopenia in a rat model of collagen-induced arthritis. Int. Immunopharmacol. 2018, 65, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Silveira, K.D.; Coelho, F.M.; Vieira, A.T.; Barroso, L.C.; Queiroz-Junior, C.M.; Costa, V.V.; Sousa, L.F.C.; Oliveira, M.L.; Bader, M.; Silva, T.A.; et al. Mechanisms of the anti-inflammatory actions of the angiotensin type 1 receptor antagonist losartan in experimental models of arthritis. Peptides 2013, 46, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Agha, A.M.; Mansour, M. Effects of captopril on interleukin-6, leukotriene B4, and oxidative stress markers in serum and inflammatory exudate of arthritic rats: Evidence of antiinflammatory activity. Toxicol. Appl. Pharmacol. 2000, 168, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Valdes, A.M.; Abhishek, A.; Muir, K.; Zhang, W.; Maciewicz, R.A.; Doherty, M. Association of Beta-Blocker Use with Less Prevalent Joint Pain and Lower Opioid Requirement in People with Osteoarthritis. Arthritis Care Res. 2017, 69, 1076–1081. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Kwoh, C.K.; Ran, D.; Ashbeck, E.L.; Lo-Ciganic, W.H. Lack of evidence that beta blocker use reduces knee pain, areas of joint pain, or analgesic use among individuals with symptomatic knee osteoarthritis. Osteoarthr. Cartil. 2020, 28, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Uzieliene, I.; Bernotiene, E.; Rakauskiene, G.; Denkovskij, J.; Bagdonas, E.; Mackiewicz, Z.; Porvaneckas, N.; Kvederas, G.; Mobasheri, A. The Antihypertensive Drug Nifedipine Modulates the Metabolism of Chondrocytes and Human Bone Marrow-Derived Mesenchymal Stem Cells. Front. Endocrinol. 2019, 10, 756. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Long, H.; Zhao, J.; Zhong, G.; Li, J. Nifedipine inhibits oxidative stress and ameliorates osteoarthritis by activating the nuclear factor erythroid-2-related factor 2 pathway. Life Sci. 2020, 253, 117292. [Google Scholar] [CrossRef] [PubMed]
- Aleksiuk, V.; Baleisis, J.; Kirdaite, G.; Uzieliene, I.; Denkovskij, J.; Bernotas, P.; Ivaskiene, T.; Mobasheri, A.; Bernotiene, E. Evaluation of Cartilage Integrity Following Administration of Oral and Intraarticular Nifedipine in a Murine Model of Osteoarthritis. Biomedicines 2023, 11, 2443. [Google Scholar] [CrossRef] [PubMed]
- Daniilidis, K.; Georges, P.; Tibesku, C.O.; Prehm, P. Positive side effects of Ca antagonists for osteoarthritic joints—Results of an in vivo pilot study. J. Orthop. Surg. Res. 2015, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Jones, M.H.; Khair, M.M.; Miniaci, A. Patient-reported outcome measures for the knee. J. Knee Surg. 2010, 23, 137–151. [Google Scholar] [CrossRef]
