

Oversizing Consideration of Proximal Stent Graft in Hemodynamically Stable and Unstable Patients Undergoing Emergent Endovascular Aortic Repair
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Approvals
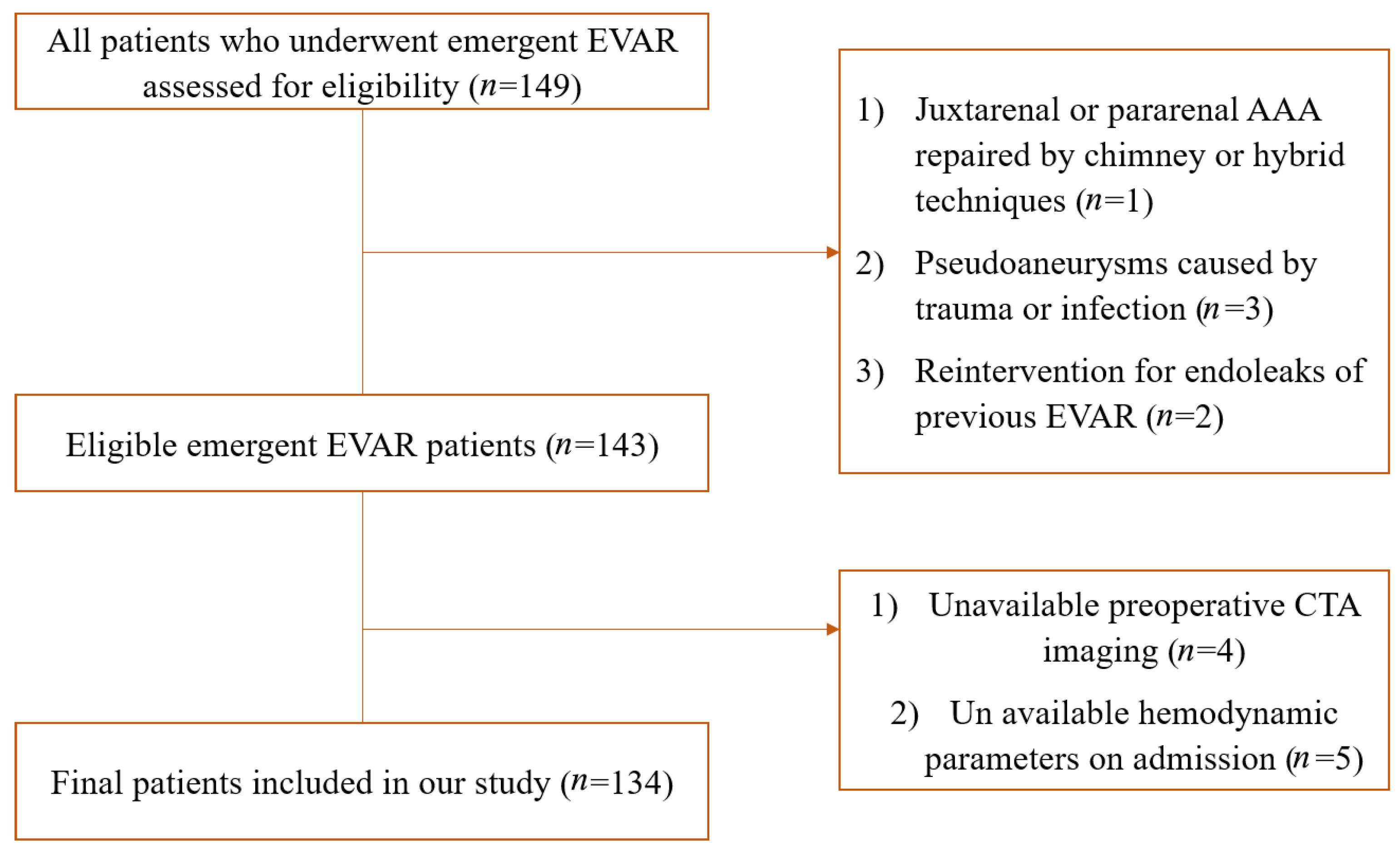
2.2. Participants
2.3. Exposures
2.4. Outcomes of Interest and Follow-Up Protocols
2.5. Variables
2.6. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Risk Factors of T1AEL in Emergent EVAR
3.3. Comparison of Outcomes in Hemodynamically Unstable and Stable Patients
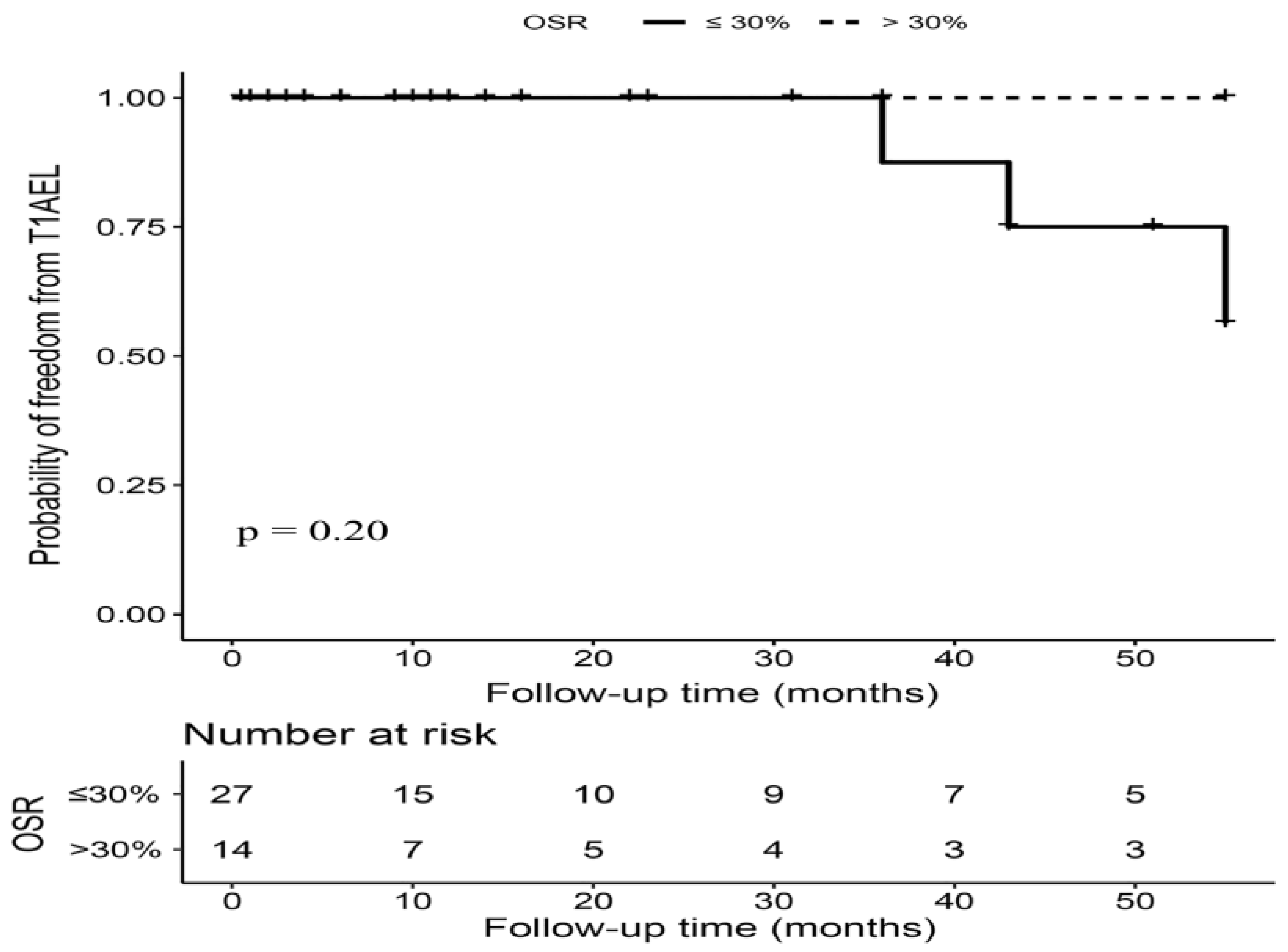
3.4. OSR > 30% versus OSR ≤ 30% in Hemodynamically Unstable Patients
3.5. OSR > 20% versus OSR ≤ 20% in Hemodynamically Stable Patients
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parodi, J.C.; Palmaz, J.C.; Barone, H.D. Transfemoral intraluminal graft implantation for abdominal aortic aneurysms. Ann. Vasc. Surg. 1991, 5, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Investigators, I.T. Comparative clinical effectiveness and cost effectiveness of endovascular strategy v open repair for ruptured abdominal aortic aneurysm: Three year results of the IMPROVE randomised trial. BMJ 2017, 359, j4859. [Google Scholar] [CrossRef] [PubMed]
- Sweeting, M.J.; Balm, R.; Desgranges, P.; Ulug, P.; Powell, J.T.; Koelemay, M.J.W.; Idu, M.M.; Kox, C.; Legemate, D.A.; Huisman, L.C.; et al. Individual-patient meta-analysis of three randomized trials comparing endovascular versus open repair for ruptured abdominal aortic aneurysm. Br. J. Surg. 2015, 102, 1229–1239. [Google Scholar] [CrossRef] [PubMed]
- Mastracci, T.M.; Garrido-Olivares, L.; Cinà, C.S.; Clase, C.M. Endovascular repair of ruptured abdominal aortic aneurysms: A systematic review and meta-analysis. J. Vasc. Surg. 2008, 47, 214–221. [Google Scholar] [CrossRef]
- Patel, R.; Sweeting, M.J.; Powell, J.T.; Greenhalgh, R.M. Endovascular versus open repair of abdominal aortic aneurysm in 15-years’ follow-up of the UK endovascular aneurysm repair trial 1 (EVAR trial 1): A randomised controlled trial. Lancet 2016, 388, 2366–2374. [Google Scholar] [CrossRef]
