
Radiomics and Artificial Intelligence for the Diagnosis and Monitoring of Alzheimer’s Disease: A Systematic Review of Studies in the Field
 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
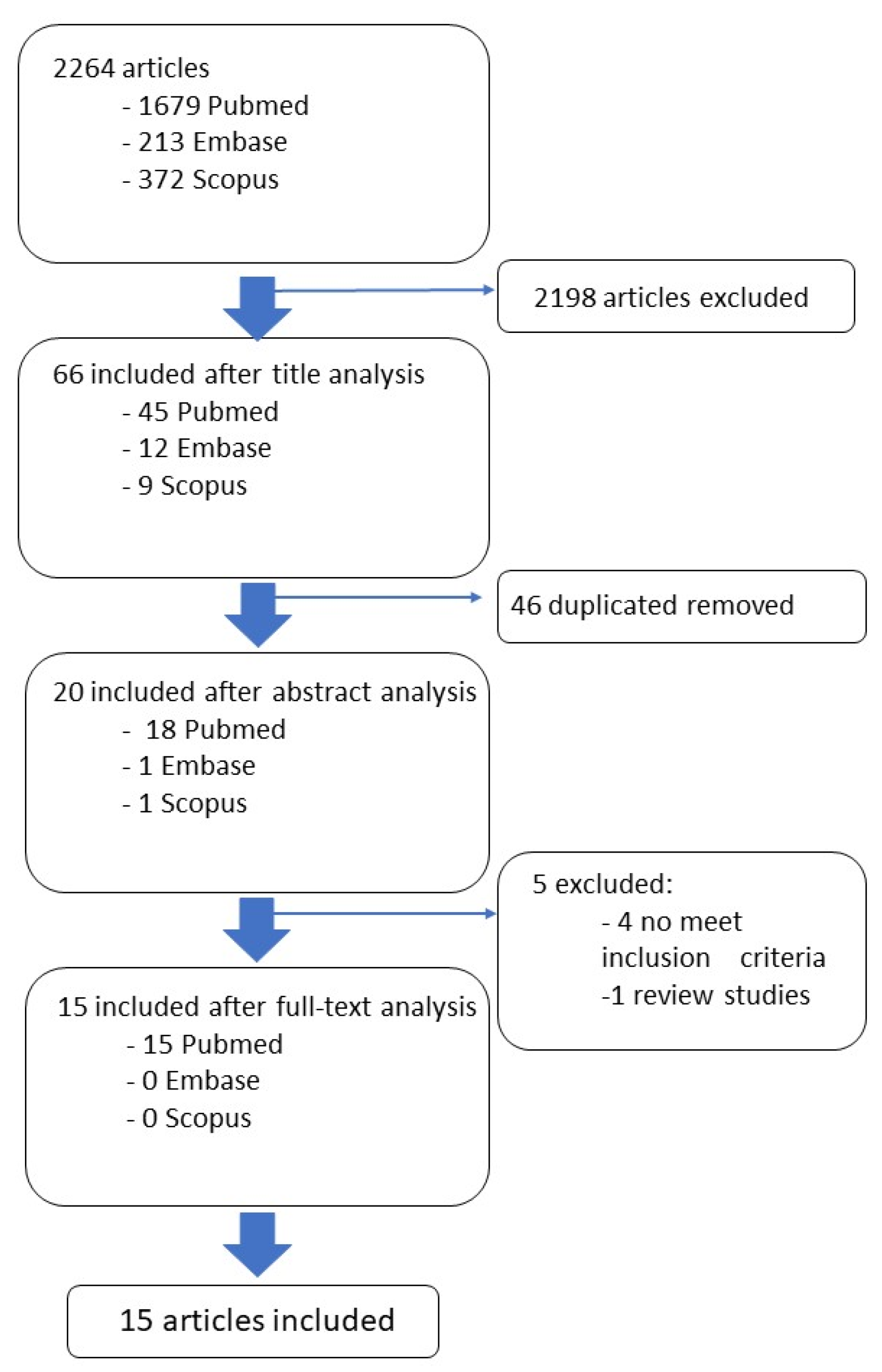
2.1. Literature Search and Study Selection
2.2. Data Collection
3. Results
3.1. Study Quality Evaluation
3.2. General Characteristics of the Study Population
3.3. Radiomic Features
3.4. Machine and Deep Learning Methods Applied to the Diagnosis of AD
3.5. Performance Metrics
3.6. Differential Diagnosis
3.7. Brain Regions and Classification Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef]
- Castiglioni, I.; Rundo, L.; Codari, M.; Di Leo, G.; Salvatore, C.; Interlenghi, M.; Gallivanone, F.; Cozzi, A.; D’Amico, N.C.; Sardanelli, F. AI applications to medical images: From machine learning to deep learning. Phys. Med. 2021, 83, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.; Limkin, E.J.; Vakalopoulou, M.; Dercle, L.; Champiat, S.; Han, S.R.; Verlingue, L.; Brandao, D.; Lancia, A.; Ammari, S.; et al. A radiomics approach to assess tumour-infiltrating CD8 cells and response to anti-PD-1 or anti-PD-L1 immunotherapy: An imaging biomarker, retrospective multicohort study. Lancet Oncol. 2018, 19, 1180–1191. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.; Wang, Y.; Wang, Y.; Jiang, S.; Fan, R.; Zhang, H.; Jiang, W. Application of radiomics and machine learning in head and neck cancers. Int. J. Biol. Sci. 2021, 17, 475–486. [Google Scholar] [CrossRef]
- Chetan, M.R.; Gleeson, F.V. Radiomics in predicting treatment response in non-small-cell lung cancer: Current status, challenges and future perspectives. Eur. Radiol. 2021, 31, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Wang, S.; Dong, D.; Wei, J.; Fang, C.; Zhou, X.; Sun, K.; Li, L.; Li, B.; Wang, M.; et al. The Applications of Radiomics in Precision Diagnosis and Treatment of Oncology: Opportunities and Challenges. Theranostics 2019, 9, 1303–1322. [Google Scholar] [CrossRef] [PubMed]
- Kohavi, R. Wrappers for Performance Enhancement and Obvious Decision Graphs. Ph.D. Thesis, Stanford University, Computer Science Department, Stanford, CA, USA, 1995. [Google Scholar]
