

Inflammatory Markers as Predictors for Prolonged Duration of Hospitalization in Maxillofacial Infections
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection Process
2.2. Inclusion and Exclusion Criteria
- Patients age 18 years and over;
- Patients with complete medical records;
- Patients suffering from an abscess of maxillofacial origin, according to the ICD-10 classification of the diseases [39].
- Aged under 18 years;
- Pregnant women;
- Patients with cancer of different locations;
- Infections of other regions except for the head and neck;
- Non-maxillofacial head and neck infection;
- Incomplete medical records.
2.3. Explanatory Variables
- Demographic data (age, gender, and environment of origin);
- Routine blood test on admission to the hospital, WBC (nr × 10³/μL), CRP (mg/L), and hemogram index NLR—values were obtained by dividing absolute neutrophil and lymphocyte counts;
- The duration of hospitalization (DH) was measured in days starting on the day of the patient’s admission through the Emergency Unit of the Department of Maxillofacial Surgery.
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Study Population
3.2. Serum Markers at Admission
- Number of observations = 108.
- Area under ROC curve = 0.7730.
- Sensitivity and specificity obtained at this cut-off point should be simultaneously close to the AUC value;
- The difference between sensitivity and specificity obtained at this cut-off point should be minimum [41].
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zamiri, B.; Hashemi, S.B.; Hashemi, S.H.; Rafiee, Z.; Ehsani, S. Prevalence of odontogenic deep head and neck spaces infection and its correlation with length of hospital stay. J. Dent. Shiraz Univ. Med. Sci. 2012, 13, 29–35. [Google Scholar]
- Jundt, J.S.; Gutta, R. Characteristics and cost impact of severe odontogenic infections. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 558–566. [Google Scholar] [CrossRef]
- Eisler, L.; Wearda, K.; Romatoski, K.; Odland, R.M. Morbidity and cost of maxillofacial infections. Otolaryngol. Head Neck Surg. 2013, 149, 84–88. [Google Scholar] [CrossRef]
- Britt, J.C.; Josephson, G.D.; Gross, C.W. Ludwig’s angina in the pediatric population: Report of a case and review of the literature. Int. J. Pediatr. Otorhinolaryngol. 2000, 52, 79–87. [Google Scholar] [CrossRef]
- Zeitoun, I.M.; Dhanarajani, P.J. Cervical cellulitis and mediastinitis caused by odontogenic infections: Report of two cases and review of literature. J. Oral Maxillofac. Surg. 1995, 53, 203–208. [Google Scholar] [CrossRef]
- Ryan, P.; McMahon, G. Severe dental infections in the emergency department. Eur. J. Emerg. Med. 2012, 19, 208–213. [Google Scholar] [CrossRef]
- Arias-Chamorro, B.; Contreras-Morillo, M.; Acosta-Moyano, A.; Ruiz-Delgado, F.; Bermudo-Añino, L.; Valiente-Álvarez, A. Multiple odontogenic abscesses. Thoracic and abdomino-perineal extension in an immuno competent patient. Med. Oral Patol. Oral Cir. Bucal. 2011, 16, e772–e775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reynolds, S.C.; Chow, A.W. Life-threatening infections of the peripharyngeal and deep fascial spaces of the head and neck. Infect. Dis. Clin. N. Am. 2007, 21, 557–576, viii. [Google Scholar] [CrossRef]
- Jiménez, Y.; Bagán, J.V.; Murillo, J.; Poveda, R. Odontogenic infections complications, systemic manifestations. Med. Oral Patol. Oral Cir. Bucal. 2004, 9, 139–147. [Google Scholar]
- Roberson, J.B.; Harper, J.L.; Jauch, E.C. Mortality associated with cervicofacial necrotizing fasciitis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1996, 82, 264–267. [Google Scholar] [CrossRef] [PubMed]
- Wheatley, M.J.; Stirling, M.C.; Kirsh, M.M.; Gago, O.; Orringer, M.B. Descending necrotizing mediastinitis: Transcervical drainage is not enough. Ann. Thorac. Surg. 1990, 49, 780–784. [Google Scholar] [CrossRef]
- Levine, T.M.; Wurster, C.F.; Krespi, Y.P. Mediastinitis occurring as a complication of odontogenic infections. Laryngoscope 1986, 96, 747–750. [Google Scholar] [CrossRef] [PubMed]
