
Combined Minimally Invasive Mitral Valve Surgery and Percutaneous Coronary Intervention: A Hybrid Concept for Patients with Mitral Valve and Coronary Pathologies
 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
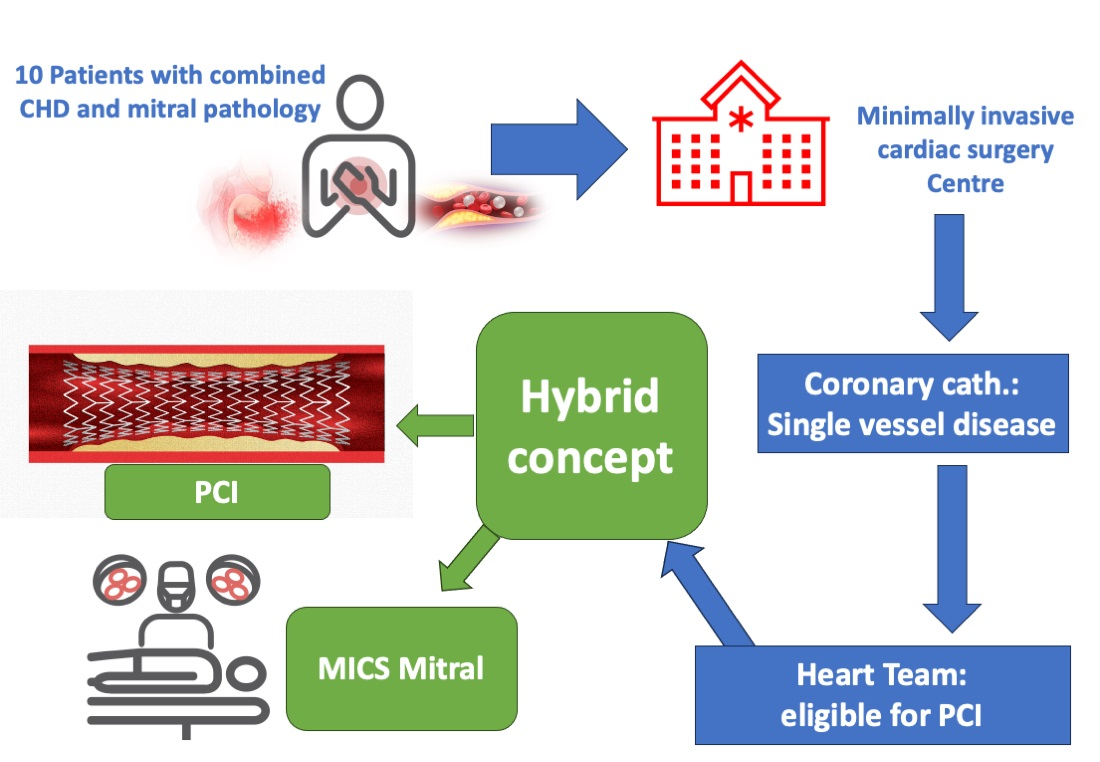
2.1. Patient Cohort
2.2. Data Collection
2.3. Statistical Analysis and Reporting
3. Results
3.1. Demographic and Medical Data
3.2. Procedural Data
3.2.1. Coronary Intervention
3.2.2. Surgical Procedure
3.3. Postoperative Data Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Speziale, G.; Nasso, G.; Esposito, G.; Conte, M.; Greco, E.; Fattouch, K.; Fiore, F.; Del Giglio, M.; Coppola, R.; Tavazzi, L. Results of mitral valve repair for Barlow disease (bileaflet prolapse) via right minithoracotomy versus conventional median sternotomy: A randomized trial. J. Thorac. Cardiovasc Surg. 2011, 142, 77–83. [Google Scholar] [CrossRef]
- Dogan, S.; Aybek, T.; Risteski, P.S.; Detho, F.; Rapp, A.; Wimmer-Greinecker, G.; Moritz, A. Minimally invasive port access versus conventional mitral valve surgery: Prospective randomized study. Ann. Thorac. Surg. 2005, 79, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Sousa-Uva, M.; Neumann, F.J.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. J. Cardio-Thoracic Surg. 2019, 55, 4–90. [Google Scholar] [CrossRef] [PubMed]
- Chitwood, R.W.; Rodriguez, E. Minimally invasive and robotic mitral valve surgery. In Cardiac Sugery in the Adult, 3rd ed.; Cohen, L.H., Ed.; McGraw-Hill: New York, NY, USA, 2008; pp. 1079–1100. [Google Scholar]
- Nasso, G.; Bonifazi, R.; Romano, V.; Bartolomucci, F.; Rosano, G.; Massari, F.; Fattouch, K.; Del Prete, G.; Riccioni, G.; Del Giglio, M.; et al. Three-year results of repaired Barlow mitral valves via right minithoracotomy versus median sternotomy in a randomized trial. Cardiology 2014, 128, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Beckmann, A.; Funkat, A.K.; Lewandowski, J.; Frie, M.; Ernst, M.; Hekmat, K.; Schiller, W.; Gummert, J.; Welz, A. German Heart Surgery Report 2015: The Annual Updated Registry of the German Society for Thoracic and Cardiovascular Surgery. Thorac. Cardiovasc Surg. 2016, 64, 462–474. [Google Scholar] [PubMed]
- Beckmann, A.; Funkat, A.K.; Lewandowski, J.; Frie, M.; Ernst, M.; Hekmat, K.; Schiller, W.; Gummert, J.; Harringer, W. German heart surgery report 2016: The annual updated registry of the German society, for thoracic and cardiovascular surgery. Thorac. Cardiovasc Surg. 2017, 65, 505–518. [Google Scholar] [PubMed]
- Beckmann, A.; Meyer, R.; Lewandowski, J.; Frie, M.; Markewitz, A.; Harringer, W. German heart surgery report 2017: The annual updated registry of the German society for thoracic and cardiovascular surgery. Thorac. Cardiovasc Surg. 2018, 66, 608–621. [Google Scholar] [PubMed]
- Beckmann, A.; Meyer, R.; Lewandowski, J.; Markewitz, A.; Harringer, W. German heart surgery report 2018: The annual updated registry of the German society for thoracic and cardiovascular surgery. Thorac. Cardiovasc Surgeon. 2019, 67, 331–344. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Muñoz, D.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2786. [Google Scholar] [CrossRef]
