
Real-World Comparison of Transcatheter Versus Surgical Aortic Valve Replacement in the Era of Current-Generation Devices

 , , , ,
, , , ,
Abstract
:
1. Introduction
2. Methods
2.1. Study Design
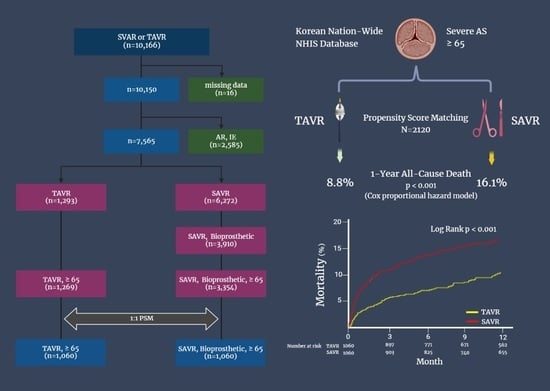
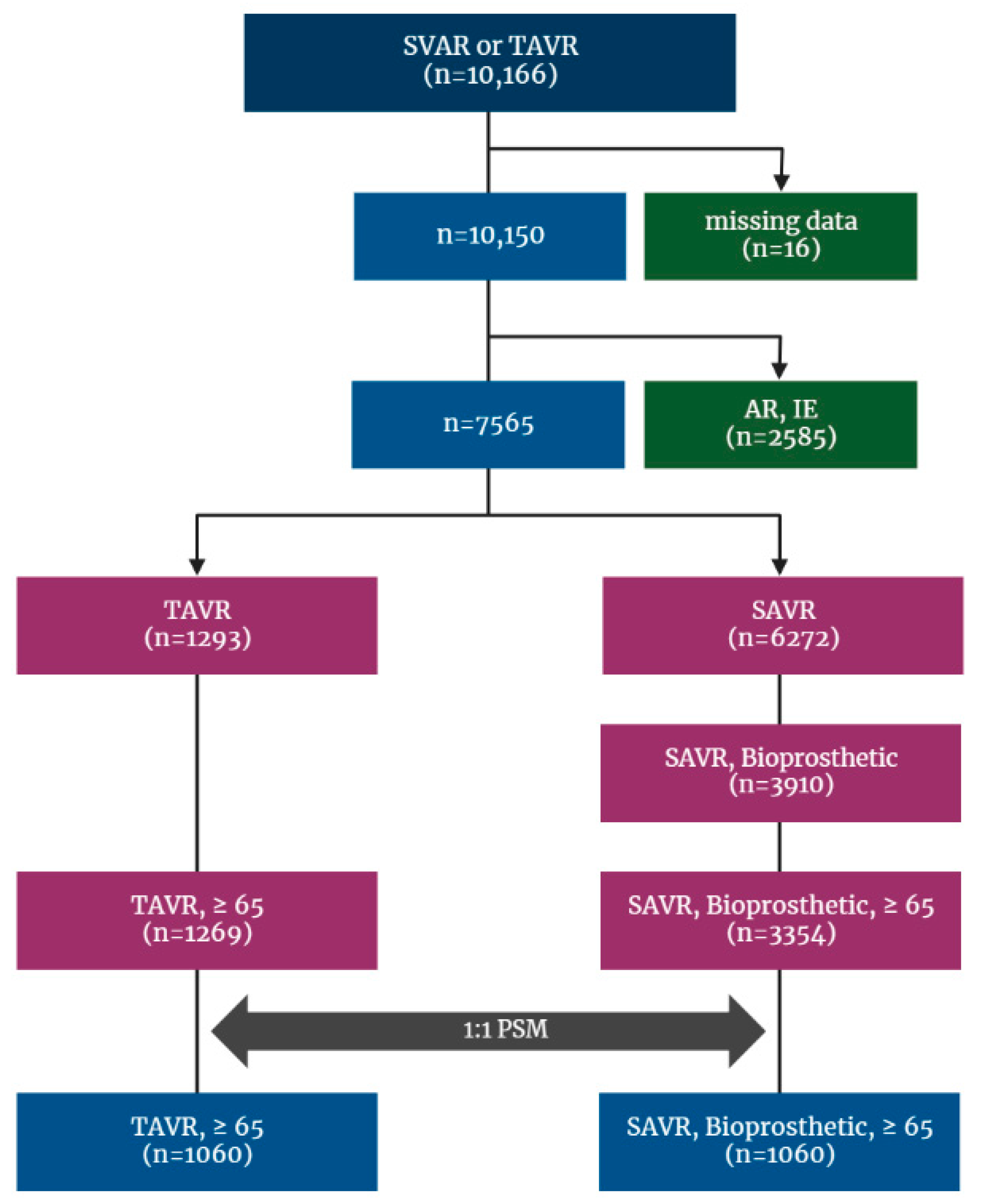
2.2. Patients Selection
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Procedures
3.3. Clinical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Leon, M.B.; Smith, C.R.; Mack, M.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N. Engl. J. Med. 2010, 363, 1597–1607. [Google Scholar] [CrossRef] [Green Version]
- Kapadia, S.R.; Leon, M.B.; Makkar, R.R.; Tuzcu, E.M.; Svensson, L.G.; Kodali, S.; Webb, J.G.; Mack, M.J.; Douglas, P.S.; Thourani, V.H.; et al. 5-year outcomes of transcatheter aortic valve replacement compared with standard treatment for patients with inoperable aortic stenosis (PARTNER 1): A randomised controlled trial. Lancet 2015, 385, 2485–2491. [Google Scholar] [CrossRef]
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef] [Green Version]
- Adams, D.H.; Popma, J.J.; Reardon, M.J.; Yakubov, S.J.; Coselli, J.S.; Deeb, G.M.; Gleason, T.G.; Buchbinder, M.; Hermiller, J., Jr.; Kleiman, N.S.; et al. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N. Engl. J. Med. 2014, 370, 1790–1798. [Google Scholar] [CrossRef] [Green Version]
- Kodali, S.K.; Williams, M.R.; Smith, C.R.; Svensson, L.G.; Webb, J.G.; Makkar, R.R.; Fontana, G.P.; Dewey, T.M.; Thourani, V.H.; Pichard, A.D.; et al. Two-year outcomes after transcatheter or surgical aortic-valve replacement. N. Engl. J. Med. 2012, 366, 1686–1695. [Google Scholar] [CrossRef] [Green Version]