- Conrozier, T.; Monet, M.; Lohse, A.; Raman, R. Getting Better or Getting Well? The Patient Acceptable Symptom State (PASS) Better Predicts Patient’s Satisfaction than the Decrease of Pain, in Knee Osteoarthritis Subjects Treated with Viscosupplementation. Cartilage 2018, 9, 370–377. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Age ± SD (range) (years) | 66.1 ± 13.2 (22–90) |
| % <65 years | 41% |
| % <50 years | 8% |
| % <40 years | <2% |
| Sex | |
| Female | 66 (62%) |
| Male | 39 (38%) |
| Body mass index (kg/m2) | |
| Median | 26.8 |
| Mean ± SD (range) | 27.5 ± 5.55 (18.3–43.7) |
| Professional status | |
| Working | 35 (33%) |
| Unemployed | 10 (10%) |
| Retired | 60 (57%) |
| Sport practice | |
| Yes n (%) | 46 (43.8%) |
| No n (%) | 59 (56.2%) |
| Patients taking drugs for knee OA (%) | 68% |
| Analgesics | 45% |
| Non-steroidal anti-inflammatory drugs | 13% |
| Glucosamine | 17% |
| Chondroitin | 9% |
| Duration of VS effectiveness (weeks) | |
| Mean ± SD | 48.2 ± 24.8 |
| Median (range) | 48 (0–156) |
| Disease duration n (%) | |
| >5 years | 85 (57%) |
| >1 and ≤5 years | 46 (31%) |
| ≤1 year and >6 months | 10 (6.7%) |
| ≤6 months | 7 (4.7%) |
| Missing data | 1 |
| Kellgren–Lawrence grade | |
| Median (range) | 3 (1–4) |
| Mean ± SD | 2.8 ± 1.1 |
| Grade 1–2 n (%) | 63 (43%) |
| Grade 3 n (%) | 41 (27%) |
| Grade 4 n (%) | 45 (30%) |
| Involved compartments | |
| Patellofemoral | 83 (57%) |
| Isolated patellofemoral | 29 (20%) |
| Tibiofemoral | 63 (43%) |
| Medial tibiofemoral | 47 (32%) |
| Unicompartmental | 89 (61%) |
| Multicompartmental | 57 (39%) |
| Missing data | 3 (2%) |
| Dosing regimen | |
| Cross-linked HA single injection | 133 (89%) |
| Linear HA repeated injections | 16 (11%) |
| Time since VS (weeks) | |
| Mean ± SD | 54.4 ± 24.4 |
| Median (range) | 52 (25–160) |
| Number of VS | |
| Mean ± SD | 3.54 ± 2.44 |
| Median (range) | 3 (1–14) |
| Synovial effusion at injection—n (%) | 101 (67.8%) |
| Volume of effusion (mL) | |
| Mean ± SD | 1.98 ± 4.47 |
| Median (range) | 1 (0–50) |
| Corticosteroid injection—n (%) | 10 (6.7%) |
| DE (Weeks) (Mean ± SD) (Range) | 95%CI | |
|---|---|---|
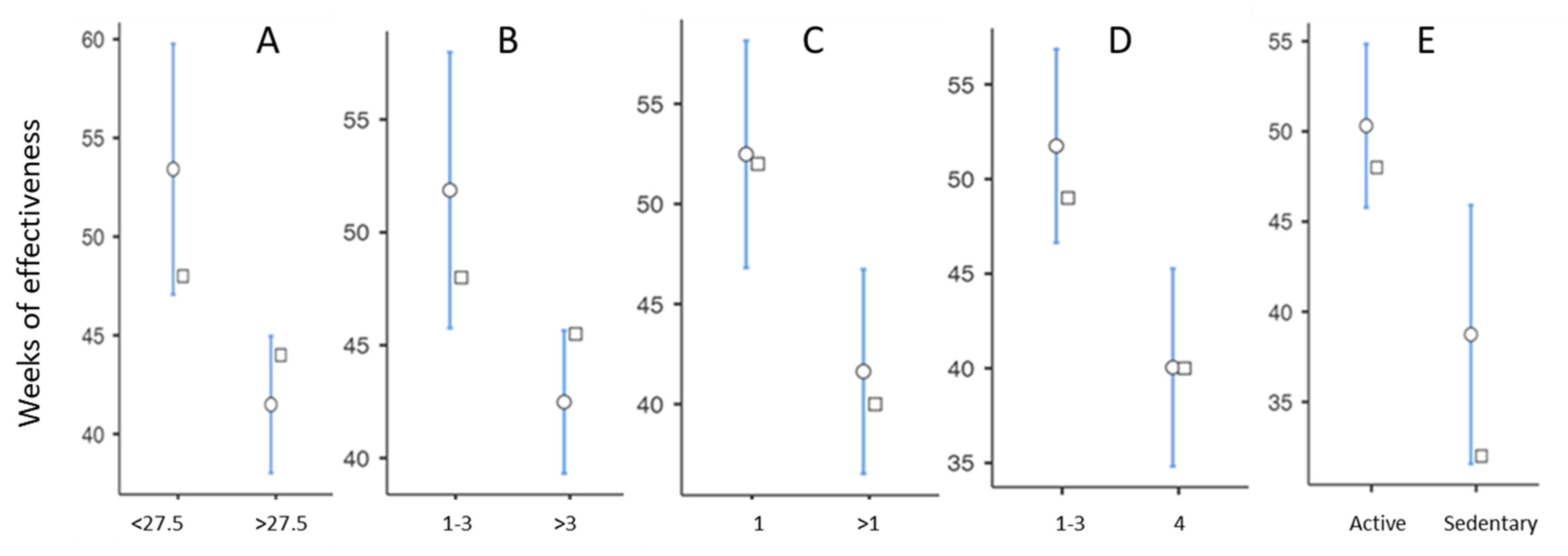
| BMI | ||
| <27.5 (n = 84) | 53.4 ± 29.7 (4–156) | 47.0–59.9 |
| >27.5 (n = 65) | 41.16 ± 14.36 (0–65) | 38.0–45.0 |