- Harding-Theobald, E.; Louissaint, J.; Maraj, B.; Cuaresma, E.; Townsend, W.; Mendiratta-Lala, M.; Singal, A.G.; Su, G.L.; Lok, A.S.; Parikh, N.D. Systematic review: Radiomics for the diagnosis and prognosis of hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2021, 54, 890–901. [Google Scholar] [CrossRef] [PubMed]
- Ligero, M.; Garcia-Ruiz, A.; Viaplana, C.; Villacampa, G.; Raciti, M.V.; Landa, J.; Matos, I.; Martin-Liberal, J.; Ochoa-de-Olza, M.; Hierro, C.; et al. A CT-based Radiomics Signature Is Associated with Response to Immune Checkpoint Inhibitors in Advanced Solid Tumors. Radiology 2021, 299, 109–119. [Google Scholar] [CrossRef]
- Wang, T.; She, Y.; Yang, Y.; Liu, X.; Chen, S.; Zhong, Y.; Deng, J.; Zhao, M.; Sun, X.; Xie, D.; et al. Radiomics for Survival Risk Stratification of Clinical and Pathologic Stage IA Pure-Solid Non-Small Cell Lung Cancer. Radiology 2022, 302, 425–434. [Google Scholar] [CrossRef]
- Yip, S.S.; Kim, J.; Coroller, T.P.; Parmar, C.; Velazquez, E.R.; Huynh, E.; Mak, R.H.; Aerts, H.J. Associations Between Somatic Mutations and Metabolic Imaging Phenotypes in Non-Small Cell Lung Cancer. J. Nucl. Med. 2017, 58, 569–576. [Google Scholar] [CrossRef]
- Salvatore, C.; Castiglioni, I.; Cerasa, A. Radiomics Approach in the Neurodegenerative Brain. Aging Clin. Exp. Res. 2021, 33, 1709–1711. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Ding, Z. MRI Radiomics Classification and Prediction in Alzheimer’s Disease and Mild Cognitive Impairment: A Review. Curr. Alzheimer Res. 2020, 17, 297–309. [Google Scholar] [CrossRef] [PubMed]
- Nardone, V.; Reginelli, A.; Grassi, R.; Boldrini, L.; Vacca, G.; D’Ippolito, E.; Annunziata, S.; Farchione, A.; Belfiore, M.P.; Desideri, I.; et al. Delta radiomics: A systematic review. Radiol. Med. 2021, 126, 1571–1583. [Google Scholar] [CrossRef]
- Sotoudeh, H.; Sarrami, A.H.; Roberson, G.H.; Shafaat, O.; Sadaatpour, Z.; Rezaei, A.; Choudhary, G.; Singhal, A.; Sotoudeh, E.; Tanwar, M. Emerging Applications of Radiomics in Neurological Disorders: A Review. Cureus 2021, 13, e20080. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 5 February 2023).