- Garatea-Crelgo, J.; Gay-Escoda, C. Mediastinitis from odontogenic infection. Report of three cases and review of the literature. Int. J. Oral Maxillofac. Surg. 1991, 20, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Zachariades, N.; Mezitis, M.; Stavrinidis, P.; Konsolaki-Agouridaki, E. Mediastinitis, thoracic empyema, and pericarditis as complications of a dental abscess: Report of a case. J. Oral Maxillofac. Surg. 1988, 46, 493–495. [Google Scholar] [CrossRef] [PubMed]
- Yeo, G.S.; Kim, H.Y.; Kwak, E.J.; Jung, Y.S.; Park, H.S.; Jung, H.D. Cavernous sinus thrombosis caused by a dental infection: A case report. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 195–198, Erratum in J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 258. [Google Scholar] [CrossRef] [Green Version]
- Colbert, S.; Cameron, M.; Williams, J. Septic thrombosis of the cavernous sinus and dental infection. Br. J. Oral Maxillofac. Surg. 2011, 49, e25–e26. [Google Scholar] [CrossRef]
- Park, S.Y.; Suh, D.W.; Park, C.M.; Oh, M.S.; Lee, D.K. Brain abscess due to odontogenic infection: A case report. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 147–151. [Google Scholar] [CrossRef] [Green Version]
- Carpenter, J.; Stapleton, S.; Holliman, R. Retrospective analysis of 49 cases of brain abscess and review of the literature. Eur. J. Clin. Microbiol. Infect. Dis. 2007, 26, 1–11. [Google Scholar] [CrossRef]
- Nezafati, S.; Ghavimi, M.A.; Yavari, A.S. Localized osteomyelitis of the mandible secondary to dental treatment: Report of a case. J. Dent. Res. Dent. Clin. Dent. Prospects 2009, 3, 67–69. [Google Scholar] [CrossRef]
- Prasad, K.C.; Prasad, S.C.; Mouli, N.; Agarwal, S. Osteomyelitis in the head and neck. Acta Oto-Laryngol. 2007, 127, 194–205. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, S.G.; Moon, S.Y.; Oh, J.S.; Park, J.U.; Jeong, M.A.; Yang, S.J.; Jung, J.W.; Kim, J.S. Sepsis developed from an odontogenic infection: Case report. J. Korean Assoc. Maxillofac. Plast. Reconstr. Surg. 2011, 33, 445–448. [Google Scholar]
- Amponsah, E.; Donkor, P. Life-threatening oro-facial infections. Ghana Med. J. 2007, 41, 33–36. [Google Scholar] [PubMed]
- Fardy, C.H.; Findlay, G.; Owen, G.; Shortland, G. Toxic shock syndrome secondary to a dental abscess. Int. J. Oral Maxillofac. Surg. 1999, 28, 60–61. [Google Scholar] [CrossRef] [PubMed]
- Ogle, O.E. Maxillofacial Infections. Dent. Clin. N. Am. 2017, 61, 235–252. [Google Scholar] [CrossRef]
- Wang, J.; Ahani, A.; Pogrel, M. A five-year retrospective study of odontogenic maxillofacial infections in a large urban public hospital. Int. J. Oral Maxillofac. Surg. 2005, 34, 646–649. [Google Scholar] [CrossRef]
- Storoe, W.; Haug, R.H.; Lillich, T. The changing face of odontogenic infections. J. Oral Maxillofac. Surg. 2001, 59, 739–748. [Google Scholar] [CrossRef]
- Allareddy, V.; Rampa, S.; Nalliah, R.; Allareddy, V. Longitudinal discharge trends and outcomes after hospitalization for mouth cellulitis and Ludwig angina. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 524–531. [Google Scholar] [CrossRef]
- Gams, K.; Shewale, J.; Demian, N.; Khalil, K.; Banki, F. Characteristics, length of stay, and hospital bills associated with severe odontogenic infections in Houston, TX. J. Am. Dent. Assoc. 2017, 148, 221–229. [Google Scholar] [CrossRef]
- Gholami, M.; Mohammadi, H.; Amiri, N.; Khalife, H. Key factors of odontogenic infections requiring hospitalization: A retrospective study of 102 cases. J. Oral Max. Surg. Med. 2017, 29, 395–399. [Google Scholar] [CrossRef]
- Seppänen, L.; Lauhio, A.; Lindqvist, C.; Suuronen, R.; Rautemaa, R. Analysis of systemic and local odontogenic infection complications requiring hospital care. J. Infect. 2008, 57, 116–122. [Google Scholar] [CrossRef]
- Zheng, L.Y.; Yang, C.; Zhang, W.J.; Cai, X.Y.; Jiang, B.; Wang, B.L.; Pu, Y.P.; Jin, J.M.; Kim, E.; Wang, J.; et al. Comparison of multi-space infections of the head and neck in the elderly and non-elderly: Part I the descriptive data. J. Craniomaxillofac. Surg. 2013, 41, E208–E212. [Google Scholar] [CrossRef] [PubMed]
- Ordinului Ministrului Sănătăţii şi al Preşedintelui Casei Naţionale de Asigurări de Sănătate nr. 1068/627/2021 Privind Aprobarea Normelor Metodologice de Aplicare în Anul 2021 a Hotărârii Guvernului nr. 696/2021; Casa Naţională de Asigurări de Sănătate: Bucharest, Romania, 2021.