- Mack, M.J.; Leon, M.B.; Smith, C.R.; Miller, D.C.; Moses, J.W.; Tuzcu, E.M.; Webb, J.G.; Douglas, P.S.; Anderson, W.N.; Blackstone, E.H.; et al. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): A randomised controlled trial. Lancet 2015, 385, 2477–2484. [Google Scholar] [CrossRef]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef]
- Reardon, M.J.; Van Mieghem, N.M.; Popma, J.J.; Kleiman, N.S.; Søndergaard, L.; Mumtaz, M.; Adams, D.H.; Deeb, G.M.; Maini, B.; Gada, H.; et al. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2017, 376, 1321–1331. [Google Scholar] [CrossRef]
- Thyregod, H.G.; Steinbrüchel, D.A.; Ihlemann, N.; Nissen, H.; Kjeldsen, B.J.; Petursson, P.; Chang, Y.; Franzen, O.W.; Engstrøm, T.; Clemmensen, P.; et al. Transcatheter Versus Surgical Aortic Valve Replacement in Patients with Severe Aortic Valve Stenosis: 1-Year Results From the All-Comers NOTION Randomized Clinical Trial. J. Am. Coll. Cardiol. 2015, 65, 2184–2194. [Google Scholar] [CrossRef] [Green Version]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef]
- Yu, C.W.; Kim, W.J.; Ahn, J.M.; Kook, H.; Kang, S.H.; Han, J.K.; Ko, Y.G.; Choi, S.H.; Koo, B.K.; Chang, K.; et al. Trends and Outcomes of Transcatheter Aortic Valve Implantation (TAVI) in Korea: The Results of the First Cohort of Korean TAVI Registry. Korean Circ. J. 2018, 48, 382–394. [Google Scholar] [CrossRef] [Green Version]
- 2021년 하반기 「경피적 대동맥판삽입 (TAVI) 」 실시 승인기관 안내. 건강보험심사평가원. Available online: https://www.hira.or.kr/bbsDummy.do?pgmid=HIRAA020002000100&brdScnBltNo=4&brdBltNo=9274&pageIndex=1#none (accessed on 16 December 2021).