- Wu, G.; Jochems, A.; Refaee, T.; Ibrahim, A.; Yan, C.; Sanduleanu, S.; Woodruff, H.C.; Lambin, P. Structural and functional radiomics for lung cancer. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3961–3974. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Song, Q.; Wang, M.; Pang, P.; Liao, Z.; Jiang, H.; Ding, Z. Hippocampus radiomic biomarkers for the diagnosis of amnestic mild cognitive impairment: A machine learning method. Front. Aging Neurosci. 2019, 11, 323. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Zhang, Y.; Li, H.; Tong, X.; Ouyang, M. How segmentation methods affect hippocampal radiomic feature accuracy in Alzheimer’s disease analysis? Eur. Radiol. 2022, 32, 6965–6976. [Google Scholar] [CrossRef]
- Chaddad, A.; Toews, M.; Desrosiers, C.; Niazi, T. Deep radiomic analysis based on modeling information flow in convolutional neural networks. IEEE Access 2019, 7, 97242–97252. [Google Scholar] [CrossRef]
- Chaddad, A.; Desrosiers, C.; Niazi, T. Deep radiomic analysis of MRI related to Alzheimer’s disease. IEEE Access 2018, 6, 58213–58221. [Google Scholar] [CrossRef]
- Du, Y.; Zhang, S.; Fang, Y.; Qiu, Q.; Zhao, L.; Wei, W.; Tang, Y.; Li, X. Radiomic Features of the Hippocampus for Diagnosing Early-Onset and Late-Onset Alzheimer’s Disease. Front. Aging Neurosci. 2022, 13, 1014. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.P.; Kim, J.; Jang, H.; Kim, J.; Kang, S.H.; Kim, J.S.; Lee, J.; Na, D.L.; Kim, H.J.; Seo, S.W. Predicting amyloid positivity in patients with mild cognitive impairment using a radiomics approach. Sci. Rep. 2021, 11, 6954. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Niu, J.; Wang, L.; Pang, P.; Wang, M.; Liao, Z.; Song, Q.; Jiang, H.; Ding, Z. Comprehensive classification models based on amygdala radiomic features for Alzheimer’s disease and mild cognitive impairment. Brain Imaging Behav. 2021, 15, 2377–2386. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Chen, Y.; Liao, Z.; Jiang, H.; Mao, D.; Wang, M.; Yu, E.; Ding, Z. Corpus callosum radiomics-based classification model in Alzheimer’s disease: A case-control study. Front. Neurol. 2018, 9, 618. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Jie, C.; Zheng, W.; Cui, J.; Wang, Z. Investigation of underlying association between whole brain regions and alzheimer’s disease: A research based on an artificial intelligence model. Front. Aging Neurosci. 2022, 14, 872530. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Jiang, J.; Shen, T.; Wu, P.; Zuo, C. Radiomics features as predictors to distinguish fast and slow progression of Mild Cognitive Impairment to Alzheimer’s disease. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 17–21 July 2018; IEEE: Piscataway, NJ, USA; 2018; pp. 127–130. [Google Scholar]
- Zhao, K.; Ding, Y.; Han, Y.; Fan, Y.; Alexander-Bloch, A.F.; Han, T.; Jin, D.; Liu, B.; Lu, J.; Song, C.; et al. Independent and reproducible hippocampal radiomic biomarkers for multisite Alzheimer’s disease: Diagnosis, longitudinal progress and biological basis. Sci. Bull. 2020, 65, 1103–1113. [Google Scholar] [CrossRef]
- Wu, Y.; Li, T.; Han, Y.; Jiang, J. Use of radiomic features and support vector machine to discriminate subjective cognitive decline and healthy controls. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; IEEE: Piscataway, NJ, USA; 2020; pp. 1762–1765. [Google Scholar]
- Ding, Y.; Zhao, K.; Che, T.; Du, K.; Sun, H.; Liu, S.; Zheng, Y.; Li, S.; Liu, B.; Liu, Y.; et al. Quantitative radiomic features as new biomarkers for Alzheimer’s disease: An amyloid PET study. Cereb. Cortex 2021, 31, 3950–3961. [Google Scholar] [CrossRef]