- Available online: https://www.spitalul-municipal-timisoara.ro/public/data_files/media/202106181301-ACTIVITATEA%20SCMUT%202020-min.pdf (accessed on 15 November 2022).
- Park, J.; Lee, J.Y.; Hwang, D.S.; Kim, Y.D.; Shin, S.H.; Kim, U.K.; Song, J.M. A retrospective analysis of risk factors of oromaxillofacial infection in patients presenting to a hospital emergency ward. Maxillofac. Plast. Reconstr. Surg. 2019, 41, 49. [Google Scholar] [CrossRef] [PubMed]
- Tan, F.Y.; Selvaraju, K.; Audimulam, H.; Yong, Z.C.; Adnan, T.H.; Balasundram, S. Length of hospital stay among oral and maxillofacial patients: A retrospective study. J. Korean Assoc. Oral Maxillofac. Surg. 2021, 47, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Peters, E.S.; Fong, B.; Wormuth, D.W.; Sonis, S.T. Risk factors affecting hospital length of stay in patients with odontogenic maxillofacial infections. J. Oral Maxillofac. Surg. 1996, 54, 1386–1391. [Google Scholar] [CrossRef]
- Available online: https://legislatie.just.ro/Public/DetaliiDocument/29780 (accessed on 15 November 2022).
- Sirin, D.A.; Ozcelik, F.; Uzun, C.; Ersahan, S.; Yesilbas, S. Association between C-reactive protein, neutrophil to lymphocyte ratio and the burden of apical periodontitis: A case-control study. Acta Odontol. Scand. 2019, 77, 142–149. [Google Scholar] [CrossRef]
- Steindel, S.J. International classification of diseases, 10th edition, clinical modification, and procedure coding system: Descriptive overview of the next generation HIPAA code sets. J. Am. Med. Inform. Assoc. 2010, 17, 274–282. [Google Scholar] [CrossRef] [Green Version]
- Unal, I. Defining an Optimal Cut-Point Value in ROC Analysis: An Alternative Approach. Comput. Math. Methods Med. 2017, 2017, 3762651. [Google Scholar] [CrossRef] [PubMed]
- Habibzadeh, F.; Habibzadeh, P.; Yadollahie, M. On determining the most appropriate test cut-off value: The case of tests with continuous results. Biochem. Med. 2016, 26, 297–307. [Google Scholar] [CrossRef] [Green Version]
- Flynn, T.R.; Shanti, R.M.; Hayes, C. Severe maxillofacial infections, part 2: Prospective outcomes study. J. Oral Maxillofac. Surg. 2006, 64, 1104–1113. [Google Scholar] [CrossRef]
