

Clinical Utility of Three-Dimensional Echocardiography in the Evaluation of Mitral Valve Disease: Tips and Tricks

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Know How
2.1. Data Acquisition
- (1)
- Live RT3DE mode: Characterized by an optimal temporal resolution despite the low spatial resolution. This modality is useful to test the gain optimization.
- (2)
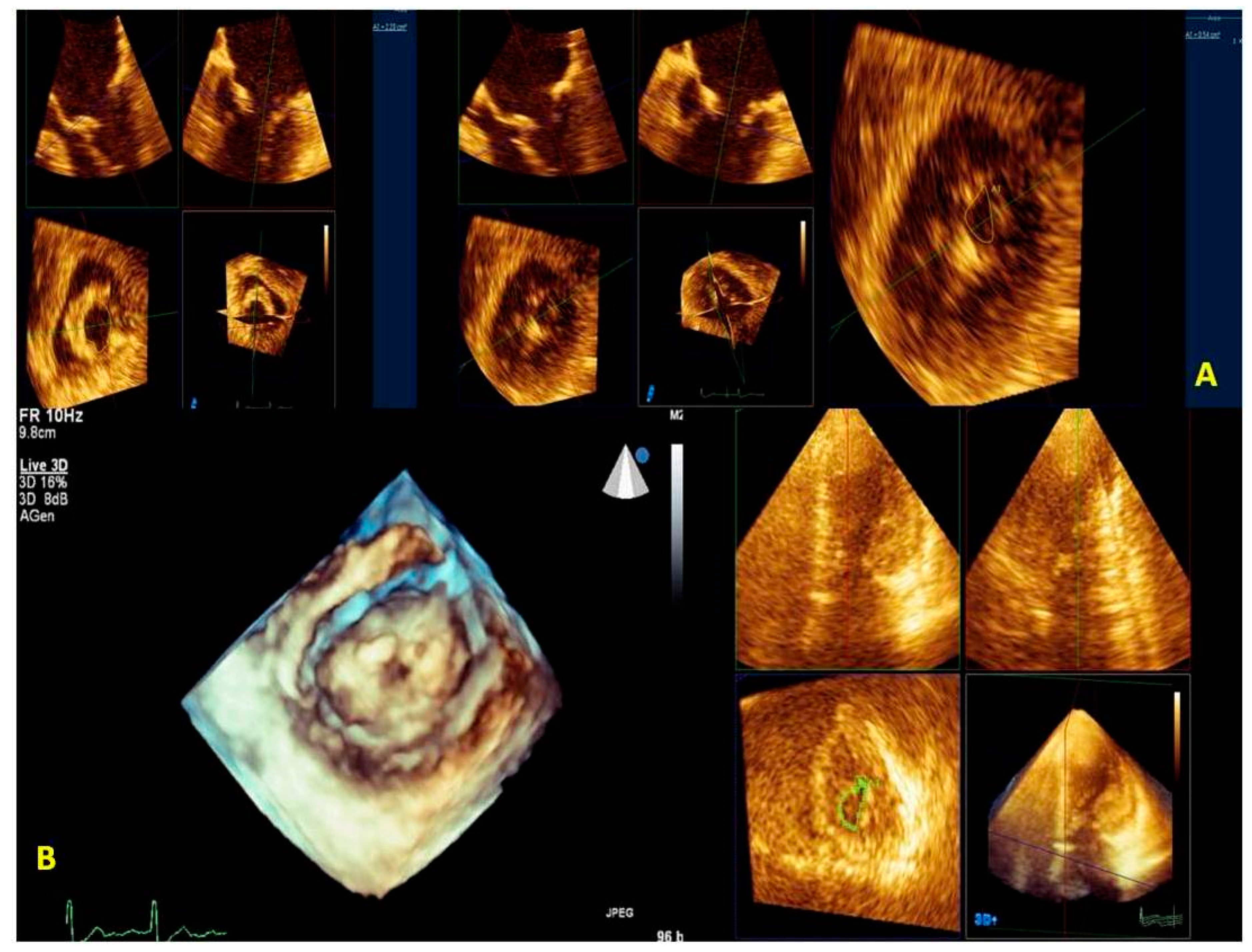
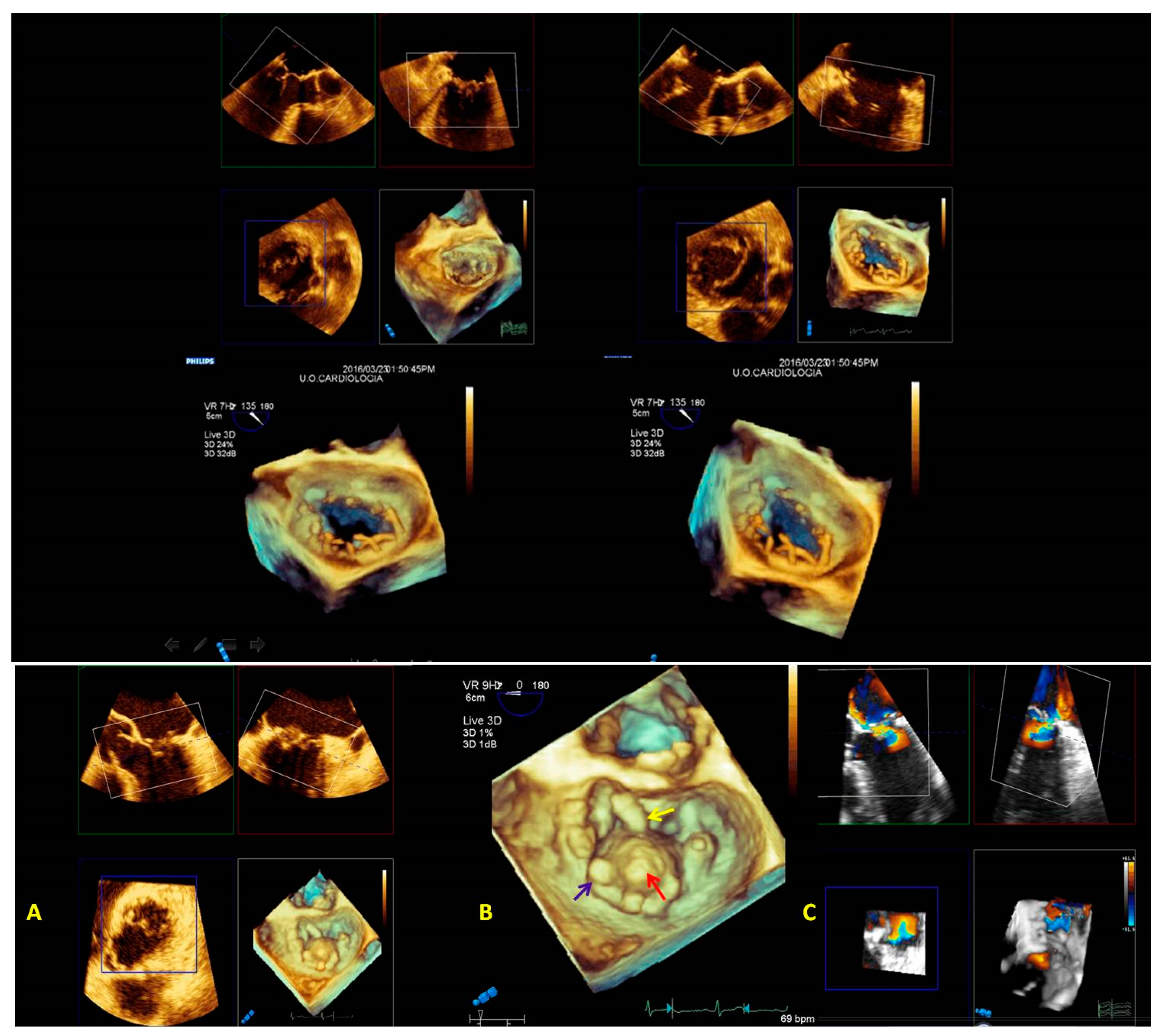
- Zoom mode: If zoom RT3DE is activated, two orthogonal 2D preview images show the ‘‘truncated’’ pyramid sector that the operator can move over the region of interest, regulating width and length and preventing respiratory or rhythm artifacts. However, it is limited by a low temporal resolution that can be improved by minimizing the sector’s width and length. (Figure 2B).