- Santana, O.; Xydas, S.; Williams, R.F.; Mawad, M.; Heimowitz, T.B.; Pineda, A.M.; Goldman, H.S.; Mihos, C.G. Hybrid approach of percutaneous coronary intervention followed by minimally invasive mitral valve surgery: A 5-year single-center experience. J. Thorac. Dis. 2017, 9, 595–601. [Google Scholar] [CrossRef]
- Santana, O.; Pineda, A.M.; Cortes-Bergoderi, M.; Mihos, C.G.; Beohar, N.; Lamas, G.A.; Lamelas, J. Hybrid approach of percutaneous coronary intervention followed by minimally invasive valve operations. Ann. Thorac. Surg. 2014, 97, 2049–2055. [Google Scholar] [CrossRef] [PubMed]
- Leacche, M.; Umakanthan, R.; Zhao, D.X.; Byrne, J.G. Surgical update hybrid procedures, do they have a role? Circ. Cardiovasc Interv. 2010, 3, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Mihos, C.G.; Santana, O.; Pineda, A.M.; Stone, G.W.; Hasty, F.; Beohar, N. Percutaneous coronary intervention followed by minimally invasive mitral valve surgery in ischemic mitral regurgitation. Innov. Technol. Tech. Cardio-Thorac. Vasc. Surg. 2015, 10, 394–397. [Google Scholar]
- Tomšič, A.; Schotborgh, M.A.; Manshanden, J.S.J.; Li, W.W.L.; de Mol, B.A.J.M. Coronary artery bypass grafting-related bleeding complications in patients treated with dual antiplatelet treatment. Eur. J. CardioThorac. Surg. 2016, 50, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Hansson, E.C.; Jidéus, L.; Åberg, B.; Bjursten, H.; Dreifaldt, M.; Holmgren, A.; Ivert, T.; Nozohoor, S.; Barbu, M.; Svedjeholm, R.; et al. Coronary artery bypass grafting-related bleeding complications in patients treated with ticagrelor or clopidogrel: A nationwide study. Eur. Heart J. 2016, 37, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.K.; Goodnough, L.T.; Levy, J.H.; Poston, R.S.; Short, M.A.; Weerakkody, G.J.; Lenarz, L.A. Mortality benefit with prasugrel in the TRITON-TIMI 38 coronary artery bypass grafting cohort: Risk-adjusted retrospective data analysis. J. Am. Coll. Cardiol. 2012, 60, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Held, C.; Åsenblad, N.; Bassand, J.P.; Becker, R.C.; Cannon, C.P.; Claeys, M.J.; Harrington, R.A.; Horrow, J.; Husted, S.; James, S.K.; et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes undergoing coronary artery bypass surgery results from the PLATO (Platelet Inhibition and Patient Outcomes) trial. J. Am. Coll. Cardiol. 2011, 57, 672–684. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.A.A.; Mehta, S.R.; Peters, R.; Zhao, F.; Lakkis, N.; Gersh, B.J.; Yusuf, S. ‘Benefits and risks of the combination of clopidogrel and aspirin in patients undergoing surgical revascularization for non-ST-elevation acute coronary syndrome: The Clopidogrel in Unstable angina to prevent Recurrent ischemic Events (CURE) Trial. Circulation 2004, 110, 1202–1208. [Google Scholar] [CrossRef]