- Ylijoki, S.; Suuronen, R.; Jousimies-Somer, H.; Meurman, J.H.; Lindqvist, C. Differences between patients with or without the need for intensive care due to severe maxillofacial infections. J. Oral Maxillofac. Surg. 2001, 59, 867–872, discussion 872–873. [Google Scholar] [CrossRef] [PubMed]
- Heim, N.; Wiedemeyer, V.; Reich, R.H.; Martini, M. The role of C-reactive protein and white blood cell count in the prediction of length of stay in hospital and severity of maxillofacial abscess. J. Craniomaxillofac. Surg. 2018, 46, 2220–2226. [Google Scholar] [CrossRef] [PubMed]
- Stathopoulos, P.; Igoumenakis, D.; Shuttleworth, J.; Smith, W.; Ameerally, P. Predictive factors of hospital stay in patients with maxillofacial infections: The role of C-reactive protein. Br. J. Oral Maxillofac. Surg. 2017, 55, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Giraddi, G.; Krishnan, G.; Shahi, A.K. Efficacy of Serum Prealbumin and CRP Levels as Monitoring Tools for Patients with Fascial Space Infections of Odontogenic Origin: A Clinicobiochemical Study. J. Maxillofac. Oral Surg. 2014, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Şentürk, M.; Azgın, İ.; Övet, G.; Alataş, N.; Ağırgöl, B.; Yılmaz, E. The role of the mean platelet volume and neutro-phil-to-lymphocyte ratio in peritonsillar abscesses. Braz. J. Otorhinolaryngol. 2016, 82, 662–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dogruel, F.; Gonen, Z.B.; Gunay-Canpolat, D.; Zararsiz, G.; Alkan, A. The Neutrophil-to-Lymphocyte ratio as a marker of recovery status in patients with severe dental infection. Med. Oral Patol. Oral Cir. Bucal. 2017, 22, e440–e445. [Google Scholar] [CrossRef]
- Ishimine, N.; Honda, T.; Yoshizawa, A.; Kawasaki, K.; Sugano, M.; Kobayashi, Y.; Matsumoto, T. Combination of white blood cell count and left shift level real-timely reflects a course of bacterial infection. J. Clin. Lab. Anal. 2013, 27, 407–411. [Google Scholar] [CrossRef]
- Gürol, G.; Çiftci, İ.H.; Terizi, H.A.; Atasoy, A.R.; Ozbek, A.; Köroğlu, M. Are there standardized cutoff values for neutro-phil-lymphocyte ratios in bacteremia or sepsis? J. Microbiol. Biotechnol. 2015, 25, 521–525. [Google Scholar] [CrossRef]