- (3)
- “Wide angle single beat”: This option has the same advantages of the zoom mode but a relatively lower temporal and spatial resolution.
- (4)
- “Full volume multiple beat” with or without color Doppler. This modality implies an electrocardiogram (ECG) synchronization permitting the analysis of an extensive volumetric data set by acquiring narrow subvolumes (two-seven sequential cardiac cycles). High spatial and temporal resolutions and a global MV view with excellent image quality represent the greatest strength of this modality (Figure 2C).
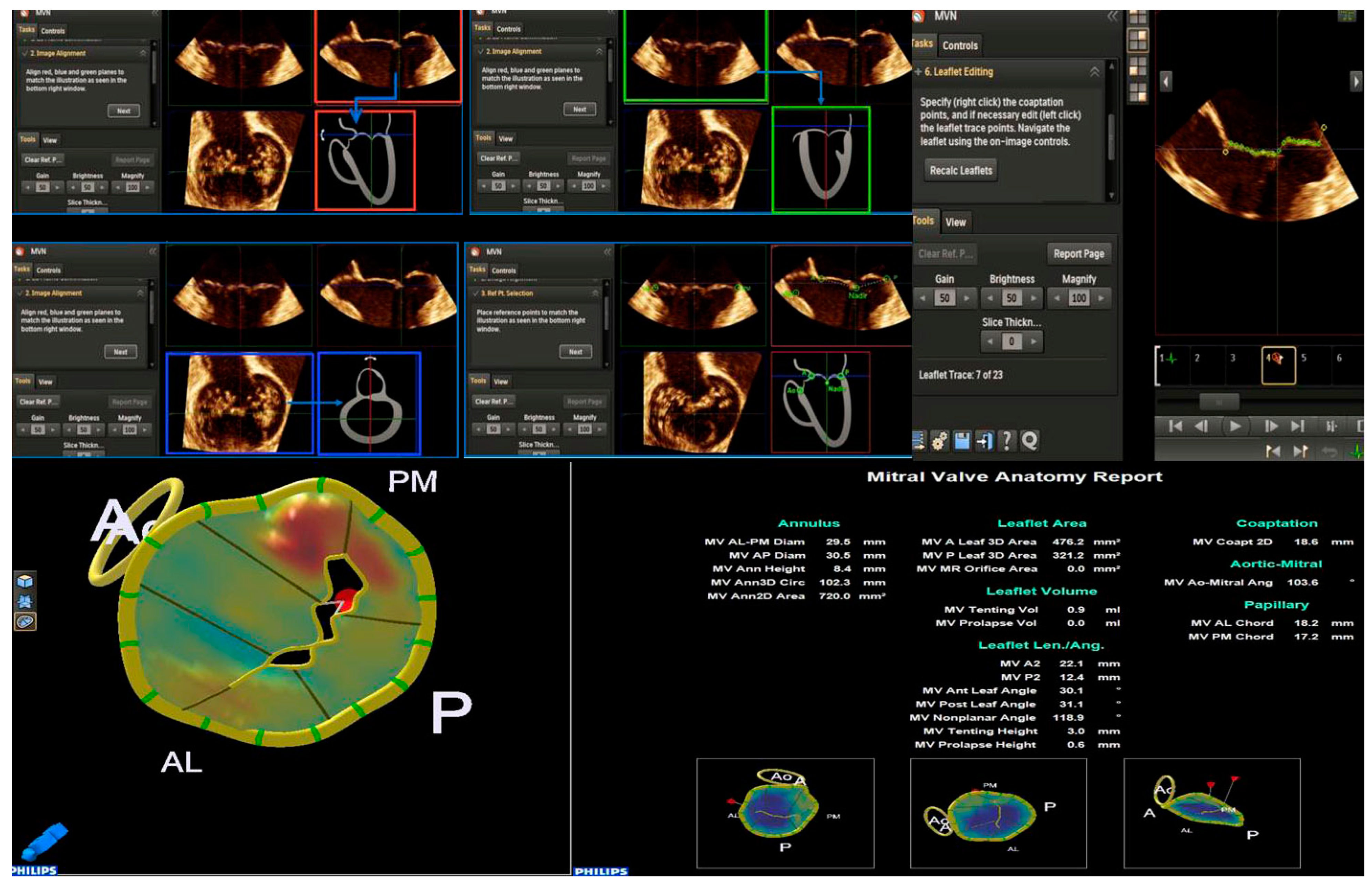
2.2. Mitral Valve Quantification (MVQ) and Mitral Valve Navigation (MVN)
2.3. Tips and Tricks for RT3DE Optimization
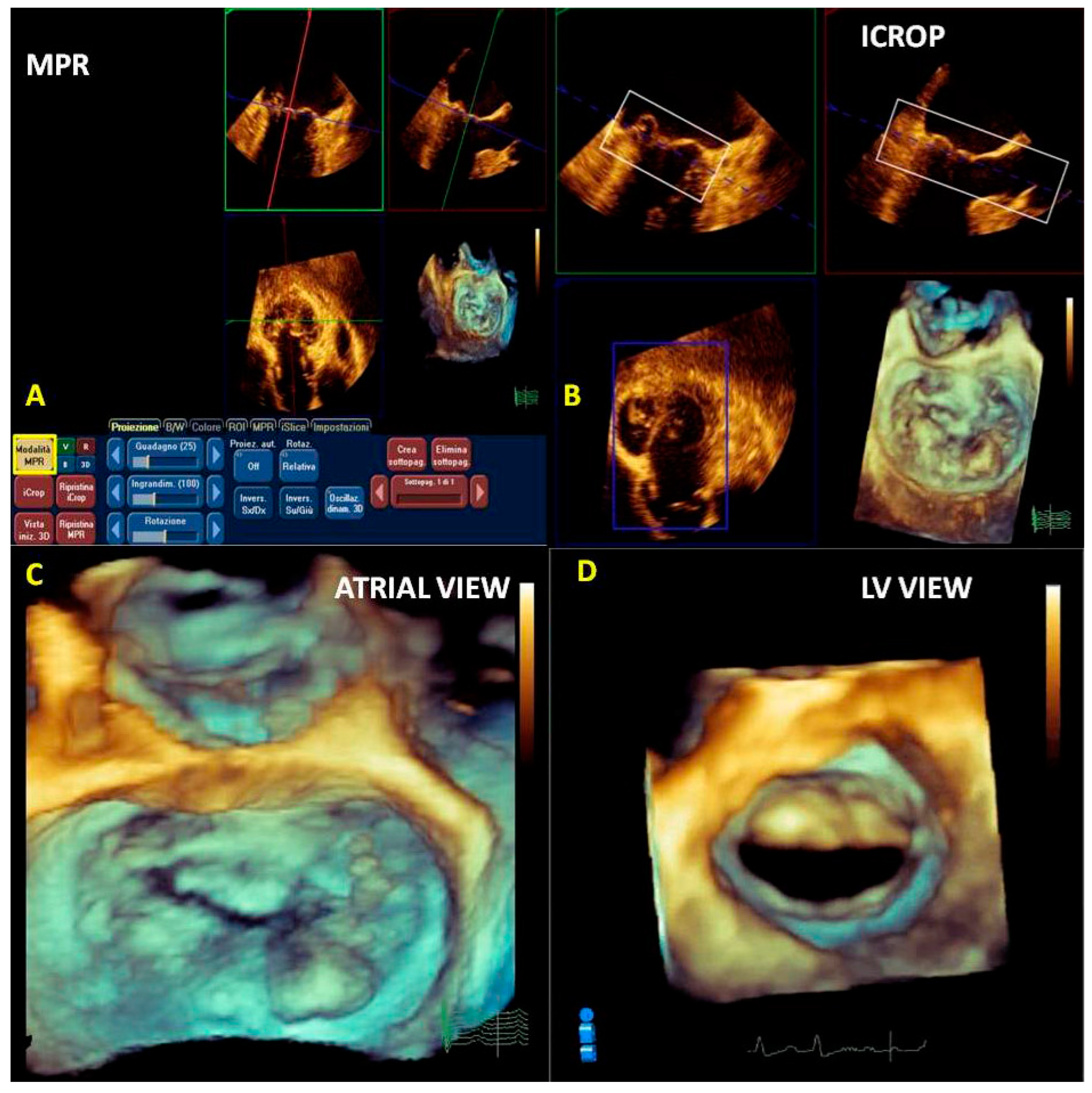
2.4. Post-Processing (Multiplanar Reconstruction and Cropping)
3. Know Why
3.1. Anatomical Characterization
3.2. Quantification of the Morphology
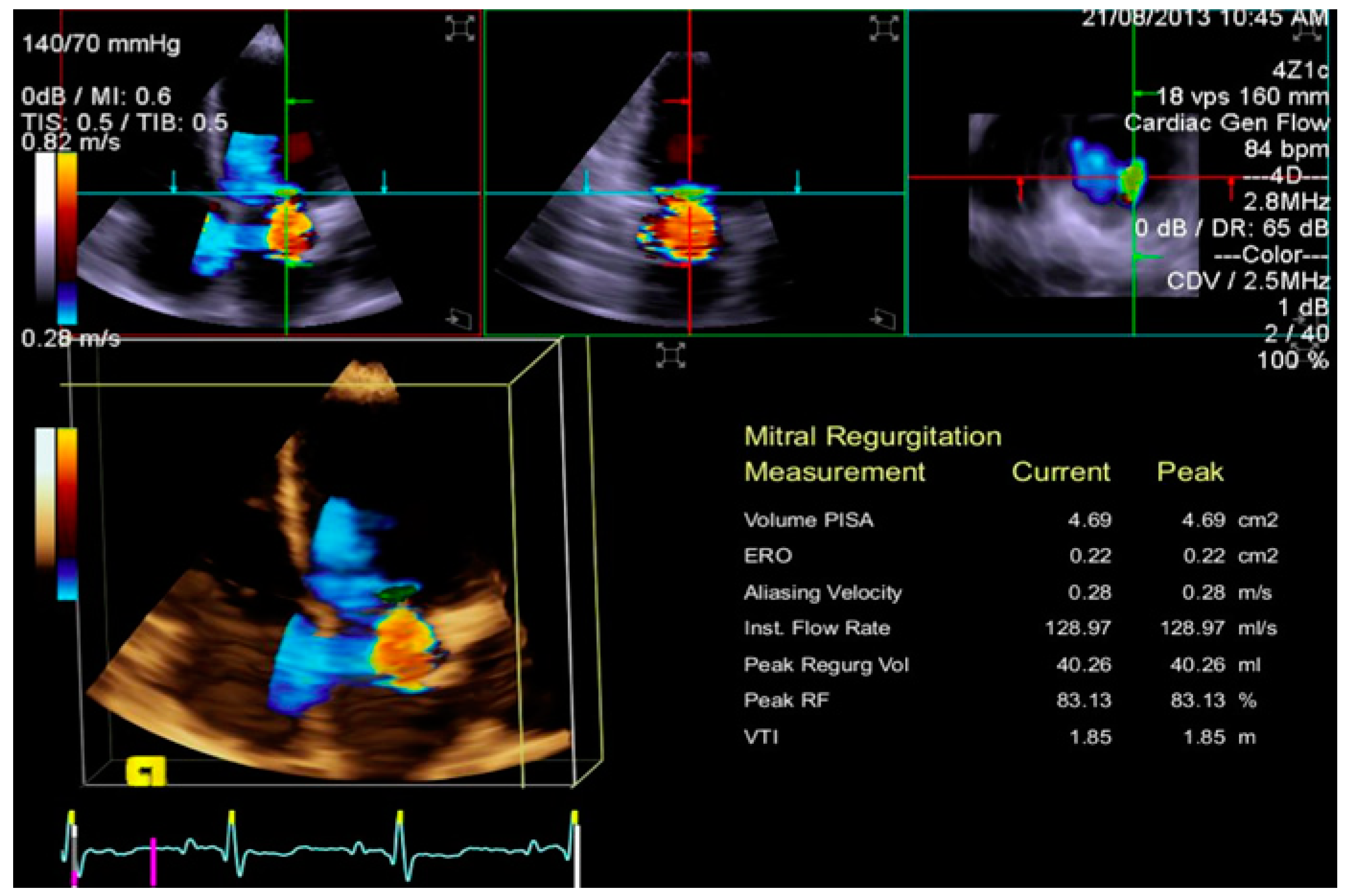
3.3. Quantification of Mitral Regurgitation
3.4. Quantification of MV Stenosis