- Major, M.; Long, G.W.; Eden, C.L.; Studzinski, D.M.; Callahan, R.E.; Brown, O.W. Long-term outcomes and interventions of postoperative type 1a endoleak following elective endovascular aortic aneurysm repair. J. Vasc. Surg. 2021, 75, 136–143.e1. [Google Scholar] [CrossRef]
- Oliveira, N.F.; Oliveira-Pinto, J.; van Rijn, M.J.; Baart, S.; Raa, S.T.; Hoeks, S.E.; Gonçalves, F.B.; Verhagen, H.J. Risk Factors, Dynamics, and Clinical Consequences of Aortic Neck Dilatation after Standard Endovascular Aneurysm Repair. Eur. J. Vasc. Endovasc. Surg. 2021, 62, 26–35. [Google Scholar] [CrossRef]
- Wanhainen, A.; Verzini, F.; Van Herzeele, I.; Allaire, E.; Bown, M.; Cohnert, T.; Dick, F.; van Herwaarden, J.; Karkos, C.; Koelemay, M.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 8–93. [Google Scholar] [CrossRef]
- Chaikof, E.L.; Dalman, R.L.; Eskandari, M.K.; Jackson, B.M.; Lee, W.A.; Mansour, M.A.; Mastracci, T.M.; Mell, M.; Murad, M.H.; Nguyen, L.L.; et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J. Vasc. Surg. 2018, 67, 2–77.e2. [Google Scholar] [CrossRef]
- Gonthier, C.; Deglise, S.; Brizzi, V.; Ducasse, E.; Midy, D.; Lachat, M.; Berard, X. Hemodynamic Conditions may Influence the Oversizing of Stent Grafts and the Postoperative Surveillance of Patients with Ruptured Abdominal Aortic Aneurysm Treated by EVAR. Ann. Vasc. Surg. 2016, 30, 308.e5–308.e10. [Google Scholar] [CrossRef]
- Jonker, F.H.; Verhagen, H.J.; Mojibian, H.; Davis, K.A.; Moll, F.L.; Muhs, B.E. Aortic endograft sizing in trauma patients with hemodynamic instability. J. Vasc. Surg. 2010, 52, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Kratzberg, J.A.; Golzarian, J.; Raghavan, M.L. Role of graft oversizing in the fixation strength of barbed endovascular grafts. J. Vasc. Surg. 2009, 49, 1543–1553. [Google Scholar] [CrossRef] [PubMed]