- Lorenzovici, L.; Székely, A. Evoluția costului pe zi spitalizare în spitalele publice din România între 2015–2019 și impactul asupra cost-eficienței medicamentelor. In Proceedings of the Conferinta Nationala de Farmacoeconomie si Management Sanitar, Poiana Brasov, Romania, 10–13 October 2019. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | Short Hospitalization (Group A) (n = 54) | Long Hospitalization (Group B) (n = 54) | Significance |
|---|---|---|---|
| Age, mean (SD) * | 44.05 (19.17) | 59.5 (15.79) | 0.047 * |
| Age range | 18–85 | 20–81 | - |
| Gender, n (%) Men *** | 34 (62.96%) | 32 (59.25%) | 0.843 *** |
| Gender, n (%) Women *** | 20 (37.03%) | 22 (40.74%) | |
| Place of origin, n (%) Urban *** | 32 (59.25%) | 30 (55.55%) | 0.845 *** |
| Place of origin, n (%) Rural *** | 22 (40.74%) | 24 (44.44%) | |
| Smoking, n (%) Yes *** | 9 (8.3) | 19 (17.6) | 0.047 *** |
| Smoking, n (%) No *** | 45 (32.4) | 35 (17.6) | |
| Comorbidities, n (%) Diabetes ** | 10 (9.3) | 28 (25.9) | <0.001 ** |
| Comorbidities, n (%) Obesity ** | 31 (28.7) | 37 (34.3) | 0.466 ** |
| Comorbidities, n (%) Chronic kidney disease ** | 14 (13.0) | 17 (15.7) | 0.590 ** |
| Comorbidities, n (%) Human Immunodeficiency Virus ** | 1 (0.9) | 1 (0.9) | 1.000 ** |
| Comorbidities, n (%) Malignancy ** | 5 (4.6) | 7 (6.5) | 0.563 ** |
| Location of the infection site, n (%) Perimaxillary ** | 13 (12.0) | 10 (9.3) | 0.531 ** |
| Location of the infection site, n (%) ** Perimandibular | 14 (13.0) | 18 (1.7) | 0.479 ** |
| Location of the infection site, n (%) Superficial lodges ** | 27 (25.0) | 29 (26.9) | 0.789 ** |
| Variables | Total Subjects | A (Short Duration of Hospitalization) | B (Long Duration of Hospitalization) | p-Value * | |||
|---|---|---|---|---|---|---|---|
| Median * | 95% CI * | Median * | 95% CI * | Median * | 95% CI * | ||
| WBC | 11,105 | (9833–11,700) | 9.34 | 8.240 to 9.900 | 12.02 | 11.516 to 12.639 | p < 0.001 |
| CRP | 63.5 | (49.6–78.63) | 45.95 | 19.660 to 61.348 | 86.00 | 65.660 to 98.000 | p < 0.001 |
| NLR | 3.23 | (3.08–3.58) | 2.99 | 2.34 to 3.29 | 3.51 | 3.20 to 3.88 | p = 0.038 |
| Duration of hospitalization | 5.5 | (5.0 to 7.66) | 4.0 | 3.00 to 4.00 | 10.0 | 9.00 to 12.66 | p < 0.001 |
| Linear Regression for Predictor Variables | WBC | CRP | NLR | |||
|---|---|---|---|---|---|---|
| Coefficient of determination R2 | 0.0786 | 0.1219 | 0.0086 | |||