| Welch’s t-test: 3.23 p: 0.002 | ||
| Sex | ||
| Female (n = 92) | 45.5 ± 18.6 (16–124) | 41.7–49.4 |
| Male (n = 57) | 52.5 ± 32.2 (0–156) | 44.0–61.1 |
| Welch’s t-test: −1.50 p: 0.138 | ||
| Physical activity | ||
| Active (n = 122) | 50.3 ± 25.5 (0–156) | 45.7–54.9 |
| Sedentary(n = 27) | 38.7 ± 19.0 (16–80) | 31.2–46.3 |
| Mann–Whitney U test: 1083 p: 0.005 | ||
| Kellgren–Lawrence grade | ||
| Grade < 4 (n = 104) | 51.8 ±26.6 (0–156) | 46.6–56.9 |
| Grade 4 (n = 45) | 40.0 ± 17.9 (4–100) | 34.7–45.4 |
| Student’s t-test: 2.70 p: 0.008 | ||
| Number of viscosupplementations | ||
| 1–3 (n = 91) | 51.9 ± 29.7 (0–156) | 45.7–58.1 |
| >3 (n = 58) | 42.5 ± 12.3 (16–73) | 39.2–45.7 |
| Welch’s t-test: 2.67 p: 0.008 | ||
| Treatment for arterial hypertension | ||
| No | 45.4 ± 19.8 (0–124) | 41.3–49.4 |
| Yes | 53.1 ± 31.3 (16–156) | 44.6–61.5 |
| Student’s t-test: −1.84 p: 0.068 | ||
| Analgesic treatment | ||
| No (n = 82) | 50.8 ± 27.7 (4–156) | 44.7–56.9 |
| Yes (n = 67) | 45.0 ± 20.6 (0–108) | 40.0–50.1 |
| Student’s t-test: 1.41 p: 0.160 | ||
| Number of involved compartments | ||
| 1 (n = 89) | 52.5 ± 27.3 (0–156) | 46.7–58.2 |
| 2 or 3 (n = 57) | 41.6 ± 19.7 (4–109) | 36.4–46.8 |
| Student’s t-test: 2.60 p: 0.010 | ||
| Involved compartments | ||
| PF (n = 29) | 48.3 ± 22.7 (16–124) | 39.6–56.9 |
| LTF (n = 13) | 44.4 ± 13.6 (20–65) | 36.2–52.6 |
| MTF (n = 47) | 57.3± 31.8 (0–156) | 48.0–66.6 |
| MTF + PF(n = 36) | 43.4 ± 18.8 (18–109) | 37.0–49.7 |
| LTF + PF (n = 10) | 32.9 ± 12.8 (16–52) | 23.7–42.1 |
| MTF + LTF (n = 3) | 48.7 ± 7.0 (42–56) | 31.2–66.1 |
| LTF + LTF + PF (n = 8) | 42.1 ± 30.9 (4–108) | 16.3–67.9 |
| ANOVA: 2.59 p = 0.046 | ||
| Treatment with SYSADOA | ||
| No (n = 111) | 48.4 ± 28.1 (0–156) | 43.1–53.7 |
| Yes (n = 38) | 47.6 ± 10.6 (26–73) | 44.1–51.1 |
| Welch’s t-test: 0.257 p: 0.797 | ||
| Treatment with NSAIDs | ||
| No (n = 130) | 48.7 ± 25.9 (0–156) | 44.2–53.2 |
| Yes (n = 19) | 44.9 ± 15.3 (26–80) | 37.5–52.3 |
| Mann–Whitney U test: 1103 p: 0.453 | ||
| Comorbidities | ||
| Non (n = 46) | 44.6 ± 16.9 (4–124) | |
| Yes (n = 103) | 49.8 ± 27.6 (0–156) | |
| Student’s t-test: −1.18 p: 0.240 | ||
| SF effusion | ||
| Yes (n = 101) | 46.3 ± 22.5 (0–155) | 41.8–50.7 |
| No (n =48) | 52.3± 28.9 (4–156) | 43.9–60.7 |
| Student’s t-test: −1.39 p: 0.168 | ||
| Dosing regimen | ||
| Single injection (n = 133) | 48.9 ± 25.8 (0–156) | 44.5–53.3 |
| 3 injections (n = 16) | 42.3 ± 14.4 (15–65) | 34.6–50 |
| Student’s t-test: 1.01 p: 0.316 | ||