- Kim, L.; Kim, J.A.; Kim, S. A guide for the utilization of Health Insurance Review and Assessment Service National Patient Samples. Epidemiol. Health 2014, 36, e2014008. [Google Scholar] [CrossRef] [Green Version]
- KOICD 질병분류 정보센터. Available online: https://www.koicd.kr/ins/act.do (accessed on 6 June 2020).
- Reinöhl, J.; Kaier, K.; Reinecke, H.; Schmoor, C.; Frankenstein, L.; Vach, W.; Cribier, A.; Beyersdorf, F.; Bode, C.; Zehender, M. Effect of Availability of Transcatheter Aortic-Valve Replacement on Clinical Practice. N. Engl. J. Med. 2015, 373, 2438–2447. [Google Scholar] [CrossRef]
- Fraccaro, C.; Tarantini, G.; Rosato, S.; Tellaroli, P.; D’Errigo, P.; Tamburino, C.; Onorati, F.; Ranucci, M.; Barbanti, M.; Grossi, C.; et al. Early and Midterm Outcome of Propensity-Matched Intermediate-Risk Patients Aged ≥80 Years with Aortic Stenosis Undergoing Surgical or Transcatheter Aortic Valve Replacement (from the Italian Multicenter OBSERVANT Study). Am. J. Cardiol. 2016, 117, 1494–1501. [Google Scholar] [CrossRef]
- Herrmann, H.C.; Daneshvar, S.A.; Fonarow, G.C.; Stebbins, A.; Vemulapalli, S.; Desai, N.D.; Malenka, D.J.; Thourani, V.H.; Rymer, J.; Kosinski, A.S. Prosthesis-Patient Mismatch in Patients Undergoing Transcatheter Aortic Valve Replacement: From the STS/ACC TVT Registry. J. Am. Coll. Cardiol. 2018, 72, 2701–2711. [Google Scholar] [CrossRef]
- Brennan, J.M.; Holmes, D.R.; Sherwood, M.W.; Edwards, F.H.; Carroll, J.D.; Grover, F.L.; Tuzcu, E.M.; Thourani, V.; Brindis, R.G.; Shahian, D.M.; et al. The association of transcatheter aortic valve replacement availability and hospital aortic valve replacement volume and mortality in the United States. Ann. Thorac. Surg. 2014, 98, 2016–2022. [Google Scholar] [CrossRef]
- Ruparelia, N.; Latib, A.; Kawamoto, H.; Buzzatti, N.; Giannini, F.; Figini, F.; Mangieri, A.; Regazzoli, D.; Stella, S.; Sticchi, A.; et al. A Comparison Between First-Generation and Second-Generation Transcatheter Aortic Valve Implantation (TAVI) Devices: A Propensity-Matched Single-Center Experience. J. Invasive Cardiol. 2016, 28, 210–216. [Google Scholar]
- Kook, H.; Jang, D.H.; Yang, K.S.; Joo, H.J.; Park, J.H.; Hong, S.J.; Lim, D.S.; Choi, S.H.; Choi, Y.J.; Chang, K.; et al. Comparing the Procedural and Clinical Outcomes of Sapien XT and Sapien 3 Valves in Transcatheter Aortic Valve Replacement in Korean Patients. Korean Circ. J. 2020, 50, 907–922. [Google Scholar] [CrossRef]
- UK TAVI Trial Investigators; Toff, W.D.; Hildick-Smith, D.; Kovac, J.; Mullen, M.J.; Wendler, O.; Mansouri, A.; Rombach, I.; Abrams, K.R.; Conroy, S.P.; et al. Effect of Transcatheter Aortic Valve Implantation vs Surgical Aortic Valve Replacement on All-Cause Mortality in Patients with Aortic Stenosis: A Randomized Clinical Trial. JAMA 2022, 327, 1875–1887. [Google Scholar]