| Residual standard deviation | 5.2600 | 5.1349 | 5.4560 | |||
| y = 4.0149 + 0.3295 × X * | y = 5.4258 + 0.0343 × X * | y = 7.760 + 0.0057 × X * | ||||
| Coeff. | SE. | Coeff. | SE. | Coeff. | SE. | |
| Intercept | 4.0149 | 1.3670 | 5.4258 | 0.7987 | 7.7609 | 0.5304 |
| Slope | 0.3295 | 0.1096 | 0.0343 | 0.0089 | 0.0057 | 0.0059 |
| F-ratio | 9.0426 | 14.7197 | 0.9280 | |||
| Significance level | p = 0.003 | p = 0.0002 | p = 0.337 | |||
| Correlation coefficient r | 0.2804 | 0.3492 | 0.0931 | |||
| Logistic regression for predictor variables | WBC | CRP | NLR | |||
| Odds ratio | 1.2394 | 1.0139 | 1.1097 | |||
| 95% CI | 1.1023 to 1.3933 | 1.0051 to 1.0227 | 0.9673 to 1.2730 | |||
| p-value | p < 0.001 | p = 0.002 | p = 0.137 | |||
| Multiple regression for predictor variables | WBC | CRP | ||||
| Odds ratio | 1.1992 | 1.0099 | ||||
| 95% CI | 1.0659 to 1.3491 | 1.0011 to 1.0189 | ||||
| p-value | 0.003 | 0.027 | ||||
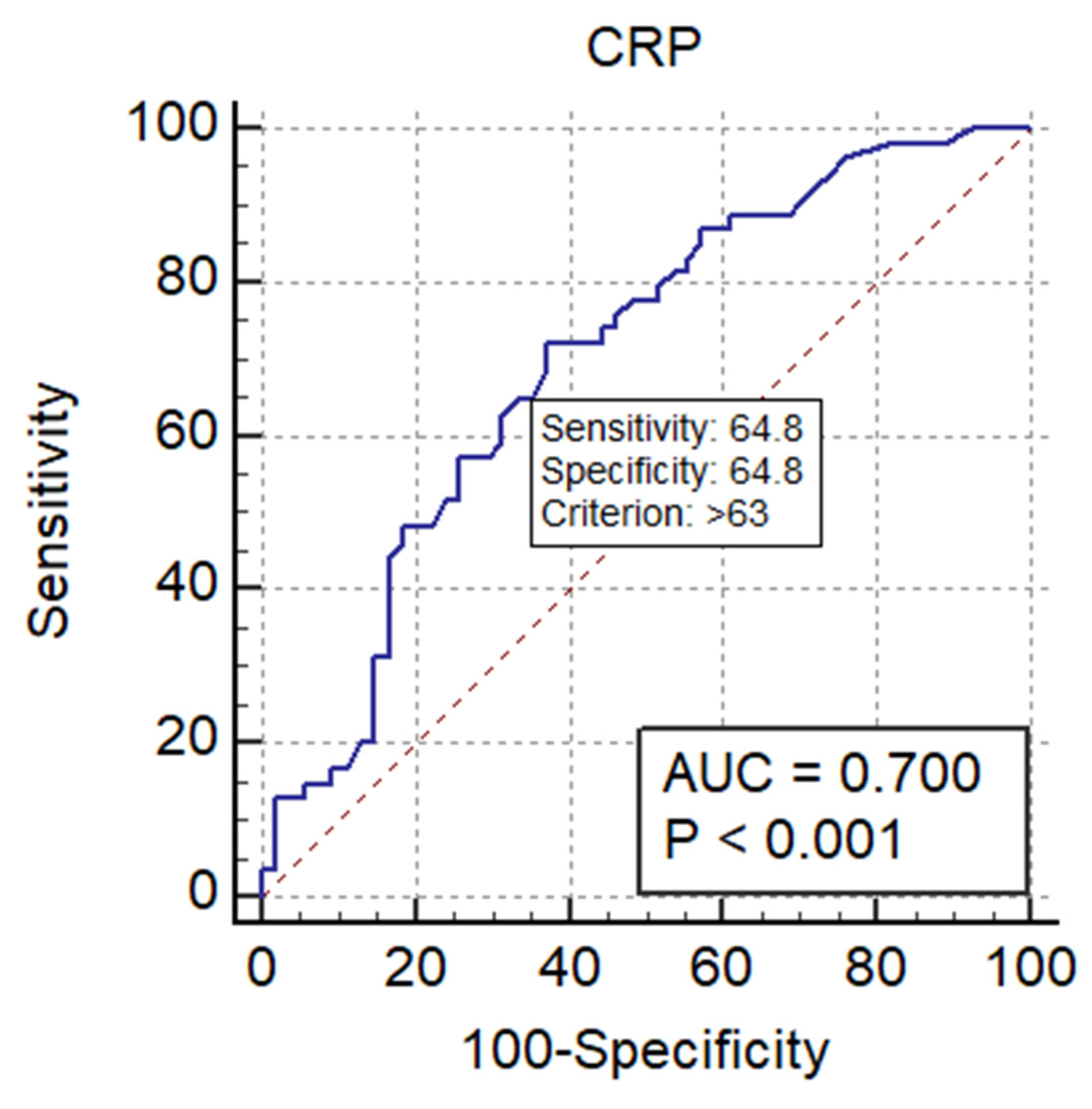
| Variables | Cut-Off Values | Area under ROC Curve (AUC) | 95% CI | Significance Level p | Sensitivity | Specificity |
|---|---|---|---|---|---|---|
| WBC | 11.03 * | 0.746 | 0.653 to 0.825 | <0.001 | 79.63 | 64.81 |
| CRP | 63 ** | 0.700 | 0.605 to 0.785 | <0.001 | 72.22 | 62.96 |
| NLR | 0.616 | 0.517 to 0.708 | 0.037 | 75.93 | 57.41 | |
| WBC and CRP | 0.773 | <0.001 | 66.67% | 77.78% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urechescu, H.; Gheran-Vida, E.; Cuzic, C.; Ancusa, O.; Ursoniu, S.; Pricop, M. Inflammatory Markers as Predictors for Prolonged Duration of Hospitalization in Maxillofacial Infections. J. Clin. Med. 2023, 12, 871. https://doi.org/10.3390/jcm12030871
Urechescu H, Gheran-Vida E, Cuzic C, Ancusa O, Ursoniu S, Pricop M. Inflammatory Markers as Predictors for Prolonged Duration of Hospitalization in Maxillofacial Infections. Journal of Clinical Medicine. 2023; 12(3):871. https://doi.org/10.3390/jcm12030871
Chicago/Turabian StyleUrechescu, Horatiu, Eleonora Gheran-Vida, Cristiana Cuzic, Oana Ancusa, Sorin Ursoniu, and Marius Pricop. 2023. "Inflammatory Markers as Predictors for Prolonged Duration of Hospitalization in Maxillofacial Infections" Journal of Clinical Medicine 12, no. 3: 871. https://doi.org/10.3390/jcm12030871