- Feng, F.; Wang, P.; Zhao, K.; Zhou, B.; Yao, H.; Meng, Q.; Wang, L.; Zhang, Z.; Ding, Y.; Wang, L. Radiomic features of hippocampal subregions in Alzheimer’s disease and amnestic mild cognitive impairment. Front. Aging Neurosci. 2018, 10, 290. [Google Scholar] [CrossRef]
- Jiang, J.; Zhang, J.; Li, Z.; Li, L.; Huang, B.; Alzheimer’s Disease Neuroimaging Initiative. Using Deep Learning Radiomics to Distinguish Cognitively Normal Adults at Risk of Alzheimer’s Disease from Normal Control: An Exploratory Study Based on Structural MRI. Front. Med. 2022, 9, 894726. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Ayodele, T.; Rogaeva, E.; Kurup, J.T.; Beecham, G.; Reitz, C. Earlyonset Alzheimer’s disease: What is missing in research? Curr. Neurol. Neurosci. Rep. 2021, 21, 4. [Google Scholar] [CrossRef] [PubMed]
- Cacace, R.; Sleegers, K.; Van Broeckhoven, C. Molecular geneticsof early-onset Alzheimer’s disease revisited. Alzheimers Dement. 2016, 12, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Hampel, H.; Molinuevo, J.L.; Blennow, K.; DeKosky, S.T.; Gauthier, S.; Selkoe, D.; Bateman, R.; et al. Advancing research diagnostic criteria for Alzheimer’s disease: The IWG-2 criteria. Lancet Neurol. 2014, 13, 614–629. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]

{kind=link}
| Order of Search | Terms |
|---|---|
| 1 | Elderly AND Radiomics AND Alzheimer |
| 2 | Radiomics AND Elderly AND Cognitive impairment |
| 3 | Texture analysis AND Elderly AND Cognitive impairment |
| 4 | Radiomics AND Elderly AND Neurological status |
| 5 | Radiomics AND Elderly AND Frailty |
| 6 | Radiomics AND Sarcopenia |
| Selection | Comparability | Outcome | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | Adequate Case Definition | Representativeness of the Cases | Selection of Controls | Definition of Controls | Main Factor | Additional Factor | Ascertainment of Exposure | Same Ascertainment for Cases and Controls | Non-Response Rate | Total (9/9) |
| Feng et al. [19] | * | * | * | * | * | 0 | * | * | * | 8 |
| Zheng et al. [20] | * | * | * | * | * | 0 | * | * | 0 | 7 |
| Chaddad et al. [21] | * | * | 0 | * | * | 0 | * | * | 0 | 6 |
| Chaddad et al. [22] | * | * | 0 | * | * | 0 | * | * | 0 | 6 |
| Du et al. [23] | * | * | * | * | * | * | * | * | * | 9 |
| Kim et al. [24] | * | * | * | * | * | 0 | * | * | * | 8 |
| Feng et al. [25] | * | * | * | * | * | 0 | * | * | * | 8 |
| Feng et al. [26] | * | * | * | * | * | * | * | * | 0 | 8 |
| Liu et al. [27] | * | * | * | * | * | * | * | * | * | 9 |
| Li et al. [28] | * | * | * | 0 | * | 0 | * | * | 0 | 5 |
| Zhao et al. [29] | * | * | * | 0 | * | 0 | 0 | * | * | 6 |
| Wu et al. [30] | * | * | 0 | 0 | * | 0 | * | * | 0 | 6 |
| Ding et al. [31] | * | * | * | * | * | 0 | * | * | * | 8 |
| Feng et al. [32] | * | * | * | * | * | 0 | * | * | * | 8 |
| Jiang et al. [33] | * | * | * | 0 | * | 0 | * | * | * | 7 |
| Study | State/Condition of Disease | Imaging Method | Imaging Evaluation | AI Algorithm | Performance Measures |
|---|---|---|---|---|---|
| Feng et al. [19] | Amnestic mild cognitive impairment | Magnetic resonance | Segmentation and feature extraction with LASSO | Logistic regression | AUC, sensitivity, specificity, precision, recall, F1-score |
| Zheng et al. [20] | Mild cognitive impairment | Magnetic resonance | Segmentation and HRF feature extraction | Support vector machine | AUC, accuracy |