- Rubens, F.D.; Ngu, J.; Malvea, A.; Samuels, S.J.; Burwash, I.G. Early Midterm Results after Valve Replacement with Contemporary Pericardial Prostheses for Severe Aortic Stenosis. Ann. Thorac. Surg. 2021, 112, 99–107. [Google Scholar] [CrossRef]
- Huckaby, L.V.; Sultan, I.; Gleason, T.G.; Chen, S.; Thoma, F.; Navid, F.; Kilic, A. Outcomes of tissue versus mechanical aortic valve replacement in patients 50 to 70 years of age. J. Card. Surg. 2020, 35, 2589–2597. [Google Scholar] [CrossRef]
- Makkar, R.R.; Thourani, V.H.; Mack, M.J.; Kodali, S.K.; Kapadia, S.; Webb, J.G.; Yoon, S.H.; Trento, A.; Svensson, L.G.; Herrmann, H.C.; et al. Five-Year Outcomes of Transcatheter or Surgical Aortic-Valve Replacement. N. Engl. J. Med. 2020, 382, 799–809. [Google Scholar] [CrossRef]
- Søndergaard, L.; Ihlemann, N.; Capodanno, D.; Jørgensen, T.H.; Nissen, H.; Kjeldsen, B.J.; Chang, Y.; Steinbrüchel, D.A.; Olsen, P.S.; Petronio, A.S.; et al. Durability of Transcatheter and Surgical Bioprosthetic Aortic Valves in Patients at Lower Surgical Risk. J. Am. Coll. Cardiol. 2019, 73, 546–553. [Google Scholar] [CrossRef]
- van Rosendael, P.J.; Delgado, V.; Bax, J.J. Pacemaker implantation rate after transcatheter aortic valve implantation with early and new-generation devices: A systematic review. Eur. Heart J. 2018, 39, 2003–2013. [Google Scholar] [CrossRef]
- Sammour, Y.; Krishnaswamy, A.; Kumar, A.; Puri, R.; Tarakji, K.G.; Bazarbashi, N.; Harb, S.; Griffin, B.; Svensson, L.; Wazni, O.; et al. Incidence, Predictors, and Implications of Permanent Pacemaker Requirement after Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2021, 14, 115–134. [Google Scholar] [CrossRef]
- Pibarot, P.; Hahn, R.T.; Weissman, N.J.; Arsenault, M.; Beaudoin, J.; Bernier, M.; Dahou, A.; Khalique, O.K.; Asch, F.M.; Toubal, O.; et al. Association of Paravalvular Regurgitation with 1-Year Outcomes after Transcatheter Aortic Valve Replacement with the SAPIEN 3 Valve. JAMA Cardiol. 2017, 2, 1208–1216. [Google Scholar] [CrossRef]
- Dayan, V.; Vignolo, G.; Soca, G.; Paganini, J.J.; Brusich, D.; Pibarot, P. Predictors and Outcomes of Prosthesis-Patient Mismatch after Aortic Valve Replacement. JACC Cardiovasc. Imaging 2016, 9, 924–933. [Google Scholar] [CrossRef]