- Alamanni, F.; Dainese, L.; Naliato, M.; Gregu, S.; Agrifoglio, M.; Polvani, G.L.; Biglioli, P.; Parolari, A.; Monzino OPCAB Investigators. On- and off-pump coronary surgery and perioperative myocardial infarction: An issue between incomplete and extensive revascularization. Eur. J. Cardio-Thorac. Surg. 2008, 34, 118–126. [Google Scholar] [CrossRef]
- Leviner, D.B.; Torregrossa, G.; Puskas, J.D. Incomplete revascularization: What the surgeon needs to know. Ann. Cardio-Thorac. Surg. 2018, 7, 463–469. [Google Scholar]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS. Eur. J. Cardio-Thorac. Surg. 2018, 53, 34–78. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | Result |
|---|---|
| Demographic data | |
| Age, years (IQR) | 75 (64–81) |
| Males, n | 7 |
| Body mass index, kg/m2 (IQR) | 29.4 (23.7–31.6) |
| Risk factors | |
| Arterial hypertension, n | 9 |
| Diabetes mellitus, n | 3 |
| Hyperlipidemia, n | 7 |
| History of smoking, n | 1 |
| Renal insufficiency, n | 4 |
| Previous cardiac surgery, n | 2 |
| EuroSCORE II, % (IQR) | 8.1 (2.5–8.6) |
| STS score, % (IQR) | 1.2 (0.7–3.1) |
| Cardiac data | |
| NYHA class, median | 3 |
| Mitral valve insufficiency, n | 10 |
| Ejection fraction, % (IQR) | 60 (40–60) |
| Tricuspid valve insufficiency, n | 1 |
| Pulmonary hypertension >60 mmHg, n | 0 |
| History of myocardial infarction, n | 4 |
| Atrial fibrillation, n | 3 |
| Pacemaker/AICD, n | 1 |
| Coronary data | |
| Previously operated patients | |
| Patient No.1 CABG | LIMA to D1 and LAD, RIMA-T to M1, intact grafts |
| Patient No.2 CABG | LIMA to LAD, RIMA-T to M1, intact grafts |
| RCA as Target vessel for PCI | both patients |
| Previously non-operated patients | |
| RCA as Target vessel for PCI, n | 1 |
| LAD as Target vessel for PCI, n | 3 |
| D1 as Target vessel for PCI, n | 1 |
| RCX as Target vessel for PCI, n | 3 |
| Patient No. | Preop. EF | Mitral Valve Pathology |
|---|---|---|
| 1 | 60% | Mixed regurgitation due to atrial remodeling due to
|
| 2 | 60% | Mixed regurgitation due to
|
| 3 | 50% | Primary regurgitation due to P3 flail due to P3 chordal rupture |
| 4 | 37% | Secondary regurgitation due to PML restriction due to LV remodeling and ICM |
| 5 | 40% | Secondary regurgitation due to PML restriction due to LV remodeling and ICM |
| 6 | 59% | Secondary regurgitation due to atrial remodeling due to long persistent atrial fibrillation (Carpentier type I) |
| 7 | 30% | Secondary regurgitation due to AML restriction due to LV remodeling and ICM |
| 8 | 60 | Primary regurgitation due to P2 flail due to P2 chordal rupture |
| 9 | 60 | Primary regurgitation due to P2 flail due to P2 chordal rupture |
| 10 | 60 | Primary regurgitation due to Barlow disease with bileaflet billowing and pronounced P2 prolapse due to chordal elongation |
| Patient No. | PCI before or after Surgery | Time Span (Days) | Target Vessel | Number of Stents | Stent Type |
|---|---|---|---|---|---|
| 1 | Before | 17 | LAD Segment 6 | 1 | 80% proximal to DES → BMS (coroflex Blue 3.0/14 proximal to DES) |
| 2 | Before | 8 | RCA Segment 3 | 1 | BMS (Coroflex Blue Ultra 2.5/14) |