| Chaddad et al. [21] | Alzheimer disease | Magnetic resonance | Entropy feature extraction | Convolutional neural network, random forest | AUC |
| Chaddad et al. [22] | Alzheimer disease | Magnetic resonance | CNN-derived feature extraction | Convolutional neural network, random forest | AUC |
| Du et al. [23] | Early and late onset of Alzheimer disease | Magnetic resonance | Segmentation and feature extraction | Support vector machine | AUC, accuracy |
| Kim et al. [24] | Amyloyd-positive and -negative | Magnetic resonance | Segmentation and feature extraction | - | AUC, sensitivity, specificity |
| Feng et al. [25] | Mild cognitive impairment | Magnetic resonance | Segmentation and feature extraction | Logistic regression | AUC, Accuracy |
| Feng et al. [26] | Alzheimer disease | Magnetic resonance | Segmentation and feature extraction | Logistic regression | AUC, accuracy, sensitivity, specificity, precision, |
| Liu et al. [27] | Alzheimer disease | Magnetic resonance | Segmentation and feature extraction | Logistic regression, K Nearest Neighbor, Support vector machine | Accuracy |
| Li et al. [28] | Mild cognitive impairment, Alzheimer disease | Magnetic resonance | Segmentation and feature extraction | Support vector machine | Accuracy |
| Zhao et al. [29] | Mild cognitive impairment | Magnetic resonance | Segmentation and feature extraction | Support vector machine, linear discriminant analysis | AUC, accuracy, sensitivity, specificity |
| Wu et al. [30] | Subjective cognitive decline | Magnetic resonance | Segmentation and feature extraction | Support vector machine, random forest | AUC, accuracy, sensitivity, specificity |
| Ding et al. [31] | Mild cognitive impairment, Alzheimer disease | Positron emission tomography | Feature extraction | Support vector machine | AUC |
| Feng et al. [32] | Mild cognitive impairment | Magnetic resonance | Segmentation and feature extraction | Support vector machine | AUC, accuracy, sensitivity, specificity |
| Jiang et al. [33] | Alzheimer disease | Magnetic resonance | Derived feature extraction | Convolutional neural network, support vector machine | AUC, accuracy, sensitivity, specificity |
| Population | Methods | Aim of the Study | Results | ||
|---|---|---|---|---|---|
| Participants in AD Groups | Participants in the HC Group | ||||
| Feng Qi [19] | n = 42 older adults, 18 M/24 F, Age 64.17 ± 10.57 years | n = 44 older adults, 20 M/24 F, Age 65.43 ± 9.70 years | After the segmentation of the left and right hippocampus, features are extracted and selected using LASSO to build two classification models based on logistic regression.
| Primary: to identify the radiomic biomarkers of the hippocampus for building the classification models in SCD/AD diagnosis. | The study reports ML classification results divided between the left and right hippocampus: AUC (L/R): 0.79/0.76 Sensitivity: (L/R) 0.54/0.69 Specificity: (L/R) 0.71/0.71 Precision: (L/R) 0.64/0.69 Recall(L/R): 0.54/0.69 F1-score (L/R): 0.58/0.69 |
| Zheng et al. [20] | n = 283 older adults, 152 M/131 F, Age 74.91 ± 7.70 years | MCI group n = 764 older adults, 447 M/317 F, Age 72.96 ± 7.70 years HC group n = 603 older adults, 277 M/326 F, Age 73.46 ± 6.17 | After calculating the HRFs of the intensity, shape and textural features from each side of the hippocampus in MRI, the consistency of the HRFs calculated from seven different hippocampal segmentation methods was validated, as well as the performance of the machine learning–based classification of AD vs. HC.