4. Know When
4.1. Mitral Regurgitation
4.2. Mitral Valve Stenosis
4.3. Mitral Valve Repair Procedures
4.4. Surgical Repair
4.5. Percutaneous Repair
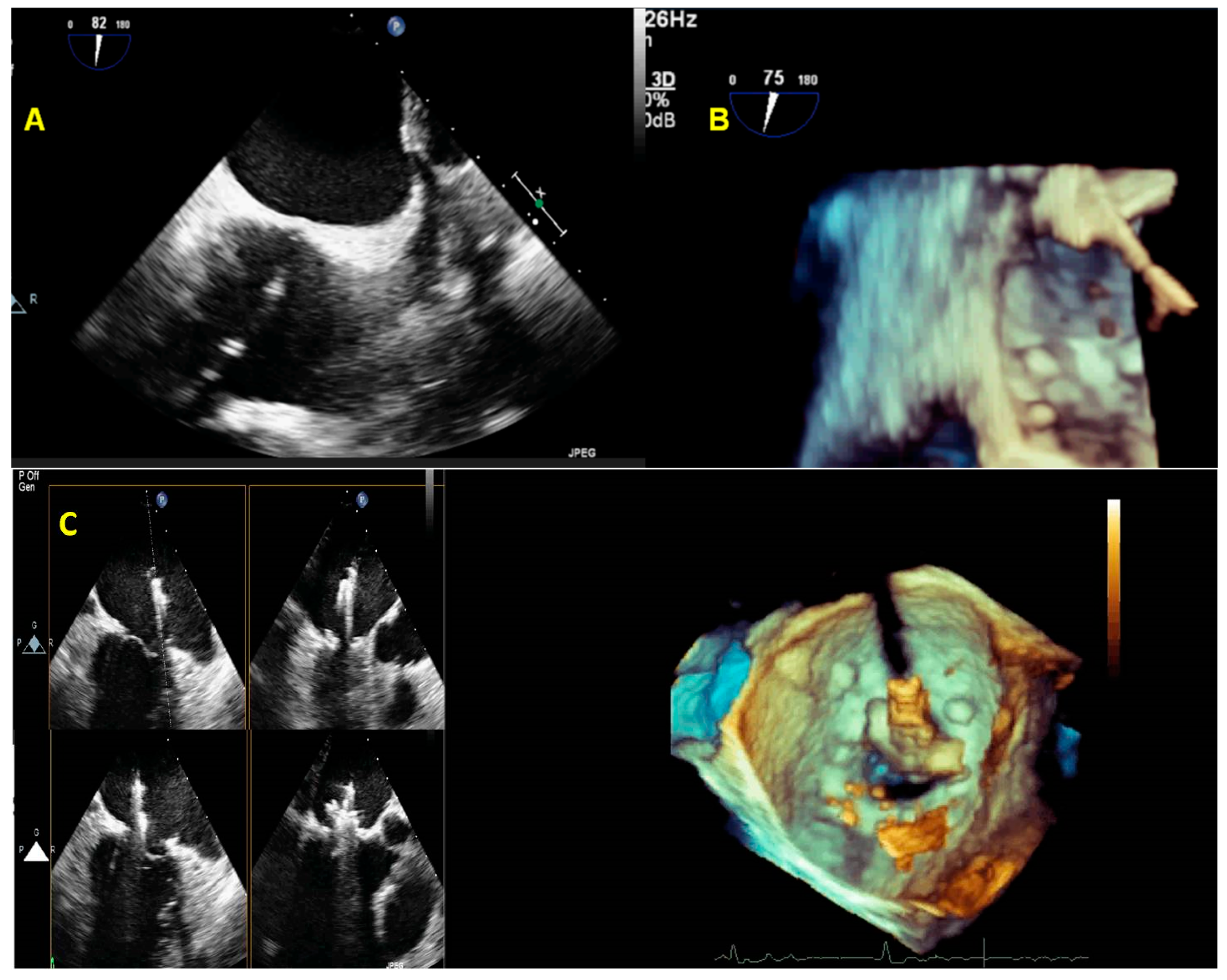
- The initial step is the guidance of the transseptal puncture. The ideal location for the puncture in most patients is the mid-fossa in the bicaval view, and the puncture site is directly visualized by the ‘tenting’ of the fossa ovalis. 3D-TEE with X-plane modality provides imaging of the entire interatrial septum (IAS). It allows the correct position and orientation of the Mullins Catheter, avoiding complications (catheter distance from aortic valve and atrial roof, Figure 20A,B).
- 2.
- The second step is the introduction of a steerable guide catheter (SGC) and advancement of the clip delivery system (CDS) into the L.A.; RT3DE with X-plane modality permits us to avoid LA free-wall injury (Figure 20C).
- 3.
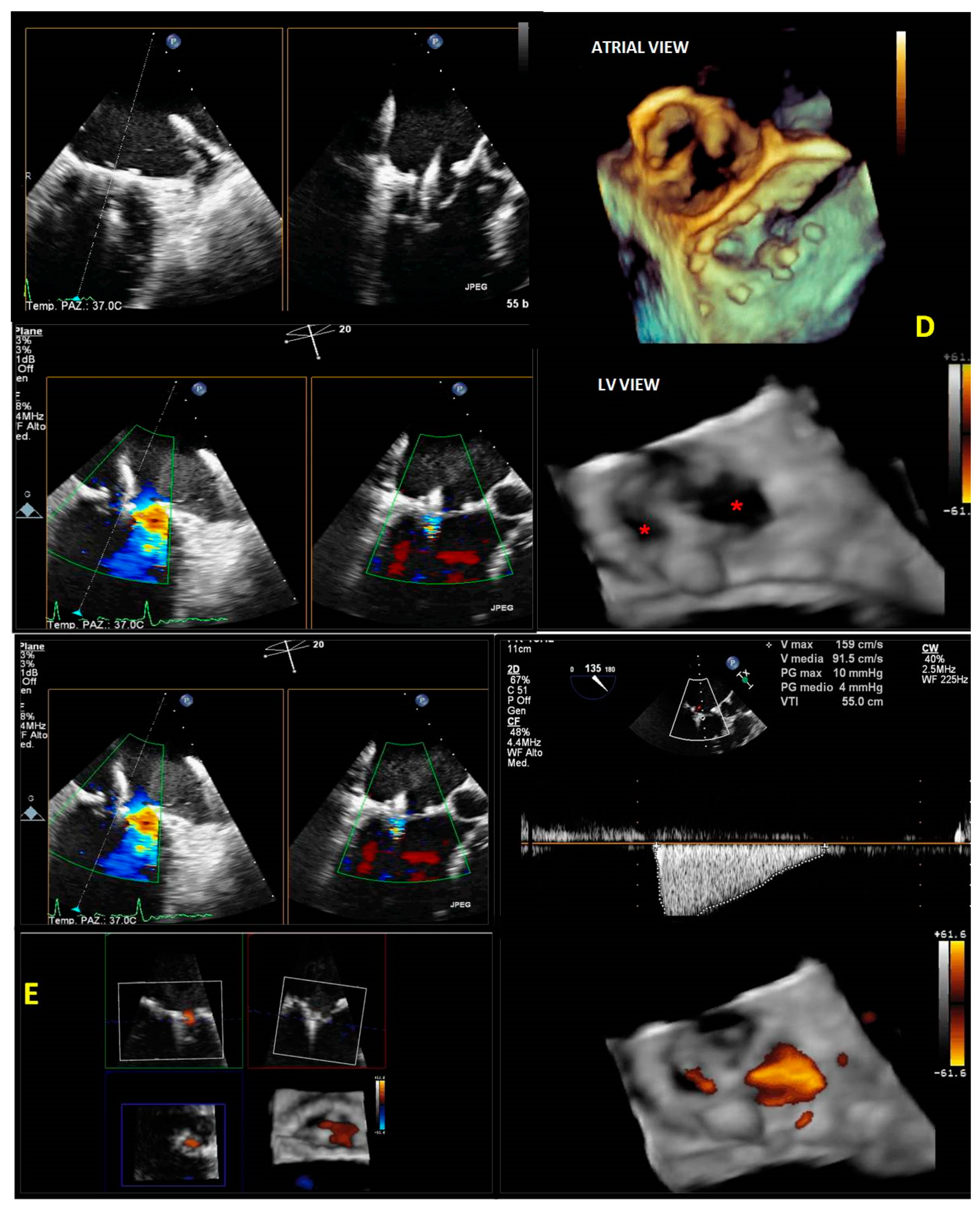
- The third step is positioning the Mitraclip above the MV. RT3DE with zoom modality en face view allows determination of when the clip is adequately positioned above the middle segments of the MV and if the orientation is perpendicular to the line of coaptation (Figure 20D).
- 4.
- The fourth step is the advancement of the Mitraclip in the LV. RT3DE with zoom modality in the L.A. or LV views represent direct visualization of the MitraClip concerning the MV and the line of coaptation, lowering the overall gain to get a clear impression of the clip in the LV views (Figure 20E).
- 5.
- The fifth step is grasping the leaflets and assessing proper leaflet insertion and clip detachment.
- 6.
- The sixth and final step is assessing the procedure results. RT3DE color may be used to evaluate the residual MV regurgitation, and 3D-TEE multiplanar reconstruction may be used to assess the post-implant mitral valve area. The clip can be repositioned or withdrawn in case of severe mitral stenosis. In case of residual significant MV regurgitation, another clip can be released.