- Hernández-Vaquero, D.; Llosa, J.C.; Díaz, R.; Khalpey, Z.; Morales, C.; Álvarez, R.; López, J.; Boye, F. Impact of patient-prosthesis mismatch on 30-day outcomes in young and middle-aged patients undergoing aortic valve replacement. J. Cardiothorac. Surg. 2012, 7, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pibarot, P.; Weissman, N.J.; Stewart, W.J.; Hahn, R.T.; Lindman, B.R.; McAndrew, T.; Kodali, S.K.; Mack, M.J.; Thourani, V.H.; Miller, D.C.; et al. Incidence and sequelae of prosthesis-patient mismatch in transcatheter versus surgical valve replacement in high-risk patients with severe aortic stenosis: A PARTNER trial cohort—A analysis. J. Am. Coll. Cardiol. 2014, 64, 1323–1334. [Google Scholar] [CrossRef] [PubMed]
- Swinkels, B.M.; de Mol, B.A.; Kelder, J.C.; Vermeulen, F.E.; ten Berg, J.M. Prosthesis-Patient Mismatch after Aortic Valve Replacement: Effect on Long-Term Survival. Ann. Thorac. Surg. 2016, 101, 1388–1394. [Google Scholar] [CrossRef] [PubMed]
- Squiers, J.J.; Robinson, N.B.; Audisio, K.; Ryan, W.H.; Mack, M.J.; Rahouma, M.; Cancelli, G.; Kirov, H.; Doenst, T.; Gaudino, M.; et al. Structural valve degeneration of bioprosthetic aortic valves: A network meta-analysis. J. Thorac. Cardiovasc. Surg. 2022, S0022-5223(22)00027-7. [Google Scholar] [CrossRef] [PubMed]
- Vincent, F.; Ternacle, J.; Denimal, T.; Shen, M.; Redfors, B.; Delhaye, C.; Simonato, M.; Debry, N.; Verdier, B.; Shahim, B.; et al. Transcatheter Aortic Valve Replacement in Bicuspid Aortic Valve Stenosis. Circulation 2021, 143, 1043–1061. [Google Scholar] [CrossRef]
- Watanabe, Y.; Hayashida, K.; Takayama, M.; Mitsudo, K.; Nanto, S.; Takanashi, S.; Komiya, T.; Kuratani, T.; Tobaru, T.; Goto, T.; et al. First direct comparison of clinical outcomes between European and Asian cohorts in transcatheter aortic valve implantation: The Massy study group vs. the PREVAIL JAPAN trial. J. Cardiol. 2015, 65, 112–116. [Google Scholar] [CrossRef] [Green Version]
- Yoon, S.H.; Ohno, Y.; Araki, M.; Barbanti, M.; Lin, M.S.; Ahn, J.M.; Yang, D.H.; Kim, Y.H.; Immé, S.; Gulino, S.; et al. Comparison of aortic root anatomy and calcification distribution between Asian and Caucasian patients who underwent transcatheter aortic valve implantation. Am. J. Cardiol. 2015, 15, 1566–1573. [Google Scholar] [CrossRef]
- Nakashima, M.; Watanabe, Y.; Hioki, H.; Nara, Y.; Nagura, F.; Hosogoe, N.; Kawashima, H.; Kataoka, A.; Otsuki, S.; Konno, K.; et al. Efficacy and safety of transcatheter aortic valve implantation with Edwards SAPIEN 3 and XT in smaller Asian anatomy. Cardiovasc. Interv. Ther. 2018, 33, 384–390. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TAVR n = 1060 | SAVR n = 1060 | SMD | p-Value | |
|---|---|---|---|---|
| Age (mean ± SD) | 79.1 ± 4.8 | 78.9 ± 4.6 | 0.279 | |
| (median, IQR) * | 79, 6 | 79, 6 | 0.047 | 0.203 |
| Age categories | −0.019 | 1.000 | ||