| Primary: identification of the optimal segmentation methods. Secondary: discrimination of AD among HC. | Regarding the classification of AD and MCI, the bilateral HRFs exhibited acceptable results for all of the involved segmentation. AUC: 0.88 Accuracy: 83.9% |
| Chaddad et al. [21] | n = 100 older adults, Age > 60 | n = 98 older adults, Age > 60 | Once the images are pre-processed, a convolution and a max pooling allow for the extraction of conditional entropy features. Such features are used to train and test a 100-trees random forest algorithm and a CNN to distinguish between AD and HC.
| Primary: The goal of this experiment is to classify between AD and HG subjects from MRI data. | The highest overall accuracy, 93.6%, is obtained from an RF classifier combining the three conditional entropy features. |
| Chaddad et al. [22] | n = 100 older adults, 41 M/59 F, Age 77 years | n = 135 older adults, 38 M/97 F, Age 71 years | MRI volumes are first processed to label subcortical areas from which radiomics features are extracted. A significance test is performed to identify features that show significant differences between AD and HC. Novel CNN-derived radiomic features based on the entropy are proposed to improve classification. These features are then used as the input to an RF model to classify AD and HG subjects.
| Primary: Propose a novel technique, based on the entropy of convolutional feature maps, to characterize the local texture in a data-driven manner and to classify AD from HG through CNN. | Among subcortical regions, the hippocampus (AUC 81.19–84.09%) and amygdala (AUC 79.70–80.27%) regions have the greatest discriminative power. Entropy features derived from CNN show an AUC of 0.925 in discriminating AD from HG after testing RF. |
| Du et al. [23] | n = 72 older adults, 35 M/37 F, Age 66.12 ± 2.8 years | n = 78 older adults, 36 M/42 F, Age 70.6 ± 7.5 years | Hippocampal segmentation and feature extraction were performed; the LASSO method was used to select radiomic features. SVM models were constructed based on the identified features to distinguish early onset AD from young control subjects, late onset AD from old control subjects and early onset AD from late onset AD subjects.
| Primary: build and validate radiomics models of the hippocampus for early onset AD and young controls, late onset AD and old controls and early onset AD and late onset AD. | SVM models have good performances. Early onset AD and HG AUC: 0.90 Accuracy: 77% Late onset AD and HG AUC: 0.94 Accuracy: 86% Early onset and late onset AUC: 0.87 Accuracy: 79% |
| Kim et al. [24] | Amyloid-positive older adults n = 166, 70 M/96 F, Age 71.9 ± 8.1 years | Amyloid-negative older adultsn = 182, 78 M 104 F, Age 70.9 ± 8.6 years | After multimodal MRI images were pre-processed, the brain region of interest was segmented, and radiomic features were extracted from each. Once radiomic features are selected through LASSO, the remaining features were used alone or in combination with baseline non-imaging predictors such as age, sex and ApoE genotype to predict amyloid positivity.
| Primary: Predicting amyloid positivity in patients with MCI. Secondary: compared the predictive value of a radiomics model with those of cortical thickness and non-imaging predictors | Amyloid positivity was predicted a using non-imaging model (a model based on features not derived from MRI) that had an AUC = 0.71. Among single MR-sequence models, T1 MRI showed an AUC of 0.71, and T2 MRI showed an AUC of 0.74. When T1 and T2 radiomics features were combined, the AUC for the test was 0.75 |
| Feng Q. et al. [25] | n = 41 older adults, 16 M/25 F, Age 76.1 ± 8.7 years | MCI group n = 60 older adults, 43 M/17 F, Age 76 ± 8.4 years HC group n = 72 older adults, 26 M/46 F, Age 75.2 ± 4.7 | Once images are pre-processed and segmented, radiomics features are extracted, and LASSO is used to reduce and select the features. Multivariate LR analysis was performed to build classification models followed by an internal validation.