| Corticosteroid injection | ||
| No (n = 138) | 48.6 ± 23.4 (4–156) | 44.6–52.5 |
| Yes (n = 10) | 44.2 ± 42.4 (0–155) | 13.9–74.5 |
| Student’s t-test: 503 p: 0.153 | ||
| Sport practice | ||
| Yes (n = 66) | 47.4 ± 23.8 (0–156) | 41.6–53.3 |
| No (n = 83) | 48.8 ± 25.8 (16–155) | 43.2–54.5 |
| Student’s t-test: −0.339 p: 0.735 | ||
| No sport (n = 83) | 49.4 ± 26.1 (16–53.5) | 43.2–54.2 |
| Sports with low impact (n = 51) | 46.3 ± 20.9 (4–124) | 40.4–52.2 |
| Sports with high impact (n = 15) | 51.4 ± 32.3 (0–156) | 33.5–68.3 |
| ANOVA: 0.347 p: 0.706 | ||
| Sportive versus active patients | ||
| Athletic (n = 66) | 47.4 ± 23.8 (0–156) | 41.6–53.3 |
| Active but not athletic (n = 56) | 53.7 ± 27.3 (18–155) | 46.4–61.0 |
| Student’s t-test: −1.35 p: 0.179 | ||
| Knee stress | ||
| High (n = 24) | 48 ± 25.98 (0–156) | 37.2–59.1 |
| Normal/moderate (n = 103) | 50.31 ± 25.14 (4–155) | 45.4–55.2 |
| Low (n = 22) | 38.5 ± 20.425 (16–80) | 29.4–47.6 |
| Kruskal–Wallis test: 7.95 p: 0.019 |
| Predictors | Estimation | Standard Error | t | p |
|---|---|---|---|---|
| Intercept | 59.75 | 3.38 | 17.68 | <0.001 |
| BMI: | ||||
| >27.5 versus <27.5 | −14.92 | 4.15 | −3.60 | <0.001 |
| Number of involved compartments | −9.13 | 3.96 | −2.30 | 0.023 |
| ≥2 versus 1 | ||||
| K-L grade: | ||||
| Grade 4 versus grade < 4 | −5.49 | 4.46 | −1.23 | 0.220 |
| Number of VS: | ||||
| >3 versus 1 to 3 | −9.35 | 3.94 | −2.37 | 0.019 |
| Arterial hypertension: | ||||
| Yes versus No | 16.39 | 4.23 | 3.88 | <0.001 |
| Physical activity: | ||||
| Sedentary versus Active | −11.75 | 5.25 | −2.24 | 0.027 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rapp, C.; Boudif, F.; Bourgoin, C.; Lohse, A.; Conrozier, T. A Cross-Sectional Study of Factors Predicting the Duration of the Efficacy of Viscosupplementation in Knee Osteoarthritis. J. Clin. Med. 2024, 13, 1949. https://doi.org/10.3390/jcm13071949
Rapp C, Boudif F, Bourgoin C, Lohse A, Conrozier T. A Cross-Sectional Study of Factors Predicting the Duration of the Efficacy of Viscosupplementation in Knee Osteoarthritis. Journal of Clinical Medicine. 2024; 13(7):1949. https://doi.org/10.3390/jcm13071949
Chicago/Turabian StyleRapp, Charles, Feriel Boudif, Charlotte Bourgoin, Anne Lohse, and Thierry Conrozier. 2024. "A Cross-Sectional Study of Factors Predicting the Duration of the Efficacy of Viscosupplementation in Knee Osteoarthritis" Journal of Clinical Medicine 13, no. 7: 1949. https://doi.org/10.3390/jcm13071949