- Sternbergh, W.C., 3rd; Money, S.R.; Greenberg, R.K.; Chuter, T.A.; Zenith Investigators. Influence of endograft oversizing on device migration, endoleak, aneurysm shrinkage, and aortic neck dilation: Results from the Zenith Multicenter Trial. J. Vasc. Surg. 2004, 39, 20–26. [Google Scholar] [CrossRef] [PubMed]
- van Prehn, J.; Schlösser, F.J.; Muhs, B.E.; Verhagen, H.J.; Moll, F.L.; van Herwaarden, J.A. Oversizing of aortic stent grafts for abdominal aneurysm repair: A systematic review of the benefits and risks. Eur. J. Vasc. Endovasc. Surg. 2009, 38, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Rakita, D.; Newatia, A.; Hines, J.J.; Siegel, D.N.; Friedman, B. Spectrum of CT findings in rupture and impending rupture of abdominal aortic aneurysms. Radiographics 2007, 27, 497–507. [Google Scholar] [CrossRef]
- Sundararajan, V.; Henderson, T.; Perry, C.; Muggivan, A.; Quan, H.; Ghali, W.A. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J. Clin. Epidemiol. 2004, 57, 1288–1294. [Google Scholar] [CrossRef]
- Oliveira, N.F.; Bastos Gonçalves, F.M.; de Vries, J.P.; Ultee, K.; Werson, D.; Hoeks, S.; Moll, F.; van Herwaarden, J.; Verhagen, H. Mid-Term Results of EVAR in Severe Proximal Aneurysm Neck Angulation. Eur. J. Vasc. Endovasc. Surg. 2015, 49, 19–27. [Google Scholar] [CrossRef]
- Lee, P.H.; Burstyn, I. Identification of confounder in epidemiologic data contaminated by measurement error in covariates. BMC Med. Res. Methodol. 2016, 16, 54. [Google Scholar] [CrossRef]
- Belkin, N.; Jackson, B.M.; Foley, P.J.; Damrauer, S.M.; Kalapatapu, V.; Golden, M.A.; Fairman, R.M.; Wang, G.J. The use of intravascular ultrasound in the treatment of type B aortic dissection with thoracic endovascular aneurysm repair is associated with improved long-term survival. J. Vasc. Surg. 2020, 72, 490–497. [Google Scholar] [CrossRef]
- Rodriguez, M.C.; Realyvasquez, A.; Galante, J.; Pevec, W.; Humphries, M. Differences in Aortic Diameter Measurements with Intravascular Ultrasound and Computed Tomography After Blunt Traumatic Aortic Injury. J. Vasc. Surg. 2016, 64, 545. [Google Scholar] [CrossRef]