| Primary: build and validate comprehensive classification models based on amygdala radiomic features to discriminate AD, MCI and NC | LR analysis based on amygdala radiomic features achieves good performance for clinical applications among AD, SCD and HC groups. Accuracy AD vs. HG: 90% Accuracy AD vs. SCD: 81% Accuracy SCD vs. HG: 75% |
| Feng Q. et al. [26] | n = 78 older adults, 25 M/53 F, Age 69.18 ± 12.23 years | n = 44 older adults, 20 M/24 F, Age 65.43 ± 9.70 years | After manual segmentation, features are extracted from the region of interest and selected using LASSO. The logistic regression method is then applied to establish a classificationmodel for AD diagnosis.
| Primary: identify the CC radiomic features related to the diagnosis of AD and build and evaluate a classification model from NC. | Eleven features were selected from the using the LASSO model. Discrimination of AD from NC: AUC: 0.720 Sensitivity: 79.2% Specificity: 50.0% Accuracy: 68.4% Precision: 73.1% PPV: 73.1% NPV: 58.3% |
| Liu et al. [27] | n = 80 older adults, 42 M/38 F, Age 65 | n = 80 older adults, 40 M/40 F, Age 64 | For each patient, MRI images were segmented into 106 subregions, and radiomic features were extracted from each. Then, an analysis is conducted of radiomic features of specific brain subregions that were most related to AD. Based on the selective radiomic features from specific brain subregions, they built an integrated model using the best machine learning algorithm.
| Primary: exploring optimal brain regions for AD radiomics diagnosis. Secondary: Evaluate the optimal ML algorithm to discriminate AD from HG. | The subregions most relevant to AD included the hippocampus, the inferior parietal lobe, the precuneus and the lateral occipital gyrus. Accuracy LR: 96.2% Accuracy KNN: 95.0% Accuracy SVM: 95.0% |
| Li et al. [28] | n = 165 older adults, 103 M/62 F, Age 75.3 ± 6.3 years | n = 32 older adults, 13 M/19 F, Age 76.2 ± 6.8 years | After segmentation, normalization and smoothing, radiomics features are extracted from MR images and selected through statistical analysis (Cox regression and t-test). The classification phase was accomplished using SVM models with three different linear, polynomial and sigmoid kernels
| Primary: prove that radiomics features could be used to identify the fast and slow conversion from MCI to AD based on MRI images. | Classification accuracy using linear, polynomial and sigmoid kernels could achieve good discrimination in distinguishing MCI-to-AD fast and slow conversion. In particular, in terms of accuracy, SVM with a polynomial kernel shows the best results. Accuracy linear: 80.0%, Accuracy polynomial: 93.3% Accuracy sigmoid: 86.6% |
| Zhao et al. [29] | n = 583 older adults, 268 M/315 F, Age 69.74 ± 8.14 years | MCI group n = 773 older adults, 429 M/344 F, Age 69.85 ± 8.31 years HC group n = 587 older adults, 268 M/319 F, Age 67.87 ± 6.82 | After the automatic segmentation of the hippocampal region, intensity-based features, shape-based features and texture-based features across eight wavelet-based frequency domains are extracted. The SVM model is built to classify the AD patients and NC.
| Primary: verify if hippocampal region features can serve as robust MRI markers for AD. Secondary: Diagnose AD through ML. | Multivariate classifier-based SVM analysis provided individual-level predictions for distinguishing AD patients HC with an accuracy of 88.21% and inter-site cross validation. |
| Wu et al. [30] | SCD group n = 103 older adults, 71 M/32 F, Age 68.4 ± 6.60 years | n = 132 older adults, 85 M/47 F, Age 67.23 ± 6.41 years | After brain sMRI segmentation and feature extraction, the t-test, autocorrelation, and Fisher score were performed for selecting the most relevant features. SVM was implemented to build a classification model, and a random forest (RF) was used as a comparison model.