5. Limitations and Future Perspectives
6. Conclusions
Funding
Conflicts of Interest
References
- Scali, M.C.; Basso, M.; Gandolfo, A.; Bombardini, T.; Bellotti, P.; Sicari, R. Real time 3D echocardiography (RT3DE) for assessment of ventricular and vascular function in hypertensive and heart failure patients. Cardiovasc. Ultrasound 2012, 10, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szulik, M.; Śliwińska, A.; Lenarczyk, R.; Szymała, M.; Kalinowski, M.E.; Markowicz-Pawlus, E.; Kalarus, Z.; Kukulski, T. 3D and 2D left ventricular systolic function imaging-- from ejection fraction to deformation. Cardiac resynchronization therapy--substudy. Acta Cardiol. 2015, 70, 21–30. [Google Scholar] [CrossRef]
- Aluru, J.S.; Barsouk, A.; Saginala, K.; Rawla, P.; Barsouk, A. Valvular Heart Disease Epidemiology. Med. Sci. 2022, 10, 32. [Google Scholar] [CrossRef]
- Robinson, S.; Ring, L.; Augustine, D.X.; Rekhraj, S.; Oxborough, D.; Harkness, A.; Lancellotti, P.; Rana, B. The assessment of mitral valve disease: A guideline from the British Society of Echocardiography. Echo. Res. Pract. 2021, 8, G87–G136. [Google Scholar] [CrossRef] [PubMed]
- Chew, P.G.; Bounford, K.; Plein, S.; Schlosshan, D.; Greenwood, J.P. Multimodality imaging for the quantitative assessment of mitral regurgitation. Quant. Imaging Med. Surg. 2018, 8, 342–359. [Google Scholar] [CrossRef] [Green Version]
- Grayburn, P.A.; Weissman, N.J.; Zamorano, J.L. Quantitation of mitral regurgitation. Circulation 2012, 126, 2005–2017. [Google Scholar] [CrossRef] [Green Version]
- Zamorano, J.-L.; de Isla, L.P. Real-time 3D Echocardiography in the Assessment of Mitral Valve Disease. E-J. Cardiol. Pract. 2005, 3. [Google Scholar]
- Muraru, D.; Hahn, R.T.; Soliman, O.I.; Faletra, F.F.; Basso, C.; Badano, L.P. 3-Dimensional echocardiography in imaging the tricuspid valve. JACC: Cardiovasc. Imaging 2019, 12, 500–515. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Tsang, W.; Adams, D.H.; Agricola, E.; Buck, T.; Faletra, F.F.; Franke, A.; Hung, J.; de Isla, L.P. EAE/ASE recommendations for image acquisition and display using three-dimensional echocardiography. Eur. Heart J. –Cardiovasc. Imaging 2012, 13, 1–46. [Google Scholar] [CrossRef]
- Salcedo, E.E.; Quaife, R.A.; Seres, T.; Carroll, J.D. A framework for systematic characterization of the mitral valve by real-time three-dimensional transesophageal echocardiography. J. Am. Soc. Echocardiogr. 2009, 22, 1087–1099. [Google Scholar] [CrossRef] [PubMed]
- Vegas, A. Three-dimensional transesophageal echocardiography: Principles and clinical applications. Ann. Card. Anaesth. 2016, 19, S35–S43. [Google Scholar] [CrossRef]
- Heo, R.; Son, J.W.; Ó Hartaigh, B.; Chang, H.J.; Kim, Y.J.; Datta, S.; Cho, I.J.; Shim, C.Y.; Hong, G.R.; Ha, J.W.; et al. Clinical Implications of Three-Dimensional Real-Time Color Doppler Transthoracic Echocardiography in Quantifying Mitral Regurgitation: A Comparison with Conventional Two-Dimensional Methods. J. Am. Soc. Echocardiogr. 2017, 30, 393–403.e397. [Google Scholar] [CrossRef]
- Avenatti, E.; Mackensen, G.B.; El-Tallawi, K.C.; Reisman, M.; Gruye, L.; Barker, C.M.; Little, S.H. Diagnostic Value of 3-Dimensional Vena Contracta Area for the Quantification of Residual Mitral Regurgitation After MitraClip Procedure. JACC Cardiovasc. Interv. 2019, 12, 582–591. [Google Scholar] [CrossRef]
- Geyer, M.; Sotiriou, E.; Tamm, A.R.; Ruf, T.F.; Kreidel, F.; Yang, Y.; Emrich, T.; Beiras-Fernandez, A.; Gori, T.; Münzel, T.; et al. Advanced Protocol for Three-Dimensional Transesophageal Echocardiography Guidance Implementing Real-Time Multiplanar Reconstruction for Transcatheter Mitral Valve Repair by Direct Annuloplasty. J. Am. Soc. Echocardiogr. 2019, 32, 1359–1365. [Google Scholar] [CrossRef] [PubMed]
- Buck, T.; Franke, A.; Monaghan, M.J. Three-Dimensional Echocardiography; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Hien, M.D.; Großgasteiger, M.; Rauch, H.; Weymann, A.; Bekeredjian, R.; Rosendal, C. Experts and beginners benefit from three-dimensional echocardiography: A multicenter study on the assessment of mitral valve prolapse. J. Am. Soc. Echocardiogr. 2013, 26, 828–834. [Google Scholar] [CrossRef] [PubMed]
- Lavall, D.; Hagendorff, A.; Schirmer, S.H.; Böhm, M.; Borger, M.A.; Laufs, U. Mitral valve interventions in heart failure. ESC Heart Fail. 2018, 5, 552–561. [Google Scholar] [CrossRef] [PubMed]
- Grayburn, P.A.; Carabello, B.; Hung, J.; Gillam, L.D.; Liang, D.; Mack, M.J.; McCarthy, P.M.; Miller, D.C.; Trento, A.; Siegel, R.J. Defining “severe” secondary mitral regurgitation: Emphasizing an integrated approach. J. Am. Coll. Cardiol. 2014, 64, 2792–2801. [Google Scholar] [CrossRef] [Green Version]
- Asgar, A.W.; Mack, M.J.; Stone, G.W. Secondary mitral regurgitation in heart failure: Pathophysiology, prognosis, and therapeutic considerations. J. Am. Coll. Cardiol. 2015, 65, 1231–1248. [Google Scholar] [CrossRef] [Green Version]
- Namazi, F.; van der Bijl, P.; Fortuni, F.; Mertens, B.J.A.; Kamperidis, V.; van Wijngaarden, S.E.; Stone, G.W.; Narula, J.; Ajmone Marsan, N.; Vahanian, A.; et al. Regurgitant Volume/Left Ventricular End-Diastolic Volume Ratio: Prognostic Value in Patients With Secondary Mitral Regurgitation. JACC Cardiovasc. Imaging. 2021, 14, 730–739. [Google Scholar] [CrossRef]
- Kamperidis, V.; Marsan, N.A.; Delgado, V.; Bax, J.J. Left ventricular systolic function assessment in secondary mitral regurgitation: Left ventricular ejection fraction vs. speckle tracking global longitudinal strain. Eur. Heart. J. 2016, 37, 811–816. [Google Scholar] [CrossRef]
- Stokke, T.M.; Hasselberg, N.E.; Smedsrud, M.K.; Sarvari, S.I.; Haugaa, K.H.; Smiseth, O.A.; Edvardsen, T.; Remme, E.W. Geometry as a Confounder When Assessing Ventricular Systolic Function: Comparison Between Ejection Fraction and Strain. J. Am. Coll. Cardiol. 2017, 70, 942–954. [Google Scholar] [CrossRef]
- Sapin, P.M.; Schroeder, K.D.; Smith, M.D.; DeMaria, A.N.; King, D.L. Three-dimensional echocardiographic measurement of left ventricular volume in vitro: Comparison with two-dimensional echocardiography and cineventriculography. J. Am. Coll. Cardiol. 1993, 22, 1530–1537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobs, L.D.; Salgo, I.S.; Goonewardena, S.; Weinert, L.; Coon, P.; Bardo, D.; Gerard, O.; Allain, P.; Zamorano, J.L.; de Isla, L.P.; et al. Rapid online quantification of left ventricular volume from real-time three-dimensional echocardiographic data. Eur. Heart. J. 2006, 27, 460–468. [Google Scholar] [CrossRef] [Green Version]