- Taalab, M.A.; Kamal, A.M.; Mohammad, A.F.; Zaki, M.M. Intravascular Ultrasound Versus Computed Tomography Angiography in Sizing and Operative Management of Endovascular Aortic Aneurysm Repair. J. Endovasc. Ther. 2023. [Google Scholar] [CrossRef] [PubMed]
- Illuminati, G.; Pacilè, M.A.; Ceccanei, G.; Ruggeri, M.; La Torre, G.; Ricco, J.-B. Peroperative intravascular ultrasound for endovascular aneurysm repair versus peroperative angiography: A pilot study in fit patients with favorable anatomy. Ann. Vasc. Surg. 2020, 64, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.-H.; Yeh, M.-L.; Chen, W.-L.; Kan, C.-D. Apparatus for Comparison of Pullout Forces for Various Thoracic Stent Grafts at Varying Neck Angulations and Oversizes. Ann. Vasc. Surg. 2016, 31, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Shiraev, T.; Agostinho, N.; Dubenec, S. Sizing Considerations for GORE Excluder in Angulated Aortic Aneurysm Necks. Ann. Vasc. Surg. 2018, 49, 152–157. [Google Scholar] [CrossRef]
- Mwipatayi, B.P.; Faraj, J.; Oshin, O.; on behalf of the ENGAGE REGISTRY co-investigators. Endurant Stent Graft Demonstrates Promising Outcomes in Challenging Abdominal Aortic Aneurysm Anatomy. J. Vasc. Surg. 2021, 73, 69–80. [Google Scholar] [CrossRef]
- IMPROVE Trial Investigators; Powell, J.T.; Hinchliffe, R.J.; Thompson, M.M.; Sweeting, M.J.; Ashleigh, R.; Bell, R.; Gomes, M.; Greenhalgh, R.M.; Grieve, R.J.; et al. Observations from the IMPROVE trial concerning the clinical care of patients with ruptured abdominal aortic aneurysm. Br. J. Surg. 2014, 101, 216–224. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Hemodynamically Stable | Hemodynamically Unstable | p-Value | |
|---|---|---|---|
| n = 90 | n = 44 | ||
| Age -y | 70.41 ± 9.89 | 72.55 ± 8.24 | 0.22 |
| MAP -mmHg | 97.91 ± 12.55 | 80.61 ± 9.30 | <0.001 |
| HR -beats/min | 77.44 ± 13.08 | 103.82 ± 5.96 | <0.001 |
| BMI -kg/m2 | 23.00 ± 3.15 | 22.93 ± 2.96 | 0.91 |