| 65~79 | 538 (50.8) | 568 (53.4) | ||
| ≥80 | 522 (49.2) | 502 (47.4) | ||
| Female | 557 (52.5) | 557 (52.5) | 0 | 1.000 |
| Hypertension | 989 (93.3) | 990 (93.4) | 0.001 | 0.931 |
| Diabetes | 727 (68.6) | 742 (70.0) | 0.014 | 0.480 |
| COPD | 231 (21.8) | 214 (20.2) | −0.016 | 0.365 |
| CAD | 655 (61.8) | 667 (62.9) | 0.011 | 0.591 |
| Previous PCI | 69 (6.5) | 69 (6.5) | 0 | 1.000 |
| Dyslipidemia | 976 (92.1) | 981 (92.5) | 0.005 | 0.684 |
| Heart failure | 593 (55.9) | 599 (56.5) | 0.014 | 0.793 |
| AF | 187 (17.6) | 192 (18.1) | 0.005 | 0.777 |
| Previous stroke | 234 (22.1) | 224 (21.1) | −0.009 | 0.598 |
| Aortic disease | 43 (4.1) | 44 (4.2) | 0.009 | 0.913 |
| PAD | 330 (31.1) | 306 (28.9) | −0.023 | 0.255 |
| CKD | 141 (13.3) | 127 (12.0) | −0.013 | 0.360 |
| ESRD | 50 (4.7) | 46 (4.3) | −0.004 | 0.676 |
| At 1 Month | At 1 Year | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| TAVR n = 1060 | SAVR n = 1060 | HR | 95% CI | p-Value | TAVR n = 1060 | SAVR n = 1060 | HR | 95% CI | p-Value | |
| All-cause death | 34 (3.2) | 83 (7.8) | 0.40 | 0.27–0.60 | <0.001 | 93 (8.8) | 171 (16.1) | 0.55 | 0.42–0.70 | <0.001 |
| Ischemic stroke | 11 (1.0) | 11 (1.0) | 0.98 | 0.42–2.26 | 0.958 | 25 (2.4) | 35 (3.3) | 0.72 | 0.43–1.20 | 0.743 |
| ICH | 4 (0.4) | 11 (1.0) | 0.36 | 0.12–1.13 | 0.080 | 23 (2.2) | 21 (2.0) | 1.10 | 0.61–2.00 | 0.743 |
| Repeat AVR | 3 (0.3) | 1 (0.1) | 2.98 | 0.31–28.65 | 0.344 | 5 (0.5) | 3 (0.4) | 1.64 | 0.39–6.85 | 0.499 |
| PPI | 87 (8.2) | 14 (1.3) | 6.28 | 3.57–11.0 | <0.001 | 100 (9.4) | 26 (2.5) | 3.95 | 2.57–6.09 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sa, Y.K.; Hwang, B.-H.; Chung, W.-B.; Lee, K.Y.; Lee, J.; Kang, D.; Ko, Y.-G.; Yu, C.W.; Kim, J.; Choi, S.-H.; et al. Real-World Comparison of Transcatheter Versus Surgical Aortic Valve Replacement in the Era of Current-Generation Devices. J. Clin. Med. 2023, 12, 571. https://doi.org/10.3390/jcm12020571
Sa YK, Hwang B-H, Chung W-B, Lee KY, Lee J, Kang D, Ko Y-G, Yu CW, Kim J, Choi S-H, et al. Real-World Comparison of Transcatheter Versus Surgical Aortic Valve Replacement in the Era of Current-Generation Devices. Journal of Clinical Medicine. 2023; 12(2):571. https://doi.org/10.3390/jcm12020571
Chicago/Turabian StyleSa, Young Kyoung, Byung-Hee Hwang, Woo-Baek Chung, Kwan Yong Lee, Jungkuk Lee, Dongwoo Kang, Young-Guk Ko, Cheol Woong Yu, Juhan Kim, Seung-Hyuk Choi, and et al. 2023. "Real-World Comparison of Transcatheter Versus Surgical Aortic Valve Replacement in the Era of Current-Generation Devices" Journal of Clinical Medicine 12, no. 2: 571. https://doi.org/10.3390/jcm12020571