- Caiani, E.G.; Corsi, C.; Sugeng, L.; MacEneaney, P.; Weinert, L.; Mor-Avi, V.; Lang, R.M. Improved quantification of left ventricular mass based on endocardial and epicardial surface detection with real time three dimensional echocardiography. Heart 2006, 92, 213–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugeng, L.; Coon, P.; Weinert, L.; Jolly, N.; Lammertin, G.; Bednarz, J.E.; Thiele, K.; Lang, R.M. Use of real-time 3-dimensional transthoracic echocardiography in the evaluation of mitral valve disease. J. Am. Soc. Echocardiogr. 2006, 19, 413–421. [Google Scholar] [CrossRef]
- Pepi, M.; Tamborini, G.; Maltagliati, A.; Galli, C.A.; Sisillo, E.; Salvi, L.; Naliato, M.; Porqueddu, M.; Parolari, A.; Zanobini, M.; et al. Head-to-head comparison of two- and three-dimensional transthoracic and transesophageal echocardiography in the localization of mitral valve prolapse. J. Am. Coll. Cardiol. 2006, 48, 2524–2530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grewal, J.; Mankad, S.; Freeman, W.K.; Click, R.L.; Suri, R.M.; Abel, M.D.; Oh, J.K.; Pellikka, P.A.; Nesbitt, G.C.; Syed, I. Real-time three-dimensional transesophageal echocardiography in the intraoperative assessment of mitral valve disease. J. Am. Soc. Echocardiogr. 2009, 22, 34–41. [Google Scholar] [CrossRef]
- Zekry, S.B.; Nagueh, S.F.; Little, S.H.; Quinones, M.A.; McCulloch, M.L.; Karanbir, S.; Herrera, E.L.; Lawrie, G.M.; Zoghbi, W.A. Comparative accuracy of two-and three-dimensional transthoracic and transesophageal echocardiography in identifying mitral valve pathology in patients undergoing mitral valve repair: Initial observations. J. Am. Soc. Echocardiogr. 2011, 24, 1079–1085. [Google Scholar] [CrossRef]
- Levine, R.A.; Handschumacher, M.D.; Sanfilippo, A.; Hagege, A.; Harrigan, P.; Marshall, J.; Weyman, A. Three-dimensional echocardiographic reconstruction of the mitral valve, with implications for the diagnosis of mitral valve prolapse. Circulation 1989, 80, 589–598. [Google Scholar] [CrossRef] [Green Version]
- Jain, S.; Malouf, J.F. Incremental value of 3-D transesophageal echocardiographic imaging of the mitral valve. Curr. Cardiol. Rep. 2014, 16, 1–9. [Google Scholar] [CrossRef]
- Biaggi, P.; Gruner, C.; Jedrzkiewicz, S.; Karski, J.; Meineri, M.; Vegas, A.; David, T.E.; Woo, A.; Rakowski, H. Assessment of mitral valve prolapse by 3D TEE: Angled views are key. JACC Cardiovasc. Imaging 2011, 4, 94–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biaggi, P.; Jedrzkiewicz, S.; Gruner, C.; Meineri, M.; Karski, J.; Vegas, A.; Tanner, F.C.; Rakowski, H.; Ivanov, J.; David, T.E. Quantification of mitral valve anatomy by three-dimensional transesophageal echocardiography in mitral valve prolapse predicts surgical anatomy and the complexity of mitral valve repair. J. Am. Soc. Echocardiogr. 2012, 25, 758–765. [Google Scholar] [CrossRef]
- Faletra, F.F.; Leo, L.A.; Paiocchi, V.L.; Caretta, A.; Viani, G.M.; Schlossbauer, S.A.; Demertzis, S.; Ho, S.Y. Anatomy of mitral annulus insights from non-invasive imaging techniques. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 843–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faletra, F.F.; Demertzis, S.; Pedrazzini, G.; Murzilli, R.; Pasotti, E.; Muzzarelli, S.; Siclari, F.; Moccetti, T. Three-dimensional transesophageal echocardiography in degenerative mitral regurgitation. J. Am. Soc. Echocardiogr. 2015, 28, 437–448. [Google Scholar] [CrossRef] [PubMed]
- La Canna, G.; Scarfò, I.; Pibarot, P. Artificial Valves. In 3D Echocardiography; CRC Press: Boca Raton, FL, USA, 2020; pp. 158–175. [Google Scholar]
- Zamorano, J.L.; Badano, L.P.; Bruce, C.; Chan, K.L.; Gonçalves, A.; Hahn, R.T.; Keane, M.G.; La Canna, G.; Monaghan, M.J.; Nihoyannopoulos, P.; et al. EAE/ASE recommendations for the use of echocardiography in new transcatheter interventions for valvular heart disease. J. Am. Soc. Echocardiogr. 2011, 24, 937–965. [Google Scholar] [CrossRef]
- La Canna, G.; Arendar, I.; Maisano, F.; Monaco, F.; Collu, E.; Benussi, S.; De Bonis, M.; Castiglioni, A.; Alfieri, O. Real-time three-dimensional transesophageal echocardiography for assessment of mitral valve functional anatomy in patients with prolapse-related regurgitation. Am. J. Cardiol. 2011, 107, 1365–1374. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar] [CrossRef]
- Chandra, S.; Salgo, I.S.; Sugeng, L.; Weinert, L.; Tsang, W.; Takeuchi, M.; Spencer, K.T.; O’Connor, A.; Cardinale, M.; Settlemier, S. Characterization of degenerative mitral valve disease using morphologic analysis of real-time three-dimensional echocardiographic images: Objective insight into complexity and planning of mitral valve repair. Circ. Cardiovasc. Imaging 2011, 4, 24–32. [Google Scholar] [CrossRef] [Green Version]
- Apor, A.; Nagy, A.I.; Kovács, A.; Manouras, A.; Andrássy, P.; Merkely, B. Three-dimensional dynamic morphology of the mitral valve in different forms of mitral valve prolapse–potential implications for annuloplasty ring selection. Cardiovasc. Ultrasound 2015, 14, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. Corrigendum to: 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2022, 43, 2022. [Google Scholar] [CrossRef]
- Lancellotti, P.; Tribouilloy, C.; Hagendorff, A.; Popescu, B.A.; Edvardsen, T.; Pierard, L.A.; Badano, L.; Zamorano, J.L. Recommendations for the echocardiographic assessment of native valvular regurgitation: An executive summary from the European Association of Cardiovascular Imaging. Eur. Heart J. –Cardiovasc. Imaging 2013, 14, 611–644. [Google Scholar] [CrossRef] [Green Version]
- Bonow, R.O.; O’Gara, P.T.; Adams, D.H.; Badhwar, V.; Bavaria, J.E.; Elmariah, S.; Hung, J.W.; Lindenfeld, J.; Morris, A.A.; Satpathy, R.; et al. 2020 Focused Update of the 2017 ACC Expert Consensus Decision Pathway on the Management of Mitral Regurgitation: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2020, 75, 2236–2270. [Google Scholar] [CrossRef] [PubMed]