| Primary: propose a radiomic approach to detect neuropathological features in subjective cognitive decline (a high-risk preclinical stage in the progress of AD) subjects based on MRI images. | SVM showed good results in the classification of SCD from HC. Accuracy: 84.7% Sensitivity: 86.9% Specificity: 82.6% |
| Ding et al. [31] | n = 291 older adults, 173 M/118 F, Age 74.69 ± 7.26 years | MCI group n = 453 older adults, 272 M/181 F, Age 73.51 ± 6.64 years HC group n = 334 older adults, 167 M/167 F, Age 73.78 ± 6.01 years | After extraction of radiomics features and group difference statistical analysis, a nonlinear SVM model with a radial basis function kernel was adopted to predict over AD cases. Feature selection was introduced by combining the t-test and SVM-RFE.
| Primary: explore whether the radiomic features of PET images are used as predictors and provide a neurobiological foundation for AD. Secondary: Diagnose AD through ML | The results showed a high accuracy in distinguishing AD from HC and predicting the MCI conversion to AD. The classification outputs were found to be significantly associated with clinical measures like the apolipoprotein E genotype. AUC AD from HC: 0.93 AUC MCI to AD: 0.83 |
| Feng et al. [32] | n = 38 older adults, 16 M/22 F, Age 71.7 ± 8.3 years | MCI group n = 33 older adults, 14 M/19 F, Age 70.6 ± 8.2 years HC group n = 45 older adults, 22 M/23 F, Age 68.2 ± 6.9 years | Region of interest is extracted after the segmentation of MR scans. Features are extracted and selected to combine the spatial and frequency characteristics. ANOVA was employed to evaluate the differences between the AD, SCD and HCgroups, and Spearman’s correlation coefficient was calculated to evaluate the relationships between the features and MMSE. The SVM model is built to perform a classification task.
| Primary: test whether radiomic features in the hippocampus can be employed for the early classification of AD and SCD. Secondary: Distinguish AD from HC through ML. | The SVM model demonstrated that radiomic features allowed for distinguishing AD from HC with a satisfying performance. AUC: 0.93 Accuracy: 86.75% Specificity: 88.89% Sensitivity: 84.21% |
| Jiang et al. [33] | n = 181 older adults, 73 M/108 F, Age 76.3 ± 5.4 years | n = 228 older adults, 112 M/116 F, Age 71.8 ± 5.7 years | Once the MRI image is pre-processed, a basic DLR model pre-training is carried out through CNN. To obtain DLR features, global max pooling is used to extract the maximum value of each feature map (last convolutional layer of the DL model). Based on the above extracted features, SVM is used to distinguish AD from HC.
| Primary: propose a novel deep learning radiomics method for distinguishing cognitively normal adults at risk of AD from NC. | The DLR method achieved the best classification performance between AD and HC compared to other models (hippocampal/traditional radiomics/clinical): AUC: 0.904 Accuracy: 92.8% Sensitivity: 88.8% Specificity: 94.4% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bevilacqua, R.; Barbarossa, F.; Fantechi, L.; Fornarelli, D.; Paci, E.; Bolognini, S.; Giammarchi, C.; Lattanzio, F.; Paciaroni, L.; Riccardi, G.R.; et al. Radiomics and Artificial Intelligence for the Diagnosis and Monitoring of Alzheimer’s Disease: A Systematic Review of Studies in the Field. J. Clin. Med. 2023, 12, 5432. https://doi.org/10.3390/jcm12165432
Bevilacqua R, Barbarossa F, Fantechi L, Fornarelli D, Paci E, Bolognini S, Giammarchi C, Lattanzio F, Paciaroni L, Riccardi GR, et al. Radiomics and Artificial Intelligence for the Diagnosis and Monitoring of Alzheimer’s Disease: A Systematic Review of Studies in the Field. Journal of Clinical Medicine. 2023; 12(16):5432. https://doi.org/10.3390/jcm12165432
Chicago/Turabian StyleBevilacqua, Roberta, Federico Barbarossa, Lorenzo Fantechi, Daniela Fornarelli, Enrico Paci, Silvia Bolognini, Cinzia Giammarchi, Fabrizia Lattanzio, Lucia Paciaroni, Giovanni Renato Riccardi, and et al. 2023. "Radiomics and Artificial Intelligence for the Diagnosis and Monitoring of Alzheimer’s Disease: A Systematic Review of Studies in the Field" Journal of Clinical Medicine 12, no. 16: 5432. https://doi.org/10.3390/jcm12165432