| Neck diameter -mm | 20.39 ± 2.41 | 20.43 ± 2.45 | 0.93 |
| OSR -% | 22% (20–27%) | 25% (22–32%) | 0.011 |
| α angle -° | 27.66 (12.93–45.42) | 32.50 (10.77–66.73) | 0.025 |
| β angle -° | 48.00 (32.00–76.00) | 57.23 (31.41–78.63) | 0.86 |
| Neck length -mm | 27.83 ± 12.97 | 25.10 ± 10.02 | 0.22 |
| Neck calcification | 0.01 (0.00–0.20) | 0.01 (0.00–0.20) | 0.76 |
| Maximum diameter -mm | 57.81 ± 14.18 | 63.82 ± 19.26 | 0.048 |
| Within IFU | 37 (41.11%) | 21 (47.73%) | 0.46 |
| Gender | 0.027 | ||
| Male | 73 (81.11%) | 28 (63.64%) | |
| Female | 17 (18.89%) | 16 (36.36%) | |
| Hypertension | 59 (65.56%) | 31 (70.45%) | 0.57 |
| Diabetes | 10 (11.11%) | 7 (15.91%) | 0.43 |
| Pulmonary diseases | 16 (17.78%) | 11 (25.00%) | 0.33 |
| Peripheral artery disease | 6 (6.67%) | 3 (6.82%) | 0.97 |
| Stroke | 6 (6.67%) | 0 (0.00%) | 0.97 |
| PCI | 11 (12.22%) | 4 (9.09%) | 0.59 |
| CKD | 8 (8.89%) | 9 (20.45%) | 0.059 |
| CCI scores | 0.41 | ||
| Mild (≤2) | 70 (77.78%) | 29 (65.91%) | |
| Moderate (3–4) | 17 (18.89%) | 10 (22.73%) | |
| Severe (≥5) | 3 (3.33%) | 5 (11.36%) | |
| Anesthesia | 0.032 | ||
| Local | 71 (78.89%) | 27 (61.36%) | |
| General | 19 (21.11%) | 17 (38.64%) | |
| Severe neck angulation | 24 (26.67%) | 18 (40.91%) | 0.10 |
| CIAA | 29 (25.66%) | 9 (19.57%) | 0.41 |
| Univariate Analysis | Multivariate Analysis * | |||
|---|---|---|---|---|
| Statistics | HR (95%CI) | p-Value | HR (95%CI) | p-Value |
| Gender | 2.76 (0.61, 12.40) | 0.19 | ||
| Age | 1.03 (0.94, 1.13) | 0.53 | ||
| HD unstable | 1.87 (0.42, 8.45) | 0.41 | ||
| MAP | 0.97 (0.91, 1.04) | 0.39 | ||
| HR | 1.01 (0.96, 1.06) | 0.78 | ||
| Anesthesia | 0.46 (0.05, 3.83) | 0.47 | ||
| α angle | 0.99 (0.97, 1.01) | 0.42 | ||
| β angle | 1.01 (0.99, 1.03) | 0.32 | ||
| SNA | 2.24 (0.43, 11.67) | 0.34 | ||
| Neck diameter | 1.27 (1.03, 1.56) | 0.028 | 0.92 (0.63, 1.35) | 0.67 |
| OSR >30% vs. ≤30% | 0.57 (0.06, 5.07) | 0.62 | ||
| OSR >20% vs. ≤20% | 0.06 (0.01, 0.31) | 0.001 | 0.06 (0.01, 0.72) | 0.026 |