- O’Gara, P.T.; Grayburn, P.A.; Badhwar, V.; Afonso, L.C.; Carroll, J.D.; Elmariah, S.; Kithcart, A.P.; Nishimura, R.A.; Ryan, T.J.; Schwartz, A. 2017 ACC Expert Consensus Decision Pathway on the Management of Mitral Regurgitation: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J. Am. Coll. Cardiol. 2017, 70, 2421–2449. [Google Scholar] [PubMed]
- Thavendiranathan, P.; Phelan, D.; Collier, P.; Thomas, J.D.; Flamm, S.D.; Marwick, T.H. Quantitative assessment of mitral regurgitation: How best to do it. JACC Cardiovasc. Imaging 2012, 5, 1161–1175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abudiab, M.M.; Chao, C.J.; Liu, S.; Naqvi, T.Z. Quantitation of valve regurgitation severity by three-dimensional vena contracta area is superior to flow convergence method of quantitation on transesophageal echocardiography. Echocardiography 2017, 34, 992–1001. [Google Scholar] [CrossRef] [Green Version]
- Militaru, S.; Bonnefous, O.; Hami, K.; Langet, H.; Houard, L.; Allaire, S.; Pouleur, A.C.; Dianis, S.; This, A.; Beauloye, C.; et al. Validation of Semiautomated Quantification of Mitral Valve Regurgitation by Three-Dimensional Color Doppler Transesophageal Echocardiography. J. Am. Soc. Echocardiogr. 2020, 33, 342–354. [Google Scholar] [CrossRef]
- Choi, J.; Heo, R.; Hong, G.-R.; Chang, H.-J.; Sung, J.M.; Shin, S.H.; Cho, I.J.; Shim, C.-Y.; Chung, N. Differential effect of 3-dimensional color Doppler echocardiography for the quantification of mitral regurgitation according to the severity and characteristics. Circ. Cardiovasc. Imaging 2014, 7, 535–544. [Google Scholar] [CrossRef] [Green Version]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef]
- Little, S.H.; Pirat, B.; Kumar, R.; Igo, S.R.; McCulloch, M.; Hartley, C.J.; Xu, J.; Zoghbi, W.A. Three-dimensional color Doppler echocardiography for direct measurement of vena contracta area in mitral regurgitation: In vitro validation and clinical experience. JACC Cardiovasc. Imaging 2008, 1, 695–704. [Google Scholar] [CrossRef] [Green Version]
- Yosefy, C.; Hung, J.; Chua, S.; Vaturi, M.; Ton-Nu, T.-T.; Handschumacher, M.D.; Levine, R.A. Direct measurement of vena contracta area by real-time 3-dimensional echocardiography for assessing severity of mitral regurgitation. Am. J. Cardiol. 2009, 104, 978–983. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.-L.; Liu, X.; Ascah, K.J.; Beauchesne, L.M.; Burwash, I.G. Comparison of real-time 3-dimensional echocardiography with conventional 2-dimensional echocardiography in the assessment of structural heart disease. J. Am. Soc. Echocardiogr. 2004, 17, 976–980. [Google Scholar] [CrossRef] [PubMed]
- Iung, B.; Baron, G.; Butchart, E.G.; Delahaye, F.; Gohlke-Bärwolf, C.; Levang, O.W.; Tornos, P.; Vanoverschelde, J.-L.; Vermeer, F.; Boersma, E. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur. Heart J. 2003, 24, 1231–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akram, M.R.; Chan, T.; McAuliffe, S.; Chenzbraun, A. Non-rheumatic annular mitral stenosis: Prevalence and characteristics. Eur. J. Echocardiogr. 2009, 10, 103–105. [Google Scholar] [CrossRef]
- Nakatani, S.; Masuyama, T.; Kodama, K.; Kitabatake, A.; Fujii, K.; Kamada, T. Value and limitations of Doppler echocardiography in the quantification of stenotic mitral valve area: Comparison of the pressure half-time and the continuity equation methods. Circulation 1988, 77, 78–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rifkin, R.D.; Harper, K.; Tighe, D. Comparison of proximal isovelocity surface area method with pressure half-time and planimetry in evaluation of mitral stenosis. J. Am. Coll. Cardiol. 1995, 26, 458–465. [Google Scholar] [CrossRef] [Green Version]
- Wunderlich, N.C.; Beigel, R.; Siegel, R.J. Management of mitral stenosis using 2D and 3D echo-Doppler imaging. JACC Cardiovasc. Imaging 2013, 6, 1191–1205. [Google Scholar] [CrossRef] [Green Version]
- Sugeng, L.; Weinert, L.; Lammertin, G.; Thomas, P.; Spencer, K.T.; DeCara, J.M.; Mor-Avi, V.; Huo, D.; Feldman, T.; Lang, R.M. Accuracy of mitral valve area measurements using transthoracic rapid freehand 3-dimensional scanning: Comparison with noninvasive and invasive methods. J. Am. Soc. Echocardiogr. 2003, 16, 1292–1300. [Google Scholar] [CrossRef]
- Karamnov, S.; Burbano-Vera, N.; Huang, C.C.; Fox, J.A.; Shernan, S.K. Echocardiographic Assessment of Mitral Stenosis Orifice Area: A Comparison of a Novel Three-Dimensional Method Versus Conventional Techniques. Anesth. Analg. 2017, 125, 774–780. [Google Scholar] [CrossRef]
- Argulian, E.; Seetharam, K. Echocardiographic 3D-guided 2D planimetry in quantifying left-sided valvular heart disease. Echocardiography 2018, 35, 695–706. [Google Scholar] [CrossRef]
- Sampaio, F.; Ladeiras-Lopes, R.; Almeida, J.; Fonseca, P.; Fontes-Carvalho, R.; Ribeiro, J.; Gama, V. Three-dimensional proximal flow convergence automatic calculation for determining mitral valve area in rheumatic mitral stenosis. Echocardiography 2017, 34, 1002–1009. [Google Scholar] [CrossRef]
- Wilkins, G.T.; Weyman, A.E.; Abascal, V.M.; Block, P.C.; Palacios, I.F. Percutaneous balloon dilatation of the mitral valve: An analysis of echocardiographic variables related to outcome and the mechanism of dilatation. Br. Heart. J. 1988, 60, 299–308. [Google Scholar] [CrossRef] [Green Version]
- Binder, T.M.; Rosenhek, R.; Porenta, G.; Maurer, G.; Baumgartner, H. Improved assessment of mitral valve stenosis by volumetric real-time three-dimensional echocardiography. J. Am. Coll. Cardiol. 2000, 36, 1355–1361. [Google Scholar] [CrossRef]
- Mannaerts, H.F.; Kamp, O.; Visser, C.A. Should mitral valve area assessment in patients with mitral stenosis be based on anatomical or on functional evaluation? A plea for 3D echocardiography as the new clinical standard. Eur. Heart. J. 2004, 25, 2073–2074. [Google Scholar] [CrossRef] [PubMed]
- Anwar, A.M.; Attia, W.M.; Nosir, Y.F.; Soliman, O.I.; Mosad, M.A.; Othman, M.; Geleijnse, M.L.; El-Amin, A.M.; Ten Cate, F.J. Validation of a new score for the assessment of mitral stenosis using real-time three-dimensional echocardiography. J Am Soc Echocardiogr 2010, 23, 13–22. [Google Scholar] [CrossRef]