| 3 | Before | 21 | D1 Segment 9 | 1 | DES Coroflex ISAER 2.5/14 |
| 4 | Before | 63 | RCA multiple segments | 2 | Segment 1: POBA 4.0 Balloon 10 bar due to previous stent stenosis Segment 2: DES Coroflex ISAR 4.0/15 Segment 3 DES Coroflex ISAR 2.75/19 |
| 5 | Before | 66 | RCX segment 12 | 1 | DES (Xience pro 2.75/12) |
| 6 | Before | 62 | RCX segment 13 | 1 | DES (Coroflex ISAR 3.0/19) |
| 7 | Before | 61 | LAD segment 6 | 1 | DES (Coroflex ISAR 3.0/14) |
| 9 | After | 48 | RCA segment 2 | 1 | BMS (Coroflex Blue 4.0/25) |
| 10 | Before | 7 | RCX segment 13 | 2 | 2x BMS (2x Coroflex 2.5/9) |
| 11 | Before | 3 | LAD segment 7 | 1 | BMS (Coroflex 3.0/25) |
| Patient No | Redo Surgery | Beating Heart Surgery | Surgery on DAPT | Surgery | Repair Technique |
|---|---|---|---|---|---|
| 1 | No | No | No | MV repair | 32 mm Ring, A2–A3 plication |
| 2 | No | No | Yes | MV repair, Cryoablation | 32 mm Ring, A1–P1 edge-to-edge stitch, P1–P2 indentation closure |
| 3 | No | No | Yes | MV repair, Cryoablation | 32 mm Ring, P2 triangular resection |
| 4 | Yes | Yes | Yes | MV repair | 36 mm Ring |
| 5 | No | Yes | Yes | MV repair | 30 mm Ring |
| 6 | No | No | Yes | MV and TV repair, Cryoablation | 28 mm Ring, 34 mm tricuspid band |
| 7 | No | No | Yes | MV repair | 32 mm Ring |
| 9 | Yes | No | No | MV repair | 30 mm Ring, P2 triangular resection |
| 10 | No | No | Yes | MV repair, PFO–closure | 34 mm Ring, P2 triangular resection |
| 11 | No | No | Yes | MV repair | 32 mm Ring, P2 triangular resection |
| Variable | Result |
|---|---|
| Postoperative myocardial infarction | 0 |
| Postoperative stroke | 0 |
| Postoperative delirium, n | 2 |
| Drain volume, mL (IQR) | 1100 (850–1450) |
| Re-thoracotomy for bleeding, n | 1 |
| Perioperative blood transfusion, n | 1 |
| Postoperative blood transfusion, n | 5 |
| Ventilation time, hours (IQR) | 10 (14–24) |
| ICU time, days (IQR) | 3 (2–4) |
| Hospital stay, days (IQR) | 8 (8–11) |
| 30-day survival rate, % | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moscoso-Ludueña, M.; Vondran, M.; Irqsusi, M.; Nef, H.; Rastan, A.J.; Ghazy, T. Combined Minimally Invasive Mitral Valve Surgery and Percutaneous Coronary Intervention: A Hybrid Concept for Patients with Mitral Valve and Coronary Pathologies. J. Clin. Med. 2023, 12, 5553. https://doi.org/10.3390/jcm12175553
Moscoso-Ludueña M, Vondran M, Irqsusi M, Nef H, Rastan AJ, Ghazy T. Combined Minimally Invasive Mitral Valve Surgery and Percutaneous Coronary Intervention: A Hybrid Concept for Patients with Mitral Valve and Coronary Pathologies. Journal of Clinical Medicine. 2023; 12(17):5553. https://doi.org/10.3390/jcm12175553
Chicago/Turabian StyleMoscoso-Ludueña, Martín, Maximilian Vondran, Marc Irqsusi, Holger Nef, Ardawan J. Rastan, and Tamer Ghazy. 2023. "Combined Minimally Invasive Mitral Valve Surgery and Percutaneous Coronary Intervention: A Hybrid Concept for Patients with Mitral Valve and Coronary Pathologies" Journal of Clinical Medicine 12, no. 17: 5553. https://doi.org/10.3390/jcm12175553