| Neck length | 0.83 (0.72, 0.95) | 0.009 | 0.74 (0.56, 0.98) | 0.033 |
| Maximum diameter | 1.03 (0.98, 1.09) | 0.24 | ||
| CIAA | 0.63 (0.13, 3.18) | 0.58 |
| Hemodynamically Unstable | Hemodynamically Stable | |||||
|---|---|---|---|---|---|---|
| OSR | ≤30% (n = 30) | >30% (n = 14) | p | ≤20% (n = 24) | >20% (n = 66) | p |
| Survival FU time-m | 24.50 (16.00–49.25) | 25.00 (9.75–53.00) | 0.99 | 30.50 (15.00–60.50) | 33.50 (11.50–69.25) | 0.57 |
| Imaging FU time-m | 10.00 (1.00–39.50) | 1.50 (1.25–32.50) | 0.87 | 16.50 (5.00–29.00) | 15.00 (5.25–34.50) | 0.71 |
| 30-day mortality | 4 (13.33%) | 0 (.00%) | 0.15 | 1 (4.17%) | 1 (1.52%) | 0.45 |
| Overall survival | 11 (36.67%) | 6 (42.86%) | 0.69 | 7 (29.17%) | 15 (22.73%) | 0.53 |
| Reintervention | 2 (6.67%) | 1 (7.14%) | 0.95 | 4 (16.67%) | 6 (9.09%) | 0.31 |
| T1AEL | 3 (11.11%) | 0 (0.00%) | 0.19 | 4 (16.67%) | 1 (1.52%) | 0.006 |
| T1BEL | 2 (7.41%) | 0 (0.00%) | 0.30 | 3 (12.50%) | 4 (6.06%) | 0.31 |
| T2EL | 5 (18.52%) | 2 (14.29%) | 0.73 | 6 (25.00%) | 14 (21.21%) | 0.70 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qi, Y.; Weng, C.; Yuan, D.; Wang, T.; Ma, Y.; Yang, Y.; Zhao, J.; Huang, B. Oversizing Consideration of Proximal Stent Graft in Hemodynamically Stable and Unstable Patients Undergoing Emergent Endovascular Aortic Repair. J. Clin. Med. 2023, 12, 7500. https://doi.org/10.3390/jcm12237500
Qi Y, Weng C, Yuan D, Wang T, Ma Y, Yang Y, Zhao J, Huang B. Oversizing Consideration of Proximal Stent Graft in Hemodynamically Stable and Unstable Patients Undergoing Emergent Endovascular Aortic Repair. Journal of Clinical Medicine. 2023; 12(23):7500. https://doi.org/10.3390/jcm12237500
Chicago/Turabian StyleQi, Yuhan, Chengxin Weng, Ding Yuan, Tiehao Wang, Yukui Ma, Yi Yang, Jichun Zhao, and Bin Huang. 2023. "Oversizing Consideration of Proximal Stent Graft in Hemodynamically Stable and Unstable Patients Undergoing Emergent Endovascular Aortic Repair" Journal of Clinical Medicine 12, no. 23: 7500. https://doi.org/10.3390/jcm12237500