- Nunes, M.C.P.; Levine, R.A.; Braulio, R.; Pascoal-Xavier, M.A.; Elmariah, S.; Gomes, N.F.A.; Soares, J.R.; Esteves, W.A.M.; Zeng, X.; Dal-Bianco, J.P.; et al. Mitral Regurgitation After Percutaneous Mitral Valvuloplasty: Insights Into Mechanisms and Impact on Clinical Outcomes. JACC Cardiovasc. Imaging 2020, 13, 2513–2526. [Google Scholar] [CrossRef] [PubMed]
- Calleja, A.; Poulin, F.; Woo, A.; Meineri, M.; Jedrzkiewicz, S.; Vannan, M.A.; Rakowski, H.; David, T.; Tsang, W.; Thavendiranathan, P. Quantitative Modeling of the Mitral Valve by Three-Dimensional Transesophageal Echocardiography in Patients Undergoing Mitral Valve Repair: Correlation with Intraoperative Surgical Technique. J. Am. Soc. Echocardiogr. 2015, 28, 1083–1092. [Google Scholar] [CrossRef]
- Feldman, T.; Wasserman, H.S.; Herrmann, H.C.; Gray, W.; Block, P.C.; Whitlow, P.; St. Goar, F.; Rodriguez, L.; Silvestry, F.; Schwartz, A. Percutaneous mitral valve repair using the edge-to-edge technique: Six-month results of the EVEREST Phase I Clinical Trial. J. Am. Coll. Cardiol. 2005, 46, 2134–2140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- St. Goar, F.G.; Fann, J.I.; Komtebedde, J.; Foster, E.; Oz, M.C.; Fogarty, T.J.; Feldman, T.; Block, P.C. Endovascular edge-to-edge mitral valve repair: Short-term results in a porcine model. Circulation 2003, 108, 1990–1993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saji, M.; Rossi, A.M.; Ailawadi, G.; Dent, J.; Ragosta, M.; Lim, D.S. Adjunctive intracardiac echocardiography imaging from the left ventricle to guide percutaneous mitral valve repair with the MitraClip in patients with failed prior surgical rings. Catheter. Cardiovasc. Interv. 2016, 87, E75–E82. [Google Scholar] [CrossRef]
- Fuchs, F.C.; Hammerstingl, C.; Werner, N.; Grube, E.; Nickenig, G. Catheter-Based Edge-to-Edge Mitral Valve Repair After Partial Rupture of Surgical Annuloplasty Ring. JACC Cardiovasc. Interv. 2015, 8, e263–e264. [Google Scholar] [CrossRef] [Green Version]
- Schäfer, U.; Kreidel, F.; Frerker, C. MitraClip implantation as a new treatment strategy against systolic anterior motion-induced outflow tract obstruction in hypertrophic obstructive cardiomyopathy. Heart Lung Circ. 2014, 23, e131–e135. [Google Scholar] [CrossRef] [PubMed]
- Agricola, E.; Taramasso, M.; Marini, C.; Montorfano, M.; Godino, C.; Alfieri, O.; Colombo, A. First-in-man MitraClip implantation to treat late postoperative systolic anterior motion: Rare cause of tardive mitral repair failure. Circ. Cardiovasc. Interv. 2014, 7, 860–862. [Google Scholar] [CrossRef] [Green Version]
- Faletra, F.F.; Berrebi, A.; Pedrazzini, G.; Leo, L.A.; Paiocchi, V.L.; Cautilli, G.; Casso, G.; Cassina, T.; Moccetti, T.; Malouf, J.F. 3D transesophageal echocardiography: A new imaging tool for assessment of mitral regurgitation and for guiding percutaneous edge-to-edge mitral valve repair. Prog. Cardiovasc. Dis. 2017, 60, 305–321. [Google Scholar] [CrossRef]
- Hahn, R.T. Transcathether Valve Replacement and Valve Repair: Review of Procedures and Intraprocedural Echocardiographic Imaging. Circ Res 2016, 119, 341–356. [Google Scholar] [CrossRef] [PubMed]
- Faletra, F.F.; Pedrazzini, G.; Pasotti, E.; Muzzarelli, S.; Dequarti, M.C.; Murzilli, R.; Schlossbauer, S.A.; Slater, I.P.; Moccetti, T. 3D TEE during catheter-based interventions. JACC Cardiovasc. Imaging 2014, 7, 292–308. [Google Scholar] [CrossRef] [Green Version]
- Wunderlich, N.C.; Siegel, R.J. Peri-interventional echo assessment for the MitraClip procedure. Eur. Heart. J. Cardiovasc. Imaging 2013, 14, 935–949. [Google Scholar] [CrossRef] [Green Version]
- Faletra, F.F.; Pedrazzini, G.; Pasotti, E.; Petrova, I.; Drasutiene, A.; Dequarti, M.C.; Muzzarelli, S.; Moccetti, T. Role of real-time three dimensional transoesophageal echocardiography as guidance imaging modality during catheter based edge-to-edge mitral valve repair. Heart 2013, 99, 1204–1215. [Google Scholar] [CrossRef]
- Altiok, E.; Hamada, S.; Brehmer, K.; Kuhr, K.; Reith, S.; Becker, M.; Schröder, J.; Almalla, M.; Lehmacher, W.; Marx, N.; et al. Analysis of procedural effects of percutaneous edge-to-edge mitral valve repair by 2D and 3D echocardiography. Circ. Cardiovasc. Imaging 2012, 5, 748–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biner, S.; Perk, G.; Kar, S.; Rafique, A.M.; Slater, J.; Shiota, T.; Hussaini, A.; Chou, S.; Kronzon, I.; Siegel, R.J. Utility of combined two-dimensional and three-dimensional transesophageal imaging for catheter-based mitral valve clip repair of mitral regurgitation. J. Am. Soc. Echocardiogr. 2011, 24, 611–617. [Google Scholar] [CrossRef]
- Tamborini, G.; Mantegazza, V.; Penso, M.; Muratori, M.; Fusini, L.; Ali, S.G.; Cefalù, C.; Italiano, G.; Volpato, V.; Gripari, P.; et al. Predictive Value of Pre-Operative 2D and 3D Transthoracic Echocardiography in Patients Undergoing Mitral Valve Repair: Long Term Follow Up of Mitral Valve Regurgitation Recurrence and Heart Chamber Remodeling. J. Cardiovasc. Dev. Dis. 2020, 7, 46. [Google Scholar] [CrossRef]
- Lang, R.M.; Addetia, K.; Narang, A.; Mor-Avi, V. 3-Dimensional Echocardiography: Latest Developments and Future Directions. JACC Cardiovasc. Imaging. 2018, 11, 1854–1878. [Google Scholar] [CrossRef] [PubMed]






















Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pino, P.G.; Madeo, A.; Lucà, F.; Ceravolo, R.; di Fusco, S.A.; Benedetto, F.A.; Bisignani, G.; Oliva, F.; Colivicchi, F.; Gulizia, M.M.; et al. Clinical Utility of Three-Dimensional Echocardiography in the Evaluation of Mitral Valve Disease: Tips and Tricks. J. Clin. Med. 2023, 12, 2522. https://doi.org/10.3390/jcm12072522
Pino PG, Madeo A, Lucà F, Ceravolo R, di Fusco SA, Benedetto FA, Bisignani G, Oliva F, Colivicchi F, Gulizia MM, et al. Clinical Utility of Three-Dimensional Echocardiography in the Evaluation of Mitral Valve Disease: Tips and Tricks. Journal of Clinical Medicine. 2023; 12(7):2522. https://doi.org/10.3390/jcm12072522
Chicago/Turabian StylePino, Paolo G., Andrea Madeo, Fabiana Lucà, Roberto Ceravolo, Stefania Angela di Fusco, Francesco Antonio Benedetto, Giovanni Bisignani, Fabrizio Oliva, Furio Colivicchi, Michele Massimo Gulizia, and et al. 2023. "Clinical Utility of Three-Dimensional Echocardiography in the Evaluation of Mitral Valve Disease: Tips and Tricks" Journal of Clinical Medicine 12, no. 7: 2522. https://doi.org/10.3390/jcm12072522